Central American Immigrant Parents’ Awareness, Acceptability, and Willingness to Vaccinate Their Adolescent Children Against Human Papillomavirus: A Pilot Cross-Sectional Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design, Setting and Sample
2.2. Ethics, Consent, and Permissions
2.3. Data Collection and Survey Measures
2.3.1. Awareness of HPV and the HPV Vaccine
2.3.2. Sources of Information About the HPV Vaccine
2.3.3. Acceptability of the HPV Vaccine and Willingness to Vaccinate
2.3.4. Participation in Future HPV-Related Cancer Prevention Study
2.3.5. Demographics, Access to Healthcare and Acculturation Level
2.4. Data Analysis
3. Results
3.1. Participants’ Characteristics
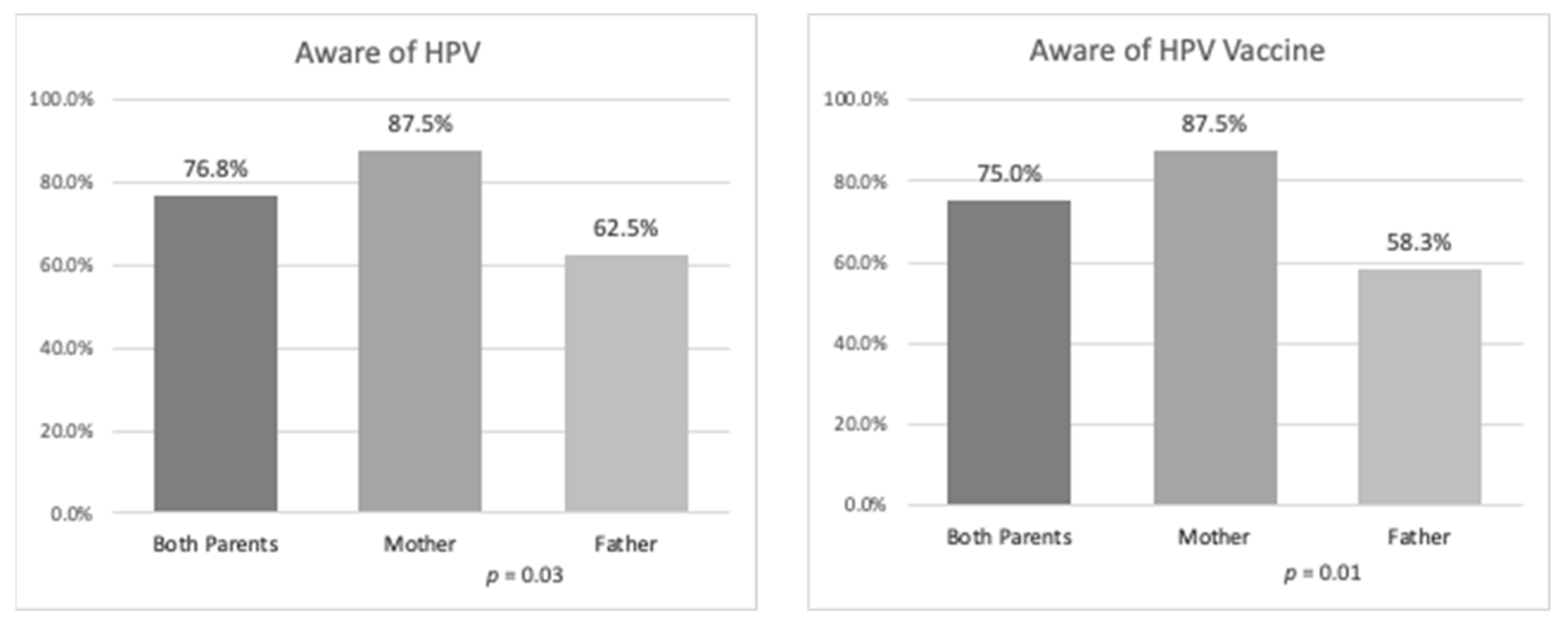
3.2. HPV and HPV Vaccine Awareness
3.3. Sources of Information About the HPV Vaccine
3.4. Acceptability of the HPV Vaccine and Willingness to Vaccinate
3.5. Interest in Participating in Future HPV-Related Cancer Prevention Study
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| US | United States |
| HPV | Human Papillomavirus |
| MA | Massachusetts |
| RI | Rhode Island |
| GED | General Education Degree |
| SASH | Short Acculturation Scale for Hispanics |
References
- Flores, A. How the U.S. Hispanic Population is Changing; Pew Research Center: Washington, DC, USA, 2017. [Google Scholar]
- National Council of La Raza. Toward a More Equitable Future: The Trends and Challenges Facing America’s Latino Children. September 2016. Available online: http://publications.nclr.org/handle/123456789/1627 (accessed on 15 January 2020).
