A Qualitative Study to Explore Perception of Impacts of Preemption of Tobacco Regulation on Counties in Appalachian Tennessee

 ,
,
Abstract
:1. Introduction
2. Methods
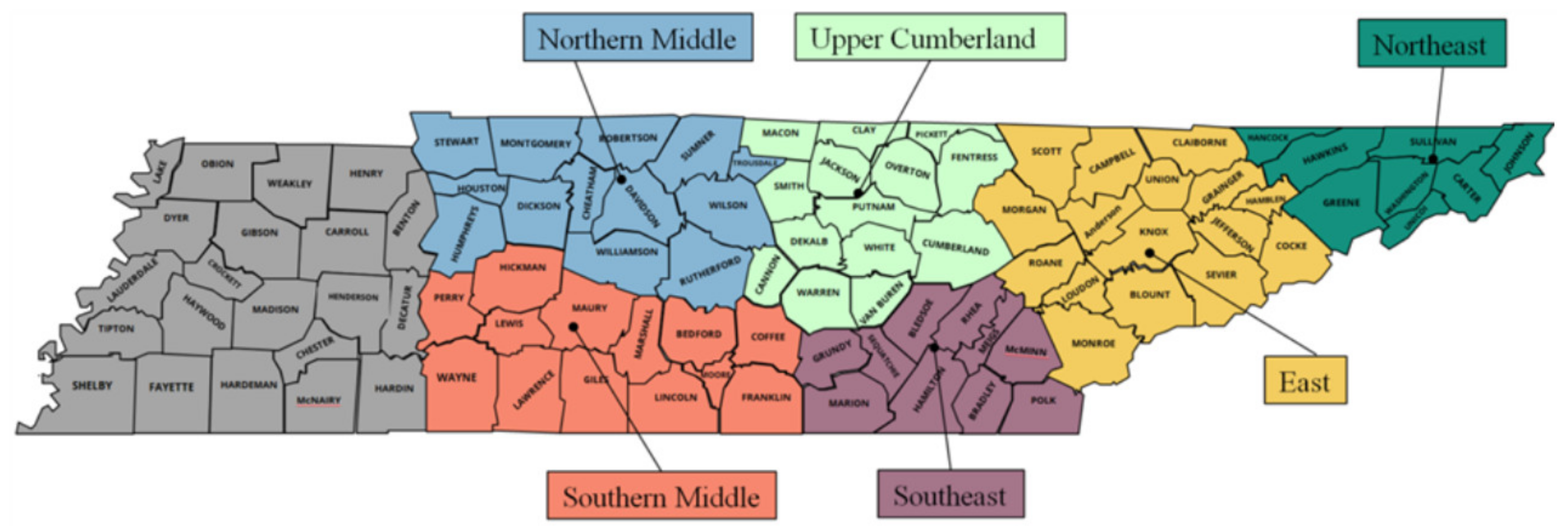
2.1. Participants
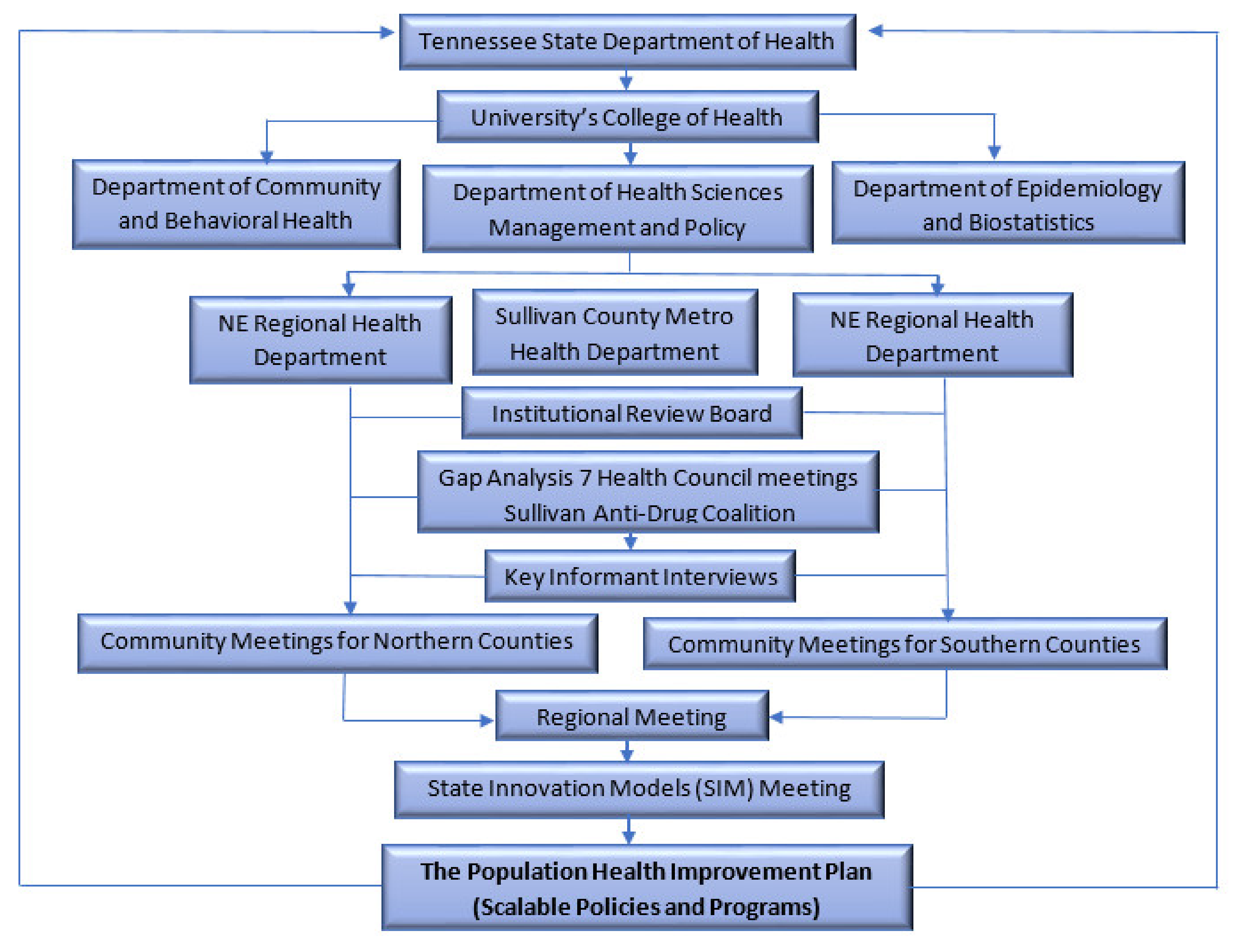
2.2. PHIP Process
2.3. Data Collection and Analysis
3. Results
3.1. Cultural and Normative Factors in Appalachian Tennessee
“The cultural history of tobacco in this area. That makes a big difference. When you’re growing and selling tobacco, that was your livelihood, that makes it a lot different then and that’s understandable. That’s cultural, yes” (Stakeholder, Northern County).
“It’s widely accepted. It’s what you do. It’s part of the culture. That smokeless tobacco is out of control here. It’s grandparents to fathers to grandchildren, great-grandchildren. It’s definitely a cyclical thing and that’s what these kids are learning and stick that little piece of dip and let it sit there and park. It’s amazing, especially how young they’re using the smokeless tobacco. That was the number one tobacco product that our fourth and fifth graders were using, or had tried already, starting at age nine, 10 or 11. It’s here. It’s accepted” (Stakeholder, Northern County).
