
Know-Me: A Toolkit for Designing Personalised Dementia Care



Abstract
:1. Introduction
1.1. Related Work
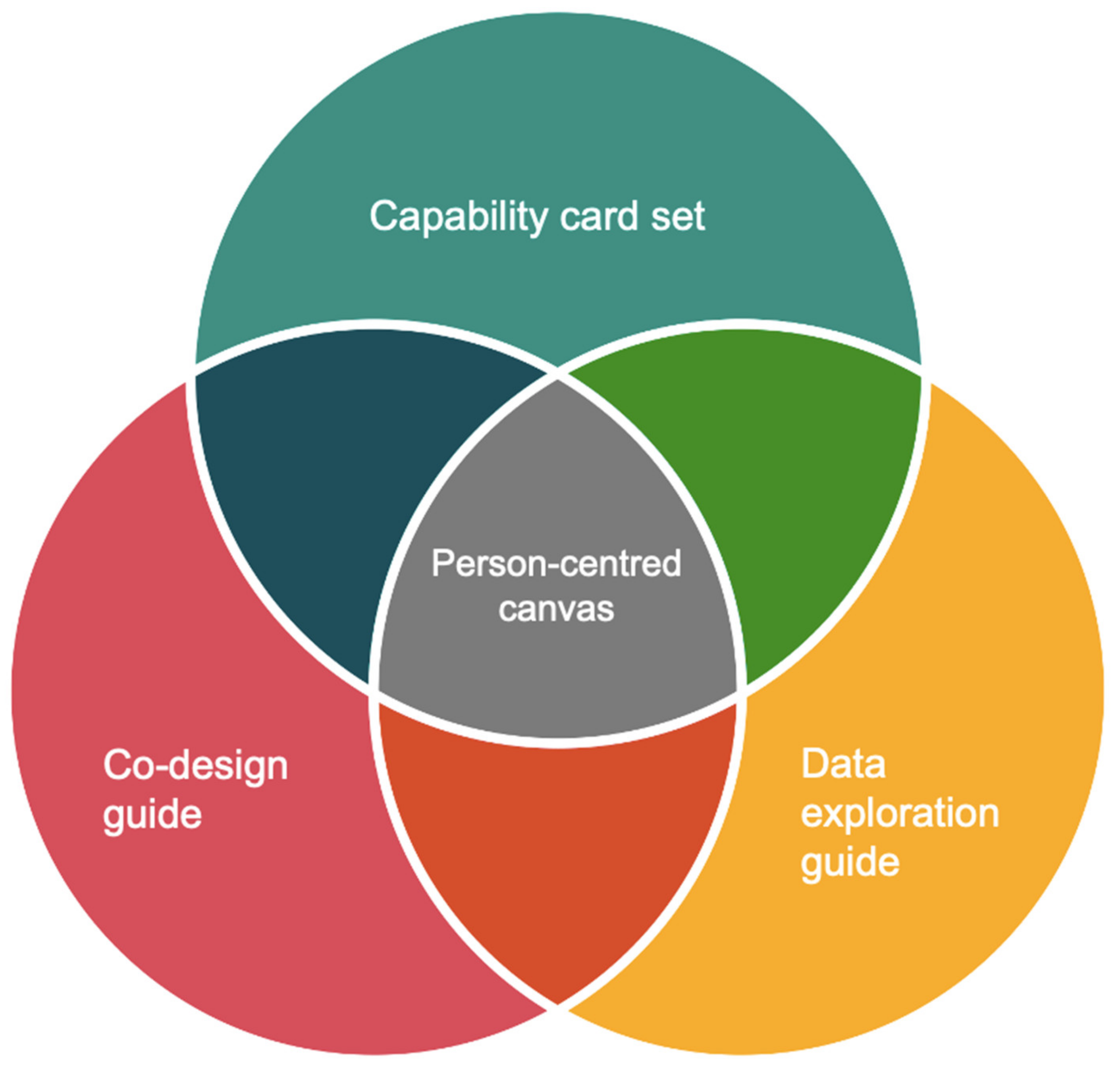
1.2. The Know-Me Toolkit
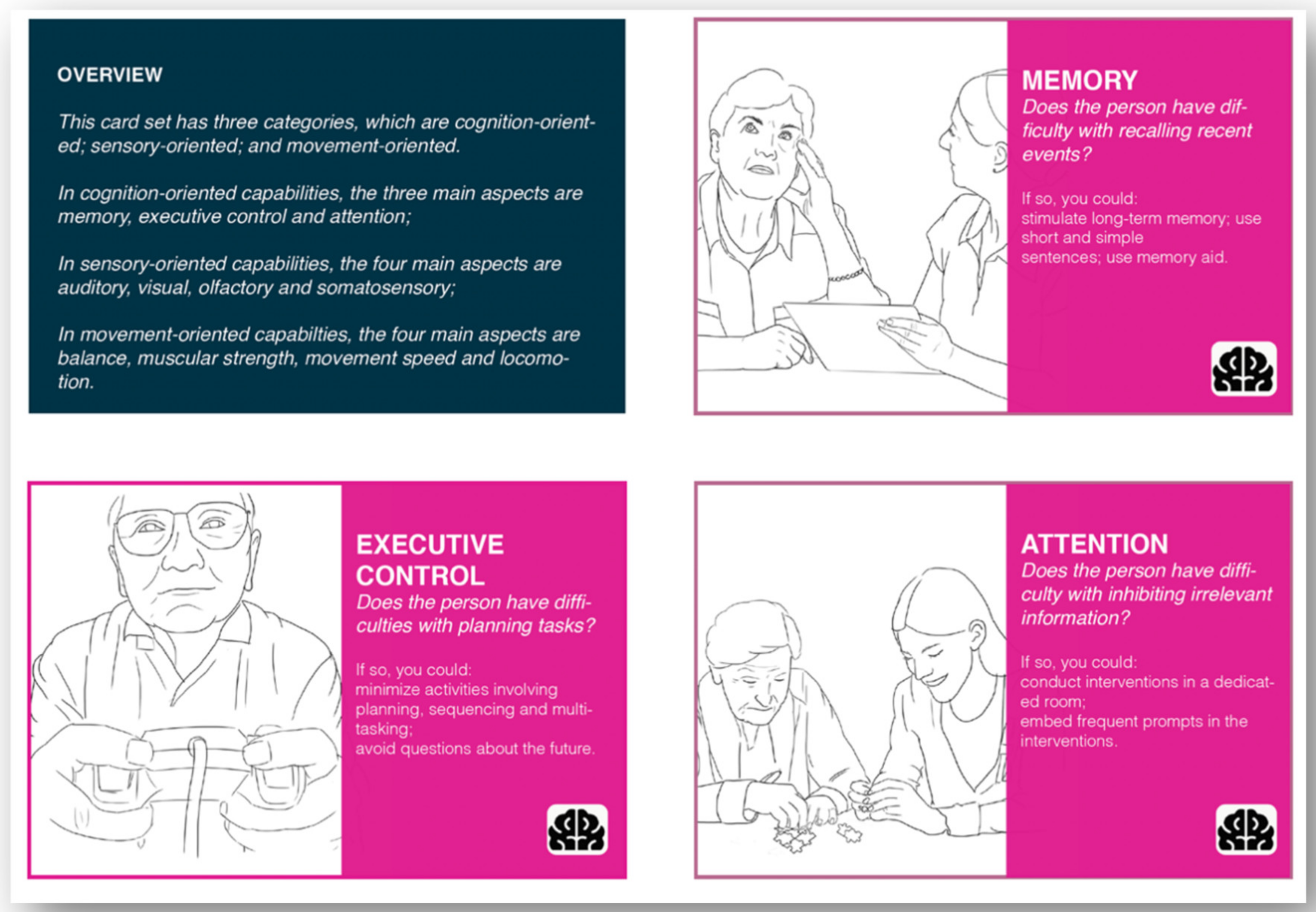
