The Correlation between Hemoglobin A1c (HbA1c) and Hyperreflective Dots (HRD) in Diabetic Patients


Abstract
:1. Introduction
2. Materials and Methods
2.1. Sampling
2.2. Sample Size Calculation
2.3. Procedure
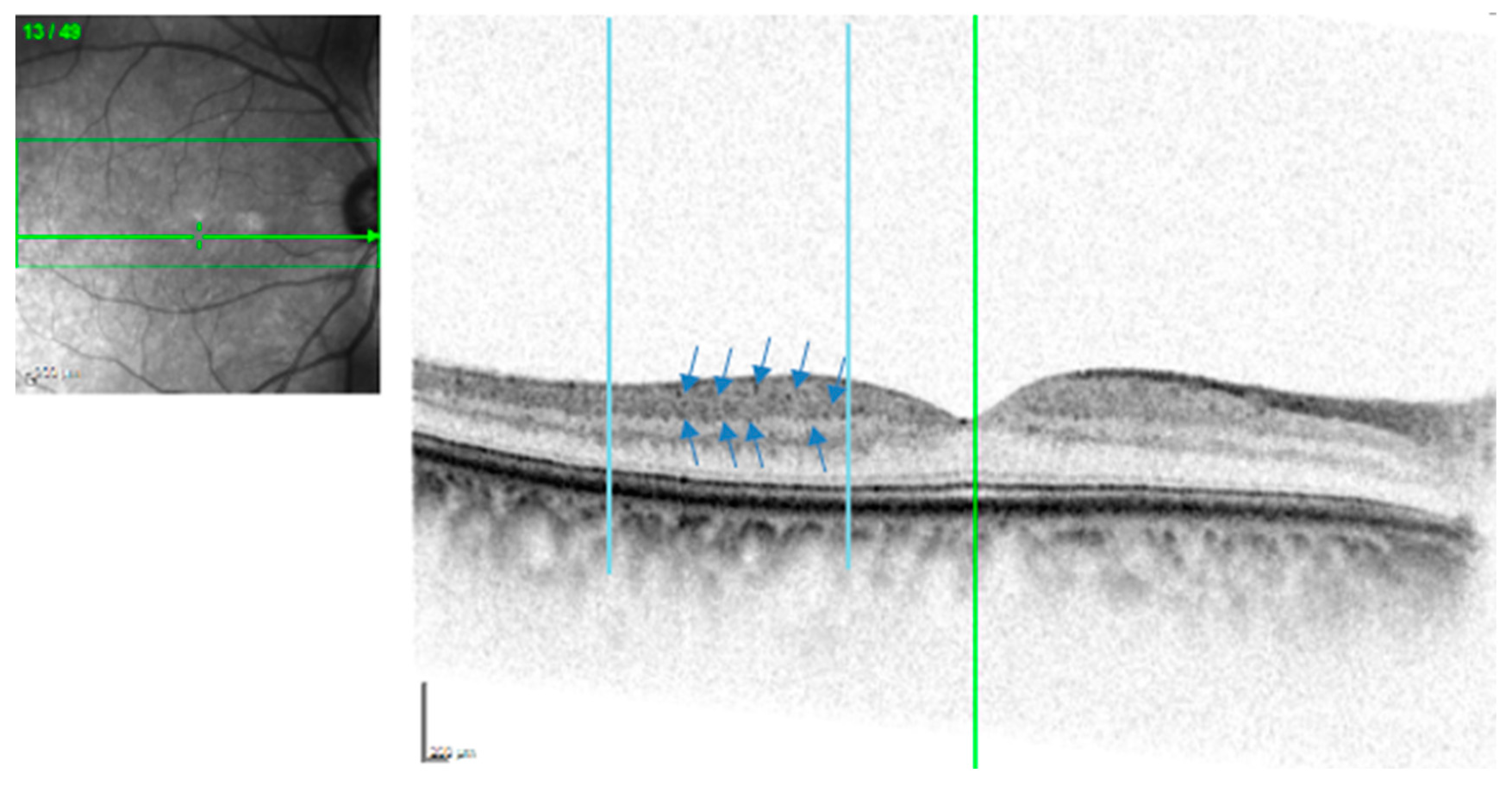
2.4. HRD Image Grading
2.5. HbA1c Levels
2.6. Statistical Analyses
3. Results
3.1. Demographic Data
3.2. Hyper-Reflective Dots (HRD) Count
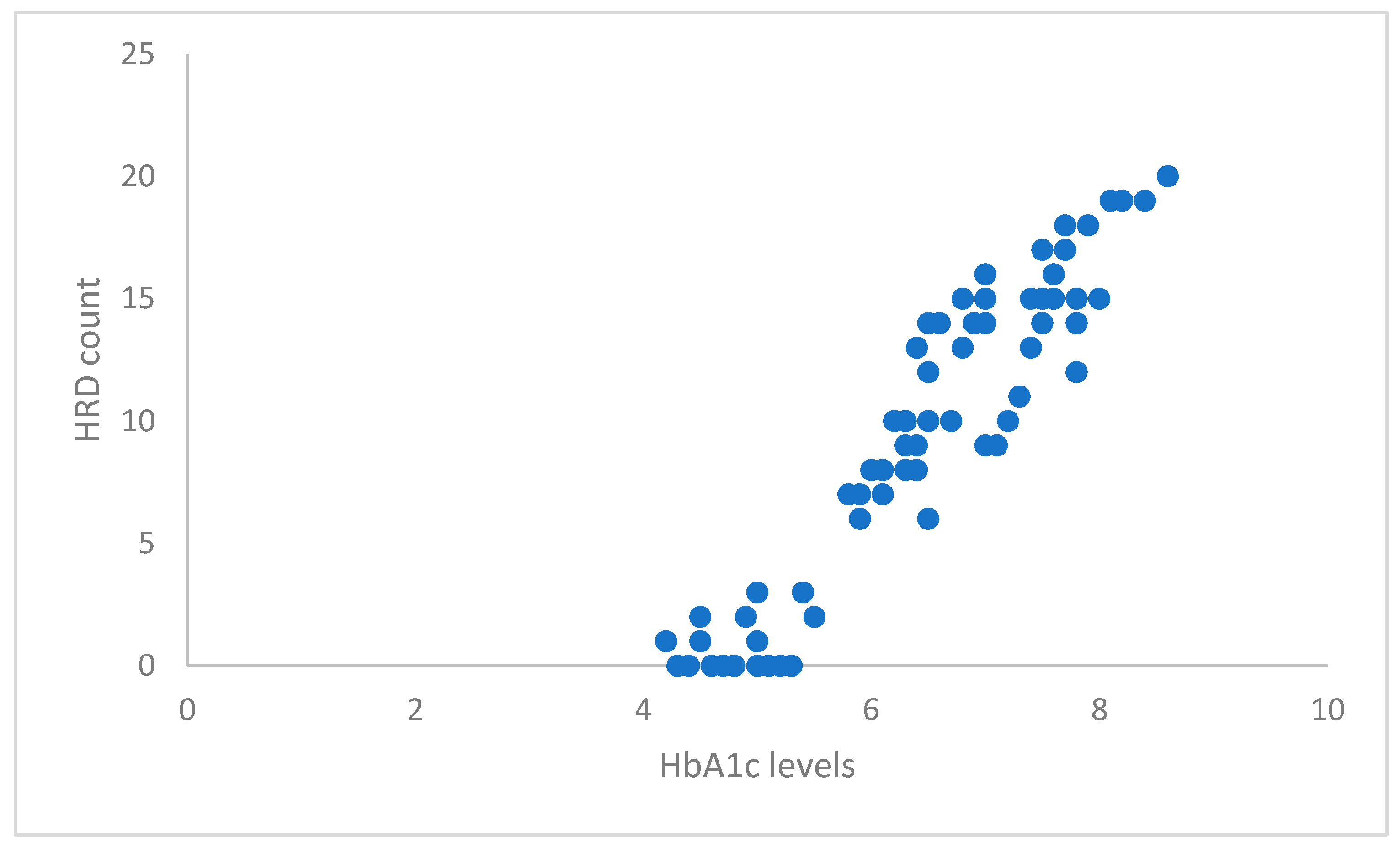
3.3. Correlation between HbA1c Levels and HRD Count
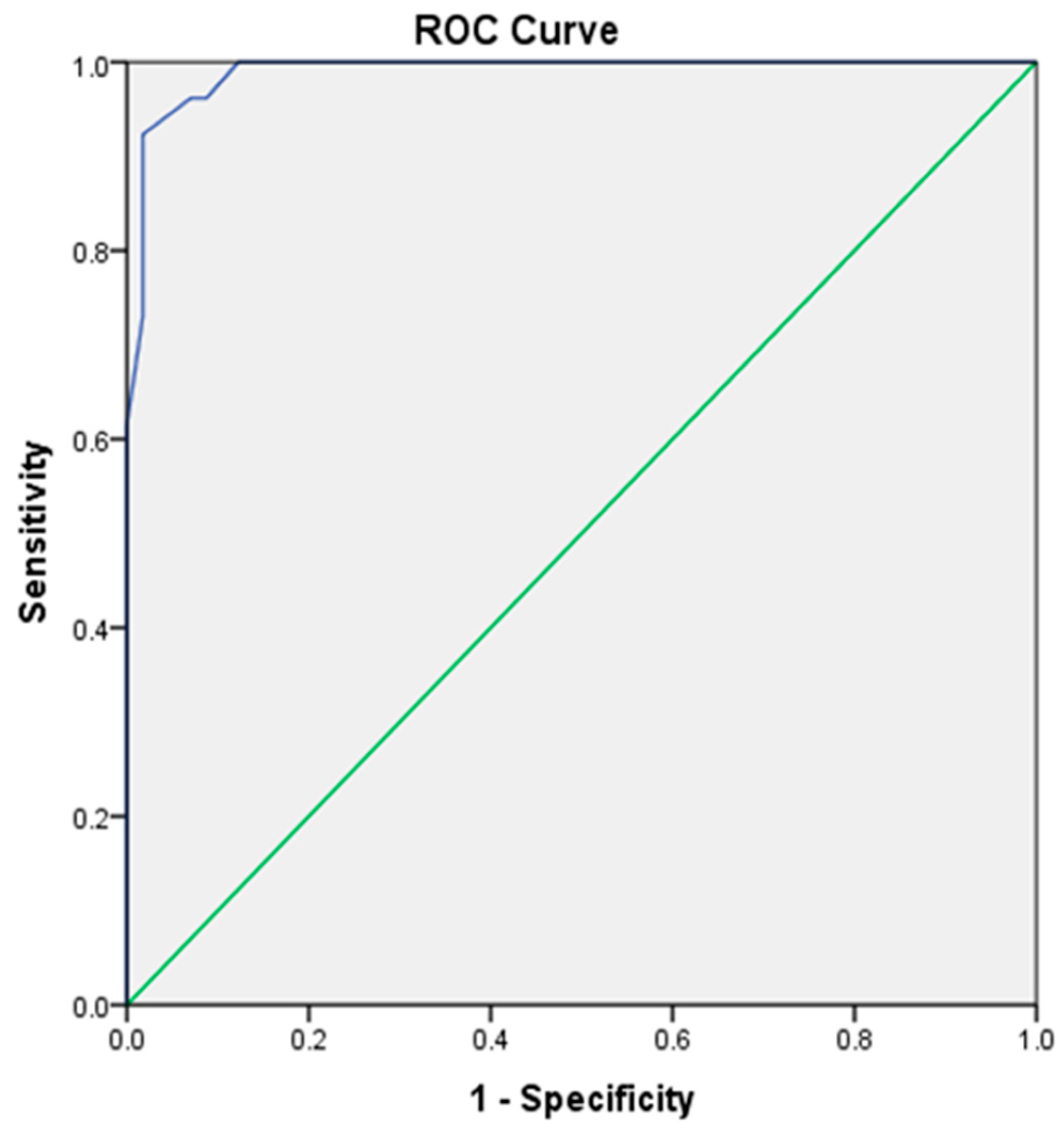
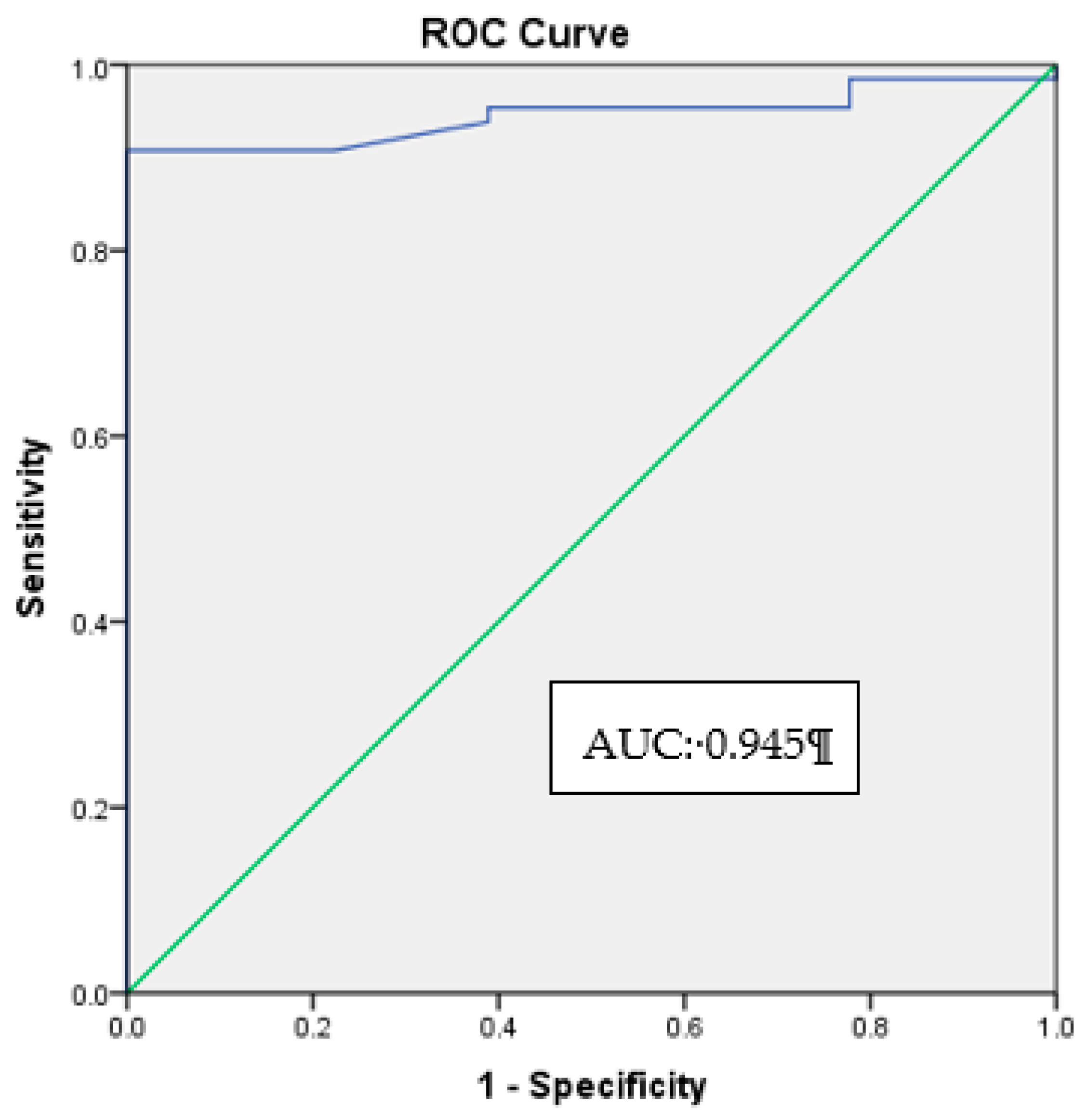
3.4. HbA1c Cut-Off Level for the Appearance of HRD
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Gardner, T.W.; Abcouwer, S.F.; Barber, A.J.; Jackson, G.R. An integrated approach to diabetic retinopathy research. Arch. Ophthalmol. 2011, 129, 230–235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malaguarnera, G.; Gagliano, C.; Bucolo, C.; Vacante, M.; Salomone, S.; Malaguarnera, M.; Leonardi, D.G.; Motta, M.; Drago, F.; Avitabile, T. Lipoprotein(a) serum levels in diabetic patients with retinopathy. Biomed. Res. Int. 2013, 2013, 943505. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El-Asrar, A.M.A. Role of inflammation in the pathogenesis of diabetic retinopathy. Middle East Afr. J. Ophthalmol. 2012, 19, 70–74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rains, J.L.; Jain, S.K. Oxidative stress, insulin signaling, and diabetes. Free Radic. Biol. Med. 2011, 50, 567–575. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malaguarnera, G.; Gagliano, C.; Giordano, M.; Salomone, S.; Vacante, M.; Bucolo, C.; Caraci, F.; Reibaldi, M.; Drago, F.; Avitabile, T.; et al. Homocysteine serum levels in diabetic patients with non proliferative, proliferative and without retinopathy. Biomed. Res. Int. 2014, 2014. [Google Scholar] [CrossRef] [PubMed]
- Dong, N.; Shi, H.; Tang, X. Plasma homocysteine levels are associated with macular thickness in type 2 diabetes without diabetic macular edema. Int. Ophthalmol. 2018, 38, 737–746. [Google Scholar] [CrossRef]
- Brazionis, L.; Rowley, K., Sr.; Itsiopoulos, C.; Harper, C.A.; O’Dea, K. Homocysteine and diabetic retinopathy. Diabetes Care 2008, 31, 50–56. [Google Scholar] [CrossRef] [Green Version]
- Tawfik, A.; Mohamed, R.; Elsherbiny, N.M.; DeAngelis, M.M.; Bartoli, M.; Al-Shabrawey, M. Homocysteine: A potential biomarker for diabetic retinopathy. J. Clin. Med. 2019, 8, 121. [Google Scholar] [CrossRef] [Green Version]
- Xu, C.; Wu, Y.; Liu, G.; Liu, X.; Wang, F.; Yu, J. Relationship between homocysteine level and diabetic retinopathy: A systematic review and meta-analysis. Diagn. Pathol. 2014, 9, 167. [Google Scholar] [CrossRef] [Green Version]
- Ibrahim, A.S.; El-Remessy, A.B.; Matragoon, S.; Zhang, W.; Patel, Y.; Khan, S.; Al-Gasyyar, M.M.; El-Shishtawy, M.M.; Liou, G.I. Retinal microglial activation and inflammation induced by amadori-glycated albumin in a rat model of diabetes. Diabetes 2011, 60, 1122–1133. [Google Scholar] [CrossRef] [Green Version]
