Using an Accelerometer-Based Step Counter in Post-Stroke Patients: Validation of a Low-Cost Tool †

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design of the Study
2.2. Setting
2.3. Device
- Left upper limb on the dorsal side of the wrist;
- Right upper limb on the dorsal side of the wrist;
- Left lower limb on the internal malleolus;
- Right lower limb on the internal malleolus;
- On the waist, medially, on a line connecting the anterior superior iliac spine (ASIS).
2.4. Population
2.5. Inclusion/Exclusion Criteria
2.6. Experimental Procedures
2.7. Data Stratification of Stroke Patients
2.8. Data Analysis
3. Results
Functional Tests Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Mehrholz, J.; Thomas, S.; Werner, C.; Kugler, J.; Pohl, M.; Elsner, B. Electromechanical-assisted training for walking after stroke. Cochrane Database Syst. Rev. 2017, 5, CD006185. [Google Scholar] [PubMed]
- Gor-García-Fogeda, M.D.; Cano de la Cuerda, R.; Carratalá Tejada, M.; Alguacil-Diego, I.M.; Molina-Rueda, F. Observational Gait Assessments in People With Neurological Disorders: A Systematic Review. Arch. Phys. Med. Rehabil. 2016, 97, 131–140. [Google Scholar] [CrossRef] [PubMed]
- Nanninga, C.S.; Meijering, L.; Postema, K.; Schönherr, M.C.; Lettinga, A.T. Unpacking community mobility: A preliminary study into the embodied experiences of stroke survivors. Disabil. Rehabil. 2017, 40, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Fulk, G.D.; Reynolds, C.; Mondal, S.; Deutsch, J.E. Predicting home and community walking activity in people with stroke. Arch. Phys. Med. Rehabil. 2010, 91, 1582–1586. [Google Scholar] [CrossRef]
- Moore, S.A.; Hallsworth, K.; Plötz, T.; Ford, G.A.; Rochester, L.; Trenell, M.I. Physical activity, sedentary behaviour and metabolic control following stroke: A cross-sectional and longitudinal study. PLoS ONE 2013, 8, e55263. [Google Scholar] [CrossRef]
- Moore, S.A.; Hickey, A.; Lord, S.; Del Din, S.; Godfrey, A.; Rochester, L. Comprehensive measurement of stroke gait characteristics with a single accelerometer in the laboratory and community: A feasibility, validity and reliability study. J. Neuroeng. Rehabil. 2017, 14, 130. [Google Scholar] [CrossRef]
- Flansbjer, U.-B.; Holmbäck, A.M.; Downham, D.; Patten, C.; Lexell, J. Reliability of gait performance tests in men and women with hemiparesis after stroke. J. Rehabil. Med. 2005, 37, 75–82. [Google Scholar]
- Salter, K.; Jutai, J.W.; Teasell, R.; Foley, N.C.; Bitensky, J.; Bayley, M. Issues for selection of outcome measures in stroke rehabilitation: ICF Participation. Disabil. Rehabil. 2005, 27, 507–528. [Google Scholar] [CrossRef]
- Danks, K.A.; Roos, M.A.; McCoy, D.; Reisman, D.S. A step activity monitoring program improves real world walking activity post stroke. Disabil. Rehabil. 2014, 36, 2233–2236. [Google Scholar] [CrossRef]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [Green Version]
