Environmental Contamination of SARS-CoV-2 in a Non-Healthcare Setting

Abstract
:1. Introduction
2. Materials and Methods
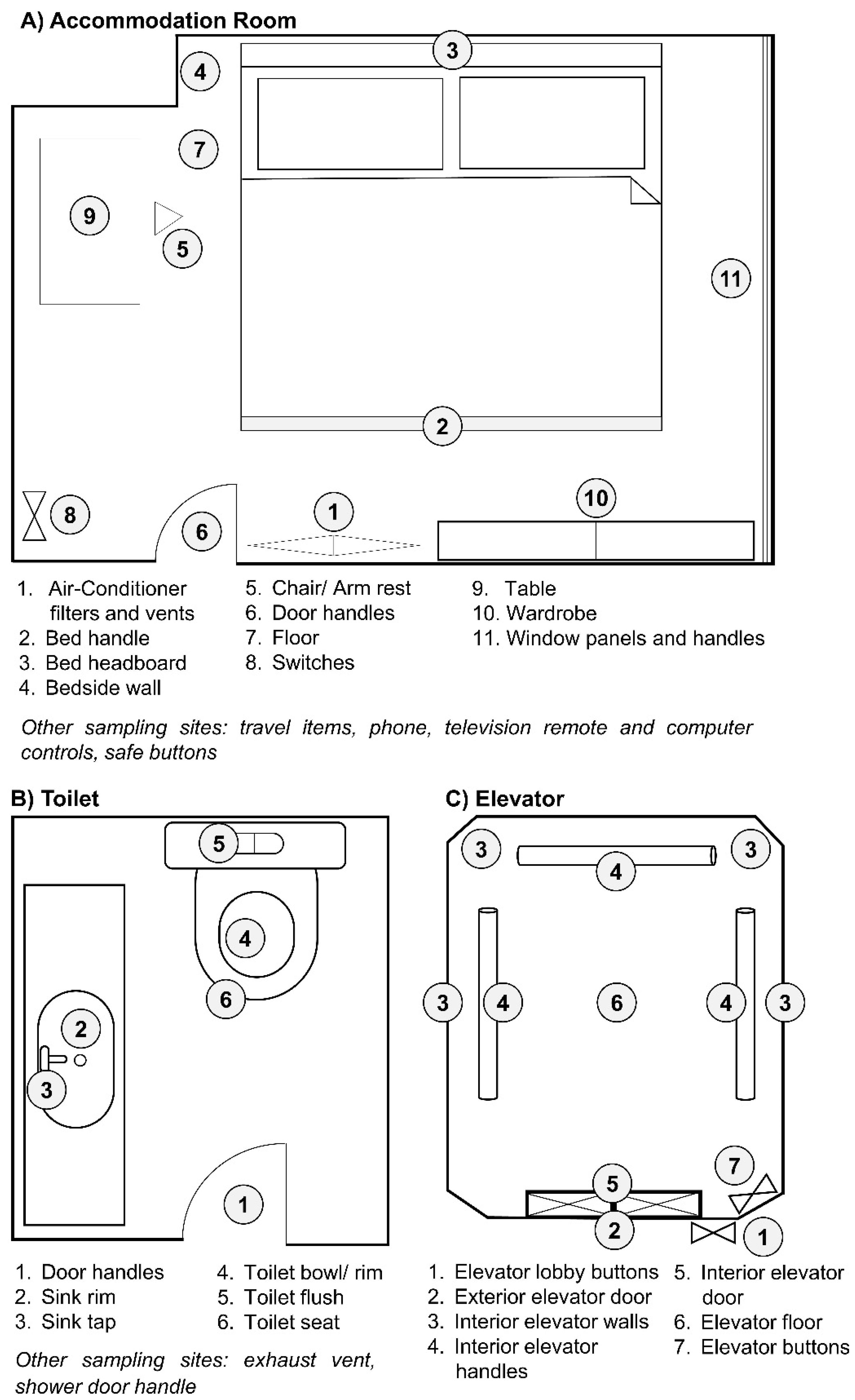
2.1. Environmental Samples
2.2. Study/Ethics Approval
2.3. Extraction of SARS-CoV-2 RNA from Environmental Samples
2.4. Detection of SARS-CoV-2 RNA by Polymerase Chain Reaction
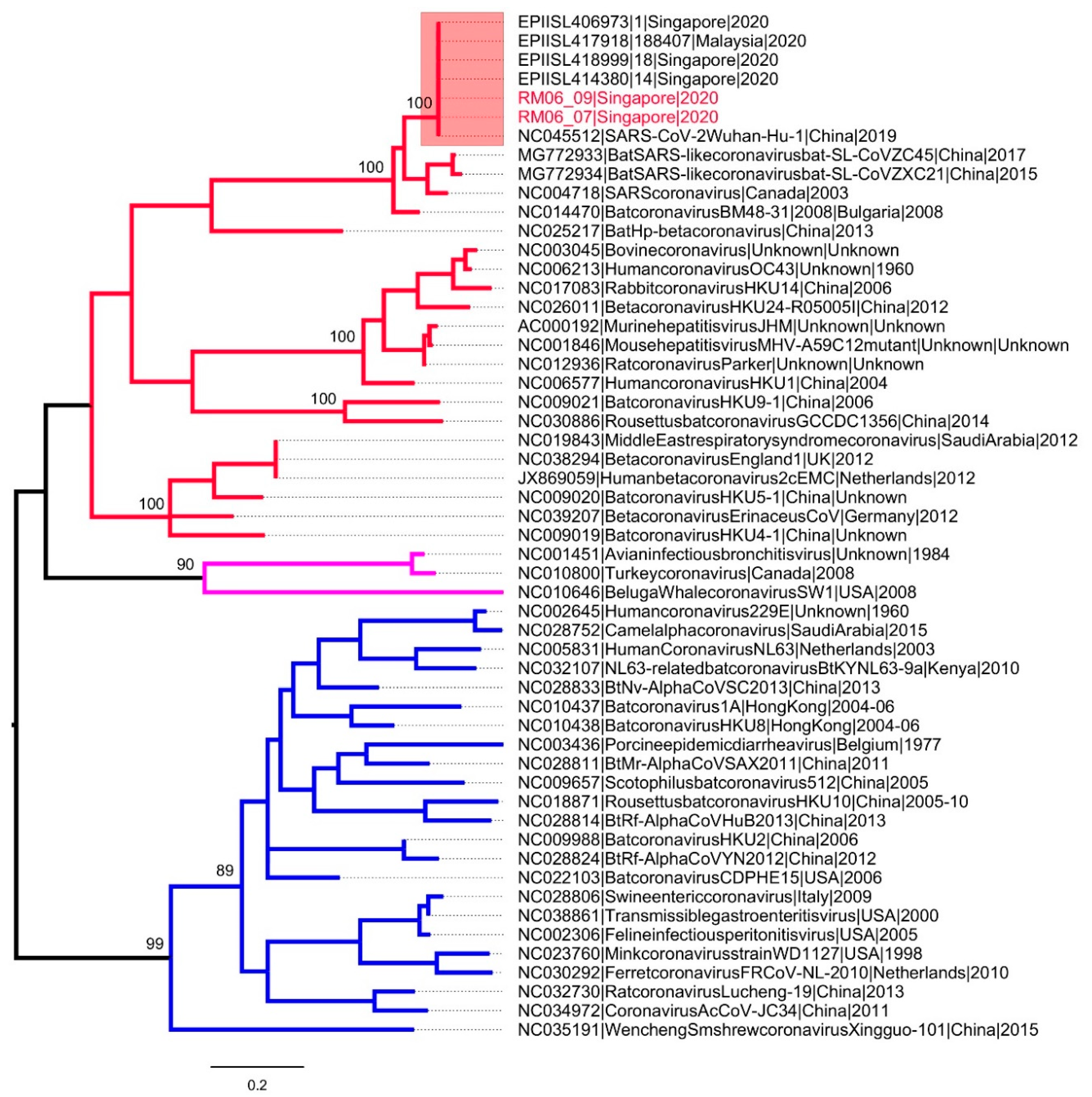
2.5. Assembly and Analysis of Genome Sequences
2.6. Data Availability
3. Results and Discussion
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Adhikari, S.P.; Meng, S.; Wu, Y.-J.; Mao, Y.-P.; Ye, R.-X.; Wang, Q.-Z.; Sun, C.; Sylvia, S.; Rozelle, S.; Raat, H.; et al. Epidemiology, causes, clinical manifestation and diagnosis, prevention and control of coronavirus disease (COVID-19) during the early outbreak period: A scoping review. Infect. Dis. Poverty 2020, 9, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sohrabi, C.; Alsafi, Z.; O’Neill, N.; Khan, M.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C.; Agha, R. World Health Organization declares global emergency: A review of the 2019 novel coronavirus (COVID-19). Int. J. Surg. 2020, 76, 71–76. [Google Scholar] [CrossRef] [PubMed]
- Pung, R.; Chiew, C.J.; Young, B.; Chin, S.; Chen, M.I.-C.; Clapham, H.E.; Cook, A.R.; Maurer-Stroh, S.; Toh, M.P.H.S.; Poh, C.; et al. Investigation of three clusters of COVID-19 in Singapore: Implications for surveillance and response measures. Lancet 2020, 395, 1039–1046. [Google Scholar] [CrossRef]
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.S.C.; et al. Clinical characteristics of coronavirus disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef]
- How COVID-19 Spreads 2020. Available online: https://www.cdc.gov/coronavirus/2019-ncov/prevent-getting-sick/how-covid-spreads.html (accessed on 11 November 2020).