- Vujosevic, S.; Bini, S.; Midena, G.; Berton, M.; Pilotto, E.; Midena, E. Hyperreflective intraretinal spots in diabetics without and with nonproliferative diabetic retinopathy: An in vivo study using spectral domain OCT. J. Diabetes Res. 2013, 2013, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Benedetto, U.; Sacconi, R.; Pierro, L.; Lattanzio, R.; Bandello, F. Optical coherence tomographic hyperreflective foci in early stages of diabetic retinopathy. Retina 2015, 35, 449–453. [Google Scholar] [CrossRef] [PubMed]
- Ores, R.; Puche, N.; Querques, G.; Blanco-Garavito, R.; Merle, B.; Coscas, G.; Oubraham, H.; Semoun, O.; Souied, E.H. Gray hyper-reflective subretinal exudative lesions in exudative age-related macular degeneration. Am. J. Ophthalmol. 2014, 158, 354–361. [Google Scholar] [CrossRef] [PubMed]
- Turgut, B.; Yildirim, H. The causes of hyperreflective dots in optical coherence tomography excluding diabetic macular edema and retinal venous occlusions. Open J. Ophthalmol. 2015, 9, 36–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gorst, C.; Kwok, C.S.; Aslam, S.; Buchan, I.; Kontopantelis, E.; Myint, P.K.; Heatlie, G.; Loke, Y.; Rutter, M.K.; Mamas, M.A. Long-term glycemic variability and risk of adverse outcomes: A systematic review and meta-analysis. Diabetes Care 2015, 38, 2354–2369. [Google Scholar] [CrossRef] [Green Version]
- Florkowski, C. HbA1c as a diagnostic test for diabetes mellitus–reviewing the evidence. Clin. Biochem. Rev. 2013, 34, 75–83. [Google Scholar]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G* Power 3: A flexible statistical power analysis program for the social, behavioral and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Automated Bio-Rad D-10 Hemoglobin Testing System Brochure. Available online: https://www.mdkhospital.com/documents/Hemoglobin%20A1c%20D10.pdf (accessed on 4 February 2020).