“Another thing I’ve seen too, culturally, and I know we’re talking about unique populations but, culturally, I have talked to people since I’ve gotten here who were raised on tobacco farms and, as children, their parents would rub tobacco leaves on their skin so they could get nicotine into a child’s body so they could acclimate to touching the tobacco as they worked it, to not get sick. Then by the time they were 10 or 12, the parents encouraged the child to start smoking so they could still handle and work the tobacco. I’ve heard this more than once” (Stakeholder, Northern County).
3.2. The Burden of Tobacco Use in Appalachian Tennessee, Compared to Tennessee and the United States
”Smoking [in Northeast or Appalachian Tennessee] is a huge problem in [name of] County” (Stakeholder, Northern County).
“It’s been a hard issue to tackle [tobacco use] here in [name of] County” (Stakeholder, Southern County).
“I’ve never done a presentation at a church that someone wasn’t related to some type of tobacco related illness or affected by that” (Stakeholder, Southern County).
“I thought that [five years of age] would be a good time to do some of the preventing youth initiation of smoking. It’s grades five through eight. It’s just one school right now” (Stakeholder, Northern County).
“…but I think for us, it’s seen as people know that kids shouldn’t be smoking, but yet parents will still provide, teachers still allow kids to dip in class. I’m not sure that enforcement is happening in our community like it should” (Stakeholder, Northern County).