- Profile: Hispanic/Latino Americans; U.S. Department of Health and Human Services Office of Minority Health: Washington, DC, USA, 2018.
- U.S. Census Bureau. One-Year Public Use Microdata Sample (PUMS); American Community Survey (ACS): Washington, DC, USA, 2018.
- Tyson, D.M.; Medina-Ramirez, P.; Flores, A.M.; Siegel, R.; Loi, C.A. Unpacking Hispanic ethnicity—Cancer mortality differentials among Hispanic subgroups in the United States, 2004–2014. Front. Public Health 2018, 6, 219. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Fedewa, S.A.; Miller, K.D.; Goding-Sauer, A.; Pinheiro, P.S.; Martinez-Tyson, D.; Jemal, A. Cancer statistics for Hispanics/Latinos, 2015. CA Cancer J. Clin. 2015, 65, 457–480. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Satterwhite, C.L.; Torrone, E.; Meites, E.; Dunne, E.F.; Mahajan, R.; Ocfemia, M.C.; Su, J.; Xu, F.; Weinstock, H. Sexually transmitted infections among US women and men: Prevalence and incidence estimates, 2008. Sex Transm. Dis. 2013, 40, 187–193. [Google Scholar] [CrossRef] [PubMed]
- Viens, L.J.; Henley, S.J.; Watson, M.; Markowitz, L.E.; Thomas, C.C.; Thompson, T.D.; Razzaghi, H.; Saraiya, M. Human Papillomavirus-Associated Cancers—United States, 2008–2012. Morb. Mortal. Wkly. Rep. 2016, 65, 661–666. [Google Scholar] [CrossRef] [PubMed]
- Bosch, F.X.; Broker, T.R.; Forman, D.; Moscicki, A.B.; Gillison, M.L.; Doorbar, J.; Stern, P.L.; Stanley, M.; Arbyn, M.; Poljak, M.; et al. Comprehensive control of human papillomavirus infections and related diseases. Vaccine 2013, 31, H1–H31. [Google Scholar] [CrossRef] [Green Version]
- Saraiya, M.; Unger, E.R.; Thompson, T.D.; Lynch, C.F.; Hernandez, B.Y.; Lyu, C.W.; Steinau, M.; Watson, M.; Wilkinson, E.J.; Hopenhayn, C.; et al. US assessment of HPV types in cancers: Implications for current and 9-valent HPV vaccines. J. Natl. Cancer Inst. 2015, 107, 6. [Google Scholar] [CrossRef] [Green Version]
- Markowitz, L.E.; Dunne, E.F.; Saraiya, M.; Lawson, H.W.; Chesson, H.; Unger, E.R. Centers for Disease Control Prevention (CDC) Advisory Committee on Immunization Practices (ACIP). Quadrivalent human papillomavirus vaccine: Recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep. 2014, 56, 1–24. [Google Scholar]
- Healthy People 2020 [Internet]. Washington, DC: U.S. Department of Health and Human Services, Office of Disease Prevention and Health Promotion. Available online: https://www.healthypeople.gov/2020/about-healthy-people/how-to-use-healthypeople.gov/frequently-asked-questions (accessed on 27 December 2019).
