Workers’ Healthcare Assistance Model (WHAM): Development, Validation, and Assessment of Sustainable Return on Investment (S-ROI)

 , ,
, ,  and
and 
Abstract
:1. Introduction
2. Literature Review
3. Materials and Methods
3.1. Study Design
3.2. Data Analyses
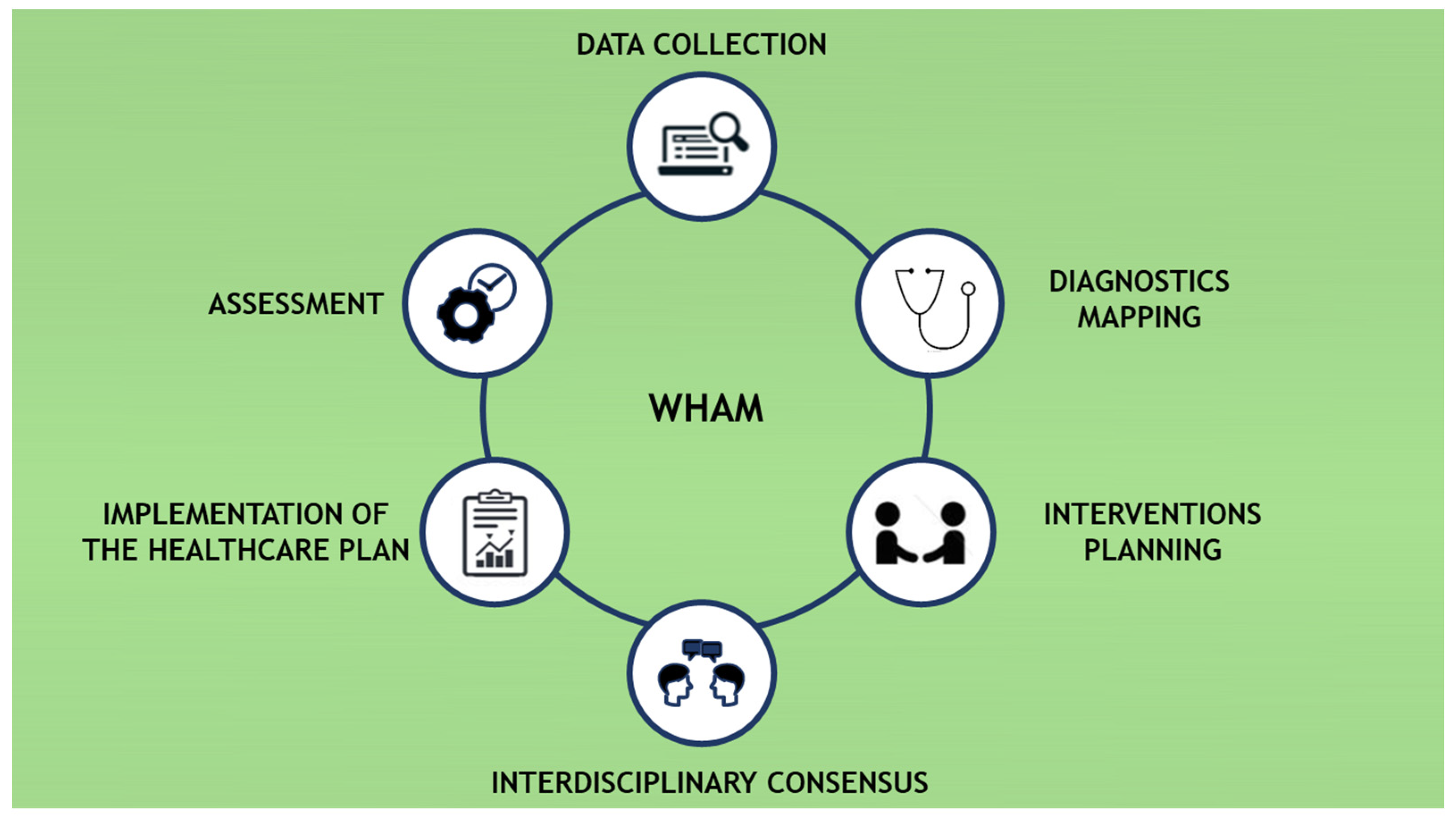
3.3. Model Development
3.3.1. Data Collection
3.3.2. Diagnostics Mapping
3.3.3. Intervention Planning
3.3.4. Interdisciplinary Consensus
3.3.5. Implementation of the Healthcare Plan
3.3.6. Assessment
3.4. WHAM Validation
3.5. Assessment of Sustainable Return on Investment (S-ROI)
3.6. Ethical Approval
4. Results
5. Discussion
Implications for Workplace
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Andersen:, K.G.; Rambaut, A.; Lipkin, W.I.; Holmes, E.C.; Garry, R.F. The proximal origin of SARS-CoV-2. Nat. Med. 2020, 26. [Google Scholar] [CrossRef] [Green Version]
- Stenvinkel, P. The One Health concept--the health of humans is intimately linked with the health of animals and a sustainable environmen. J. Intern. Med. 2020, 287, 223–225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Health Services Delivery Programme Division of Health Systems and Public Health. Integrated Care Models: An Overview; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- Brasil. Ministério da Saúde Agência Nacional de Saúde Suplementar. Duas Faces da Mesma Moeda: Microrregulação e Modelos Assistenciais na Saúde Suplementar. In [National Agency for Supplementary Health. Two Faces of the Same Coin: Microregulation and Care Models in Supplementary Health]; Agência Nacional de Saúde Suplementar: Rio de Janeiro, Brazil, 2005. [Google Scholar]
- Campos, G.W.S. Reforma da Reforma: Repensando a Saúde [Reform Reform: Rethinking Health]; Hucitec: São Paulo, Brazil, 1992. [Google Scholar]
- Campos, G.W.S. Modelos Assistenciais e Unidades Básicas de Saúde: Elementos para Debate [Care Models and Basic Health Units: Elements for Debate]. In Planejamento Sem Normas; Campos, G.W.S., Ed.; Hucitec: São Paulo, Brazil, 1994; pp. 53–60. [Google Scholar]
- Paim, J.A. Modelos de atenção e vigilância da saúde [Health care and surveillance models]. In Epidemiologia e Saúde; Rouquayrol, M., Almeida, F., Eds.; MEDSI: Rio de Janeiro, Brazil, 2003; pp. 567–586. [Google Scholar]
- Merhy, E.E. Saúde: Cartografia do Trabalho vivo [Health: Mapping of Living Work]; Hucitec: São Paulo, Brazil, 2002. [Google Scholar]
- Morosini, M.V.G.C.; Corbo, A.D.A. Modelos de Atenção e a Saúde da Família [Models of Care and Family Health]; EPSJV, Fiocruz: Rio de Janeiro, Brazil, 2007. [Google Scholar]
- Rosa, W.A.G.; Labate, R.C. Programa Saúde da Família: A construção de um novo modelo de assistência [Family Health Program: The construction of a new care model]. Rev. Lat. Am. Enfermagem. 2005, 13, 1027–1034. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paim, J.S. Modelos de atenção à saúde no Brasil [Health care models in Brazil]. In Políticas e Sistema de Saúde no Brasil; Giovanella, L., Escorel, S., Lobato, L.V.C., Noronha, J.C., Carvalho, A.I., Eds.; Fiocruz: Rio de Janeiro, Brazil, 2008; pp. 547–573. [Google Scholar]
- Santos, M. Communication on health and safety risk control in contemporary society: An interdisciplinary approach. Ciência Saúde Coletiva saúde coletiva 2007, 12, 1375–1386. [Google Scholar]
- Mendes, E.V. O Cuidado das Condições Crônicas na Atenção Primária à saúde: O Imperativo da Consolidação da Estratégia da Saúde da Família [The Care of Chronic Conditions in Primary Health Care: The Imperative of Consolidating the Family Health Strategy]; Organização Pan-Americana da Saúde: Brasília, Brazil, 2012. [Google Scholar]