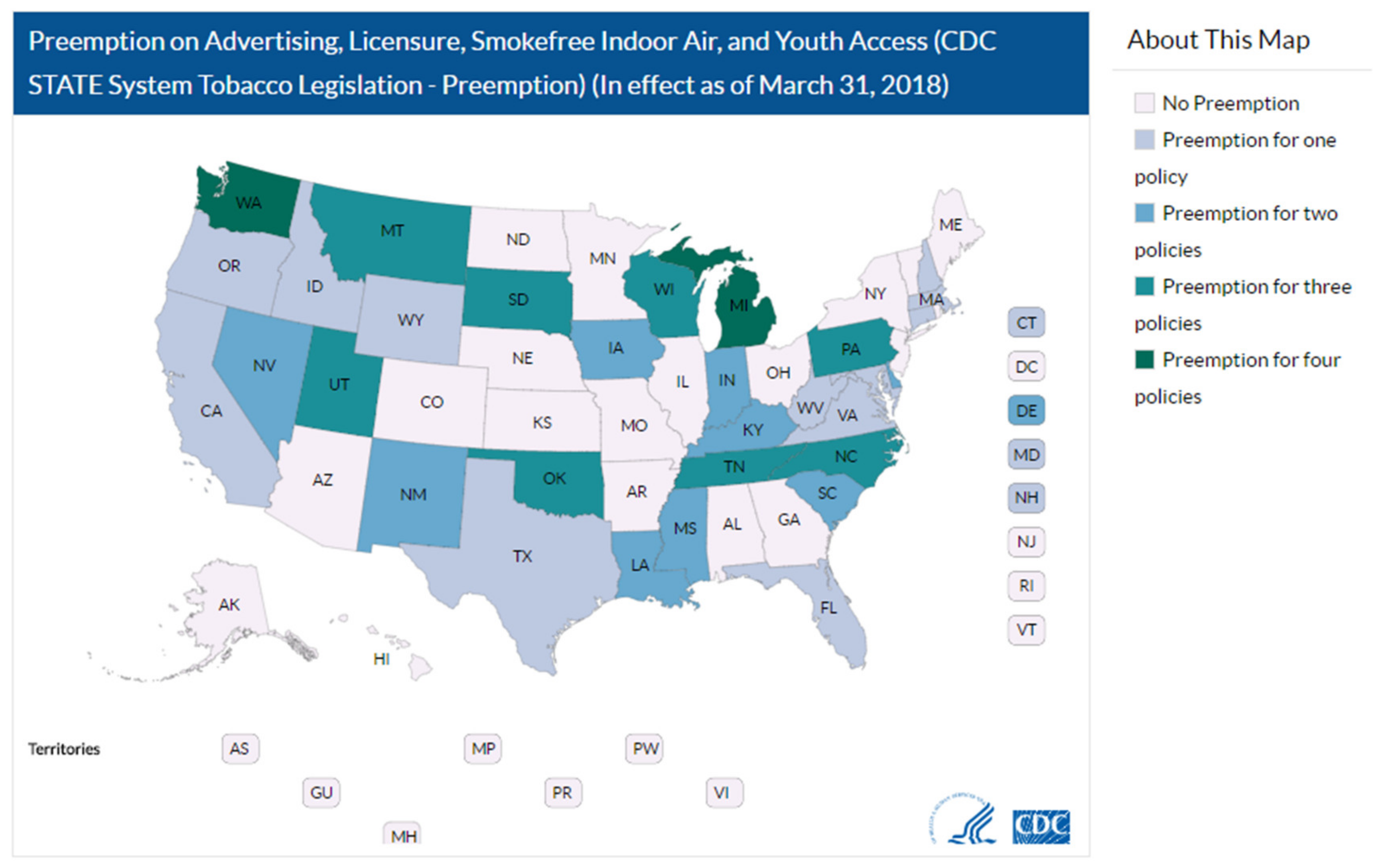
3.3. Concern about the Existence of State Preemption on Tobacco Control Regulation
“Preemption is a big thing that needs to be looked at statewide” (Stakeholder, Southern County).
“NSPA [the Non-Smoker Protection Act] not enough, counties want more control/pre-emption a barrier” (Stakeholder, Southern County).
“Either get rid of the preemption or get [local] exemptions [from the preemption]” (Stakeholder, Northern County).
3.4. Influence of State Preemption on Tobacco Control Efforts in Appalachian Tennessee
“…And we have to do that at a state level because of preemption in Tennessee. I think that’s where we need to be stronger to change policies, to change behaviors. An example would be the preemption law in Tennessee. We’re not able to pass any local ordinances in our own community by our residents. It actually has to be a statewide endeavor. I think that we’re challenged” (Stakeholder, Northern County).
“That is something that the [name of organization] is focused on. We have an implementation plan, and number one on it is to change policy in [name of] County. Where it gets sticky is that the state has a preemption law” (Stakeholder, Northern County).
“[Local] governments, I think their hands are tied because of the preemption” (Stakeholder, Southern County).
3.5. Coping with State Preemption of Tobacco Control in Appalachian Tennessee
“Currently, we’re doing the Knock Tobacco Out of the [public] Park. We actually went to City Council. They didn’t go totally smoke-free, but they’re going to allow us to put the benches in the park that say tobacco-free, or actually in the middle school playground, benches, picnic tables, trash cans, trying to reduce secondhand smoke” (Stakeholder, Southern County).