- Ahmad, S.; Harris, T.; Limb, E.; Kerry, S.; Victor, C.; Ekelund, U.; Iliffe, S.; Whincup, P.; Beighton, C.; Ussher, M.; et al. Evaluation of reliability and validity of the General Practice Physical Activity Questionnaire (GPPAQ) in 60-74 year old primary care patients. BMC Fam. Pract. 2015, 16, 113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Danquah, I.H.; Petersen, C.B.; Skov, S.S.; Tolstrup, J.S. Validation of the NPAQ-short—A brief questionnaire to monitor physical activity and compliance with the WHO recommendations. BMC Public Health 2018, 18, 601. [Google Scholar] [CrossRef] [PubMed]
- Bassett, D.R.; Toth, L.P.; LaMunion, S.R.; Crouter, S.E. Step Counting: A Review of Measurement Considerations and Health-Related Applications. Sports Med. 2017, 47, 1303–1315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lynch, E.A.; Jones, T.M.; Simpson, D.B.; Fini, N.A.; Kuys, S.S.; Borschmann, K.; Kramer, S.; Johnson, L.; Callisaya, M.L.; Mahendran, N.; et al. Activity monitors for increasing physical activity in adult stroke survivors. Cochrane Database Syst. Rev. 2018, 7, CD012543. [Google Scholar] [CrossRef] [PubMed]
- Sprager, S.; Juric, M.B. Inertial Sensor-Based Gait Recognition: A Review. Sensors 2015, 15, 22089–22127. [Google Scholar] [CrossRef]
- Fusca, M.; Negrini, F.; Perego, P.; Magoni, L.; Molteni, F.; Andreoni, G. Validation of a Wearable IMU System for Gait Analysis: Protocol and Application to a New System. Appl. Sci. 2018, 8, 1167. [Google Scholar] [CrossRef] [Green Version]
- O’Brien, M.K.; Shawen, N.; Mummidisetty, C.K.; Kaur, S.; Bo, X.; Poellabauer, C.; Kording, K.; Jayaraman, A. Activity Recognition for Persons With Stroke Using Mobile Phone Technology: Toward Improved Performance in a Home Setting. J. Med. Internet Res. 2017, 19, e184. [Google Scholar] [CrossRef]
- Camomilla, V.; Bergamini, E.; Fantozzi, S.; Vannozzi, G. Trends Supporting the In-Field Use of Wearable Inertial Sensors for Sport Performance Evaluation: A Systematic Review. Sensors 2018, 18, 873. [Google Scholar] [CrossRef] [Green Version]
- Garcia-Byrne, F.; Wycherley, T.P.; Bishop, C.; Schwerdt, S.; Porter, J.; Buckley, J.D. Accelerometer detected lateral sway during a submaximal running test correlates with endurance exercise performance in elite Australian male cricket players. J. Sci. Med. Sport 2019. [CrossRef]
- Stetter, B.J.; Buckeridge, E.; Nigg, S.R.; Sell, S.; Stein, T. Towards a wearable monitoring tool for in-field ice hockey skating performance analysis. Eur. J. Sport Sci. 2019, 19, 893–901. [Google Scholar] [CrossRef]
- Dyrstad, S.M.; Hansen, B.H.; Holme, I.M.; Anderssen, S.A. Comparison of self-reported versus accelerometer-measured physical activity. Med. Sci. Sports Exerc. 2014, 46, 99–106. [Google Scholar] [CrossRef] [PubMed]
