Mortality Risk from Respiratory Diseases Due to Non-Optimal Temperature among Brazilian Elderlies

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
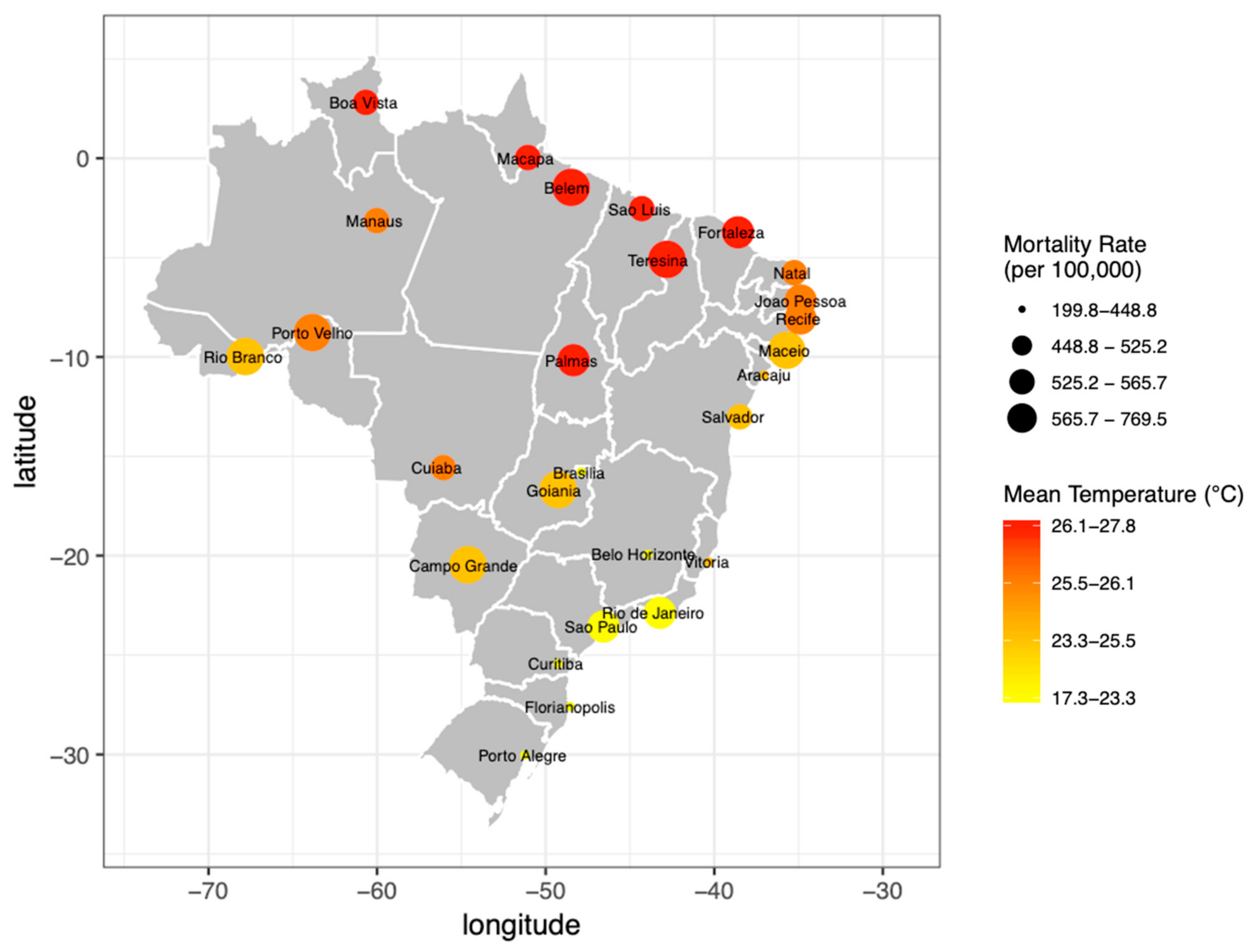
2.1. Study Area and Period
2.2. Data
2.3. Statistical Analysis
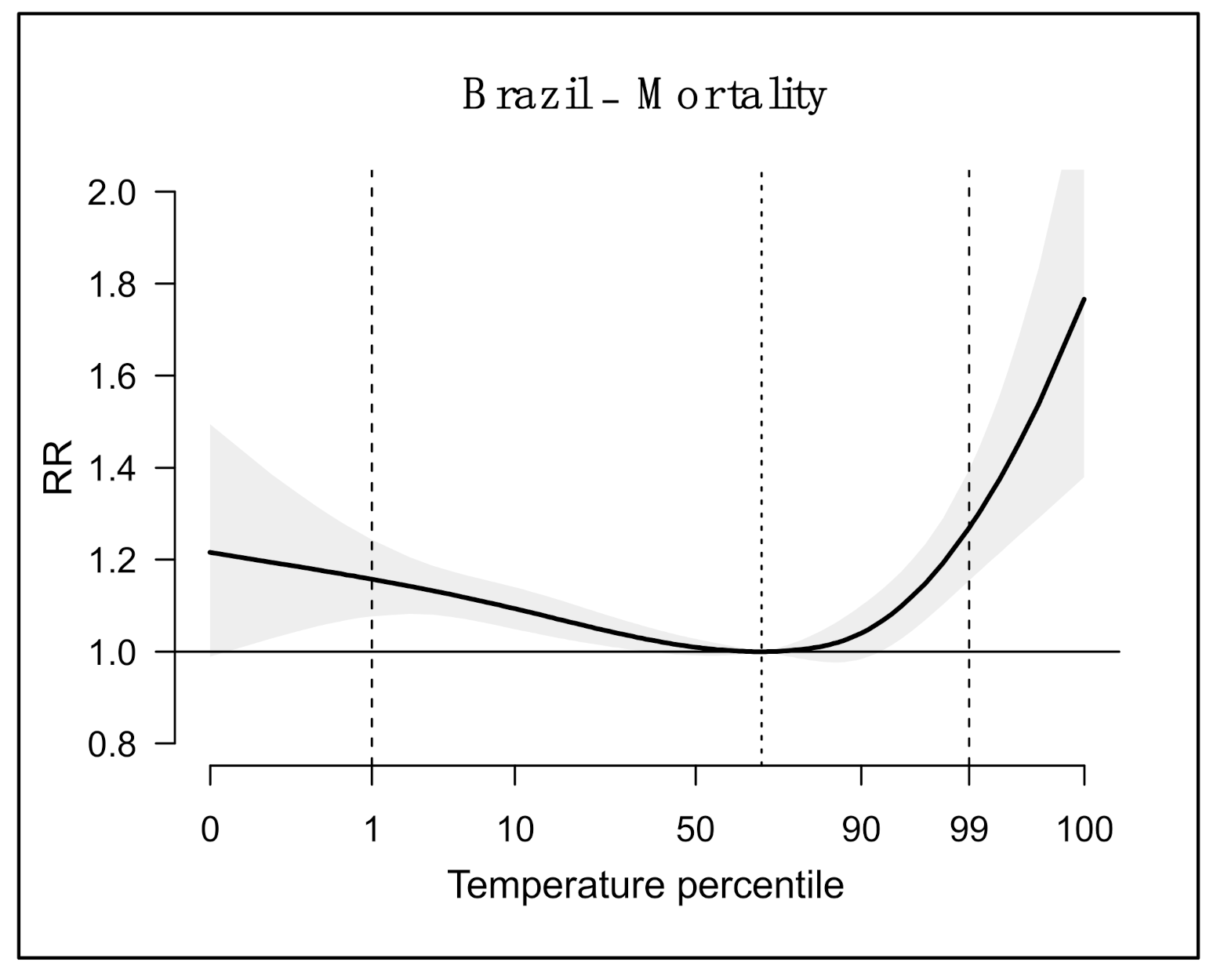
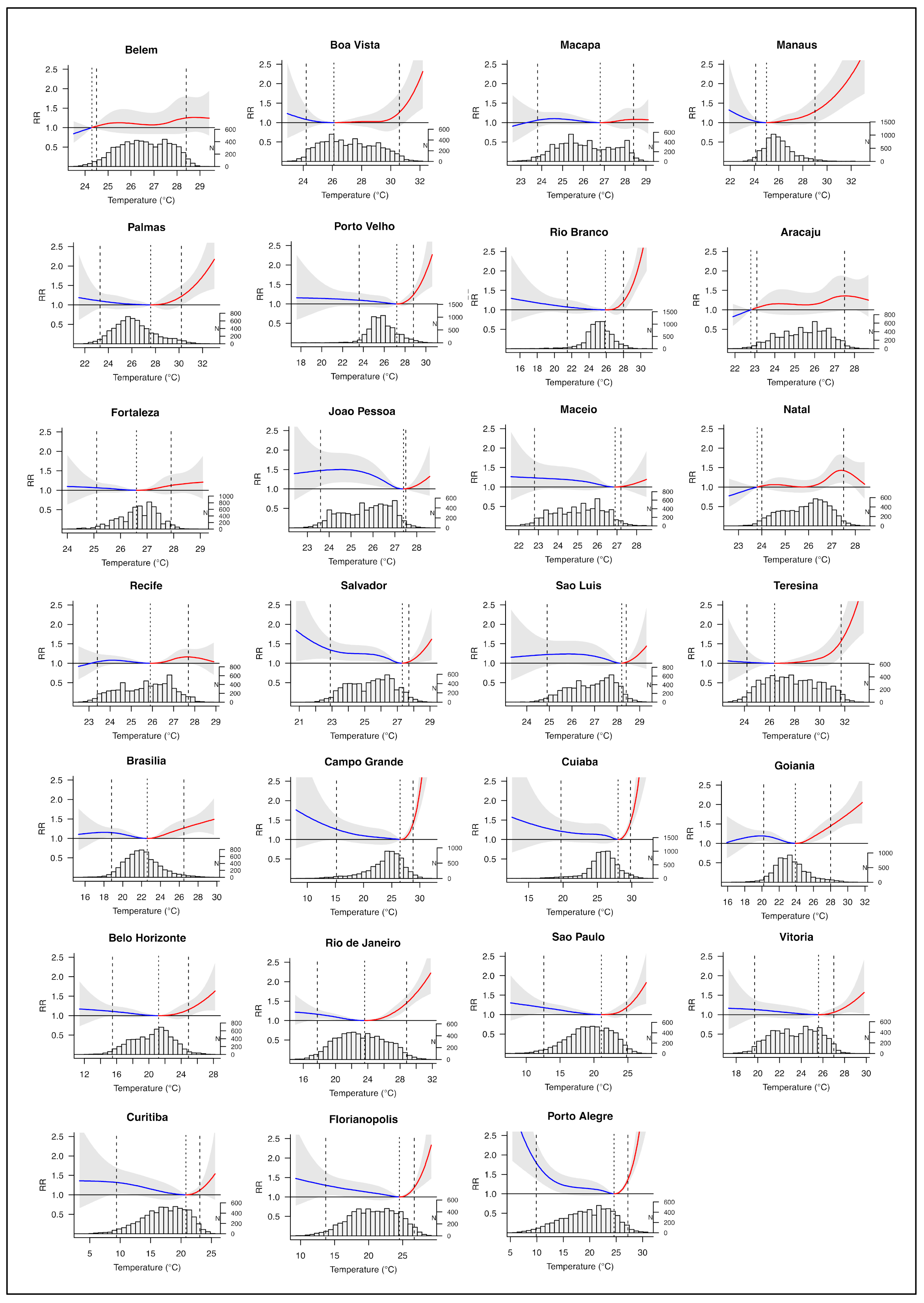
3. Results
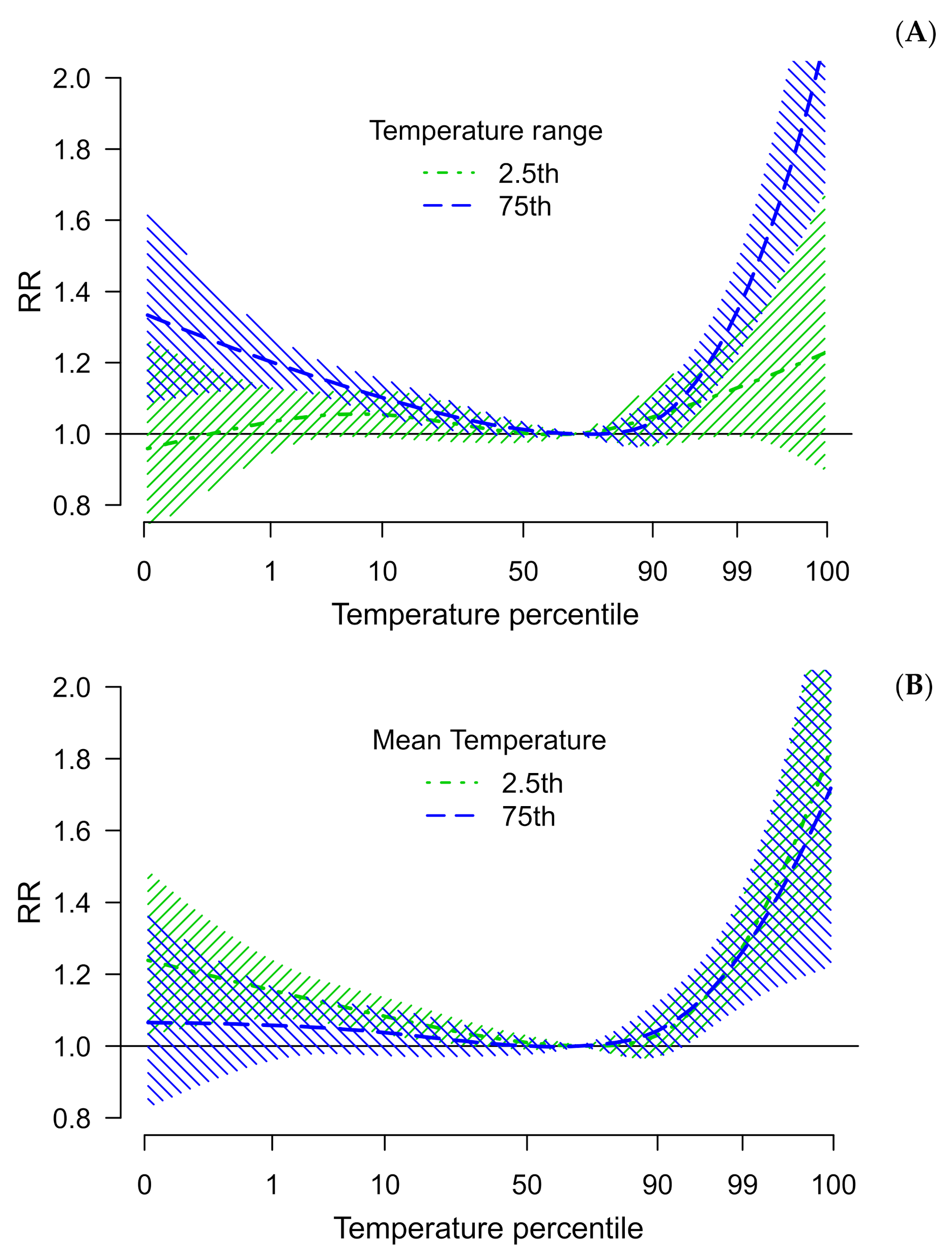
Sensitivity Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rossati, A. Global Warming and Its Health Impact. Int. J. Occup. Environ. Med. 2017, 8, 7–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- IPCC. Global Warming of 1.5 °C. An IPCC Special Report on The Impacts of Global Warming of 1.5 °C above Pre-Industrial Levels and Related Global Greenhouse Gas Emission Pathways, in The Context of Strengthening The Global Response to The Threat of Climate Change, Sustainable Development, And Efforts To Eradicate Poverty; Masson-Delmotte, V., Zhai, P., Pörtner, H.-O., Roberts, D., Skea, J., Shukla, P.R., Pirani, A., Moufouma-Okia, W., Péan, C., Pidcock, R., et al., Eds.; IPCC: Geneva, Switzerland, 2018; Available online: https://www.ipcc.ch/sr15/download/#full (accessed on 3 May 2021).