“We developed a TATU group, which was Teens against Tobacco Use. Took them to a training and then they came back and they did some tobacco education at the middle school level for younger students” (Stakeholder, Northern County).
4. Discussion
“That [preemption] is something that the [name of organization] is focused on. We have an implementation plan, and number one on it is to change policy in [name of] County. Where it gets sticky is that the state has a preemption law” (Stakeholder, Northern County).
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A


References
- U.S Health and Human Services. The Health Consequences of Smoking—50 Years of Progress: A Report of the Surgeon General; 2014; pp. 1–36. [Google Scholar]
- Hiscock, R.; Bauld, L.; Amos, A.; Fidler, J.A.; Munafò, M. Socioeconomic status and smoking: A review. Ann. New York Acad. Sci. 2012, 1248, 107–123. [Google Scholar] [CrossRef] [PubMed]
- Haustein, K.-O. Smoking and poverty. Eur. J. Cardiovasc. Prev. Rehabil. Off. J. Eur. Soc. Cardiol. Work. Groups Epidemiol. Prev. Card. Rehabil. Exerc. Physiol. 2006, 13, 312–318. [Google Scholar] [CrossRef]
- Haustein, K.O. Smoking and Low Socio-Economic Status. Available online: https://www.researchgate.net/publication/7547788_Smoking_and_low_socio-economic_status (accessed on 28 January 2020).
- Assari, S.; Mistry, R. Educational attainment and smoking status in a national sample of American adults; evidence for the blacks’ diminished return. Int. J. Environ. Res. Public Health. 2018, 15, 763. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mensah, G.A.; Mokdad, A.H.; Ford, E.S.; Greenlund, K.J.; Croft, J.B. State of disparities in cardiovascular health in the United States. Circulation 2005, 111, 1233–1241. [Google Scholar] [CrossRef] [PubMed]
- Ezzati, M.; Oza, S.; Danaei, G.; Murray, C.J.L. Trends and cardiovascular mortality effects of state-level blood pressure and uncontrolled hypertension in the United States. Circulation 2008, 117, 905–914. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- U.S Centers for Disease Control and Prevention (CDC). Healthy People. 2010. Available online: https://www.healthypeople.gov (accessed on 28 January 2020).
- Centers for Disease Control. Best Practices for Comprehensive Tobacco Control Programs: 2014; 2014. Available online: https://www.cdc.gov/tobacco (accessed on 26 January 2020).
- Antman, E.; Arnett, D.; Jessup, M.; Sherwin, C. The 50th anniversary of the US surgeon general’s report on tobacco: what we’ve accomplished and where we go from here. J. Am. Heart Assoc. 2014, 3. [Google Scholar] [CrossRef] [Green Version]
- Walton, K.; Wang, T.W.; Schauer, G.L. State-specific prevalence of quit attempts among adult cigarette smokers—United States, 2011–2017. Morb. Mortal. Wkly. Rep. 2019, 6868, 621–626. [Google Scholar] [CrossRef] [Green Version]
- Creamer, M.R.; Wang, T.W.; Babb, S.; Cullen, K.A.; Day, H.; Willis, G.; Jamal, A.; Neff, L. Tobacco Product Use and Cessation Indicators Among Adults—United States, 2018. MMWR Morb. Mortal. Wkly. Rep. 2019, 68, 1013–1019. [Google Scholar] [CrossRef] [Green Version]
- Studlar, D.T. Tobacco control-comparative politics in the United States and Canada. Tobacco Control-Comparative Politics in the United States and Canada; UTPress: Toronto, Canada, 2002; ISBN 1551114569. [Google Scholar]
- Cairney, P.; Studlar, D.T.; Mamudu, H.M. Global Tobacco Control: Power, Policy, Governance and Transfer; Palgrave Macmillan: New York, NY, USA, 2011. [Google Scholar] [CrossRef]
- Rhoades, R.R.; Beebe, L.A. Tobacco Control and Prevention in Oklahoma: Best Practices in a Preemptive State. J. Okla. State Med Assoc. 2015, 108, 434–440. [Google Scholar]
- American Lung Association National President, B; Harold Wimmer, C.P. American Lung Association “State of Tobacco Control” 2019 2 Lung.Org 1-800-LUNGUSA. Available online: https://www.lung.org/research/sotc/state-grades/tennessee (accessed on 26 January 2020).