- Fortune, E.; Lugade, V.A.; Kaufman, K.R. Posture and movement classification: The comparison of tri-axial accelerometer numbers and anatomical placement. J. Biomech. Eng. 2014, 136, 051003. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zijlstra, W.; Hof, A.L. Assessment of spatio-temporal gait parameters from trunk accelerations during human walking. Gait Posture 2003, 18, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Kamišalić, A.; Fister, I.; Turkanović, M.; Karakatič, S. Sensors and Functionalities of Non-Invasive Wrist-Wearable Devices: A Review. Sensors 2018, 18, 1714. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joseph, C.; Strömbäck, B.; Hagströmer, M.; Conradsson, D. Accelerometry: A feasible method to monitor physical activity during sub-acute rehabilitation of persons with stroke. J. Rehabil. Med. 2018, 50, 429–434. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.; Park, S.; Shin, H. Detection of Hemiplegic Walking Using a Wearable Inertia Sensing Device. Sensors 2018, 18, 1736. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fini, N.A.; Burge, A.T.; Bernhardt, J.; Holland, A.E. Two Days of Measurement Provides Reliable Estimates of Physical Activity Poststroke: An Observational Study. Arch. Phys. Med. Rehabil. 2019, 100, 883–890. [Google Scholar] [CrossRef]
- Bernhard, F.P.; Sartor, J.; Bettecken, K.; Hobert, M.A.; Arnold, C.; Weber, Y.G.; Poli, S.; Margraf, N.G.; Schlenstedt, C.; Hansen, C.; et al. Wearables for gait and balance assessment in the neurological ward—Study design and first results of a prospective cross-sectional feasibility study with 384 inpatients. BMC Neurol. 2018, 18, 114. [Google Scholar] [CrossRef]
- Ancillao, A.; Tedesco, S.; Barton, J.; O’Flynn, B. Indirect Measurement of Ground Reaction Forces and Moments by Means of Wearable Inertial Sensors: A Systematic Review. Sensors 2018, 18, 2564. [Google Scholar] [CrossRef] [Green Version]
- Da-Silva, R.H.; Moore, S.A.; Rodgers, H.; Shaw, L.; Sutcliffe, L.; van Wijck, F.; Price, C.I. Wristband Accelerometers to motiVate arm Exercises after Stroke (WAVES): A pilot randomized controlled trial. Clin. Rehabil. 2019, 33, 1391–1403. [Google Scholar] [CrossRef]
- Valkenet, K.; Bor, P.; van Delft, L.; Veenhof, C. Measuring physical activity levels in hospitalized patients: A comparison between behavioural mapping and data from an accelerometer. Clin. Rehabil. 2019, 33, 1233–1240. [Google Scholar] [CrossRef] [PubMed]
- Thakkar, N.; Jamnik, V.; Ardern, C.I. Cross-associations between physical activity and sedentary time on metabolic health: A comparative assessment using self-reported and objectively measured activity. J. Public Health 2018, 40, e464–e473. [Google Scholar] [CrossRef] [PubMed]
- Kanai, M.; Izawa, K.P.; Kobayashi, M.; Onishi, A.; Kubo, H.; Nozoe, M.; Mase, K.; Shimada, S. Effect of accelerometer-based feedback on physical activity in hospitalized patients with ischemic stroke: A randomized controlled trial. Clin. Rehabil. 2018, 32, 1047–1056. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.-Y.; Kwon, S.; Kim, W.-S.; Hahn, S.J.; Park, J.; Paik, N.-J. Feasibility, reliability, and validity of using accelerometers to measure physical activities of patients with stroke during inpatient rehabilitation. PLoS ONE 2018, 13, e0209607. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shull, P.B.; Jirattigalachote, W.; Hunt, M.A.; Cutkosky, M.R.; Delp, S.L. Quantified self and human movement: A review on the clinical impact of wearable sensing and feedback for gait analysis and intervention. Gait Posture 2014, 40, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Vanroy, C.; Vissers, D.; Cras, P.; Beyne, S.; Feys, H.; Vanlandewijck, Y.; Truijen, S. Physical activity monitoring in stroke: SenseWear Pro2 activity accelerometer versus Yamax Digi-Walker SW-200 pedometer. Disabil. Rehabil. 2014, 36, 1695–1703. [Google Scholar] [CrossRef] [Green Version]
- Gebruers, N.; Vanroy, C.; Truijen, S.; Engelborghs, S.; De Deyn, P.P. Monitoring of physical activity after stroke: A systematic review of accelerometry-based measures. Arch. Phys. Med. Rehabil. 2010, 91, 288–297. [Google Scholar] [CrossRef]
- Klassen, T.D.; Simpson, L.A.; Lim, S.B.; Louie, D.R.; Parappilly, B.; Sakakibara, B.M.; Zbogar, D.; Eng, J.J. “Stepping Up” Activity Poststroke: Ankle-Positioned Accelerometer Can Accurately Record Steps During Slow Walking. Phys. Ther. 2016, 96, 355–360. [Google Scholar] [CrossRef] [Green Version]
- Beyaert, C.; Vasa, R.; Frykberg, G.E. Gait post-stroke: Pathophysiology and rehabilitation strategies. Neurophysiol. Clin. Clin. Neurophysiol. 2015, 45, 335–355. [Google Scholar] [CrossRef]
- O’Brien, M.K.; Hidalgo-Araya, M.D.; Mummidisetty, C.K.; Vallery, H.; Ghaffari, R.; Rogers, J.A.; Lieber, R.; Jayaraman, A. Augmenting Clinical Outcome Measures of Gait and Balance with a Single Inertial Sensor in Age-Ranged Healthy Adults. Sensors 2019, 19, 4537. [Google Scholar] [CrossRef] [Green Version]
- Job, M.; Dottor, A.; Viceconti, A.; Testa, M. Ecological Gait as a Fall Indicator in Older Adults: A Systematic Review. Gerontologist 2019. [Google Scholar] [CrossRef] [PubMed]
- Trojaniello, D.; Ravaschio, A.; Hausdorff, J.M.; Cereatti, A. Comparative assessment of different methods for the estimation of gait temporal parameters using a single inertial sensor: Application to elderly, post-stroke, Parkinson’s disease and Huntington’s disease subjects. Gait Posture 2015, 42, 310–316. [Google Scholar] [CrossRef] [PubMed]
- Hui, J.; Heyden, R.; Bao, T.; Accettone, N.; McBay, C.; Richardson, J.; Tang, A. Validity of the Fitbit One for Measuring Activity in Community-Dwelling Stroke Survivors. Physiother. Can. 2018, 70, 81–89. [Google Scholar] [CrossRef] [PubMed]
- Salvo, D.; Torres, C.; Villa, U.; Rivera, J.A.; Sarmiento, O.L.; Reis, R.S.; Pratt, M. Accelerometer-based physical activity levels among Mexican adults and their relation with sociodemographic characteristics and BMI: A cross-sectional study. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 79. [Google Scholar] [CrossRef] [Green Version]