- De Sousa, T.C.M.; Amancio, F.; Hacon, S.D.S.; Barcellos, C. Doenças sensíveis ao clima no Brasil e no mundo: Revisão sistemática. Rev. Panam. Salud Pública 2018, 42, e85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gasparrini, A.; Armstrong, B.; Kovats, S.; Wilkinson, P. The effect of high temperatures on cause-specific mortality in England and Wales. Occup. Environ. Med. 2011, 69, 56–61. [Google Scholar] [CrossRef] [PubMed]
- Zanobetti, A.; O’Neill, M.S. Longer-Term Outdoor Temperatures and Health Effects: A Review. Curr. Epidemiol. Rep. 2018, 5, 125–139. [Google Scholar] [CrossRef]
- Antunes, L.; Silva, S.P.; Marques, J.; Nunes, B.; Antunes, S. The effect of extreme cold temperatures on the risk of death in the two major Portuguese cities. Int. J. Biometeorol. 2016, 61, 127–135. [Google Scholar] [CrossRef]
- Fuhrmann, C.M.; Sugg, M.M.; Konrad, C.E.; Waller, A. Impact of Extreme Heat Events on Emergency Department Visits in North Carolina (2007–2011). J. Community Health 2015, 41, 146–156. [Google Scholar] [CrossRef]
- Han, J.; Liu, S.; Zhang, J.; Zhou, L.; Fang, Q.; Zhang, J.; Zhang, Y. The impact of temperature extremes on mortality: A time-series study in Jinan, China. BMJ Open 2017, 7, e014741. [Google Scholar] [CrossRef]