- Walker, T.Y.; Elam-Evans, L.D.; Yankey, D.; Markowitz, L.E.; Williams, C.L.; Fredua, B.; Singleton, J.A.; Stokley, S. National, Regional, State and Selected Local Area Vaccination Coverage Among Adolescents Aged 13-17 Year-United States, 2018. MMWR Morb. Mortal. Rep. 2019, 68, 718–723. [Google Scholar] [CrossRef]
- Aragones, A.; Genoff, M.; Gonzalez, C.; Shuk, E.; Gany, F. HPV vaccine and Latino immigrant parents: If they offer it, we will get it. J. Immigr. Minority Health 2016, 18, 1060–1065. [Google Scholar] [CrossRef]
- Colón-López, V.; Quiñones, V.; Del Toro-Mejías, L.M.; Conde-Toro, A.; Serra-Rivera, M.J.; Martínez, T.M.; Rodríguez, V.; Berdiel, L.; Villanueva, H. HPV awareness and vaccine willingness among Dominican immigrant parents attending a federal qualified health clinic in Puerto Rico. J. Immigr. Minority Health 2015, 17, 1086–1090. [Google Scholar] [CrossRef] [Green Version]
- Warner, E.L.; Lai, D.; Carbajal-Salisbury, S.; Garza, L.; Bodson, J.; Mooney, K.; Kepka, D. Latino parents’ perceptions of the HPV vaccine for sons and daughters. J. Community Health 2015, 40, 387–394. [Google Scholar] [CrossRef] [PubMed]
- Kepka, D.; Ding, Q.; Bodson, J.; Warner, E.L.; Mooney, K. Latino parents’ awareness and receipt of the HPV vaccine for sons and daughters in a state with low three-dose completion. J. Cancer Educ. 2015, 30, 808–812. [Google Scholar] [CrossRef] [PubMed]
- Galbraith, K.V.; Lechuga, J.; Jenerette, C.M.; Moore, L.A.; Palmer, M.H.; Hamilton, J.B. Parental acceptance and uptake of the HPV vaccine among African-Americans and Latinos in the United States: A literature review. Soc. Sci. Med. 2016, 159, 116–126. [Google Scholar] [CrossRef] [PubMed]
- Parra-Medina, D.; Morales-Campos, D.Y.; Mojica, C.; Ramirez, A.G. Promotora outreach, education and navigation support for HPV vaccination to Hispanic women with unvaccinated daughters. J. Cancer Educ. 2015, 30, 353–359. [Google Scholar] [CrossRef] [PubMed]
- Katz, I.T.; Bogart, L.M.; Fu, C.M.; Liu, Y.; Cox, J.E.; Samuels, R.C.; Chase, T.; Schubert, P.; Schuster, M.A. Barriers to HPV immunization among Blacks and Latinos: A qualitative analysis of caregivers, adolescents, and providers. BMC Public Health 2016, 16, 874. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bodson, J.; Warner, E.L.; Kepka, D. Moderate awareness and limited knowledge relating to cervical cancer, HPV, and the HPV vaccine among Hispanics/Latinos in Utah. Health Promot. Pract. 2016, 17, 548–556. [Google Scholar] [CrossRef]
- Kepka, D.; Warner, E.L.; Kinney, A.Y.; Spigarelli, M.G.; Mooney, K. Low human papillomavirus (HPV) vaccine knowledge among Latino parents in Utah. J. Immigr. Minority Health 2015, 17, 125–131. [Google Scholar] [CrossRef]
- Kepka, D.L.; Coronado, G.D.; Rodriguez, H.P.; Thompson, B. Development of a radionovela to promote HPV vaccine awareness and knowledge among Latino parents. Public Health Rep. 2012, 127, 130–138. [Google Scholar] [CrossRef] [Green Version]