- Joseph, C.; Conradsson, D.; Hagströmer, M.; Lawal, I.; Rhoda, A. Objectively assessed physical activity and associated factors of sedentary behavior among survivors of stroke living in Cape Town, South Africa. Disabil. Rehabil. 2018, 40, 2509–2515. [Google Scholar] [CrossRef]
- Ouyang, F.; Wang, Y.; Huang, W.; Chen, Y.; Zhao, Y.; Dang, G.; Zhang, C.; Lin, Y.; Zeng, J. Association between socioeconomic status and post-stroke functional outcome in deprived rural southern China: A population-based study. BMC Neurol. 2018, 18, 12. [Google Scholar] [CrossRef]
- De Ridder, R.; De Blaiser, C. Activity trackers are not valid for step count registration when walking with crutches. Gait Posture 2019, 70, 30–32. [Google Scholar] [CrossRef]
- Jayaraman, C.; Mummidisetty, C.K.; Mannix-Slobig, A.; McGee Koch, L.; Jayaraman, A. Variables influencing wearable sensor outcome estimates in individuals with stroke and incomplete spinal cord injury: A pilot investigation validating two research grade sensors. J. Neuroeng. Rehabil. 2018, 15, 19. [Google Scholar] [CrossRef]
- Lee, J.A.; Laurson, K.R. Validity of the SenseWear armband step count measure during controlled and free-living conditions. J. Exerc. Sci. Fit. 2015, 13, 16–23. [Google Scholar] [CrossRef] [Green Version]
- Perera, S.; Mody, S.H.; Woodman, R.C.; Studenski, S.A. Meaningful change and responsiveness in common physical performance measures in older adults. J. Am. Geriatr. Soc. 2006, 54, 743–749. [Google Scholar] [CrossRef]
- Hachiya, M.; Murata, S.; Otao, H.; Kamijou, K.; Mizota, K.; Asami, T. Reproducibility and validity of the 50-meter walking test in community-dwelling elderly. J. Phys. Ther. Sci. 2015, 27, 1511–1514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van der Krogt, M.M.; Delp, S.L.; Schwartz, M.H. How robust is human gait to muscle weakness? Gait Posture 2012, 36, 113–119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perry, J.; Garrett, M.; Gronley, J.K.; Mulroy, S.J. Classification of walking handicap in the stroke population. Stroke 1995, 26, 982–989. [Google Scholar] [CrossRef] [PubMed]
- Fulk, G.D.; Combs, S.A.; Danks, K.A.; Nirider, C.D.; Raja, B.; Reisman, D.S. Accuracy of 2 activity monitors in detecting steps in people with stroke and traumatic brain injury. Phys. Ther. 2014, 94, 222–229. [Google Scholar] [CrossRef] [Green Version]
- Carroll, S.L.; Greig, C.A.; Lewis, S.J.; McMurdo, M.E.; Sniehotta, F.F.; Johnston, M.; Johnston, D.W.; Scopes, J.; Mead, G.E. The use of pedometers in stroke survivors: Are they feasible and how well do they detect steps? Arch. Phys. Med. Rehabil. 2012, 93, 466–470. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [Green Version]
- Clay, L.; Webb, M.; Hargest, C.; Adhia, D.B. Gait quality and velocity influences activity tracker accuracy in individuals post-stroke. Top. Stroke Rehabil. 2019, 26, 412–417. [Google Scholar] [CrossRef]
- Schaffer, S.D.; Holzapfel, S.D.; Fulk, G.; Bosch, P.R. Step count accuracy and reliability of two activity tracking devices in people after stroke. Physiother. Theory Pract. 2017, 33, 788–796. [Google Scholar] [CrossRef]