- Son, J.-Y.; Liu, J.C.; Bell, M.L. Temperature-related mortality: A systematic review and investigation of effect modifiers. Environ. Res. Lett. 2019, 14, 073004. [Google Scholar] [CrossRef]
- Bunker, A.; Wildenhain, J.; Vandenbergh, A.; Henschke, N.; Rocklöv, J.; Hajat, S.; Sauerborn, R. Effects of Air Temperature on Climate-Sensitive Mortality and Morbidity Outcomes in the Elderly; a Systematic Review and Meta-analysis of Epidemiological Evidence. EBioMedicine 2016, 6, 258–268. [Google Scholar] [CrossRef] [Green Version]
- Yu, W.; Mengersen, K.; Wang, X.; Ye, X.; Guo, Y.; Pan, X.; Tong, S. Daily average temperature and mortality among the elderly: A meta-analysis and systematic review of epidemiological evidence. Int. J. Biometeorol. 2011, 56, 569–581. [Google Scholar] [CrossRef] [Green Version]
- Gouveia, N.; Hajat, S.; Armstrong, B. Socioeconomic differentials in the temperature–mortality relationship in São Paulo, Brazil. Int. J. Epidemiol. 2003, 32, 390–397. [Google Scholar] [CrossRef] [Green Version]
- Silva, E.N.; Ribeiro, H. Impact of urban atmospheric environment on hospital admissions in the elderly. Rev. Saude Publica 2002, 46, 694–701. [Google Scholar] [CrossRef] [Green Version]
- Pinheiro, S.D.L.L.D.A.; Saldiva, P.H.N.; Schwartz, J.; Zanobetti, A. Isolated and synergistic effects of PM10 and average temperature on cardiovascular and respiratory mortality. Rev. Saúde Pública 2014, 48, 881–888. [Google Scholar] [CrossRef] [Green Version]