- Hodge, J.G.; Corbett, A. Legal Preemption and the Prevention of Chronic Conditions. Prev. Chronic Dis. 2016, 13, 160121. [Google Scholar] [CrossRef] [Green Version]
- Mowery, P.D.; Babb, S.; Hobart, R.; Tworek, C.; MacNeil, A. The impact of state preemption of local smoking restrictions on public health protections and changes in social norms. J. Environ. Public Health 2012, 2012. [Google Scholar] [CrossRef]
- Shipan, C.R.; Volden, C. Bottom-Up Federalism: The Diffusion of Antismoking Policies from U.S. Cities to States. Am. J. Political Sci. 2006, 50, 825–843. [Google Scholar] [CrossRef]
- Americas Health Rankings. Explore Smoking in Tennessee | 2018 Senior Report. Available online: http://www.americashealthrankings.org/explore/senior/measure/smoking_sr/state/TN (accessed on 26 January 2020).
- County Health Rankings. Tennessee 2020 County Health Rankings Report. Available online: http://www.countyhealthrankings.org (accessed on 10 April 2020).
- Truth Initiative. Tobacco Nation: An Ongoing Crisis Examining the Health and Policy Disparities of U.S. STATES with the Highest Smoking Rates. Available online: https://gis.truthinitiative.org/tobacco_nation (accessed on 10 April 2020).
- Behringer, B.; Friedell, G.H. Cdc for Health Disparities in Appalachia. 2006. Available online: http://www.cdc.gov/pcd/issues/2006/oct/06_0067.htm (accessed on 26 January 2020).
- Mamudu, H.M.; Littleton, M.A.; Wang, L. Regional Population Health Improvement Plan Tobacco Cessation in Northeast Tennessee Final Report; East Tennessee State University: Johnson City, TN, USA, 2016; Available online: https://www.etsu.edu/cph/hsmp/tobaccopolicy/documents/simreport2016.pdf (accessed on 6 May 2020).
- CDC. State Preemption of Local Smoke-Free Laws in Government Work Sites, Private Work Sites, and Restaurants-United States, 2005–2009. Available online: https://www.cdc.gov/mmwr/preview/mmwrhtml/mm5904a4.htm (accessed on 26 January 2020).
- STATE System Preemption Fact Sheet. Available online: https://www.cdc.gov/statesystem/factsheets/preemption/Preemption.html (accessed on 8 April 2020).
- Ferketich, A.K.; Liber, A.; Pennell, M.; Nealy, D.; Hammer, J.; Berman, M. Clean Indoor Air Ordinance Coverage in the Appalachian Region of the United States. Am. J. Public Health 2010, 100, 1313–1318. [Google Scholar] [CrossRef] [PubMed]
- Mamudu, H.M.; Dadkar, S.; Veeranki, S.P.; He, Y.; Barnes, R.; Glantz, S.A. Multiple streams approach to tobacco control policymaking in a tobacco-growing state. J. Commun. Health. 2014, 39, 633–645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mamudu, H.M.; Veeranki, S.P. Tennessee’s smokefree policy: it’s time for local control. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pubmed/24261184 (accessed on 26 January 2020).
- Mamudu, H.M.; Dadkar, S.; Veeranki, S.P.; Org, E. Tobacco Control in Tennessee: Stakeholder Analysis of the Development of the Non¬Smoker Protection Act. 2012. Available online: https://escholarship.org/uc/item/8z38c04x (accessed on 26 January 2020).
- Mintz, M. Blowing Smoke Rings around the Statehouses, by Mintz, Morton-The Washington Monthly, Volume 28, Issue 5, May 1996 | Online Research Library: Questia. Available online: https://www.questia.com/magazine/1G1-18285110/blowing-smoke-rings-around-the-statehouses (accessed on 28 January 2020).
- Tobacco Control Legal Consortium Fact Sheet. Preemption: The Biggest Challenge to Tobacco Control Background. 2014. Available online: https://publichealthlawcenter.org/sites/default/files/resources/tclc-fs-preemption-tobacco-control-challenge-2014.pdf (accessed on 10 April 2020).
- Swan, J.; Goss, K.F. Lessons from other community-based programs of the National Cancer Institute - ETSU and Northeast State Libraries. Available online: https://etsu.primo.exlibrisgroup.com/discovery/openurl?institution=01ETSU_INST&vid=01ETSU_INST:ETSU&date=1995&aulast=Swan,J.&aulast=Goss,K.F.&aulast=R.A.Couto&iuid=305583&spage=156&title=Sowingseedsinthemountains:Community-basedcoalitionsforc (accessed on 28 January 2020).
- Americans for Nonsmoker’s Rights. History of Preemption of Smokefree Air by State. 2018. Available online: https://www.no-smoke.org (accessed on 26 January 2020).