- Campos, C.; DePaul, V.G.; Knorr, S.; Wong, J.S.; Mansfield, A.; Patterson, K.K. Validity of the ActiGraph activity monitor for individuals who walk slowly post-stroke. Top. Stroke Rehabil. 2018, 25, 295–304. [Google Scholar] [CrossRef]
- Van Criekinge, T.; Saeys, W.; Hallemans, A.; Velghe, S.; Viskens, P.-J.; Vereeck, L.; De Hertogh, W.; Truijen, S. Trunk biomechanics during hemiplegic gait after stroke: A systematic review. Gait Posture 2017, 54, 133–143. [Google Scholar] [CrossRef]
- Masse, F.; Gonzenbach, R.; Paraschiv-Ionescu, A.; Luft, A.R.; Aminian, K. Wearable Barometric Pressure Sensor to Improve Postural Transition Recognition of Mobility-Impaired Stroke Patients. IEEE Trans. Neural Syst. Rehabil. Eng. Publ. IEEE Eng. Med. Biol. Soc. 2016, 24, 1210–1217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shumway-Cook, A.; Patla, A.E.; Stewart, A.; Ferrucci, L.; Ciol, M.A.; Guralnik, J.M. Environmental demands associated with community mobility in older adults with and without mobility disabilities. Phys. Ther. 2002, 82, 670–681. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lord, S.E.; Rochester, L. Measurement of community ambulation after stroke: Current status and future developments. Stroke 2005, 36, 1457–1461. [Google Scholar] [CrossRef] [PubMed]
- Bergmann, J.H.M.; McGregor, A.H. Body-worn sensor design: What do patients and clinicians want? Ann. Biomed. Eng. 2011, 39, 2299–2312. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Sex (n) | Age (Years) | Comfortable Walking Speed (m/s) | Walking Aids (n) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Subgroup | Males | Females | n | Mean | DS | Min | Max | Mean | DS | Min | Max | None | Cane | Walker |
| V1 | 10 | 2 | 12 | 61.08 | 20.13 | 27 | 84 | 0.36 | 0.14 | 0.13 | 0.56 | 1 | 8 | 3 |
| V2 | 5 | 9 | 14 | 58.5 | 14.87 | 23 | 81 | 0.67 | 0.02 | 0.64 | 0.7 | 8 | 5 | 1 |
| V3 | 12 | 5 | 17 | 63.65 | 9.75 | 40 | 77 | 1.08 | 3.37 | 0.86 | 1.35 | 14 | 0 | 3 |
| A1 | 14 | 9 | 23 | 58.61 | 15.36 | 23 | 77 | 0.96 | 0.26 | 0.42 | 1.35 | |||
| A2 | 9 | 4 | 13 | 59.92 | 14.26 | 27 | 81 | 0.48 | 0.18 | 0.18 | 0.69 | |||
| A3 | 4 | 3 | 7 | 72.43 | 10.85 | 55 | 84 | 0.63 | 0.31 | 0.13 | 0.97 | |||
| 10 m Walking Test—Healthy Subjects | |||||
|---|---|---|---|---|---|
| Measures | Right | Left | |||
| Ankle | Arm | Ankle | Arm | Waist | |
| Mean Manual Count (steps ± SD) | 14.60 ± 1.65 | ||||
| Mean Step Counter (steps ± SD) | 15.30 ± 1.89 | 13.30 ± 2.71 | 14.60 ± 2.17 | 15.30 ± 6.83 | 15.00 ± 1.41 |
| MAPE (% ± SD) | 4.75 ± 4.44 | 12.78 ± 14.15 | 6.31 ± 10.04 | 19.39 ± 30.6 | 4.52 ± 5.55 |
| ICC (95%CI) | 0.92 (0.73–0.98) | 0.33 (−0.33 to 0.78) | 0.46 (−0.19 to 0.83) | 0.24 (−0.42 to 0.73) | 0.84 (0.50 to 0.96) |
| 50 m Walking Test—Healthy Subjects | |||||
| Mean Manual Count (steps ± SD) | 69.30 ± 6.34 | ||||
| Mean Step Counter (steps ± SD) | 70.20 ± 6.49 | 57.60 ± 14.22 | 70.00 ± 6.24 | 57.60 ± 12.48 | 66.50 ± 6.34 |