- Chou, S.C.; Lyra, A.D.A.; Mourão, C.; Dereczynski, C.P.; Pilotto, I.L.; Gomes, J.; Bustamante, J.; Tavares, P.; Silva, A.; Rodrigues, D.; et al. Assessment of Climate Change over South America under RCP 4.5 and 8.5 Downscaling Scenarios. Am. J. Clim. Chang. 2014, 3, 512–527. [Google Scholar] [CrossRef] [Green Version]
- Sanches, F.; Verdum, R.; Fisch, G.; Gass, S.L.B.; Rocha, V.M. Extreme Rainfall Events in the Southwest of Rio Grande do Sul (Brazil) and Its Association with the Sandization Process. Am. J. Clim. Chang. 2019, 8, 441–453. [Google Scholar] [CrossRef] [Green Version]
- De Carvalho, A.A.; Montenegro, A.A.D.A.; Da Silva, H.P.; Lopes, I.; De Morais, J.E.F.; Da Silva, T.G.F. Trends of rainfall and temperature in Northeast Brazil. Rev. Bras. Eng. Agrícola Ambient. 2020, 24, 15–23. [Google Scholar] [CrossRef] [Green Version]
- Gasparrini, A.; Guo, Y.; Hashizume, M.; Lavigne, E.; Zanobetti, A.; Schwartz, J.; Tobias, A.; Tong, S.; Rocklöv, J.; Forsberg, B.; et al. Mortality risk attributable to high and low ambient temperature: A multicountry observational study. Lancet 2015, 386, 369–375. [Google Scholar] [CrossRef]