- Silva Júnior, A.G.; Alves, C. Modelos Assistenciais em Saúde: Desafios e perspectivas [Health Care Models: Challenges and perspectives]. In Modelos de Atenção e a Saúde da Família; Morosini, M.V.G.C., Corbo, A.D.A., Eds.; EPSJV, Fiocruz: Rio de Janeiro, Brazil, 2007; pp. 27–41. [Google Scholar]
- Fertonani, H.P.; De Pires, D.E.P.; Biff, D.; Dos Scherer, M.D.A. The health care model: Concepts and challenges for primary health care in Brazil. Cienc. e Saude Coletiva 2015, 20, 1869–1878. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coelho, M.O.; Jorge, M.S.B. Technology of relations as device of humanized attendance in basic attention to health in the perspective of access, sheltering and attachment. Cienc. e Saude Coletiva 2009, 14, 1523–1531. [Google Scholar] [CrossRef] [Green Version]
- Capra, F. O Ponto de Mutação [The Mutation Point], 30th ed.; Cortez: São Paulo, Brazil, 2012. [Google Scholar]
- Silva Júnior, A.G. Modelos Tecnoassistenciais em Saúde: O Debate do Campo da Saúde Coletiva [Techno-Health Care Models: The Debate in the Field of puBlic Health]; Hucitec: São Paulo, Brazil, 1998. [Google Scholar]
- Costa, A.S.; Viterbo, L.M.F.; Silva, I.B.; Nascimento, S.d.O.; Vidal, D.G.; Dinis, M.A.P. Use of Light Technologies as a Strategy for Changing the Health Profile of Workers with Chronic Conditions in the Oil Industry, Bahia, Brazil. In Proceedings of the Person Centred Healthcare International Congress Proceedings; APASD: Porto, Portugal, 2020; pp. 55–56. [Google Scholar]
- Scarpi, M.J. Introduction. In Administração em Saúde: Autogestão de Consultórios e Clínicas; Doc: Rio de Janeiro, Brazil, 2010; pp. 17–18. [Google Scholar]
- Faria, H.P.D.; Coelho, I.B.; Werneck, M.A.F.; Santos, M.A. Dos Modelo Assistencial e Atenção Básica à Saúde [Care Model and Primary Health Care], 2nd ed.; Nescon/UFMG, Coopmed: Belo Horizonte, Brazil, 2010. [Google Scholar]
- Agency for Clinical Innovation. Understanding the Process to Develop a Model of Care: An. ACI Framework; Agency for Clinical Innovation: Sydney, Australia, 2013. [Google Scholar]
- Viterbo, L.M.F.; Dinis, M.A.P.; Vidal, D.G.; Costa, A.S. Implementation of an Interdisciplinary Approach to Promote Workers Global Health Status in the Oil Industry, Brazil (2006–2015). Int. J. Environ. Res. Public Heal. 2019, 16, 2148. [Google Scholar] [CrossRef] [Green Version]
- Viterbo, L.M.F.; Costa, A.S.; Dinis, M.A.P. Interdisciplinarity: An articulating movement in the field of worker’s health. In La Comunicación ante el Ciudadano; Viniegra, L.M., Chávez, S.M., Rodrigo, E.M., Eds.; Editorial GEDISA: Madrid, Spain, 2018; pp. 323–334. ISBN 9788417690045. [Google Scholar]
- Almeida, G.E.S.D. Significados e limites das estratégias de integração disciplinar: Uma reflexão sobre as contribuições da saúde do trabalhador [Meanings and limits concerned to the strategies of disciplinary integration: A reflection about the contributions from the work]. Cien. Saude Colet. 2000, 7, 335–347. [Google Scholar]
- Lacaz, F.A.D.C. O campo Saúde do Trabalhador: Resgatando conhecimentos e práticas sobre as relações trabalho-saúde [The Field of Occupational Health: Rescuing knowledge and practices about work-health relations]. Cad. Saude Publica 2007, 23, 757–766. [Google Scholar] [CrossRef] [Green Version]
- Annandale, E. The Sociology of Health and Medicine: A Critical Introduction; Polity Press: Cambridge, UK, 1998. [Google Scholar]
- Kelly, M.P.; Morgan, A.; Bonnefoy, J.; Butt, J.; Bergman, V.; Mackenbach, W.J.; Exworthy, M.; Popay, J.; Tugwell, P.; Robinson, V.; et al. The Social Determinants of Health: Developing an Evidence Base for Political Action; Final Report to World Health Organization Commission on the Social Determinants of Health; National Institute for Health and Clinical Excellence: London, UK, 2007. [Google Scholar]