- Kepka, D.; Coronado, G.D.; Rodriguez, H.P.; Thompson, B. Evaluation of a radionovela to promote HPV vaccine awareness and knowledge among Hispanic parents. J. Community Health 2011, 36, 957–965. [Google Scholar] [CrossRef] [Green Version]
- Kornfeld, J.; Byrne, M.M.; Vanderpool, R.; Shin, S.; Kobetz, E. HPV knowledge and vaccine acceptability among Hispanic fathers. J. Prim. Prev. 2013, 34, 59–69. [Google Scholar] [CrossRef] [Green Version]
- Colón-López, V.; Del Toro-Mejías, L.M.; Conde-Toro, A.; Serra-Rivera, M.J.; Martínez, T.M.; Rodríguez, V.; Ríos, A.M.; Berdiel, L.; Villanueva, H. Views on HPV and HPV vaccination: The experience at a federal qualified clinic in Puerto Rico. J. Health Care Poor Underserved 2016, 27, 1411. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calo, W.A.; Fernández, M.E.; Fernández-Espada, N.; Colón-López, V. Exploring the role of ethnic identity on the attitudes towards HPV vaccine advertising among Puerto Ricans: A qualitative analysis. J. Immigr. Minority Health 2015, 17, 314–317. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suárez, P.; Wallington, S.F.; Greaney, M.L.; Lindsay, A.C. Exploring HPV Knowledge, Awareness, Beliefs, Attitudes, and Vaccine Acceptability of Latino Fathers Living in the United States: An Integrative Review. J. Community Health 2019, 44, 844–856. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lindsay, A.C.; Greaney, M.L.; Rabello, L.M.; Kim, Y.Y.; Wallington, S.F. Brazilian Immigrant Parents' Awareness of HPV and the HPV Vaccine and Interest in Participating in Future HPV-Related Cancer Prevention Study: An Exploratory Cross-Sectional Study Conducted in the USA. J. Racial Ethn. Health Disparities 2020. [Google Scholar] [CrossRef]
- Shields, P.; Rangarjan, N. A Playbook for Research Methods: Integrating Conceptual Frameworks and Project Management; New Forums Press: Stillwater, OK, USA, 2013; ISBN 9781581072471. [Google Scholar]
- Lindsay, A.C.; Wallington, S.F.; Greaney, M.L.; Hasselman, M.H.; Machado, M.M.; Mezzavilla, R.S.; Detro, B.M. Sociocultural and Environmental Influences on Brazilian Immigrant Mothers’ Beliefs and Practices Related to Child Feeding and Weight Status. Matern Child Health J. 2017, 21, 1085–1094. [Google Scholar] [CrossRef]
- Lindsay, A.C.; Moura Arruda, C.A.; Tavares Machado, M.M.; De Andrade, G.P.; Greaney, M.L. Exploring how Brazilian immigrant mothers living in the USA obtain information about physical activity and screen time for their preschool-aged children: A qualitative study. BMJ Open 2018, 8, e021844. [Google Scholar] [CrossRef] [Green Version]
- Lindsay, A.C.; Wallington, S.F.; Muñoz, M.A.; Greaney, M.L. A qualitative study conducted in the USA exploring Latino fathers’ beliefs, attitudes and practices related to their young children’s eating, physical activity and sedentary behaviours. Public Health Nutr. 2018, 21, 403–415. [Google Scholar] [CrossRef] [Green Version]