- Silveira, I.H.; Oliveira, B.F.A.; Cortes, T.R.; Junger, W.L. The effect of ambient temperature on cardiovascular mortality in 27 Brazili-an cities. Sci. Total Environ. 2019, 691, 996–1004. [Google Scholar] [CrossRef]
- Dee, D.P.; Uppala, S.M.; Simmons, A.J.; Berrisford, P.; Poli, P.; Kobayashi, S.; Andrae, U.; Balmaseda, M.A.; Balsamo, G.; Bauer, P.; et al. The ERA-Interim reanalysis: Configuration and performance of the data assimilation system. Q. J. R. Meteorol. Soc. 2011, 137, 553–597. [Google Scholar] [CrossRef]
- Gasparrini, A. Distributed lag linear and non-linear models in R: The package dlnm. J. Stat. Softw. 2011, 43, 1–20. Available online: http://www.jstatsoft.org/v43/i08/ (accessed on 3 May 2021). [CrossRef] [Green Version]
- Peng, R.D.; Dominici, F.; Louis, T.A. Model choice in time series studies of air pollution and mortality. J. R. Stat. Soc. Ser. A Stat. Soc. 2006, 169, 179–203. [Google Scholar] [CrossRef] [Green Version]
- Gasparrini, A.; Armstrong, B.; Kenward, M.G. Multivariate meta-analysis for non-linear and other multi-parameter associations. Stat. Med. 2012, 31, 3821–3839. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing, Vienna, Austria. 2013. Available online: http://www.R-project.org/ (accessed on 11 March 2021).