- Siegel, M.; Carol, J.; Jordan, J.; Hobart, R.; Schoenmarklin, S.; DuMelle, F.; Fisher, P. Preemption in tobacco control: Review of an emerging public health problem. J. Am. Med Assoc. 1997, 278, 858–863. [Google Scholar] [CrossRef]
- Shelton, D.M.; Alciati, M.H.; Chang, M.M.; Fishman, J.A.; Fues, L.A.; Michaels, J.; Bazile, R.J.; Bridgers Jr, J.C.; Rosenthal, J.L.; Kutty, L. State laws on tobacco control-United States, 1995. MMWR CDC Surveill. Summ. Morb. Mortal. Weekly Report CDC Surveill. Summ. Cent. Dis. Control 1995, 44, 1–28. [Google Scholar]
- Nixon, M.L.; Mahmoud, L.; Glantz, S.A. Tobacco industry litigation to deter local public health ordinances: The industry usually loses in court. Tobacco Control. 2004, 13, 65–73. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine (IOM). For the Public’s Health: Revitalizing Law and Policy to Meet New Challenges; National Academies Press: Washington, DC, USA, 2011. [Google Scholar] [CrossRef]
- O’Connor, J.C.; MacNeil, A.; Chriqui, J.F.; Tynan, M.; Bates, H.; Eidson, S.K.S. Preemption of local smoke-free air ordinances: the implications of judicial opinions for meeting national health objectives. J. Law Med. Ethics J. Am. Soc. Law Med. Ethics 2008, 36, 403–412. [Google Scholar] [CrossRef]
- Pomeranz, J.L.; Pertschuk, M. State preemption: A significant and quiet threat to public health in the United States. Am. J. Public Health 2017, 107, 900–902. [Google Scholar] [CrossRef]
- Pertschuk, M.; Pomeranz, J.L.; Aoki, J.R.; Larkin, M.A.; Paloma, M. Assessing the impact of federal and state preemption in public health: A framework for decision makers. J. Public Health Manag. Pract. 2013, 19, 213–219. [Google Scholar] [CrossRef] [Green Version]
- Yañez, E.; Cox, G.; Cooney, M.; Eadie, R. Preemption in public health: The dynamics of clean indoor air laws. J. Law Med. Ethics 2003, 31, 84–85. [Google Scholar] [CrossRef] [PubMed]
- Gorovitz, E.; Mosher, J.; Pertschuk, M. Preemption or prevention? lessons from efforts to control firearms, alcohol, and tobacco. J. Public Health Policy 1998, 19, 36–50. Available online: http://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pubmed/9581429 (accessed on 28 January 2020). [CrossRef] [PubMed]
- Conlisk, E.; Siegel, M.; Lengerich, E.; mac Kenzie, W.; Malek, S.; Eriksen, M. The status of local smoking regulations in North Carolina following a state preemption bill. JAMA 1995, 273, 805–807. Available online: http://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pubmed/7861576 (accessed on 26 January 2020). [CrossRef] [Green Version]
- Stark, M.J.; Rohde, K.; Maher, J.E.; Pizacani, B.A.; Dent, C.W.; Bard, R.; Carmella, S.G.; Benoit, A.R.; Thomson, N.M.; Hecht, S.S. The impact of clean indoor air exemptions and preemption policies on the prevalence of a tobacco-specific lung carcinogen among nonsmoking bar and restaurant workers. Am. J. Public Health 2007, 97, 1457–1463. [Google Scholar] [CrossRef] [PubMed]
- Israel, B.A.; Schulz, A.J.; Parker, E.A.; Becker, A.B. Community-based participatory research: Policy recommendations for promoting a partnership approach in health research. Educ. Health 2001, 14, 182–197. [Google Scholar] [CrossRef]
- Owusu, D.; Mamudu, H.M.; Collins, C.; Robertson, C.; Wang, L.; Rafie, B.; Littleton, M.A. The Use of Alternative Tobacco Products and Associated Factors among School-going Youth in Central Appalachia HHS Public Access. J. Health Care Poor Underserved 2019, 30, 249–264. [Google Scholar] [CrossRef]
- County Health Rankings. Washington County, Tennessee | County Health Rankings & Roadmaps. Available online: https://www.countyhealthrankings.org/app/tennessee/2019/rankings/washington/county/outcomes/overall/snapshot (accessed on 26 January 2020).