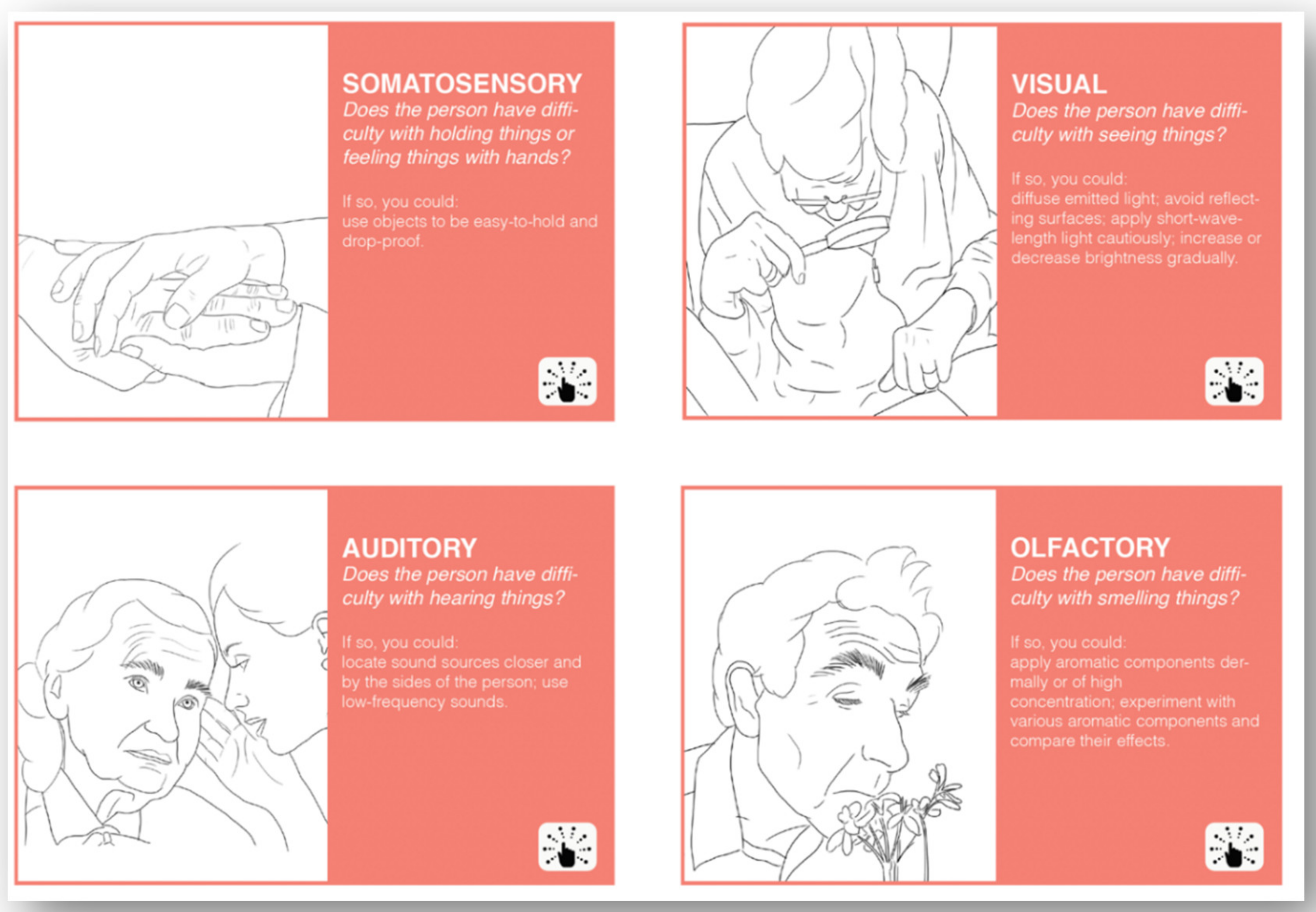
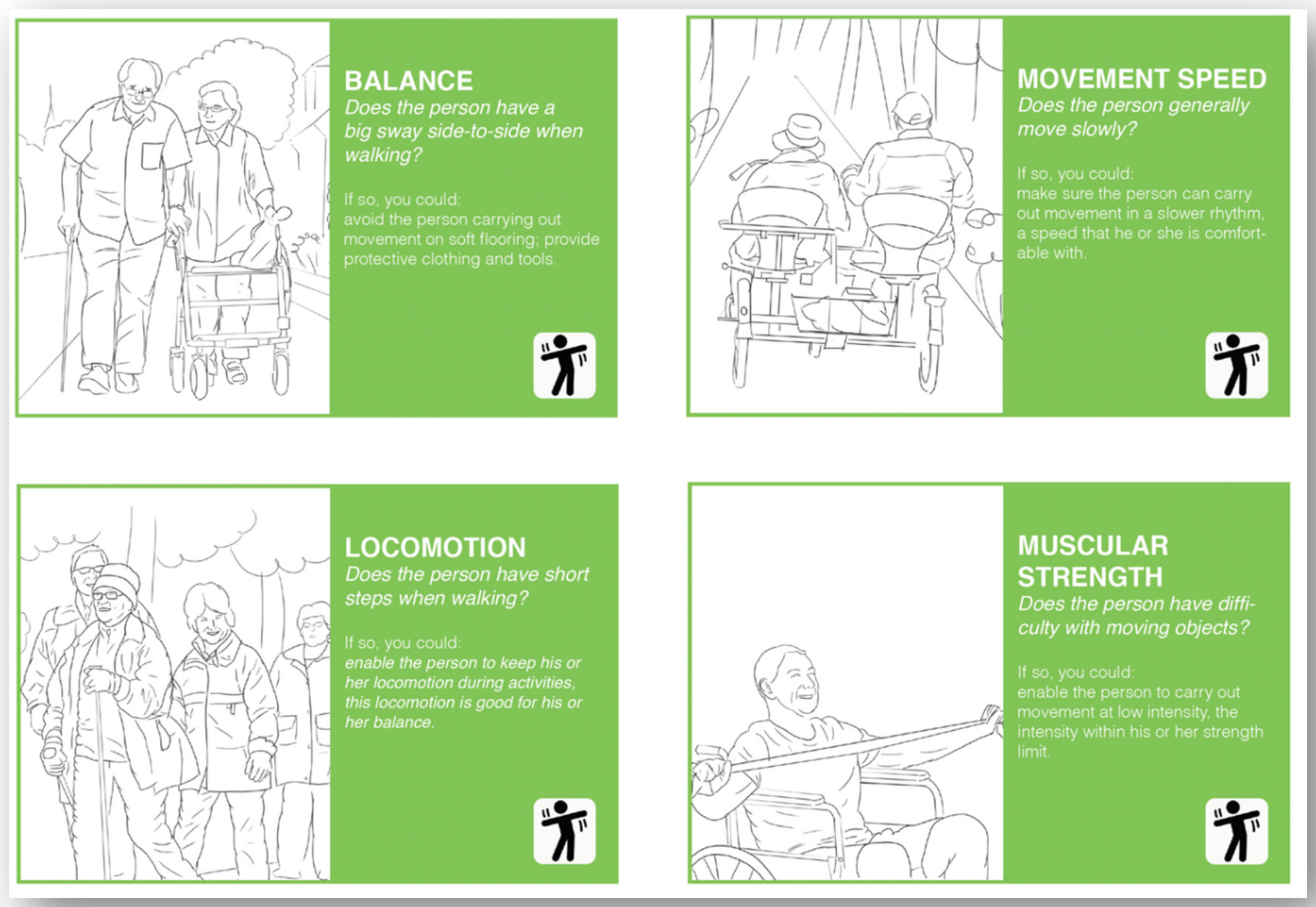
1.2.1. Capability Card Set
1.2.2. Co-Design Guide