- Carreras, H.; Zanobetti, A.; Koutrakis, P. Effect of daily temperature range on respiratory health in Argentina and its modification by impaired socio-economic conditions and PM10 exposures. Environ. Pollut. 2015, 206, 175–182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, S.; Insaf, T.Z.; Luo, M.; Hwang, S.-A. The effects of ambient temperature variation on respiratory hospitalizations in summer, New York State. Int. J. Occup. Environ. Health 2012, 18, 188–197. [Google Scholar] [CrossRef] [PubMed]
- Michelozzi, P.; Accetta, G.; De Sario, M.; D’Ippoliti, D.; Marino, C.; Baccini, M.; Biggeri, A.; Anderson, H.R.; Katsouyanni, K.; Ballester, F.; et al. High Temperature and Hospitalizations for Cardiovascular and Respiratory Causes in 12 European Cities. Am. J. Respir. Crit. Care Med. 2009, 179, 383–389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, Y.-K.; Ho, T.-J.; Wang, Y.-C. Mortality risk associated with temperature and prolonged temperature extremes in elderly populations in Taiwan. Environ. Res. 2011, 111, 1156–1163. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Breitner, S.; Pan, X.; Franck, U.; Leitte, A.M.; Wiedensohler, A.; Von Klot, S.; Wichmann, H.-E.; Peters, A.; Schneider, A. Associations between air temperature and cardio-respiratory mortality in the urban area of Beijing, China: A time-series analysis. Environ. Health 2011, 10, 51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Basu, R. High ambient temperature and mortality: A review of epidemiologic studies from 2001 to 2008. Environ. Health 2009, 8, 40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ye, X.; Wolff, R.; Yu, W.; Vaneckova, P.; Pan, X.; Tong, S. Ambient temperature and morbidity: A review of epidemiological evi-dence. Environ. Health Perspect. 2012, 120, 19–28. [Google Scholar] [CrossRef] [Green Version]
- Zhao, Q.; Li, S.; Coelho, M.D.S.Z.S.; Saldiva, P.H.N.; Xu, R.; Huxley, R.R.; Abramson, M.J.; Guo, Y. Ambient heat and hospitalisation for COPD in Brazil: A nationwide case-crossover study. Thorax 2019, 74, 1031–1036. [Google Scholar] [CrossRef]
- Marandola, E., Jr.; Hogan, D.J. Vulnerabilidade do lugar vs. vulnerabilidade sociodemográfica: Implicações metodológicas de uma velha questão. Rev. Bras. Estud. Popul. 2009, 26, 161–181. [Google Scholar]
- Hacon, S.; Barcellos, C.; Xavier, D.R.; Gracie, R.; Oliveira, B.F.A.; Artaxo, P.; Ignotti, E. Capítulo 5: Saúde. Mudanças Climáticas em Rede: Um Olhar Interdisciplinar; Nobre, C.A., Marengo, J.A., Eds.; INCT: São José dos Campos, SP, Brazil, 2016. [Google Scholar]
- IBGE. Pesquisa Nacional de Saúde: 2013: Ciclos de Vida: Brasil e Grandes Regiões/IBGE, Coordenação deTrabalho e Rendimento; IBGE: Rio de Janeiro, Brazil, 2015.
- Stopa, S.R.; Malta, D.C.; Monteiro, C.N.; Szwarcwald, C.L.; Goldbaum, M.; Galvão Cesar, C.L. Use of and access to health services in Brazil, 2013 National Health Survey. Rev. Saude Publica 2017, 51, 3s. [Google Scholar] [CrossRef]
- da Silveira, D.P.; Araujo, D.V.; Gomes, G.H.G.; Lima, K.C.; Estrella, K.; Oliveira, M.; Veras, R.; Neves, R.V.d.; Assalim, V.M. Idoso Na Saúde Suplementar: Uma Urgência Para A Saúde da Sociedade e Para A Sustentabilidade do Setor. Rio de Janeiro: Agência Nacional de Saúde Suplementar. 2016. Available online: http://www.ans.gov.br/images/stories/Materiais_para_pesquisa/Materiais_por_assunto/web_final_livro_idosos.pdf (accessed on 13 July 2020).