- Jenchitr, W.; Samaiporn, S.; Lertmeemongkolchai, P.; Chongwiriyanurak, T.; Anujaree, P.; Chayaboon, D.; Pohikamjorn, A. Prevalence of diabetic retinopathy in relation to duration of diabetes mellitus in community hospitals of lampang. J. Med. Assoc. Thai. 2004, 87, 1321–1326. [Google Scholar]
- Tapp, R.J.; Shaw, J.E.; Harper, C.A.; De Courten, M.P.; Balkau, B.; McCarty, D.J.; Taylor, H.R.; Welborn, T.A.; Zimmet, P.Z. The prevalence of and factors associated with diabetic retinopathy in the Australian population. Diabetes Care 2003, 26, 1731–1737. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.; Saaddine, J.B.; Chou, C.F.; Cotch, M.F.; Cheng, Y.J.; Geiss, L.S.; Gregg, E.W.; Albright, A.L.; Klein, B.E.; Klein, R. Prevalence of diabetic retinopathy in the United States, 2005–2008. JAMA 2010, 304, 649–656. [Google Scholar] [CrossRef]
- Lim, M.C.; Lee, S.Y.; Cheng, B.C.; Wong, D.W.; Ong, S.G.; Ang, C.L.; Yeo, I.Y. Diabetic retinopathy in diabetics referred to a tertiary centre from a nationwide screening programme. Ann. Acad. Med. Singap. 2008, 37, 753–759. [Google Scholar] [PubMed]
- Krishnaiah, S.; Das, T.; Nirmalan, P.K.; Shamanna, B.R.; Nutheti, R.; Rao, G.N.; Thomas, R. Risk factors for diabetic retinopathy: Findings from the andhra pradesh eye disease study. Clin. Ophthalmol. 2007, 1, 475–482. [Google Scholar] [PubMed]