- Chen, Y.-C.; Huang, L.-M.; Chan, C.-C.; Su, C.-P.; Chang, S.-C.; Chang, Y.-Y.; Chen, M.-L.; Hung, C.-C.; Chen, W.-J.; Lin, F.-Y.; et al. SARS in hospital emergency room. Emerg. Infect. Dis. 2004, 10, 782–788. [Google Scholar] [CrossRef]
- Dowell, S.F.; Simmerman, J.M.; Erdman, D.D.; Wu, J.-S.J.; Chaovavanich, A.; Javadi, M.; Yang, J.-Y.; Anderson, L.J.; Tong, S.; Ho, M.S. Severe acute respiratory syndrome coronavirus on hospital surfaces. Clin. Infect. Dis. 2004, 39, 652–657. [Google Scholar] [CrossRef] [Green Version]
- Bin, S.Y.; Heo, J.Y.; Song, M.S.; Lee, J.; Kim, E.H.; Park, S.J.; Kwon, H.-I.; Kim, S.M.; Kim, Y.-I.; Si, Y.-J. Environmental contamination and viral shedding in MERS patients during MERS-CoV outbreak in South Korea. Clin. Infect. Dis. 2016, 62, 755–760. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.-H.; Chang, S.Y.; Sung-Han, K.; Park, J.H.; Bin Kim, H.; Lee, H.; Choi, J.-P.; Choi, W.S.; Min, J.-Y. Extensive Viable Middle East Respiratory Syndrome (MERS) coronavirus contamination in air and surrounding environment in MERS isolation wards. Clin. Infect. Dis. 2016, 63, 363–369. [Google Scholar] [CrossRef] [Green Version]
- Ong, S.W.X.; Tan, Y.K.; Chia, P.Y.; Lee, T.H.; Ng, O.T.; Wong, M.S.Y.; Marimuthu, K. Air, surface environmental, and personal protective equipment contamination by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) from a symptomatic patient. JAMA 2020, 323, 1610–1612. [Google Scholar] [CrossRef] [Green Version]
- Kampf, G.; Todt, D.; Pfaender, S.; Steinmann, E. Persistence of coronaviruses on inanimate surfaces and their inactivation with biocidal agents. J. Hosp. Infect. 2020, 104, 246–251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Doremalen, N.; Bushmaker, T.; Morris, D.H.; Holbrook, M.G.; Gamble, A.; Williamson, B.N.; Tamin, A.; Harcourt, J.L.; Thornburg, N.J.; Gerber, S.I.; et al. Aerosol and surface stability of SARS-CoV-2 as compared with SARS-CoV-1. N. Engl. J. Med. 2020, 382, 1564–1567. [Google Scholar] [CrossRef] [PubMed]
- Interim Guidelines for Environmental Cleaning and Disinfection in Residences That May Be Exposed to the COVID-19 Virus 2020. Available online: https://www.nea.gov.sg/our-services/public-cleanliness/environmental-cleaning-guidelines/guidelines/interim-guidelines-for-environmental-cleaning-and-disinfection-in-residences (accessed on 11 November 2020).