- Buckley, J.P.; Samet, J.M.; Richardson, D.B. Does air pollution confound studies of temperature? Epidemiology 2014, 25, 242–245. [Google Scholar] [CrossRef]
- O’Neill, M.S.; Hajat, S.; Zanobetti, A.; Ramirez-Aguilar, M.; Schwartz, J. Impact of control for air pollution and respiratory epidem-ics on the estimated associations of temperature and daily mortality. Int. J. Biometeorol. 2005, 50, 121–129. [Google Scholar] [CrossRef] [Green Version]
- Anderson, G.B.; Dominici, F.; Wang, Y.; McCormack, M.C.; Bell, M.L.; Peng, R.D. Heat-related Emergency Hospitalizations for Respiratory Diseases in the Medicare Population. Am. J. Respir. Crit. Care Med. 2013, 187, 1098–1103. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cities | Total Deaths (n) | Temperature (°C) | |||||
|---|---|---|---|---|---|---|---|
| Average | Minimum | P25 | P50 | P75 | Maximum | ||
| Midwest | |||||||
| Brasilia | 12,510 | 22.1 | 15.3 | 20.8 | 21.9 | 23.15 | 29.7 |
| Campo Grande | 7544 | 23.9 | 8.0 | 22.3 | 24.5 | 26.0 | 32.1 |
| Cuiaba | 4011 | 25.8 | 12.6 | 24.8 | 25.9 | 27.1 | 32.3 |
| Goiânia | 11,932 | 23.4 | 15.9 | 22.1 | 23.2 | 24.4 | 31.7 |
| North | |||||||
| Belem | 15,569 | 26.6 | 23.5 | 25.8 | 26.6 | 27.5 | 29.4 |
| Boa Vista | 970 | 27.2 | 22.9 | 25.7 | 27.0 | 28.6 | 32.2 |
| Macapa | 1463 | 26.1 | 22.6 | 25.1 | 26.0 | 27.2 | 29.1 |
| Manaus | 8628 | 26.0 | 21.9 | 25.2 | 25.8 | 26.7 | 33.1 |
| Palmas | 593 | 26.2 | 21.5 | 25.0 | 26.0 | 27.2 | 33.0 |
| Porto Velho | 2344 | 25.9 | 17.6 | 25.0 | 25.7 | 26.6 | 30.6 |
| Rio Branco | 2568 | 25.1 | 15.0 | 24.4 | 25.2 | 26.1 | 30.7 |
| Northeast | |||||||
| Aracaju | 3735 | 25.4 | 21.9 | 24.5 | 25.6 | 26.4 | 28.7 |
| Fortaleza | 19,315 | 26.7 | 24.0 | 26.2 | 26.8 | 27.2 | 29.1 |
| João Pessoa | 6199 | 25.7 | 22.4 | 24.8 | 25.9 | 26.6 | 28.6 |
| Maceió | 7115 | 25.1 | 21.6 | 24.1 | 25.2 | 26 | 28.5 |
| Natal | 6176 | 25.9 | 22.6 | 25.1 | 26.1 | 26.7 | 28.4 |
| Recife | 16,599 | 25.7 | 22.5 | 24.7 | 25.8 | 26.6 | 28.9 |
| Salvador | 19,442 | 25.4 | 20.8 | 24.3 | 25.5 | 26.5 | 29.1 |
| São Luis | 5602 | 26.9 | 23.3 | 26.1 | 27.0 | 27.7 | 29.3 |
| Teresina | 5686 | 27.8 | 22.7 | 26.1 | 27.7 | 29.5 | 33.5 |
| South | |||||||
| Curitiba | 13,175 | 17.3 | 3.3 | 14.9 | 17.6 | 20.1 | 25.6 |
| Florianopolis | 2651 | 20.7 | 9.3 | 18.2 | 20.8 | 23.5 | 29.2 |
| Porto Alegre | 14,888 | 19.5 | 5.4 | 16.3 | 20.0 | 23.2 | 31.0 |
| Southeast | |||||||
| Belo Horizonte | 20,274 | 20.4 | 11.4 | 18.5 | 20.7 | 22.2 | 28.2 |
| Rio de Janeiro | 90,887 | 23.2 | 15.0 | 20.8 | 23.0 | 25.5 | 31.8 |
| São Paulo | 121,459 | 19.4 | 7.7 | 17.3 | 19.6 | 21.8 | 27.7 |
| Vitória | 1307 | 23.5 | 17.3 | 21.8 | 23.6 | 25.2 | 29.8 |
| Brazil | 422,642 | 24.3 | 3.3 | 22.9 | 25.2 | 26.6 | 33.5 |
| Cities | MMT | Total | Cold | Heat | ||||
|---|---|---|---|---|---|---|---|---|
| % | °C | AF% | (95% IC) | AF% | (95% IC) | AF% | (95% IC) | |
| Midwest | ||||||||
| Brasília | 65 | 22.6 | 6.02 | (1.56, 10.09) | 3.4 | (−0.22, 6.47) | 2.62 | (0.18, 4.77) |
| Campo Grande | 81 | 26.5 | 6.84 | (−5.48, 16.66) | 4.64 | (−7.29, 14.88) | 2.2 | (1.07, 3.20) |
| Cuiabá | 87 | 28.0 | 10.69 | (−5.56, 22.69) | 8.35 | (−8.05, 21.53) | 2.34 | (1.57, 3.02) |
| Goiânia | 66 | 23.9 | 8.08 | (3.47, 12.76) | 4.33 | (1.05, 7.54) | 3.75 | (1.84, 5.60) |
| North | ||||||||