- Graham, H.; White, P.C.L. Social determinants and lifestyles: Integrating environmental and public health perspectives. Public Health 2016, 141, 270–278. [Google Scholar] [CrossRef]
- Malta, D.C.; Felisbino-Mendes, M.S.; Machado, Í.E.; Passos, V.M.D.A.; Abreu, D.M.X.D.; Ishitani, L.H.; Velásquez-Meléndez, G.; Carneiro, M.; Mooney, M.; Naghavi, M. Fatores de risco relacionados à carga global de doença do Brasil e Unidades Federadas [Risk factors related to the global burden of disease in Brazil and Federated Units], 2015. Rev. Bras. Epidemiol. 2017, 20, 217–232. [Google Scholar]
- Dinis, M.A.P. Environment and Human Health. J. Environ. Pollut. Hum. Heal. 2016, 4, 52–59. [Google Scholar] [CrossRef] [Green Version]
- Oliveira, G.M.; Vidal, D.G.; Viterbo, L.M.F.; Costa, A.S.; Ferraz, M.P. Health Monitoring and Intervention Plan on Oil Industry Workers: Results from a Case-Study. In Occupational and Environmental Safety and Health II. Studies in Systems, Decision and Control; Arezes, P.M., Baptista, J.S., Barroso, M.P., Carneiro, P., Cordeiro, P., Costa, N., Melo, R.B., Miguel, A.S., Perestrelo, G., Eds.; Springer International Publishing: Cham, Switzerland, 2020; pp. 265–274. ISBN 978-3-030-41486-3. [Google Scholar]
- Casini, M.; Bastianoni, S.; Gagliardi, F.; Gigliotti, M.; Riccaboni, A.; Betti, G. Sustainable Development Goals Indicators: A Methodological Proposal for a Multidimensional Fuzzy Index in the Mediterranean Area. Sustainability 2019, 11, 1198. [Google Scholar] [CrossRef] [Green Version]
- Da Silva, J.M.; dos Santos, M.O.S.; Augusto, L.G.D.S.; Gurgel, I.G.D. Desenvolvimento sustentável e saúde do trabalhador nos estudos de impacto ambiental de refinarias no Brasil [Sustainable development and worker health in the environmental impact studies of refineries in Brazil]. Saude e Soc. 2013, 22, 687–700. [Google Scholar] [CrossRef] [Green Version]
- Raziq, A.; Maulabakhsh, R. Impact of Working Environment on Job Satisfaction. 2nd Glob. Conf. Bus. Econ. Manag. Tour. 2015, 23, 717–725. [Google Scholar] [CrossRef]
- Carande-Kulis, V.; Stevens, J.A.; Florence, C.S.; Beattie, B.L.; Arias, I. A cost–benefit analysis of three older adult fall prevention interventions. J. Saf. Res. 2015, 52, 65–70. [Google Scholar] [CrossRef]
- Pelletier, K.R. A review and analysis of the health and cost-effective outcome studies of comprehensive health promotion and disease prevention programs. Am. J. Health Promot. 1991, 5, 311–313. [Google Scholar] [CrossRef]
- Goetzel, R.Z.; Ozminkowski, R.J. The Health and Cost Benefits of Work Site Health-Promotion Programs. Ann. Rev. Public Health 2008, 29, 303–323. [Google Scholar] [CrossRef] [Green Version]
- Bly, J.L.; Jones, R.C.; Richardson, J.E. Impact of worksite health promotion on health care costs and utilization. Evaluation of Johnson & Johnson’s Live for Life program. JAMA 1986, 256, 3235–3240. [Google Scholar]
- Breslow, L.; Fielding, J.; Herrman, A.A.; Wilbur, C.S. Worksite health promotion: Its evolution and the Johnson & Johnson experience. Prev. Med. (Baltim) 1990, 19, 13–21. [Google Scholar]
- Ozminkowski, R.J.; Dunn, R.L.; Goetzel, R.Z.; Cantor, R.I.; Murnane, J.; Harrison, M. A return on investment evaluation of the Citibank, N.A., health management program. Am. J. Health Promot. 1999, 14, 31–43. [Google Scholar] [CrossRef]
- Serxner, S.; Anderson, D.R.; Gold, D. Building program participation: Strategies for recruitment and retention in worksite health promotion programs. Am. J. Health Promot. 2004, 18, 1–6. [Google Scholar]