- Lindsay, A.C.; Greaney, M.L.; Wallington, S.F.; Wright, J.A.; Hunt, A.T. Depressive Symptoms and Length of U.S. Residency Are Associated with Obesity among Low-Income Latina Mothers: A Cross-Sectional Analysis. Int. J. Environ. Res. Public Health 2017, 14, 869. [Google Scholar] [CrossRef] [Green Version]
- Faugier, J.; Sargeant, M. Sampling hard to reach populations. J. Adv. Nurs. 1997, 26, 790–797. [Google Scholar] [CrossRef]
- Marin, G.; Sabogal, F.; Marin, B.V.; Otero-Sabogal, G.; Perez-Stable, E.J. Development of a short acculturation scale for Hispanics. Hisp. J. Behav. Sci. 1987, 9, 183–205. [Google Scholar] [CrossRef]
- Ellison, J.; Jandorf, L.; Duhamel, K. Assessment of the short acculturation scale for Hispanics (SASH) among low-income, immigrant Hispanics. J. Cancer Educ. 2011, 26, 478–483. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boakye, A.E.; Tobo, B.B.; Rojek, R.P.; Mohammed, K.A.; Geneus, C.J.; Osazuwa-Peters, N. Approaching a decade since HPV vaccine licensure: Racial and gender disparities in knowledge and awareness of HPV and HPV vaccine. Hum. Vaccin. Immunother. 2017, 13, 2713–2722. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Read, D.S.; Joseph, M.A.; Polishchuk, V.; Suss, A.L. Attitudes and perceptions of the HPV vaccine in Caribbean and African-American adolescent girls and their parents. J. Pediatric Adolesc. Gynecol. 2010, 23, 242–245. [Google Scholar] [CrossRef] [PubMed]
- Kontos, E.Z.; Emmons, K.M.; Puleo, E.; Viswanath, K. Contribution of communication inequalities to disparities in human papillomavirus vaccine awareness and knowledge. Am. J. Public Health 2012, 102, 1911–1920. [Google Scholar] [CrossRef] [PubMed]
- Kobetz, E.; Dunn Mendoza, A.; Menard, J.; Finney Rutten, L.; Diem, J.; Barton, B.; Kornfeld, J.; McKenzie, N. One size does not fit all: Differences in HPV knowledge between Haitian and African American women. Cancer Epidemiol. Biomark. Prev. 2010, 19, 366–370. [Google Scholar] [CrossRef] [Green Version]
- Lechuga, J.; Vera-Cala, L.; Martinez-Donate, A. HPV vaccine awareness, barriers, intentions, and uptake in Latina women. J. Immigr. Minority Health 2016, 18, 173–178. [Google Scholar] [CrossRef]
- Jeudin, P.; Liveright, E.; Del Carmen, M.G.; Perkins, R.B. Race, ethnicity, and income factors impacting human papillomavirus vaccination rates. Clin. Ther. 2014, 36, 24–37. [Google Scholar] [CrossRef]
- Lin, L.; Benard, V.B.; Greek, A.; Hawkins, N.A.; Roland, K.B.; Saraiya, M. Racial and ethnic differences in human papillomavirus positivity and risk factors among low-income women in federally qualified health centers in the United States. Prev. Med. 2015, 81, 258–261. [Google Scholar] [CrossRef] [Green Version]
- Sanderson, M.; Coker, A.L.; Eggleston, K.S.; Fernandez, M.E.; Arrastia, C.D.; Fadden, M.K. HPV vaccine acceptance among Latina mothers by HPV status. J. Women’s Health 2009, 18, 1793–1799. [Google Scholar] [CrossRef] [Green Version]