1.2.3. Data Exploration Guide
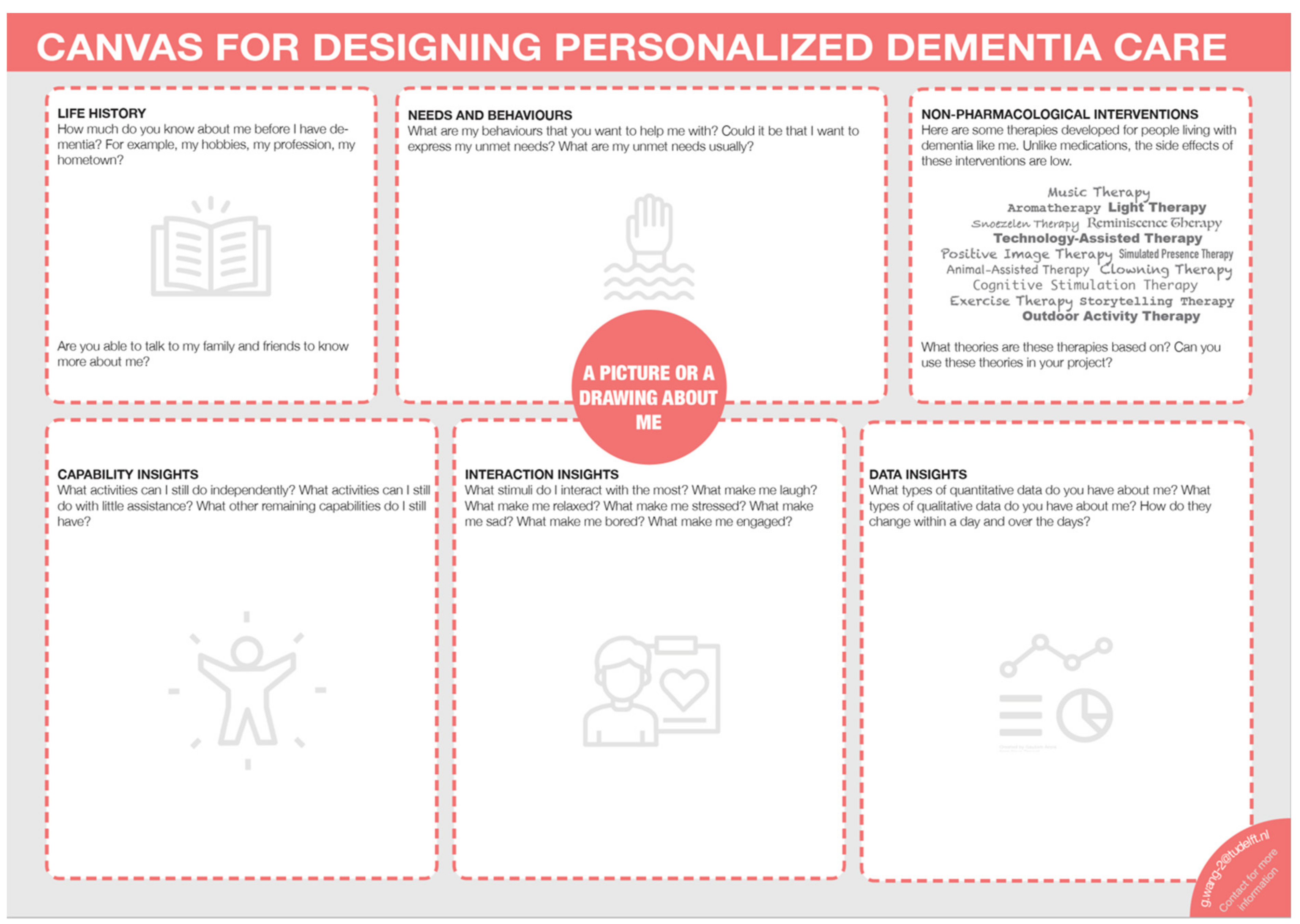
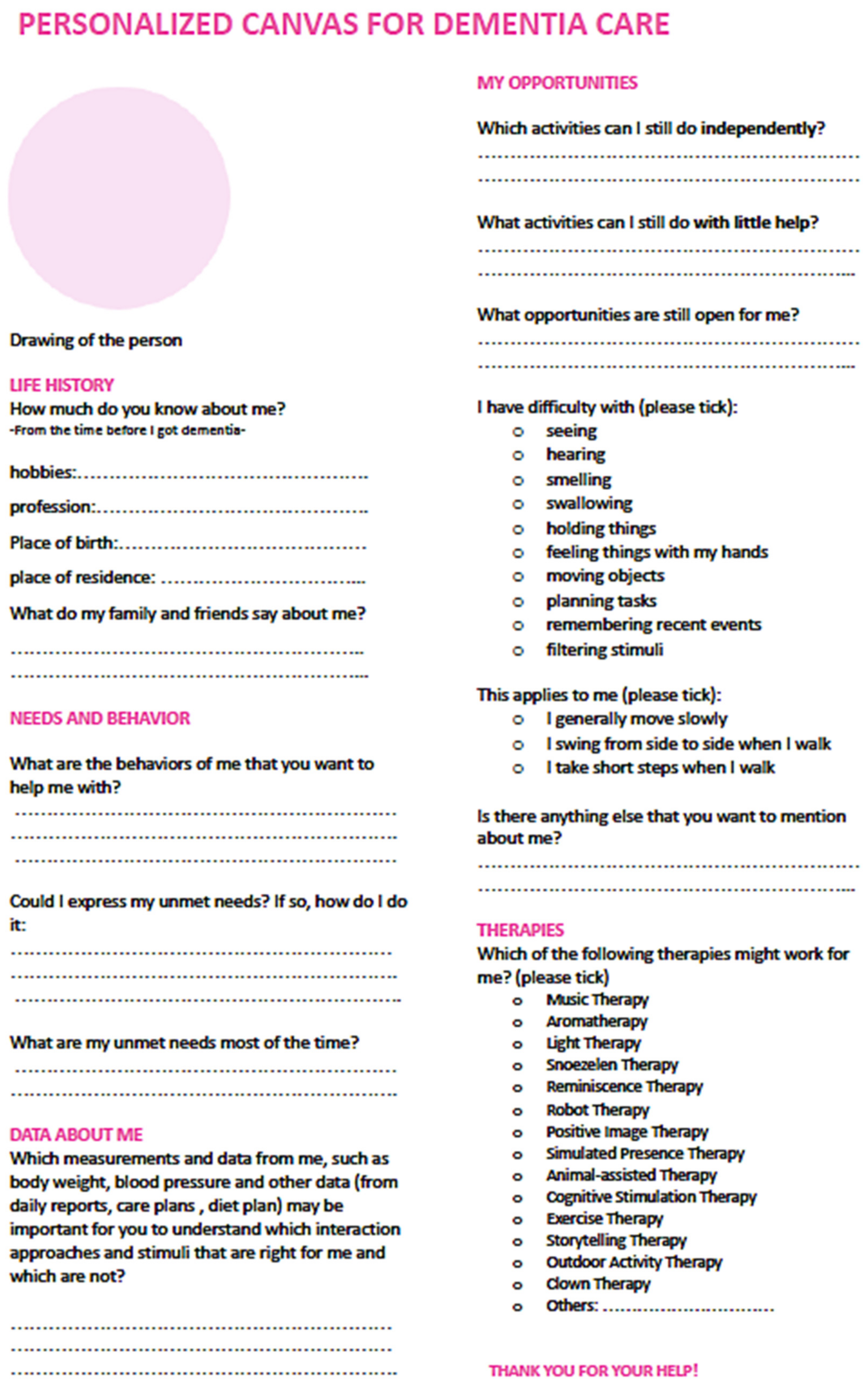
1.2.4. Person-Centred Canvas
1.2.5. User Manual
1.3. Aims and Objectives
- What is the perceived usefulness of this toolkit?