- Poisal, J.A.; Truffer, C.; Smith, S.; Sisko, A.; Cowan, C.; Keehan, S.; Dickensheets, B. Health spending projections through 2016: Modest changes obscure part D’s impact. Health Aff. (Millwood) 2007, 26, w242–w253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dement, J.M.; Epling, C.; Joyner, J.; Cavanaugh, K. Impacts of Workplace Health Promotion and Wellness Programs on Health Care Utilization and Costs: Results From an Academic Workplace. J. Occup. Environ. Med. 2015, 57, 1159–1169. [Google Scholar] [CrossRef] [PubMed]
- Munir, F.; Miller, P.; Biddle, S.J.H.; Davies, M.J.; Dunstan, D.W.; Esliger, D.W.; Gray, L.J.; O’Connell, S.E.; Waheed, G.; Yates, T.; et al. A Cost and Cost-Benefit Analysis of the Stand More AT Work (SMArT Work) Intervention. Int. J. Environ. Res. Public Health 2020, 17, 1214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peik, S.; Schimmel, E.; Hejazi, S. Projected return on investment of a corporate global health programme. BMC Public Health 2019, 19, 1476. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gao, L.; Flego, A.; Dunstan, D.W.; Winkler, E.A.; Healy, G.N.; Eakin, E.G.; Willenberg, L.; Owen, N.; LaMontagne, A.D.; Lal, A.; et al. Economic evaluation of a randomized controlled trial of an intervention to reduce office workers’ sitting time: The “Stand Up Victoria” trial. Scand. J. Work. Environ. Health 2018, 44, 503–511. [Google Scholar] [CrossRef]
- Viterbo, L.M.F.; Dinis, M.A.P.; Vidal, D.G.; Costa, A.S.; Oliveira, P.V.G.; do Nascimento, J.G.; Simões, H.; do Nascimento, J.G.; Simões, H. Health Risk Assessment in Oil Industry in Bahia, Brazil: The Worker’s Health Risk Index (WHRI). In Occupational and Environmental Safety and Health II; Arezes, P.M., Baptista, J.S., Barroso, M.P., Carneiro, P., Cordeiro, P., Costa, N., Melo, R.B., Miguel, A.S., Perestrelo, G., Eds.; Springer International Publishing: Cham, Switzerland, 2020; pp. 311–321. ISBN 978-3-030-41486-3. [Google Scholar]
- Viterbo, L.M.F.; Dinis, M.A.P.; Costa, A.S.; Vidal, D.G. Development and Validation of an Interdisciplinary Worker’s Health Approach Instrument (IWHAI). Int. J. Environ. Res. Public Health 2019, 16, 2803. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization ICD-11—International Classification of Diseases 11th Revision. The Global Standard for Diagnostic Health Information. Available online: https://icd.who.int/en (accessed on 17 March 2020).
- Truppel, T.C.; Meier, M.J.; Calixto, R.D.C.; Peruzzo, S.A.; Crozeta, K. Sistematização da Assistência de Enfermagem em Unidade de Terapia Intensiva [Systematization of Nursing Care in an Intensive Care Unit]. Rev. Bras. Enferm. 2010, 62, 221–227. [Google Scholar] [CrossRef]
- Nóbrega, M.M.L.D.; Garcia, T.R. Classificação Internacional para a Prática de Enfermagem: Instrumental tecnológico para a prática profissional [International Classification for Nursing Practice: Technological instrument for professional practice]. Rev. Bras. Enferm. 2009, 62, 758–761. [Google Scholar] [CrossRef] [Green Version]
- Academy of Nutrition and Dietetics. International Dietetics and Nutritional Terminology (Idnt) Reference Manual: Standard Language for the Nutrition Care Process, 4th ed.; Academy of Nutrition and Dietetics: Cleveland, OH, USA, 2012. [Google Scholar]
- World Health Organization. International Classification of Functioning, Disability and Health; World Health Organization: Geneva, Switzerland, 2001. [Google Scholar]
- Dinis, M.A.P.; Sousa, H.F.P.; Moura, A.D.; Viterbo, L.M.F.; Pinto, R.J. Health Behaviors as a Mediator of the Association Between Interpersonal Relationships and Physical Health in a Workplace Context. Int. J. Environ. Res. Public Health 2019, 16, 2392. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wellcast Decision Support Our Analytical Tool: Wellcast Roi. Available online: http://www.wellcast-roi.com/pt/?p=wellcastroi (accessed on 20 March 2020).