- Sabanayagam, C.; Liew, G.; Tai, E.S.; Shankar, A.; Lim, S.C.; Subramaniam, T.; Wong, T.Y. Relationship between glycated haemoglobin and microvascular complications: Is there a natural cut-off point for the diagnosis of diabetes? Diabetologia 2009, 52, 1279–1289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care 2014, 37, S81–S90. [Google Scholar] [CrossRef] [Green Version]
- Peters, A.L.; Davidson, M.B.; Schriger, D.L.; Hasselblad, V. A Clinical approach for the diagnosis of diabetes mellitus: An analysis using glycosylated hemoglobin levels. JAMA 1996, 276, 1246–1252. [Google Scholar] [CrossRef]
- Wong, T.Y.; Liew, G.; Tapp, R.J.; Schmidt, M.I.; Wang, J.J.; Mitchell, P.; Klein, R.; Klein, B.E.; Zimmet, P.; Shaw, J. Relation between fasting glucose and retinopathy for diagnosis of diabetes: Three population-based cross-sectional studies. Lancet 2008, 371, 736–743. [Google Scholar] [CrossRef] [Green Version]
- Tapp, R.J.; Zimmet, P.Z.; Harper, C.A.; de Courten, M.P.; McCarty, D.J.; Balkau, B.; Taylor, H.R.; Welborn, T.A.; Shaw, J.E. Diagnostic thresholds for diabetes: The association of retinopathy and albuminuria with glycaemia. Diabetes Res. Clin. Pract. 2006, 73, 315–321. [Google Scholar] [CrossRef]
- Radin, M.S. Pitfalls in hemoglobin A1c measurement: When results may be misleading. J. Gen. Intern. Med. 2014, 29, 388–394. [Google Scholar] [CrossRef]
- World Health Organisation Consultation. Use of Glycated Haemoglobin (HbA1c) in the Diagnosis of Diabetes Mellitus. 2011. Available online: https://www.who.int/diabetes/publications/report-hba1c_2011.pdf (accessed on 24 June 2018).