- Fry, C.E.; Tindle, H.A.; Young, C.; Rogus, E.I.; Frist, W.H.; Buntin, M.B. Development of a Tobacco Control Prescription in a Southern US City HHS Public Access. Commun. Health Partnersh. 2019, 13, 237–245. [Google Scholar] [CrossRef]
- Kang, J.Y.; Kenemer, B.; Mahoney, M.; Tynan, M.A. State Preemption: Impacts on Advances in Tobacco Control. J. Public Health Manag. Pract. 2020, 26, S54–S61. [Google Scholar] [CrossRef]
- Studlar, D.T. Tobacco Control. in West. Virginia: You’ve Come a Long Way, Maybe; West Virginia: Morgantown, WV, USA, 2006; Volume 23, pp. 1–10. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
| Organization/Institution | Title | Gap Analysis | Interviews | Community Meeting | Regional Meeting |
|---|---|---|---|---|---|
| Health Councils × 7 | ✓ | ✓ | ✓ | ||
| Sullivan County Anti-Drug Coalition | ✓ | ✓ | ✓ | ||
| Carter County Health Dept. | Health Educator | ✓ | ✓ | ✓ | |
| Carter County Health Dept. | Health Educator | ✓ | ✓ | ||
| Carter and Johnson County Health Dept. | Director | ✓ | ✓ | ||
| Carter County | Counselor | ✓ | |||
| Greene County Health Dept. | Health Educator | ✓ | ✓ | ✓ | |
| Greene County Health Dept. | Director | ✓ | |||
| Greene County Laughlin Hospital | Wellness Director | ✓ | |||
| Greene County Schools Coordinated School Health | Coordinator | ✓ | |||
| Greene County Takoma Hospital | Wellness Director | ✓ | ✓ | ||
| Greene County—Plus Mark Inc. | Employee Wellness Programs | ✓ | |||
| Greene County—John Deere Products | Plant Nurse | ✓ | ✓ | ||
| Hancock Health Dept. | Health Educator | ✓ | ✓ | ✓ | |
| Hancock Coordinated School Health | Coordinator | ✓ | ✓ | ||
| Hancock County School-based Clinic | Health Educator | ✓ | |||
| Hawkins County Health Dept. | Director | ✓ | ✓ | ||
| Hawkins County Health Dept. | Health Educator | ✓ | ✓ | ||
| Hawkins County—Church Hill Health Dept. | PPI Tobacco Team Leader | ✓ | |||
| Hawkins County—Church Hill Health Dept. | RDA | ✓ | ✓ | ||
| Hawkins County Coordinated School Health | Coordinator | ✓ | |||
| Johnson County Health Dept. | Health Educator | ✓ | ✓ | ✓ | |
| Johnson County ACTION | Executive Director, Prevention Coordinator | ✓ | ✓ | ✓ | |
| Johnson County/Mountain City Nursing Clinic | Site Coordinator | ✓ | ✓ | ||
| Johnson County—Pregnancy Support Center | Director | ✓ | ✓ | ||
| Sullivan County Health Dept. | Tobacco Specialist | ✓ | ✓ | ||
| Sullivan County Health Dept. | Director | ✓ | |||
| Sullivan County Anti-Drug Coalition | Prevention Coordinator | ✓ | ✓ | ✓ | |
| Sullivan County Anti-Drug Coalition | Director | ✓ | ✓ | ||
| Sullivan County Health Dept. | Tobacco Specialist | ✓ | |||
| Sullivan County | Physician | ✓ | |||
| Sullivan County—Kingsport YMCA | CEO | ✓ | |||
| Unicoi Health Dept. | Health Educator | ✓ | ✓ | ||
| Unicoi Health Dept. | Director | ✓ | ✓ | ||
| Unicoi Hospital (MHSA) | Nurse Manager | ✓ | ✓ | ||
| Unicoi Project Access | Navigator | ✓ | ✓ | ||
| Unicoi YMCA | Director | ✓ | |||
| Washington County Health Dept. | Director | ✓ | ✓ | ✓ | |
| Washington County Health Dept. | Health Educator | ✓ | ✓ | ✓ | |
| American Cancer Society | Community Manager | ✓ | ✓ | ||
| American Cancer Society | Community Manager | ✓ | ✓ | ||
| Frontier Health | Wellness Facilitator | ✓ | ✓ | ||
| Frontier Health | Director | ✓ | ✓ | ||
| ETSU—Family Medicine | Professor and Head of Clinical Research | ✓ | ✓ | ✓ | |
| ETSU—Nursing Clinics - | Director School-based Clinics | ✓ | ✓ | ✓ | |
| ETSU—Nursing Clinics | Executive Director | ✓ | |||
| ETSU Wellness Committee | Member | ✓ | |||
| ETSU Human Resources | Director | ✓ | |||
| ETSU Center for Community Outreach | Director | ✓ | |||
| Hispanic Community | ETSU Outreach | ✓ | ✓ | ||
| Hispanic Community | NE State Spanish Teacher | ✓ | |||
| Hispanic Community | Tobacco interest | ✓ | |||
| African American Community | ETSU staff | ✓ | |||
| Mountain States Health Alliance | Regional Outreach Manager | ✓ | |||
| Northeast Regional Health Dept. | Director | ✓ | |||
| Northeast Regional Health Dept. | Health Council Coordinator | ✓ | ✓ | ||
| Northeast Regional Health Dept | Program Manager | ✓ | |||
| Niswonger Foundation | Director of Program and Outreach | ✓ | |||
| Wellmont Hospitals | Director Quality | ✓ | |||
| Wellmont Hospitals | Practice Administrator | ✓ | |||
| Wellmont Hospitals | Director of Community | ✓ | |||
| Totals | 8 | 28 | 66 | 120 |
| S/N | Organization | Description of Policies and Programs |
|---|---|---|
| 1 | Local Businesses | |
| Crown Laboratories | • Smoke-free campus; must smoke inside cars only, including ENDS. • Optional life insurance policy gives rates based on smoking status through Boston Mutual. | |