- Interim Guidelines for Environmental Cleaning and Disinfection of Areas Exposed to Confirmed Case(s) of COVID-19 in Non-Healthcare Premises 2020. Available online: https://www.nea.gov.sg/our-services/public-cleanliness/environmental-cleaning-guidelines/guidelines/guidelines-for-environmental-cleaning-and-disinfection (accessed on 11 November 2020).
- Wang, J.; Du, G. COVID-19 may transmit through aerosol. Ir. J. Med. Sci. 2020, 189, 1143–1144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Booth, T.F.; Kournikakis, B.; Bastien, N.; Ho, J.; Kobasa, D.; Stadnyk, L.; Li, Y.; Spence, M.; Paton, S.; Henry, B.; et al. Detection of airborne severe acute respiratory syndrome (SARS) coronavirus and environmental contamination in SARS outbreak units. J. Infect. Dis. 2005, 191, 1472–1477. [Google Scholar] [CrossRef] [PubMed]
- Julian, T.R.; Tamayo, F.J.; Leckie, J.O.; Boehm, A.B. Comparison of surface sampling methods for virus recovery from fomites. Appl. Environ. Microbiol. 2011, 77, 6918–6925. [Google Scholar] [CrossRef] [Green Version]
- Woo, P.C.Y.; Lau, S.K.P.; Chu, C.-M.; Chan, K.-H.; Tsoi, H.-W.; Huang, Y.; Wong, B.H.L.; Poon, R.W.S.; Cai, J.J.; Luk, W.-K.; et al. Characterization and complete genome sequence of a novel coronavirus, coronavirus HKU1, from patients with pneumonia. J. Virol. 2005, 79, 884–895. [Google Scholar] [CrossRef] [Green Version]
- Shu, Y.; McCauley, J. GISAID: Global initiative on sharing all influenza data-from vision to reality. Euro Surveill. 2017, 22, 30494. [Google Scholar] [CrossRef] [Green Version]
- Coronavirus Disease (COVID-19) Technical Guidance: Laboratory Testing for 2019-nCoV in Humans 2020. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technical-guidance/laboratory-guidance (accessed on 11 November 2020).
- Ta, H. BioEdit: A user-friendly biological sequence alignment editor and analysis program for Windows 95/98/NT. Nucl Acids Symp Ser. 1999, 41, 95–98. [Google Scholar]
- Kumar, S.; Stecher, G.; Tamura, K. MEGA7: Molecular Evolutionary Genetics Analysis version 7.0 for bigger datasets. Mol. Biol. Evol. 2016, 33, 1870–1874. [Google Scholar] [CrossRef] [Green Version]
- Wei, W.E.; Li, Z.; Chiew, C.J.; Yong, S.E.; Toh, M.P.; Lee, V.J. Presymptomatic transmission of SARS-CoV-2-Singapore, January 23–March 16, 2020. MMWR. Morb. Mortal. Wkly. Rep. 2020, 69, 411–415. [Google Scholar] [CrossRef] [Green Version]
- Jiang, F.-C.; Jiang, X.-L.; Wang, Z.-G.; Meng, Z.-H.; Shao, S.-F.; Anderson, B.D.; Ma, M.-J. Detection of severe acute respiratory syndrome coronavirus 2 RNA on surfaces in quarantine rooms. Emerg. Infect. Dis. 2020, 26, 2162–2164. [Google Scholar] [CrossRef]
- Yamagishi, T.; Ohnishi, M.; Matsunaga, N.; Kakimoto, K.; Kamiya, H.; Okamoto, K.; Suzuki, M.; Gu, Y.; Sakaguchi, M.; Tajima, T.; et al. Corrigendum to: Environmental sampling for severe acute respiratory syndrome coronavirus 2 during a COVID-19 outbreak on the diamond princess cruise ship. J. Infect. Dis. 2020. [Google Scholar] [CrossRef] [PubMed]
- Matson, M.J.; Yinda, C.K.; Seifert, S.N.; Bushmaker, T.; Fischer, R.J.; van Doremalen, N.; Lloyd-Smith, J.O.; Munster, V.J. Effect of environmental conditions on SARS-CoV-2 stability in human nasal mucus and sputum. Emerg Infect. Dis 2020, 26. [Google Scholar]
- Santarpia, J.L.; Rivera, D.N.; Herrera, V.L.; Morwitzer, M.J.; Creager, H.M.; Santarpia, G.W.; Crown, K.K.; Brett-Major, D.M.; Schnaubelt, E.R.; Broadhurst, M.J.; et al. Aerosol and surface contamination of SARS-CoV-2 observed in quarantine and isolation care. Sci Rep. 2020, 10, 12732. [Google Scholar] [CrossRef] [PubMed]
- Consensus Document on the Epidemiology of Severe Acute Respiratory Syndrome (SARS) 2003. Available online: https://www.who.int/csr/sars/WHOconsensus.pdf?ua=1 (accessed on 11 November 2020).