- Gallagher, E.J.; Le Roith, D.; Bloomgarden, Z. Review of hemoglobin A1c in the management of diabetes. J. Diabetes 2009, 1, 9–17. [Google Scholar] [CrossRef]
- Coscas, G.; De Benedetto, U.; Coscas, F.; Calzi, C.I.; Vismara, S.; Roudot-Thoraval, F.; Bandello, F.; Souied, E. Hyperreflective dots: A new spectral-domain optical coherence tomography entity for follow-up and prognosis in exudative age-related macular degeneration. Ophthalmologica 2013, 229, 32–37. [Google Scholar] [CrossRef]
- Uji, A.; Murakami, T.; Nishijima, K.; Akagi, T.; Horii, T.; Arakawa, N.; Muraoka, Y.; Ellabban, A.A.; Yoshimura, N. Association between hyperreflective foci in the outer retina, status of photoreceptor layer, and visual acuity in diabetic macular edema. Am. J. Ophthalmol. 2012, 153, 710–717. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grigsby, J.G.; Cardona, S.M.; Pouw, C.E.; Muniz, A.; Mendiola, A.S.; Tsin, A.T.; Allen, D.M.; Cardona, A.E. The role of microglia in diabetic retinopathy. J. Ophthalmol. 2014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Framme, C.; Schweizer, P.; Imesch, M.; Wolf, S.; Wolf-Schnurrbusch, U. Behavior of SD-OCT–detected hyperreflective foci in the retina of anti-VEGF–treated patients with diabetic macular edema. Investig. Ophthalmol. Vis. Sci. 2012, 53, 5814–5818. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tang, J.; Kern, T.S. Inflammation in diabetic retinopathy. Prog. Retin. Eye Res. 2011, 30, 343–358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gustavsson, C.G.; Agardh, C.D. Inflammatory activity increases with haemoglobin A1c in patients with acute coronary syndrome. Scand. Cardiovasc. J. 2009, 43, 380–385. [Google Scholar] [CrossRef] [PubMed]