- Alexander, A.B.; Stupiansky, N.W.; Ott, M.A.; Herbenick, D.; Reece, M.; Zimet, G.D. Parent-son decision-making about human papillomavirus vaccination: A qualitative analysis. BMC Pediatrics 2012, 12, 192. [Google Scholar] [CrossRef] [Green Version]
- Cover, J.K.; Nghi, N.Q.; LaMontagne, D.S.; Huyen, D.T.; Hien, N.T.; Nga le, T. Acceptance patterns and decision-making for human papillomavirus vaccination among parents in Vietnam: An in-depth qualitative study post-vaccination. BMC Public Health 2012, 12, 629. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Savas, L.S.; Fernández, M.E.; Jobe, D.; Carmack, C.C. Human papillomavirus vaccine: 2-1-1 helplines and minority parent decision-making. Am. J. Prev. Med. 2012, 43, S490–S496. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perkins, R.B.; Tipton, H.; Shu, E.; Marquez, C.; Belizaire, M.; Porter, C.; Clark, J.A.; Pierre-Joseph, N. Attitudes toward HPV vaccination among low-income and minority parents of sons: A qualitative analysis. Clin. Pediatrics 2013, 52, 231–240. [Google Scholar] [CrossRef] [PubMed]
- Perkins, R.B.; Apte, G.; Marquez, C.; Porter, C.; Belizaire, M.; Clark, J.A.; Pierre-Joseph, N. Factors affecting human papillomavirus vaccine use among White, Black and Latino parents of sons. Pediatric Infect. Dis. J. 2013, 32, e38–e44. [Google Scholar] [CrossRef]
- Perkins, R.B.; Pierre-Joseph, N.; Marquez, C.; Iloka, S.; Clark, J.A. Why do low-income minority parents choose human papillomavirus vaccination for their daughters? J. Pediatrics 2010, 157, 617–622. [Google Scholar] [CrossRef] [Green Version]
- Maertens, J.A.; Jimenez-Zambrano, A.M.; Albright, K.; Dempsey, A.F. Using Community Engagement to Develop a Web-Based Intervention for Latinos about the HPV Vaccine. J Health Commun. 2017, 4, 285–293. [Google Scholar] [CrossRef]
- Lu, P.J.; Yankey, D.; Fredua, B.; O’Halloran, A.C.; Williams, C.; Markowitz, L.E.; Elam-Evans, L.D. Association of Provider Recommendation and Human Papillomavirus Vaccination Initiation among Male Adolescents Aged 13-17 Years-United States. J. Pediatr. 2019, 206, 33–41.e1. [Google Scholar] [CrossRef]
- Landis, K.; Bednarczyk, R.A.; Gaydos, L.M. Correlates of HPV vaccine initiation and provider recommendation among male adolescents, 2014 NIS-Teen. Vaccine 2018, 36, 3498–3504. [Google Scholar] [CrossRef]
- Daniel, J. Choosing the size of the sample. In Sampling Essentials: Practical Guidelines for Making Sampling Choices; Daniel, J., Ed.; SAGE Publications, Inc.: Thousand Oaks, CA, USA, 2012; pp. 236–253. [Google Scholar]
- Granberry, P.; Torres, M.I.; Brenner, P.S.; Smollin, L.M.; Saavedra, J.; Person, S.D.; Allison, J.; Rosal, M.C. Cinco Minutos Solamente: Using Interviewer’s Social Capital to Increase Latino Community Survey Response Rates. J. Appl. Soc. Sci. 2017, 159–171. [Google Scholar] [CrossRef]


{kind=link}
| Variables | Total Sample | Fathers | Mothers | ||||||
|---|---|---|---|---|---|---|---|---|---|
| N | % | M (SD) | N | % | M (SD) | N | % | M (SD *) | |