- What are the desired improvements for this toolkit?
2. Materials and Methods
2.1. Context
2.2. Procedure
3. Results
4. Discussion
4.1. Main Findings
4.2. Comparisons with State-of-the-Art Toolkits
4.3. Limitations
4.4. Future Work
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organisation. WHO|Global Action Plan on the Public Health Response to Dementia 2017–2025; World Health Organization: Geneva, Switzerland, 2017; Available online: http://www.who.int/mental_health/neurology/dementia/action_plan_2017_2025/en/ (accessed on 13 January 2021).
- World Health Organisation. Dementia. Available online: https://www.who.int/news-room/fact-sheets/detail/dementia (accessed on 30 July 2020).
- Alzheimer’s Association. 2020 Alzheimer’s disease facts and figures. Alzheimer’s Dement. 2020, 16, 391–460. [Google Scholar] [CrossRef] [PubMed]
- Kitwood, T.M. Dementia Reconsidered: The Person Comes First, 1st ed.; Open University Press: Hong Kong, China, 1997. [Google Scholar]
- Sheth, A.; Jaimini, U.; Thirunarayan, K.; Banerjee, T. Augmented personalized health: How smart data with IoTs and AI is about to change healthcare. In Proceedings of the RTSI 2017-IEEE 3rd International Forum on Research and Technologies for Society and Industry, Modena, Italy, 11–13 September 2017; Volume 2017. [Google Scholar] [CrossRef]
- Backonja, U.; Haynes, S.C.; Kim, K.K. Data Visualizations to Support Health Practitioners’ Provision of Personalized Care for Patients With Cancer and Multiple Chronic Conditions: User-Centered Design Study. JMIR Hum. Factors 2018, 5, e11826. [Google Scholar] [CrossRef] [PubMed]
- Korhonen, O.; Väyrynen, K.; Krautwald, T.; Bilby, G.; Broers, H.A.T.; Giunti, G.; Isomursu, M. Data-Driven Personalization of a Physiotherapy Care Pathway: Case Study of Posture Scanning. JMIR Rehabilitation Assist. Technol. 2020, 7, e18508. [Google Scholar] [CrossRef] [PubMed]
- Yeh, R.W.; Kramer, D.B. Decision Tools to Improve Personalized Care in Cardiovascular Disease. Circulation 2017, 135, 1097–1100. [Google Scholar] [CrossRef] [Green Version]
- Wang, H.; Zhao, Y.; Yu, L.; Liu, J.; Zwetsloot, I.M.; Cabrera, J.; Tsui, K.-L. A Personalized Health Monitoring System for Community-Dwelling Elderly People in Hong Kong: Design, Implementation, and Evaluation Study. J. Med Internet Res. 2020, 22, e19223. [Google Scholar] [CrossRef] [PubMed]
- Personalized Dementia Solutions Inc. Available online: https://dementiasolutions.ca/cdcp/ (accessed on 25 January 2021).
- Fazio, S.; Zimmerman, S.; Doyle, P.J.; Shubeck, E.; Carpenter, M.; Coram, P.; Klinger, J.H.; Jackson, L.; Pace, D.; Kallmyer, B.; et al. What Is Really Needed to Provide Effective, Person-Centered Care for Behavioral Expressions of Dementia? Guidance from The Alzheimer’s Association Dementia Care Provider Roundtable. J. Am. Med Dir. Assoc. 2020, 21, 1582–1586.e1. [Google Scholar] [CrossRef] [PubMed]
- Jais, C.; Hignett, S.; Hogervorst, E.; Habell, M. How Can Human Factors Be Used in the Design of Dementia Care Environments? How Can Human Factors & Ergonomics Be Used in the Design of Dementia-Care Environments? 2015. Available online: https://dspace.lboro.ac.uk/2134/18490 (accessed on 11 December 2017).
- Treadaway, C.; Fennell, J.; Taylor, A.; Kenning, G. Designing for playfulness through compassion: Design for advanced dementia. Des. Health 2019, 3, 1–21. [Google Scholar] [CrossRef]
- Designing for People with Dementia–MinD. Available online: https://designingfordementia.eu/ (accessed on 21 February 2021).
- Visual Diaries–Designing for People with Dementia. Available online: https://designingfordementia.eu/resources/mind-tools/visual-diaries (accessed on 26 January 2021).