- Mahmood, S.S.; Levy, D.; Vasan, R.S.; Wang, T.J. The Framingham Heart Study and the epidemiology of cardiovascular disease: A historical perspective. Lancet 2014, 383, 999–1008. [Google Scholar] [CrossRef] [Green Version]
- Brasil. Ministério da Saúde. Approves Regulatory Norms of Research Involving Human Beings; National Health Council Resolution No 466 of December 12, 2012; Diário Oficial da União: Brasília, Brazil, 2012.
- Eng, J.Y.; Moy, F.M.; Bulgiba, A. Impact of a workplace health promotion program on employees’ blood pressure in a public university. PLoS ONE 2016, 11, e0148307. [Google Scholar] [CrossRef] [PubMed]
- Hochart, C.; Lang, M. Impact of a Comprehensive Worksite Wellness Program on Health Risk, Utilization, and Health Care Costs. Popul. Health Manag. 2011, 14, 111–116. [Google Scholar] [CrossRef] [PubMed]
- Preshaw, P.M.; Alba, A.L.; Herrera, D.; Jepsen, S.; Konstantinidis, A.; Makrilakis, K.; Taylor, R. Periodontitis and diabetes: A two-way relationship. Diabetologia 2012, 55, 21–31. [Google Scholar] [CrossRef] [Green Version]
- Lertpimonchai, A.; Rattanasiri, S.; Arj-Ong Vallibhakara, S.; Attia, J.; Thakkinstian, A. The association between oral hygiene and periodontitis: A systematic review and meta-analysis. Int. Dent. J. 2017, 67, 332–343. [Google Scholar] [CrossRef] [Green Version]
- Viterbo, L.M.F.; Vidal, D.G.; Costa, A.S.; Dinis, M.A.P. Effectiveness of an Oral Health Program Among Brazilian Oil Workers. In Occupational and Environmental Safety and Health II. Studies in Systems, Decision and Control; Arezes, P.M., Baptista, J.S., Barroso, M.P., Carneiro, P., Cordeiro, P., Costa, N., Melo, R.B., Miguel, A.S., Perestrelo, G., Eds.; Springer International Publishing: Cham, Switzerland, 2020; pp. 305–310. ISBN 978-3-030-41486-3. [Google Scholar]
- Sami, W.; Ansari, T.; Butt, N.S.; Rashid, M.; Hamid, A. Effect Of Diet Counseling On Type 2 Diabetes Mellitus. Int. J. Sci. Technol. Res. 2015, 4, 112–118. [Google Scholar]
- Holynska, A.; Kucharska, A.; Sinska, B.; Panczyk, M. The level of nutrition knowledge versus dietary habits of diabetes patients treated with insulin. Pol. Merkur. Lekarski 2015, 39, 292–296. [Google Scholar]
- Breen, C.; Ryan, M.; Gibney, M.J.; O’Shea, D. Diabetes-related nutrition knowledge and dietary intake among adults with type 2 diabetes. Br. J. Nutr. 2015, 114, 439–447. [Google Scholar] [CrossRef] [Green Version]
- Warnakulasuriya, S.; Kashyap, R.; Dasanayake, A.P. Is workplace screening for potentially malignant oral disorders feasible in India? J. Oral. Pathol. Med. 2010, 39, 672–676. [Google Scholar] [CrossRef]
- Jirathananuwat, A.; Pongpirul, K. Promoting physical activity in the workplace: A systematic meta-review. J. Occup. Health 2017, 59, 385–393. [Google Scholar] [CrossRef] [PubMed]
- Skovlund, S.V.; Blafoss, R.; Sundstrup, E.; Andersen, L.L. Association between physical work demands and work ability in workers with musculoskeletal pain: Cross-sectional study. BMC Musculoskelet. Disord. 2020, 21, 166. [Google Scholar] [CrossRef] [PubMed]
- Welch, A.; Healy, G.; Straker, L.; Comans, T.; O’Leary, S.; Melloh, M.; Sjogaard, G.; Pereira, M.; Chen, X.; Johnston, V. Process evaluation of a workplace-based health promotion and exercise cluster-randomised trial to increase productivity and reduce neck pain in office workers: A RE-AIM approach. BMC Public Health 2020, 20, 180. [Google Scholar]
- Hafez, D.; Fedewa, A.; Moran, M.; O’Brien, M.; Ackermann, R.; Kullgren, J.T. Workplace Interventions to Prevent Type 2 Diabetes Mellitus: A Narrative Review. Curr. Diab. Rep. 2017, 17, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gan, Y.; Yang, C.; Tong, X.; Sun, H.; Cong, Y.; Yin, X.; Li, L.; Cao, S.; Dong, X.; Gong, Y.; et al. Shift work and diabetes mellitus: A meta-analysis of observational studies. Occup. Environ. Med. 2015, 72, 72–78. [Google Scholar] [CrossRef] [Green Version]