| MAPE (% ± SD) | 1.63 ± 1.54 | 17.49 ± 18.43 | 1.03 ± 0.97 | 17.0 ± 15.85 | 6.32 ±16.51 |
| ICC (95%CI) | 0.98 (0.93 to 0.99) | 0.25 (−0.40 to 0.74) | 0.99 (0.98 to 0.99) | 0.38 (−0.28 to 0.80) | 0.54 (−0.08 to 0.86) |
| 6 min Walking Test—Healthy Subjects | |||||
| Mean Manual Count (steps ± SD) | 689.60 ± 52.42 | ||||
| Mean Step Counter (steps ± SD) | 695.20 ± 54.08 | 572.70 ± 99.08 | 694.00 ± 50.73 | 534.00 ± 120.42 | 690.60 ± 51.62 |
| MAPE (% ± SD) | 1.02 ± 0.83 | 16.7 ± 14.9 | 0.66 ± 0.88 | 22.47 ± 17.81 | 1.64 ± 3.14 |
| ICC (95%CI) | 0.99 (0.96 to 0.99) | 0.06 (−0.55 to 0.64) | 0.99 (0.97 to 0.99) | 0.05 (−0.57 to 0.63) | 0.92 (0.70 to 0.98) |
| Timed Up and Go Test—Healthy Subjects | |||||
| Mean Manual Count (steps ± SD) | 9.60 ± 1.17 | ||||
| Mean Step Counter (steps ± SD) | 10.20 ± 3.9 | 12.10 ± 1.68 | 11.50 ± 1.72 | 12.60 ± 1.90 | 11.30 ± 0.67 |
| MAPE (% ± SD) | 26.08 ± 30.59 | 31.33 ± 16.12 | 22.56 ± 14.01 | 33.86 ± 16.49 | 18.81 ± 11.55 |
| ICC (95%CI) | 0.21 (−0.45 to 0.72) | –0.03 (−0.62 to 0.58) | 0.36 (−0.31 to 0.79) | 0.24 (−0.42 to 0.74) | 0.51 (−0.13 to 0.85) |
| 10 m Walking Test—Pathological Subjects. | |||||
|---|---|---|---|---|---|
| Measures | Healthy | Pathological | |||
| Ankle | Arm | Ankle | Arm | Waist | |
| Mean Manual Count (steps ± SD) | 25.38 ± 9.55 | ||||
| Mean Step Counter (steps ± SD) | 16.93 ± 9.70 | 11.32 ± 9.58 | 18.44 ± 9.17 | 15.07 ± 8.57 | 13.23 ± 9.25 |
| MAPE (% ± SD) | 30.97 ± 38.14 | 48.56 ± 43.12 | 29.62 ± 35.37 | 39.98 ± 37.25 | 45.08 ± 43.15 |
| ICC (95%CI) | −0.19 (−0.46 to 0.11) | −0.41 (−0.63 to 0.13) | −0.20 (−0.47 to 0.10) | −0.50 (−0.34 to 0.26) | −0.42 (−0.64 to 0.14) |
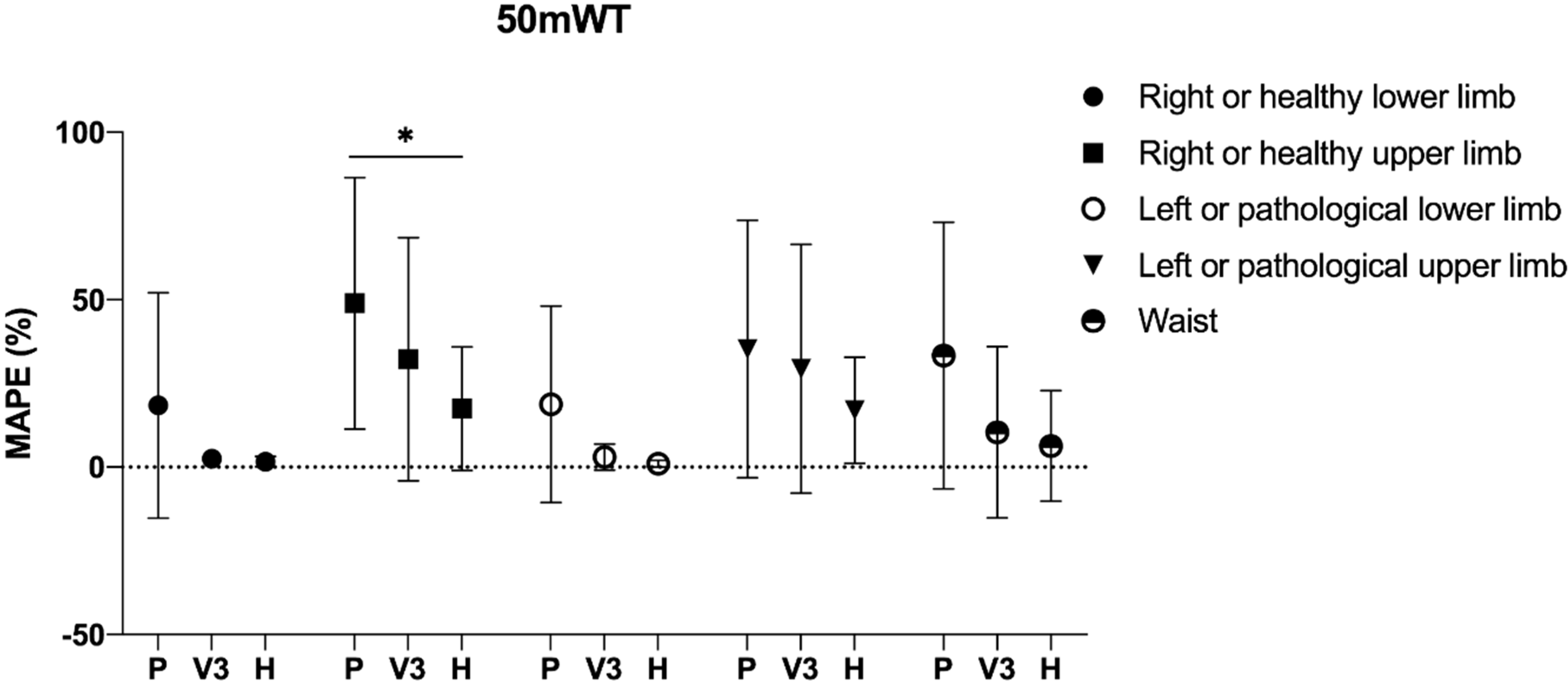
| 50 m Walking Test—Pathological Subjects | |||||
| Mean Manual Count (steps ± SD) | 110.91 ± 44.23 | ||||
| Mean Step Counter (steps ± SD) | 88.95 ± 48.29 | 52.44 ± 35.07 | 90.30 ± 39.34 | 69.39 ± 43.88 | 66.83 ± 34.20 |
| MAPE (% ± SD) | 18.45 ± 33.68 | 48.96 ± 37.53 | 18.74 ± 29.34 | 35.26 ± 38.44 | 33.30 ± 39.81 |
| ICC (95%CI) | 0.37 (0.08 to 0.60) | −0.32 (−0.57 to 0.02) | 0.06 (−0.24 to 0.36) | 0.07 (−0.24 to 0.36) | −0.40 (−0.61 to 0.10) |
| 6 min Walking Test—Pathological Subjects | |||||
| Mean Manual Count (steps ± SD) | 536.76 ± 113.29 | ||||
| Mean Step Counter (steps ± SD) | 485.76 ± 213.60 | 309.36 ± 226.62 | 497.24 ± 218.63 | 383.61 ± 229.09 | 418.88 ± 239.06 |
| MAPE (% ± SD) | 17.13 ± 31.72 | 48.31 ± 38.51 | 20.61 ± 29.65 | 36.60 ± 37.88 | 31.14 ± 39.22 |
| ICC (95%CI) | 0.69 (0.50 to 0.82) | 0.45 (0.17 to 0.66) | 0.70 (0.51 to 0.83) | 0.45 (0.17 to 0.66) | 0.57 (0.33 to 0.74) |
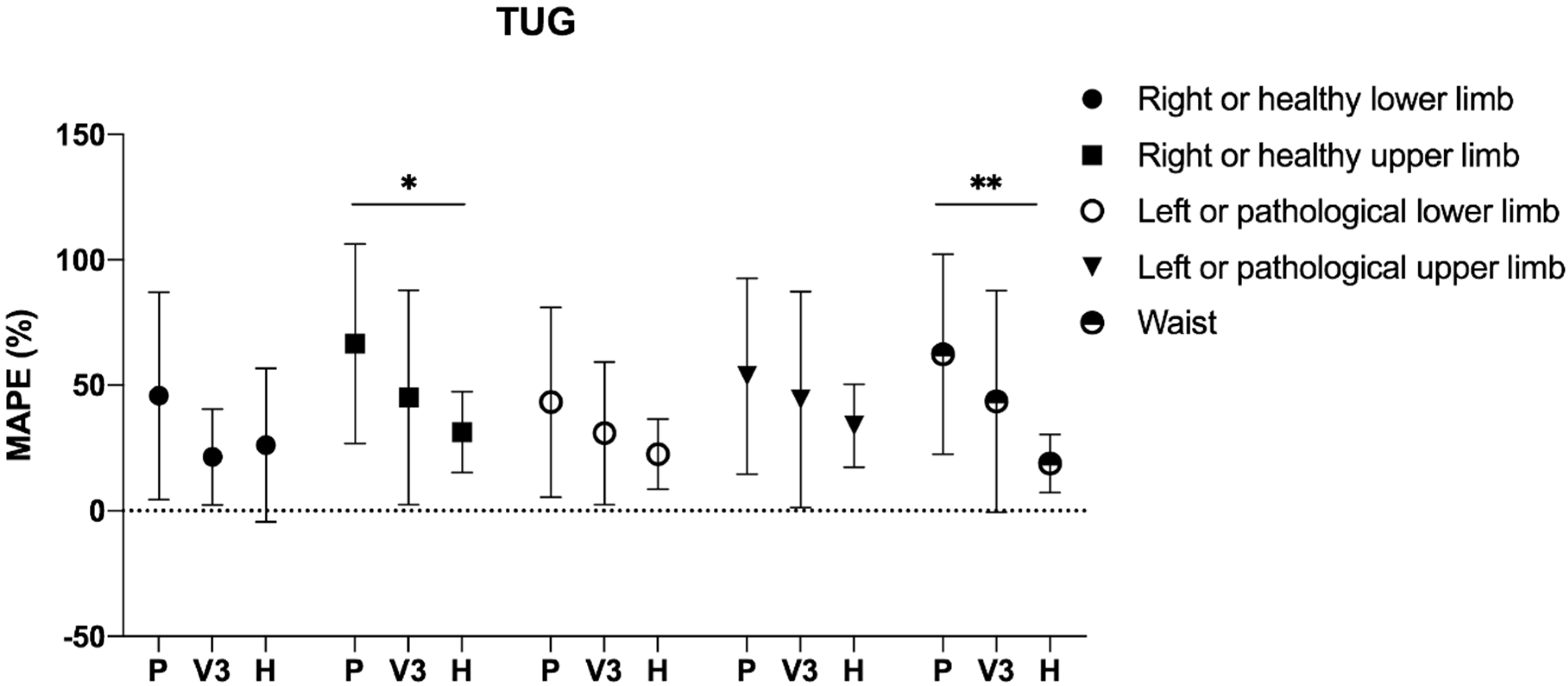
| Timed Up and Go Test—Pathological Subjects | |||||
| Mean Manual Count (steps ± SD) | 20.38 ± 11.24 | ||||
| Mean Step Counter (steps ± SD) | 12.44 ± 9.85 | 6.93 ± 8.37 | 12.58 ± 9.42 | 10.61 ± 9.79 | 7.02 ± 7.01 |
| MAPE (% ± SD) | 45.40 ± 41.04 | 67.81 ± 39.95 | 42.93 ± 37.15 | 54.53 ± 39.68 | 63.79 ± 40.13 |