- Abrahão, J.S.; Sacchetto, L.; Rezende, I.M.; Rodrigues, R.A.L.; Crispim, A.P.C.; Moura, C.; Mendonça, D.C.; Reis, E.; Souza, F.; Oliveira, G.F.G.; et al. Detection of SARS-CoV-2 RNA on public surfaces in a densely populated urban area of Brazil: A potential tool for monitoring the circulation of infected patients. Sci. Total. Environ. 2020, 142645. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Case | No. of Sites | No. of Samples 1 | Days after Occupancy | Estimated Floor Area (m2) | Ventilation | Air-Conditioning System | Active Ingredient in Disinfectants |
|---|---|---|---|---|---|---|---|
| 1 2 | Commercial Boarding Room (n = 1) Toilets (n = 6) | 120 3 | 1 | Room—4 Toilet—1.2 | Mechanical ventilation limited to toilets only | Wall-mounted fan coil unit | Sodium chlorite |
| 2 4 | Home Residence Room (n = 2) Toilet (n = 1) | 100 | 3 | Room 1—12 Room 2—14.5 Toilet—3.8 | Naturally ventilated, ambient temperature | Wall-mounted fan coil unit (not used since case vacated) | Hydrogen peroxide and peroxyacetic acid |
| 3 4 | 1 | ||||||
| 4 | Commercial Boarding Room (n = 1) Toilet (n = 1) | 40 | 3 | Room—50 Toilet—5 | Mechanical ventilation | Fan coil unit | Benzalkonium chloride |
| 5 | Elevators of public housing (n = 3) | 96 | 2 | 1.7 | Mechanical and natural, ambient temperature | Nil | Sodium hypochlorite |
| 6 | Elevators of public housing (n = 3) | 78 | 3 | 1.7 | Mechanical and natural, ambient temperature | Nil | Sodium hypochlorite |
| PCR Round | Primer | Sequence(5′-3′) | Target Region | Product Size |
|---|---|---|---|---|
| First round | SARSCoV2_FN1 | ggttgggattatcctaaatgtga | RNA dependent RNA polymerase (RdRp) gene | 440-bp |
| SARSCoV2_RN1 | gcatcgtcagagagtatcatcat | |||
| Second round /Nested | SARSCoV2-F2N2 | ATGCTTAGAATTATGGCCTCACTTG | 356 bp | |
| SARSCoV2_RN2 | CGTAAAACTCATTCACAAAGTCTGT |
| Sampling Location and Surface | RT-PCR Results in Samples Collected before and after Disinfection 1 | |||||
|---|---|---|---|---|---|---|
| Before | After | Before | After | Before | After | |
| Case 1 | Cases 2 and 3 | Case 4 | ||||
| Accommodation room | ||||||
| Air samples | 0 (3) | 0 (3) | NA | NA | NA | NA |
| Air-conditioner filters and vents | 0 (6) | 0 (6) | 0 (6) | 0 (6) | 0 (1) | 0 (1) |
| Bed handle | 1 (1) | 0 (1) | NA | NA | NA | NA |
| Bed headboards | 1 (1) | 0 (1) | 0 (2) | 0 (2) | 0 (1) | 0 (1) |
| Beside walls | 0 (2) | 0 (2) | 0 (2) | 0 (2) | NA | NA |
| Chairs/ arm rests | 0 (1) | 0 (1) | 0 (2) | 0 (2) | 0 (1) | 0 (1) |
| Door handles | 0 (1) | 0 (1) | 0 (2) | 0 (2) | 0 (1) | 0 (1) |
| Floor | NA | NA | 0 (2) | 0 (2) | NA | NA |
| Cups | NA | NA | 0 (2) | 0 (2) | 0 (1) | 0 (1) |
| Travel items | NA | NA | 0 (2) | 0 (2) | 0 (1) | 0 (1) |