- Clark, P.G.; Leinhaas, M.M.; Filinson, R. Developing and Evaluating an Interdisciplinary Clinical Team Training Program: Lessons Taught and Lessons Learned. Educ. Gerontol. 2002, 28, 491–510. [Google Scholar] [CrossRef]
- Costa, A.S.; Viterbo, L.M.F.; Vidal, D.G.; Dinis, M.A.P.; Simões, H. Communication of Environmental Risks to Potentially Exposed Workers: An Experience in the Oil Industry, Bahia, Brazil. In Occupational and Environmental Safety and Health II. Studies in Systems, Decision and Control; Arezes, P.M., Baptista, J.S., Barroso, M.P., Carneiro, P., Cordeiro, P., Costa, N., Melo, R.B., Miguel, A.S., Perestrelo, G., Eds.; Springer International Publishing: Cham, Switzerland, 2020; pp. 59–64. ISBN 978-3-030-41486-3. [Google Scholar]
- Aldana, S.G. Financial impact of health promotion programs: A comprehensive review of the literature. Am. J. Health Promot. 2001, 15, 296–320. [Google Scholar] [CrossRef]
- Chapman, L.S. Meta-evaluation of worksite health promotion economic return studies: 2005 update. Am. J. Health Promot. 2005, 19, 1–11. [Google Scholar] [CrossRef]
- Pelletier, K.R. A review and analysis of the clinical and cost-effectiveness studies of comprehensive health promotion and disease management programs at the worksite: Update VI 2000-2004. J. Occup. Environ. Med. 2005, 47, 1051–1058. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Population n (%) | Sample n (%) | Difference (%) | p | |
|---|---|---|---|---|
| Sex | ||||
| Male | 1117 (87.6) | 884 (91.6) | 4.0 | >0.05 |
| Female | 158 (12.4) | 81 (8.4) | −4.0 | |
| Age Group | 0.7 | |||
| ≤29 | 50 (3.9) | 44 (4.6) | −0.5 | |
| 30 a 39 | 350 (27.5) | 261 (27.0) | 2.5 | |
| 40 a 49 | 245 (19.2) | 209 (21.7) | −1.1 | |
| 50 a 59 | 556 (43.6) | 410 (42.5) | −1.6 | |
| ≥60 | 74 (5.8) | 41 (4.2) | 4.0 | |
| Total | 1275 | 965 |
| Dimension | Indicator (Assessment Number) | Prevalent Diagnostics | n (%) | Prevalent Intervention | n (%) |
|---|---|---|---|---|---|
| Physical Education | Physical Activity Level (527) | General Physical Resistance—Sedentary | 140 (26.6) | Guide and Clarify the Frequency and Duration of Activities Performed to Increase the Level of Physical Activity | 290 (55.1) |
| Contemplation Stage for Physical Activity Practice (322) | Serious Difficulty in Making Decisions—Contemplation | 96 (29.8) | Encourage Thinking about Starting a Physical Activity Program, Warning about the Harm of Physical Inactivity | 273 (84.8) | |
| Feeling of Pain (71) | Moderate Pain | 34 (47.9) | Guide to Work Physiotherapy | 35 (49.3) | |
| Cardiorespiratory Fitness (135) | Regular Aerobic Capacity | 103 (76.3) | Recommend Specific Physical Activity | 89 (66.4) | |
| Abdominal Strength Level (222) | General Physical Resistance—Regularly Active | 58 (26.1) | Stimulate and Guide for Resistance Exercise | 134 (60.4) | |
| Flexibility Level (386) | Mobility of Several Joints—Weak Moderate Disability | 85 (22.0) | Encourage and Guide for Flexibility Exercise | 273 (70.7) | |
| Manual Gripping Force (121) | General Physical Resistance—Regularly Active | 32 (26.4) | Stimulate and Guide for Resistance Exercise | 93 (77.5) | |
| Nursing | Ergonomic Risks—Physical Aspects (193) | Impaired Ergonomic Condition | 148 (76.7) | Promote Ergonomic Comfort | 191 (99.0) |
| Ergonomic Risks—Organizational Aspects (46) | Stress due to Change or Transfer of Environment | 16 (34.8) | Obtain Data on Ability to Manage Stress | 19 (42.2) | |
| Work Environment Health Conditions (140) | Impaired Health Surveillance | 133 (95.0) | Inspect the Workplace | 100 (71.4) | |
| Family Relationships (25) | Impaired Family Process | 9 (36.0) | Support Family Coping Process | 12 (48.0) | |
| Social Aspects—Leisure (14) | Impaired Ability to Perform Leisure Activities | 14 (100.0) | Implement Leisure and Fun Activities for Workers and Family Members | 7 (50.0) | |
| Self-Care Level (585) | Health-Seeking Behavior | 165 (28.2) | Reinforce Positive Behavior | 106 (18.1) | |