| Bristol Motor Speedway | • Smoke-free policy (including ENDS) that is enforced through the social media, text message. | |
| Academy Hill Condo Association, Jonesborough | • Smoke-free building policy, requires no smoking by residents in the building | |
| 2 | Educational Systems | |
| East Tennessee State University’s Tobacco free policy | • Ban on the use of smoked, smokeless, and any lit product (including ENDS), except in private vehicles. • Campus patrol to ensure compliance. • Noncompliance is progressively penalized. • Standing tobacco committee. • Organization of campus educational events. • Cessation services available and accessible to students. • Continuous research to assess policy efficacy, attitudes, compliance, etc. | |
| All school systems in the region | • Tobacco free campus, including ENDS | |
| Teens against Tobacco Use (TATU) | • School based health promotion program, peer-to-peer educational programs for students aged 14–17 years. | |
| Tar Wars | • School-based 4-h health curriculum targeting youth aged 8–14 years. | |
| The Michigan Model for Health | • School-based health curriculum implemented by coordinated School Health. | |
| 3 | Public Organizations | |
| Johnson City Power Board (JCPB) | • Smoke free campus, including ENDS. • No smoking in JCPB vehicles or in front of customers or out on a job. • Campus has designated smoking areas. • Contracted MSHA nurse that periodically conducts smoking cessation classes and works on a one-on-one basis with employees. | |
| 4 | Health Organizations | |
| Mountain States Health Alliance (MSHA)’s nicotine-free workforce and smoke-free campus | • All employees should be nicotine-free. • Nicotine-dependent employees are provided with support for cessation. • Random test for compliance. • Smoke-free hospital campus. | |
| Woodridge Hospital of Mountain States Health Alliance | • Tobacco-free mental health facility. • No smoking by patients and provides patients with nicotine replacement therapies. | |
| 5 | Governmental programs and policies | |
| Smoke-/tobacco-free outdoor public places | • Campaigns to make ball parks and other outdoor places smoke-/tobacco-free. | |
| Gold Sneaker Initiative | • Developed to augment health and wellness policy in childcare facilities whereby facilities with Gold Sneaker recognition must adopt a tobacco-free policy. | |
| Clinical Effort Against Second Hand Smoke Exposure (C.E.A.S.E) | • A training module for healthcare providers that seeks to address family tobacco use in a routine and effective manner. | |
| Unsmokeable | • A movement led by the Sullivan County Regional Health Department to encourage and inspire Sullivan County youth to live a smoke-free life. | |
| Tennessee Intervention for Pregnant Smokers (TIPS) | • A program that offers cessation assistance to pregnant women and healthcare provider training to enable them to deliver brief smoking cessation counseling and assistance to pregnant patients. | |
| Power to Quit | • An incentive-based program involving cessation support during pregnancy. | |
| Freedom from Smoking Cessation | • Classes taught in Washington and Unicoi counties. | |
| Tobacco Quitline | • A toll-free telephone service offering personalized support for individuals wanting to quit. | |
| 6 | Non-Governmental initiatives | |
| Baby and Me Tobacco Free | • An incentive-based program for pregnant women and women with infant children are given vouchers to purchase diapers for staying smoke-free. | |
| Project Connect | • An adolescent tobacco cessation and reduction program. | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mamudu, H.M.; Osedeme, F.; Robertson, C.; Littleton, M.A.; Owusu, D.; Wang, L.; Studlar, D.T. A Qualitative Study to Explore Perception of Impacts of Preemption of Tobacco Regulation on Counties in Appalachian Tennessee. Int. J. Environ. Res. Public Health 2020, 17, 3230. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17093230
Mamudu HM, Osedeme F, Robertson C, Littleton MA, Owusu D, Wang L, Studlar DT. A Qualitative Study to Explore Perception of Impacts of Preemption of Tobacco Regulation on Counties in Appalachian Tennessee. International Journal of Environmental Research and Public Health. 2020; 17(9):3230. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17093230
Chicago/Turabian StyleMamudu, Hadii M., Fenose Osedeme, Crystal Robertson, Mary Ann Littleton, Daniel Owusu, Liang Wang, and Donley T. Studlar. 2020. "A Qualitative Study to Explore Perception of Impacts of Preemption of Tobacco Regulation on Counties in Appalachian Tennessee" International Journal of Environmental Research and Public Health 17, no. 9: 3230. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17093230