| Phone | NA | NA | NA | NA | 0 (1) | 0 (1) |
| Television remote and computer controls | NA | NA | 0 (6) | 0 (6) | 0 (1) | 0 (1) |
| Safe buttons | NA | NA | NA | NA | 0 (1) | 0 (1) |
| Switches | 0 (2) | 0 (2) | 0 (2) | 0 (2) | 0 (2) | 0 (2) |
| Tables | 0 (1) | 0 (1) | 0 (2) | 0 (2) | 0 (2) | 0 (2) |
| Wardrobe | NA | NA | 0 (2) | 0 (2) | NA | NA |
| Window panels and handles | NA | NA | 0 (7) | 0 (7) | NA | NA |
| Sub Total | 2 (18) | 0 (18) | 0 (39) | 0 (39) | 0 (13) | 0 (13) |
| Toilets | ||||||
| Exhaust vents | 0 (6) | 0 (6) | NA | NA | NA | NA |
| Door handle | 0 (6) | 0 (6) | 0 (2) | 0 (2) | NA | NA |
| Shower door handle | 0 (6) | 0 (6) | 0 (1) | 0 (1) | 0 (1) | 0 (1) |
| Sink rims | 0 (6) | 0 (6) | 0 (2) | 0 (2) | 0 (1) | 0 (1) |
| Sink taps | 0 (6) | 0 (6) | 0 (1) | 0 (1) | 0 (1) | 0 (1) |
| Toilet bowl/rim | 0 (6) | 0 (6) | 0 (2) | 0 (2) | 0 (1) | 0 (1) |
| Toilet flush | 0 (6) | 0 (6) | 0 (1) | 0 (1) | 0 (1) | 0 (1) |
| Toilet seat | NA | NA | 0 (2) | 0 (2) | 0 (2) | 0 (2) |
| Sub Total | 0 (42) | 0 (42) | 0 (11) | 0 (11) | 0 (7) | 0 (7) |
| Elevators | Case 5 | Case 6 | ||||
| Elevator lobby buttons | 0 (6) | 0 (6) | 0 (6) | 0 (6) | ||
| Exterior elevator doors | 0 (6) | 0 (6) | 0 (6) | 0 (6) | ||
| Interior elevator walls | 0 (9) | 0 (9) | 0 (15) | 0 (15) | ||
| Interior elevator handles | 0 (9) | 0 (9) | 0 (9) | 0 (9) | ||
| Interior elevator doors | 0 (3) | 0 (3) | 0 (3) | 0 (3) | ||
| Elevator floors | 0 (3) | 0 (3) | 0 (3) | 0 (3) | ||
| Elevator buttons | 0 (3) | 0 (3) | 0 (6) | 0 (6) | ||
| Sub Total | 0 (39) | 0 (39) | 0 (48) | 0 (48) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wong, J.C.C.; Hapuarachchi, H.C.; Arivalan, S.; Tien, W.P.; Koo, C.; Mailepessov, D.; Kong, M.; Nazeem, M.; Lim, M.; Ng, L.C. Environmental Contamination of SARS-CoV-2 in a Non-Healthcare Setting. Int. J. Environ. Res. Public Health 2021, 18, 117. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18010117
Wong JCC, Hapuarachchi HC, Arivalan S, Tien WP, Koo C, Mailepessov D, Kong M, Nazeem M, Lim M, Ng LC. Environmental Contamination of SARS-CoV-2 in a Non-Healthcare Setting. International Journal of Environmental Research and Public Health. 2021; 18(1):117. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18010117
Chicago/Turabian StyleWong, Judith Chui Ching, Hapuarachchige Chanditha Hapuarachchi, Sathish Arivalan, Wei Ping Tien, Carmen Koo, Diyar Mailepessov, Marcella Kong, Mohammad Nazeem, Merrill Lim, and Lee Ching Ng. 2021. "Environmental Contamination of SARS-CoV-2 in a Non-Healthcare Setting" International Journal of Environmental Research and Public Health 18, no. 1: 117. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18010117