| Medicine | Tobacco Use (22) | Tobacco Use | 16 (72.7) | Encourage Health-Seeking Behavior | 21 (95.5) |
| Stress Level and Symptoms (64) | Symptoms and Signs Related to Emotional State | 13 (20.3) | Encourage Health-Seeking Behavior | 38 (59.4) | |
| Dyslipidemia (515) | Pure hypercholesterolemia | 179 (34.8) | Encourage Health-Seeking Behavior | 362 (70.4) | |
| Diabetes Mellitus (68) | Non-insulin-dependent | 53 (77.9) | Guide to Specialist | 42 (61.8) | |
| Systemic Arterial Hypertension (94) | Primary Essential Hypertension | 82 (87.2) | Encourage Health-Seeking Behavior | 51 (54.3) | |
| Musculoskeletal Pathology (111) | Low Back Pain | 21 (18.9) | Encourage Health-Seeking Behavior | 69 (62.2) | |
| Psychiatric Pathology (10) | Generalized Anxiety | 2 (20.0) | Encourage Health-Seeking Behavior | 7 (77.8) | |
| Altered Glycemia (93) | Increased Blood Glucose | 62 (66.7) | Guide to Specialist | 50 (53.8) | |
| Altered Blood Pressure (220) | Primary Essential Hypertension | 111 (50.5) | Guide to Specialist | 96 (43.6) | |
| Nutrition | Energy Balance Intake (339) | Excessive Estimated Energy Intake | 239 (70.5) | Adequate Macronutrients | 296 (87.6) |
| Simple Carbohydrate Intake (148) | Excessive Carbohydrate Intake | 74 (50.0) | Adequate Macronutrients | 83 (56.5) | |
| Saturated Lipids Intake (47) | Lipid Type Intake in Disagreement with Needs | 30 (63.8) | Adequate Macronutrients | 17 (36.2) | |
| Sodium Mineral Intake (3) | Excessive Oral Intake | 2 (66.7) | Instruct Knowledge Related to Nutrition | 2 (66.7) | |
| Fibre Intake (240) | Inadequate Fiber Intake | 224 (93.3) | Adequate Macronutrients | 92 (38.8) | |
| Alcohol Consumption (196) | Excessive Alcohol Intake | 194 (99.0) | Guide on Alcohol Consumption | 147 (75.4) | |
| Level of Food Knowledge (289) | Limited Adherence to Nutrition Recommendations | 48 (16.6) | Promote Continued Food and Nutrition Education | 245 (84.8) | |
| Body Weight Condition (596) | Overweight—Obesity | 312 (52.3) | Modify the Distribution, Type, or Amount of Food Nutrients Within Meals or over Time | 469 (78.8) | |
| Altered Triglycerides (268) | Change in Laboratory Values Related to Nutrition | 189 (70.5) | Modify the Distribution, Type, or Amount of Food Nutrients Within Meals or over Time | 227 (85.0) | |
| Dentistry | Oral Hygiene Quality (803) | Adequate Oral Hygiene | 438 (54.5) | Prophylaxis, Topical Application of Fluoride, and Guidance on Correct Oral Hygiene | 420 (52.0) |
| Periodontal Condition (378) | Supragingival Tartar | 223 (59.0) | Supragingival Tartarectomy, Prophylaxis, Topical Application of Fluoride, and Guidance on Brushing Technique and Wire Use | 260 (67.0) | |
| Bruxism (34) | Other Somatoform Disorders Related to Stressful Events—Bruxism | 33 (97.1) | Guide to Specialist | 13 (35.1) | |
| Periodontal Disease (27) | Chronic Periodontitis | 18 (66.7) | Guide to Periodontist Treatment | 17 (60.7) | |
| Caries (84) | Dentin Caries | 50 (59.5) | Guide to Restorative Treatment with External Dentist | 62 (72.9) | |
| Oral Lesion on Soft or Hard Tissue (3) | Leukoplakia and Other Disorders of the Oral Epithelium, Including the Tongue | 1 (33.3) | Guide to Specialist | 2 (66.7) |
| Health Outcomes | ||||||||
|---|---|---|---|---|---|---|---|---|
| Modifiable Health Behaviors | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 |
| Altered Blood Glucose | 0.65 | 0.25 | 0.14 | 0.45 | ||||
| Stress Level and Symptoms | ||||||||
| Altered Blood Pressure | 0.21 | 0.21 | 0.18 | |||||
| Alcohol Consumption | 0.09 | 0.13 | ||||||
| Social Aspects - Leisure | ||||||||
| Self-Care Level | 0.08 | 0.25 | ||||||
| Family Relationships | ||||||||
| Body Weight Conditions | 0.06 | 0.15 | 0.23 | |||||
| Energy Balance Intake | 0.48 | 0.07 | 0.21 | 0.36 | 0.32 | 0.17 | 0.44 | |
| Simple Carbohydrate Intake | 0.16 | 0.25 | 0.33 | |||||
| Saturated Lipids Intake | 0.11 | |||||||
| Sodium Mineral Intake | 0.07 | |||||||
| Fibre Intake | 0.06 | |||||||
| Tobacco Use | ||||||||