- Visual Cards–Designing for People with Dementia. Available online: https://designingfordementia.eu/resources/mind-tools/visual-cards (accessed on 26 January 2021).
- Persona Toolkit–Designing for People with Dementia. Available online: https://designingfordementia.eu/resources/mind-tools/persona-toolkit (accessed on 26 January 2021).
- Treadaway, C.; Fennell, J.; Prytherch, D.; Kenning, G.; Prior, A.; Wlaters, A. How to Design for Advanced Dementia: A Toolkit for Designers; Cardiff Met Press: Cardiff, UK, 2018. [Google Scholar]
- Harvard Business Review. Digital Health Tools Offer New Opportunities for Personalized Care. Available online: https://hbr.org/2020/11/digital-health-tools-offer-new-opportunities-for-personalized-care (accessed on 23 January 2021).
- Wang, G.; Albayrak, A.; Molenbroek, J.; van der Cammen, T.J.M. Non-pharmacological Interventions for People with Dementia: Design Recommendations from an Ergonomics Perspective. In Proceedings of the 20th Congress of the International Ergonomics Association, Florence, Italy, 26–30 August 2018; pp. 112–122. [Google Scholar] [CrossRef] [Green Version]
- Wang, G.; Albayrak, A.; van der Cammen, T.J.M. Converting Wandering Behaviour into A Guided Activity. 2019. Available online: https://nbn-resolving.org/urn:nbn:de:bsz:14-qucosa2-365983 (accessed on 20 May 2021).
- Beck, E.; Obrist, M.; Bernhaupt, R.; Tscheligi, M. Instant Card Technique: How and Why to Apply in User-Centered Design. In Proceedings of the Tenth Conference on Participatory Design, Bloomington, IN, USA, 1–4 October 2008; pp. 162–165. Available online: https://www.researchgate.net/publication/221631209_Instant_card_technique_how_and_why_to_apply_in_user-centered_design (accessed on 14 January 2021).
- Wang, G.; Marradi, C.; Albayrak, A.; van der Cammen, T.J.M. Co-designing with people with dementia: A scoping review of involving people with dementia in design research. Maturitas 2019, 127, 55–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, G.; Gong, H.; Albayrak, A.; van der Cammen, T.J.M.; Kortuem, G. Personalising Management of Behavioural and Psychological Symptoms of Dementia in Nursing Homes: Exploring the Synergy of Quantitative and Qualitative Data. BioMed Res. Int. 2020, 2020, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Wang, G.; Albayrak, A.; Kortuem, G.; van der Cammen, T.J.M. A Digital Platform for Facilitating Personalized Dementia Care in Nursing Homes: A Formative Evaluation Study (Preprint). JMIR Form. Res. 2020. [Google Scholar] [CrossRef]
- Algase, D.L.; Beck, C.; Kolanowski, A.; Whall, A.; Berent, S.; Richards, K.; Beattie, E. Need-driven dementia-compromised behavior: An alternative view of disruptive behavior. Am. J. Alzheimer’s Dis. 1996, 11, 10–19. [Google Scholar] [CrossRef]
- Wang, G.; Albayrak, A.; van der Cammen, T.J.M. A systematic review of non-pharmacological interventions for BPSD in nursing home residents with dementia: From a perspective of ergonomics. Int. Psychogeriatr. 2019, 31, 1137–1149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steinberg, M.; Shao, H.; Zandi, P.; Lyketsos, C.G.; Welsh-Bohmer, K.A.; Norton, M.C.; Breitner, J.C.; Steffens, D.C.; Tschanz, J.T. Cache County Investigators Point and 5-year period prevalence of neuropsychiatric symptoms in dementia: The Cache County Study. Int. J. Geriatr. Psychiatry 2007, 23, 170–177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Treadaway, C. Personalization and Compassionate Design. In HCI and Design in the Context of Dementia. Human–Computer Interaction Series, 1st ed.; Brankaert, R., Kenning, G., Eds.; Springer: Cham, Switzerland, 2020; pp. 49–61. [Google Scholar]
- Design Council. What Is the Framework for Innovation? Design Council’s Evolved Double Diamond. Available online: https://www.designcouncil.org.uk/news-opinion/what-framework-innovation-design-councils-evolved-double-diamond (accessed on 8 December 2020).