| Belém | 1 | 24.3 | 10.06 | (−18.81, 29.89) | −0.05 | (−0.16, 0.04) | 10.11 | (−15.26, 29.90) |
| Boa Vista | 33 | 26.1 | 3.55 | (−5.85, 11.54) | 0.85 | (−2.67, 3.7) | 2.7 | (−6.78, 9.49) |
| Macapá | 67 | 26.8 | 5.15 | (−0.42, 10.77) | 4.00 | (−3.48, 10.5) | 1.15 | (−3.38, 4.97) |
| Manaus | 18 | 25 | 4.55 | (−2.50, 10.8) | 0.22 | (−0.35, 0.81) | 4.33 | (−2.95, 10.51) |
| Palmas | 80 | 27.6 | 4.12 | (−3.30, 10.84) | 2.46 | (−6.66, 10.78) | 1.66 | (−1.07, 3.98) |
| Porto Velho | 85 | 27.2 | 5.11 | (−4.64, 13.45) | 3.77 | (−7.4, 14.27) | 1.34 | (0.33, 2.31) |
| Rio Branco | 70 | 25.9 | 2.73 | (−1.68, 6.37) | 1.01 | (−2.98, 4.77) | 1.72 | (−1.7, 4.60) |
| Northeast | ||||||||
| Aracajú | 1 | 22.8 | 14.55 | (−9.66, 33.21) | −0.05 | (−0.14, 0.03) | 14.6 | (−11.5, 32.00) |
| Fortaleza | 38 | 26.6 | 2.91 | (−2.55, 7.63) | 0.87 | (−1.34, 2.93) | 2.05 | (−3.04, 6.2) |
| Joao Pessoa | 96 | 27.4 | 22.95 | (8.94, 34.16) | 22.84 | (8.64, 34.79) | 0.11 | (−0.14, 0.31) |
| Maceió | 95 | 26.9 | 11.53 | (−6.16, 25.75) | 11.44 | (−6.32, 25.42) | 0.09 | (−0.25, 0.37) |
| Natal | 1 | 23.8 | 9.3 | (−7.37, 22.18) | −0.06 | (−0.17, 0.05) | 9.36 | (−6.25, 21.97) |
| Recife | 52 | 25.9 | 4.96 | (0.54, 8.81) | 2.12 | (−1.4, 5.59) | 2.84 | (−0.93, 6.31) |
| Salvador | 93 | 27.3 | 15.25 | (5.04, 24.57) | 14.92 | (4.09, 23.28) | 0.33 | (0.01, 0.63) |
| Sao Luís | 93 | 28.2 | 12.86 | (−3.51, 25.64) | 12.61 | (−4.67, 25.18) | 0.25 | (−0.14, 0.63) |
| Teresina | 29 | 26.4 | 6.85 | (−2.11, 14.35) | 0.28 | (−2.79, 2.91) | 6.57 | (−1.37, 13.41) |
| South | ||||||||
| Curitiba | 82 | 20.8 | 9.8 | (−4.12, 21.13) | 9.14 | (−4.05, 21.25) | 0.66 | (−0.18, 1.43) |
| Florianopolis | 84 | 24.5 | 11.24 | (−0.58, 22.22) | 9.82 | (−2.68, 20.63) | 1.41 | (0.82, 1.97) |
| Porto Alegre | 86 | 24.6 | 16.36 | (4.41, 26.63) | 14.65 | (1.88, 25.19) | 1.70 | (1.26, 2.08) |
| Southeast | ||||||||
| Belo Horizonte | 58 | 21.2 | 3.7 | (−1.20, 8.01) | 2.33 | (−1.43, 6.12) | 1.37 | (−1.74, 3.99) |
| Rio de Janeiro | 56 | 23.6 | 7.91 | (4.56, 10.99) | 3.33 | (0.83, 5.6) | 4.57 | (2.31, 6.45) |
| São Paulo | 67 | 21.1 | 4.99 | (1.07, 8.59) | 3.64 | (−0.84, 7.72) | 1.35 | (−0.89, 3.55) |
| Vitória | 81 | 25.6 | 4.71 | (−4.75, 12.65) | 4.25 | (−5.89, 13.88) | 0.46 | (−0.68, 1.5) |
| Brazil | 67 * | 25.9 * | 7.54 | (5.36, 9.21) | 4.69 | (2.94, 6.17) | 2.84 | (1.45, 3.95) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jacobson, L.d.S.V.; Oliveira, B.F.A.d.; Schneider, R.; Gasparrini, A.; Hacon, S.d.S. Mortality Risk from Respiratory Diseases Due to Non-Optimal Temperature among Brazilian Elderlies. Int. J. Environ. Res. Public Health 2021, 18, 5550. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115550
Jacobson LdSV, Oliveira BFAd, Schneider R, Gasparrini A, Hacon SdS. Mortality Risk from Respiratory Diseases Due to Non-Optimal Temperature among Brazilian Elderlies. International Journal of Environmental Research and Public Health. 2021; 18(11):5550. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115550
Chicago/Turabian StyleJacobson, Ludmilla da Silva Viana, Beatriz Fátima Alves de Oliveira, Rochelle Schneider, Antonio Gasparrini, and Sandra de Souza Hacon. 2021. "Mortality Risk from Respiratory Diseases Due to Non-Optimal Temperature among Brazilian Elderlies" International Journal of Environmental Research and Public Health 18, no. 11: 5550. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115550