| Socio-demographic variables | |||||||||
| Age | 56 | 43.2 (6.4) | 24 | 39.6 (8.2) | 32 | 45.8 (7.3) | |||
| Educational attainment | |||||||||
| Less than high school | 28 | 50.0 | 14 | 58.3 | 14 | 43.8 | |||
| High school/diploma (GED) 1 | 18 | 32.1 | 7 | 29.2 | 11 | 34.3 | |||
| More than high school | 10 | 17.9 | 3 | 12.5 | 7 | 21.9 | |||
| Marital Status | |||||||||
| Married/Cohabitating | 43 | 76.8 | 19 | 79.2 | 24 | 75.0 | |||
| Divorced/separated | 10 | 17.9 | 4 | 16.7 | 6 | 18.7 | |||
| Single | 3 | 5.2 | 1 | 4.1 | 2 | 6.3 | |||
| Number of children 11–19 years of age | |||||||||
| 1 | 32 | 57.1 | 13 | 54.2 | 19 | 59.4 | |||
| 2 | 22 | 39.3 | 10 | 41.7 | 12 | 31.5 | |||
| 3 | 2 | 3.6 | 1 | 8.3 | 1 | 3.1 | |||
| Annual household income 2 | |||||||||
| Less than US$40,000/year | 44 | 78.6 | 15 | 62.5 | 29 | 90.6 | |||
| More than or equal to US$40,000/year | 10 | 17.9 | 7 | 29.2 | 3 | 9.4 | |||
| Missing | 2 | 3.5 | 2 | 8.3 | 0 | 0 | |||
| Health insurance status | |||||||||
| Government health insurance | 45 | 80.4 | 15 | 62.5 | 30 | 93.7 | |||
| Private health insurance | 5 | 8.9 | 5 | 20.8 | 0 | 0 | |||
| Uninsured | 6 | 10.7 | 4 | 16.7 | 2 | 6.3 | |||
| Foreign-born | |||||||||
| Yes | 54 | 96.4 | 23 | 95.8 | 31 | 96.8 | |||
| No | 2 | 3.6 | 1 | 4.2 | 1 | 3.2 | |||
| Country of Origin of foreign-born | |||||||||
| El Salvador | 27 | 50.0 | 13 | 56.6 | 14 | 45.2 | |||
| Guatemala | 14 | 25.9 | 5 | 21.7 | 9 | 29.0 | |||
| Honduras | 12 | 22.2 | 5 | 21.7 | 7 | 22.6 | |||
| Panama | 1 | 1.9 | 0 | 0 | 1 | 3.2 | |||
| Acculturation variables | |||||||||
| Years of residence in the United States | 54 | 13.7 (7.2) | 23 | 15.8 (8.9) | 31 | 12.9 (9.4) | |||
| SASH score 3, 4 | |||||||||
| <2.99 | 51 | 94.4 | 21 | 91.3 | 30 | 96.8 | |||
| ≥2.99 | 3 | 5.6 | 2 | 8.7 | 1 | 3.2 | |||
| Survey Measures | Total Sample | Fathers | Mothers | p-Value 1 | |||
|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | ||
| Awareness of HPV | |||||||
| Yes | 43 | 76.8 | 15 | 62.5 | 28 | 87.5 | p = 0.03 |
| No | 13 | 23.1 | 9 | 32.5 | 4 | 12.5 | p = 0.03 |
| Awareness of the HPV vaccine | |||||||
| Yes | 42 | 75.0 | 14 | 58.3 | 28 | 87.5 | p = 0.01 |
| No | 14 | 25.0 | 10 | 41.7 | 4 | 12.5 | p = 0.03 |
| Sources of information about the HPV vaccine 2 ,3 | |||||||
| Health care information sources | |||||||
| Child’s physician | 35 | 83.3 | 8 | 57.1 | 27 | 96.4 | p = 0.01 |
| Nurses | 6 | 14.3 | 2 | 14.3 | 4 | 14.3 | p = 0.96 |
| Public health campaigns | 7 | 16.7 | 5 | 35.7 | 2 | 7.1 | p = 0.02 |
| Non-health care information sources | |||||||
| Personal sources | |||||||
| Family | 10 | 23.8 | 7 | 50.0 | 3 | 10.7 | p = 0.05 |
| Friends | 2 | 4.8 | 0 | 0 | 2 | 7.1 | p = 0.54 |
| Media sources | |||||||
| Internet | 10 | 23.8 | 4 | 28.6 | 6 | 21.4 | p = 0.61 |
| Television or radio | 8 | 19.0 | 6 | 42.9 | 2 | 7.1 | p = 0.06 |
| Billboards | 2 | 4.8 | 1 | 7.1 | 1 | 3.6 | p = 1.00 |
| Acceptability of the HPV vaccine 4 | |||||||