- Brucklacher, R.M.; Patel, K.M.; VanGuilder, H.D.; Bixler, G.V.; Barber, A.J.; Antonetti, D.A.; Lin, C.M.; LaNoue, K.F.; Gardner, T.W.; Bronson, S.K.; et al. Whole genome assessment of the retinal response to diabetes reveals a progressive neurovascular inflammatory response. BMC Med. Genom. 2008, 1, 26. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Frequency (%) | Mean ± SD Confidence Interval | Normal (n = 25) | Diabetic without Retinopathy (n = 32) | Diabetic with Mild to Moderate NPDR (n = 26) |
|---|---|---|---|---|---|
| Age (years) | Mean ± SD (Range) | 52.40 ± 10.30 | 58.50 ± 6.04 | 58.38 ± 3.35 | |
| 95% Confidence Interval | 48.2–56.7 | 56.3–60.7 | 57.0–59.7 | ||
| Gender | |||||
| Male | 29 (34.9) | 11 | 11 | 7 | |
| Female | 54 (65.1) | 14 | 21 | 19 | |
| Race/ethnicity | |||||
| Malay | 54 (65.1) | 16 | 23 | 15 | |
| Chinese | 12 (14.5) | 6 | 3 | 3 | |
| Indian | 17(20.5) | 3 | 6 | 8 | |
| Other | 0 | 0 | 0 | 0 | |
| Diabetes duration (years) | Mean ± SD (Range) | 6.6 ± 1.6 | 9.0 ± 1.6 | ||
| 95% Confidence Interval | 6.0–7.1 | 8.4–9.6 | |||
| HbA1c level | Mean ± SD (Range) | 4.80 ± 0.34 | 6.43 ± 0.41 | 7.66 ± 0.41 | |
| 95% Confidence Interval | 6.3–6.6 | 7.5–7.8 |
| HbA1c Level | Sensitivity (%) | Specificity (%) |
|---|---|---|
| 6.80 | 100.00 | 87.70 |
| 6.90 | 96.20 | 91.20 |
| 7.00 | 96.20 | 93.00 |
| 7.10 | 92.30 | 98.20 |
| 7.20 | 88.50 | 98.20 |