| Level of Food Knowledge | 0.46 | 0.11 | 0.25 | 0.28 | 0.18 | 0.31 | ||
| Oral Hygiene Quality | 0.14 | 0.12 | 0.30 | 0.58 | ||||
| Cardiorespiratory Fitness | 0.08 | |||||||
| Contemplation Stage for Physical Activity | 0.31 | 0.09 | ||||||
| Handgrip Strength | 0.15 | |||||||
| Physical Activity Level | 0.29 | 0.10 | ||||||
| Abdominal Strength Level | 0.18 | 0.12 | ||||||
| Feeling of Pain | 0.40 | |||||||
| Flexibility Level | 0.19 | 0.12 | ||||||
| Bruxism | 1.00 | 0.27 | ||||||
| Periodontal Condition | 0.10 | 0.26 | 0.76 | |||||
| Indicators | Multidisciplinary Risk Coefficient | ||||
|---|---|---|---|---|---|
| Physical Education | Nursing | Medicine | Nutrition | Dentistry | |
| Physical Activity Level | −0.57 * | ||||
| Contemplation Stage for Physical Activity Practice | −0.59 * | ||||
| Feeling of Pain | −0.31 * | ||||
| Cardiorespiratory Fitness | −0.32 * | ||||
| Abdominal Strength Level | −0.47 * | ||||
| Flexibility Level | −0.41 * | ||||
| Manual Gripping Force | −0.22* | ||||
| Ergonomic Risks—Physical Aspects | −0.44 * | ||||
| Ergonomic Risks—Organizational Aspects | −0.13 * | ||||
| Work Environment Health Conditions | −0.26 * | ||||
| Family Relationships | −0.16 * | ||||
| Social Aspects—Leisure | −0.03 | ||||
| Self-Care Level | −0.07 * | ||||
| Tobacco Use | −0.52 * | ||||
| Stress Level and Symptoms | −0.22 * | ||||
| Dyslipidemia | −0.39 * | ||||
| Diabetes Mellitus | −0.60 * | ||||
| Systemic Arterial Hypertension | −0.49 * | ||||
| Musculoskeletal Pathology | −0.37 * | ||||
| Psychiatric Pathology | −0.28 | ||||
| Altered Glycemia | −0.25 * | ||||
| Altered Blood Pressure | −0.42 * | ||||
| Energy Balance Intake | −0.37 * | ||||
| Simple Carbohydrate Intake | −0.11 * | ||||
| Saturated Lipids Intake | −0.13 * | ||||
| Sodium Mineral Intake | −0.04 | ||||
| Fibre Intake | −0.25 * | ||||
| Alcohol Consumption | −0.45 * | ||||
| Level of Food Knowledge | −0.18 * | ||||
| Body Weight Condition | −0.47 * | ||||
| Altered Triglycerides | −0.43 * | ||||
| Oral Hygiene Quality | −0.55 * | ||||
| Periodontal Condition | −0.66 * | ||||
| Bruxism | −0.34 * | ||||
| Periodontal Disease | −0.54 * | ||||
| Caries | −0.37 * | ||||
| Oral Lesion on Soft or Hard Tissues | −0.82 * | ||||
| Predictor Dimensions | Step 1 | Step 2 | Step 3 | Step 4 | Step 5 | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| B | t | B | t | B | t | B | t | B | t | |
| Medicine | 0.272 | 22.28 | 0.285 | 24.57 | 0.234 | 26.61 | 0.216 | 30.91 | 0.205 | 35.03 |
| Dentistry | 0.223 | 18.66 | 0.209 | 21.01 | 0.195 | 24.66 | 0.166 | 29.35 | ||
| Physical Education | 0.179 | 20.81 | 0.169 | 24.93 | 0.179 | 29.82 | ||||
| Nutrition | 0.174 | 24.06 | 0.194 | 29.45 | ||||||
| Nursing | 0.168 | 20.76 | ||||||||
| R | 0.58 | 0.72 | 0.82 | 0.89 | 0.93 | |||||
| R2 | 0.34 | 0.52 | 0.67 | 0.79 | 0.86 | |||||
| R2a | 0.34 | 0.51 | 0.66 | 0.79 | 0.86 | |||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Viterbo, L.M.F.; Costa, A.S.; Vidal, D.G.; Dinis, M.A.P. Workers’ Healthcare Assistance Model (WHAM): Development, Validation, and Assessment of Sustainable Return on Investment (S-ROI). Int. J. Environ. Res. Public Health 2020, 17, 3143. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17093143
Viterbo LMF, Costa AS, Vidal DG, Dinis MAP. Workers’ Healthcare Assistance Model (WHAM): Development, Validation, and Assessment of Sustainable Return on Investment (S-ROI). International Journal of Environmental Research and Public Health. 2020; 17(9):3143. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17093143
Chicago/Turabian StyleViterbo, Lilian Monteiro Ferrari, André Santana Costa, Diogo Guedes Vidal, and Maria Alzira Pimenta Dinis. 2020. "Workers’ Healthcare Assistance Model (WHAM): Development, Validation, and Assessment of Sustainable Return on Investment (S-ROI)" International Journal of Environmental Research and Public Health 17, no. 9: 3143. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17093143