| Yes | 36 | 85.7 | 9 | 64.3 | 27 | 96.4 | p = 0.06 |
| No | 1 | 2.4 | 0 | 0 | 1 | 3.6 | p = 1.00 |
| Don’t know | 5 | 12.2 | 5 | 35.7 | 0 | 0 | p = 0.01 |
| Willingness to vaccinate if recommended by child’s physician 5 | |||||||
| Yes | 18 | 90.0 | 13 | 86.7 | 5 | 100 | p = 1.00 |
| No | 2 | 10.0 | 2 | 13.3 | 0 | 0 | p = 1.00 |
| Interest in participating in HPV-related cancer prevention study | |||||||
| Yes | 49 | 87.5 | 20 | 83.3 | 29 | 90.6 | p = 0.42 |
| No | 7 | 12.5 | 4 | 16.7 | 3 | 9.4 | p = 0.42 |
| Survey Measures | SASH Score 1 | Educational Attainment | Household Income 2 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| N (%) | N (%) | N (%) | |||||||
| <2.99 | ≥2.99 | p-Value | <HS | ≥HS | p-Value | <US$40k | ≥US$40k | p-Value 3 | |
| Awareness of HPV | |||||||||
| Yes | 41 (80.4) | 2 (66.7) | p = 1.00 | 15 (53.6) | 26 (92.8) | p = 0.001 | 33 (75.0) | 10 (100.0) | p = 0.08 |
| No | 10 (19.6) | 1 (33.3) | p = 1.00 | 13 (46.4) | 2 (7.2) | p = 0.001 | 11 (25.0) | 0 (0) | p = 0.08 |
| Awareness of the HPV vaccine | |||||||||
| Yes | 39 (76.5) | 2 (66.7) | p = 1.00 | 15 (53.6) | 26 (92.8) | p = 0.001 | 31 (70.5) | 10 (100.0) | p = 0.05 |
| No | 12 (23.5) | 1 (33.3) | p = 1.00 | 13 (46.4) | 2 (7.2) | p = 0.001 | 13 (29.5) | 0 | p = 0.28 |
| Uptake of the vaccine 4 | |||||||||
| Yes | 33 (86.8) | 3 (100.0) | p = 1.00 | 11 (73.3) | 25 (96.2) | p = 0.03 | 26 (86.7) | 10 (100.0) | p = 0.56 |
| No | 5 (13.2) | 0 (0) | p = 1.00 | 4 (26.7) | 1 (3.8) | p = 0.03 | 4 (13.3) | 0 | p = 0.56 |
| Willingness to vaccinate if recommended by child’s physician 5 | |||||||||
| Yes | 15 (88.2) | 0 | 13 (90.0) | 3 (100.0) | p = 0.58 | 15 (88.2) | 0 | ||
| No | 2 (11.8) | 0 | 4 (10.0) | 0 (0) | p = 0.58 | 2 (11.8) | 0 | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lindsay, A.C.; Pineda, J.A.; Valdez, M.J.; Torres, M.I.; Granberry, P.J. Central American Immigrant Parents’ Awareness, Acceptability, and Willingness to Vaccinate Their Adolescent Children Against Human Papillomavirus: A Pilot Cross-Sectional Study. Int. J. Environ. Res. Public Health 2020, 17, 2869. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17082869
Lindsay AC, Pineda JA, Valdez MJ, Torres MI, Granberry PJ. Central American Immigrant Parents’ Awareness, Acceptability, and Willingness to Vaccinate Their Adolescent Children Against Human Papillomavirus: A Pilot Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2020; 17(8):2869. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17082869
Chicago/Turabian StyleLindsay, Ana Cristina, Joanna A. Pineda, Madelyne J. Valdez, Maria Idalí Torres, and Phillip J. Granberry. 2020. "Central American Immigrant Parents’ Awareness, Acceptability, and Willingness to Vaccinate Their Adolescent Children Against Human Papillomavirus: A Pilot Cross-Sectional Study" International Journal of Environmental Research and Public Health 17, no. 8: 2869. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17082869