| ICC (95%CI) | −0.28 (−0.54 to 0.01) | −0.23 (−0.49 to 0.08) | 0.05 (−0.25 to 0.34) | −0.17 (−0.44 to 0.14) | −0.26 (−0.52 to 0.04) |
| 10 m Walking Test—Group V3 | |||||
|---|---|---|---|---|---|
| Measures | Healthy | Pathological | |||
| Ankle | Arm | Ankle | Arm | Waist | |
| Mean Manual Count (steps ± SD) | 19.00 ± 3.79 | ||||
| Mean Step Counter (steps ± SD) | 18.94 ± 3.51 | 11.18 ± 7.63 | 19.59 ± 2.74 | 13.65 ± 7.08 | 15.94 ± 5.17 |
| MAPE (% ± SD) | 10.05 ± 10.00 | 37.22 ± 43.11 | 11.96 ± 15.51 | 31.23 ± 35.66 | 20.47 ± 33.89 |
| ICC (95%CI) | 0.92 (0.73 to 0.98) | 0.33 (−0.33 to 0.78) | 0.46 (−0.19 to 0.83) | 0.24 (−0.42 to 0.73) | 0.84 (0.50 to 0.96) |
| 50 m Walking Test—Group V3 | |||||
| Mean Manual Count (steps ± SD) | 83.63 ± 21.59 | ||||
| Mean Step Counter (steps ± SD) | 84.44 ± 20.71 | 54.19 ± 31.45 | 84.56 ± 23.12 | 57.06 ± 34.36 | 74.56 ± 18.90 |
| MAPE (% ± SD) | 2.52 ± 2.41 | 32.19 ± 36.29 | 3.00 ± 3.85 | 29.34 ± 37.15 | 10.39 ± 25.58 |
| ICC (95%CI) | 0.98 (0.93 to 0.99) | 0.25 (−0.40 to 0.74) | 0.99 (0.98 to 0.99) | 0.38 (−0.28 to 0.80) | 0.54 (−0.08 to 0.86) |
| 6 min Walking Test—Group V3 | |||||
| Mean Manual Count (steps ± SD) | 636.35 ± | ||||
| Mean Step Counter (steps ± SD) | 646.24 ± | 409.53 ± | 642.82 ± | 448.82 ± | 591.76 ± |
| MAPE (% ± SD) | 1.79 ± 29.58 | 35.63 ± 37.05 | 3.31 ± 29.77 | 30.06 ± 35.68 | 8.71 ± 37.92 |
| ICC (95%CI) | 0.99 (0.96 to 0.99) | 0.06 (−0.55 to 0.64) | 0.99 (0.97 to 0.99) | 0.05 (−0.57 to 0.63) | 0.92 (0.70 to 0.98) |
| Timed Up and Go Test—Group V3 | |||||
| Mean Manual Count (steps ± SD) | 14.94 ± 3.16 | ||||
| Mean Step Counter (steps ± SD) | 16.88 ± 3.59 | 9.18 ± 7.02 | 14.00 ± 6.74 | 9.53 ± 7.51 | 9.18 ± 6.96 |
| MAPE (% ± SD) | 21.46 ± 19.08 | 45.18 ± 42.67 | 30.90 ± 28.41 | 44.28 ± 42.98 | 43.55 ± 44.09 |
| ICC (95%CI) | 0.21 (−0.45 to 0.72) | −0.03 (−0.62 to 0.58) | 0.36 (−0.31 to 0.79) | 0.24 (−0.42 to 0.74) | 0.51 (−0.13 to 0.85) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Negrini, F.; Gasperini, G.; Guanziroli, E.; Vitale, J.A.; Banfi, G.; Molteni, F. Using an Accelerometer-Based Step Counter in Post-Stroke Patients: Validation of a Low-Cost Tool. Int. J. Environ. Res. Public Health 2020, 17, 3177. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17093177
Negrini F, Gasperini G, Guanziroli E, Vitale JA, Banfi G, Molteni F. Using an Accelerometer-Based Step Counter in Post-Stroke Patients: Validation of a Low-Cost Tool. International Journal of Environmental Research and Public Health. 2020; 17(9):3177. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17093177
Chicago/Turabian StyleNegrini, Francesco, Giulio Gasperini, Eleonora Guanziroli, Jacopo Antonino Vitale, Giuseppe Banfi, and Franco Molteni. 2020. "Using an Accelerometer-Based Step Counter in Post-Stroke Patients: Validation of a Low-Cost Tool" International Journal of Environmental Research and Public Health 17, no. 9: 3177. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17093177