| Groups | HRD Count (Mean ± SD) | T-Test (Total IR vs. OR) | |||
|---|---|---|---|---|---|
| Inner Retina (IR) | Outer Retina (OR) | Total | t-Value | p-Value | |
| Normal | 0.48 ± 0.87 | 0 | 0.48 ± 0.87 | 12.20 | <0.05 |
| Diabetic without retinopathy | 10.16 ± 3.30 | 0.09 ± 0.39 | 10.25 ± 3.37 | ||
| Mild-to-moderate NPDR | 14.42 ± 3.50 | 0.54 ± 0.90 | 14.96 ± 3.08 | ||
| HbA1c Level (%) | Sensitivity (%) | Specificity (%) |
|---|---|---|
| 4.90 | 95.40 | 61.10 |
| 5.00 | 93.80 | 61.10 |
| 5.10 | 90.80 | 77.80 |
| 5.20 | 90.80 | 83.30 |
| 5.30 | 90.80 | 94.40 |
| 5.40 | 89.20 | 96.60 |
| 5.50 | 87.10 | 96.60 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wong, B.S.; Sharanjeet-Kaur, S.; Ngah, N.F.; Sawri, R.R. The Correlation between Hemoglobin A1c (HbA1c) and Hyperreflective Dots (HRD) in Diabetic Patients. Int. J. Environ. Res. Public Health 2020, 17, 3154. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17093154
Wong BS, Sharanjeet-Kaur S, Ngah NF, Sawri RR. The Correlation between Hemoglobin A1c (HbA1c) and Hyperreflective Dots (HRD) in Diabetic Patients. International Journal of Environmental Research and Public Health. 2020; 17(9):3154. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17093154
Chicago/Turabian StyleWong, Bing Seng, Sharanjeet Sharanjeet-Kaur, Nor Fariza Ngah, and Rajan Rajasudha Sawri. 2020. "The Correlation between Hemoglobin A1c (HbA1c) and Hyperreflective Dots (HRD) in Diabetic Patients" International Journal of Environmental Research and Public Health 17, no. 9: 3154. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17093154