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Hao, C. Cultura: Achieving Intercultural Empathy through Contextual User Research in Design. Ph.D. Thesis, Delft University of Technolgy, Delft, The Netherlands, 2019. [Google Scholar]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Theme | Sub-Theme | Example Quote |
|---|---|---|
| Understand the context and users | Provide knowledge about the end-users before field study | “Allow for you to get information about PwD without needing to be there in person.” |
| Gain insights from the caregivers | “I do believe that I could have used the person-centred canvas to gain better insights from the caregivers.” | |
| Narrow down the design brief | “Design for dementia is an elaborate topic, so the toolkit gives you hands-on tips on where to start.” | |
| Understand the capabilities of PwD | “Capability cards helped me when designing my product that is multi-sensory and how to adjust it so that people with dementia can enjoy the product.” | |
| Initiate the ideation | Understand the needs and wishes of PwD | “I think these tools are helpful during the ideation phase to understand the needs and wishes of the users better.” |
| Offer a design direction | “In the first period, I didn’t know what to do; it gave me helpful instructions, like which direction I could think about (for instance, music therapy).” | |
| Develop the concept | Use as a knowledge source | “I needed to design something the size of an image that PwD could still see. Therefore, I checked the capability cards.” |
| Provide criteria for improving the design | “The capability cards helped to think of what you need to still improve the concept.” | |
| Test the prototype | Answer some user testing questions | “For me, it could answer some of the questions that I wanted to determine in user testing.” |
| Predict the reactions of PwD | “Give insight into the way the end-user handles certain things/products.” |
| Theme | Sub-Theme | Example Quote |
|---|---|---|
| Elaborate the tools | Provide more examples of how each tool could be used | “Maybe examples of how they are used in a design process, how they come back in a final design.” |
| The capability cards could be more detailed | “I think it will be better if there are more classification of different stages and types of dementia in the cards.” | |
| Include how to use the toolkit with the caregivers | “The canvas would also have helped if the caregivers had time to fill them in.” | |
| Add more elements to the toolkit | Add literature resources about dementia | “I think that’s ‘more literature resources for further explanation of dementia’ which means making this tool becomes a literature searching tool for designers to use.” |
| Include methods for evaluating responses of PwD | “I used the positive response schedule by introducing an activity between the caregiver and the person with Dementia. It helped me understand, observe and mark the behaviour of both the PwD and the caregiver.” | |
| Include methods for remote testing | “I would like to see the reactions of PwD themselves. So maybe more technological support with cameras, etc.” | |
| Make the toolkit more accessible | Visibility of the website | “More a practical thing; it is a bit difficult to find the website and also to find different sections of the website.” |
| The user manual should be more visible | “Not really sure which manual you’re referring to.” | |
| Hardcopy and templates to make it more accessible | “Maybe these tools could be made into one booklet with templates so researchers could use it on the fly.” | |
| Provide the toolkit at an earlier stage of the design process | “It gave me inspiration. But these cards were shown to me at a late stage, so, unfortunately, I could not use them as much as I wanted.” |
| Feature | “Know-Me” Toolkit | Toolkit by MinD | Toolkit by LAUGH |
|---|---|---|---|
| Target users | Designers and healthcare professionals | Designers | Designers |
| Components | Ergonomics in Ageing; Co-design; Data-enabled Design | Ergonomics in Ageing; Co-design; | Ergonomics in Ageing; Co-design; |
| Design goal | Personalised design | Generic design | Personalised design |
| Stages of dementia that are applicable | All stages | All stages | Moderate to late stages |
| Design examples on how to use the toolkit | Design examples available online now | Design examples available online | Design examples available online |
| Format | Cards, interactive tools, canvas | Cards, canvas | Booklet |
| Detailedness of instructions | Step-by-step instructions | Step-by-step instructions | Only design elements are explained |
| Interactivity and layered design | Some tools are interactive digitally with a layered design | None of the tools is interactive digitally or with layered design | None of the tools is interactive digitally or with layered design |
| Accessibility | Does not yet appear on the first page of Google search with the search term “design toolkit dementia” | Appears on the first page of Google search with the search term “design toolkit dementia” | Appears on the first page of Google search with the search term “design toolkit dementia” |
| Hardcopy availability | The interactive tools cannot be easily printed—is rectified | Can be easily printed | Can be easily printed |
| User manual availability | Available on the website | Rationale of each tool is explained on the website | No user manual |
| Design stages that are applicable | For the whole design process | For the whole design process | For the whole design process |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, G.; Albayrak, A.; Hogervorst, E.; van der Cammen, T.J.M. Know-Me: A Toolkit for Designing Personalised Dementia Care. Int. J. Environ. Res. Public Health 2021, 18, 5662. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115662
Wang G, Albayrak A, Hogervorst E, van der Cammen TJM. Know-Me: A Toolkit for Designing Personalised Dementia Care. International Journal of Environmental Research and Public Health. 2021; 18(11):5662. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115662
Chicago/Turabian StyleWang, Gubing, Armagan Albayrak, Eef Hogervorst, and Tischa J. M. van der Cammen. 2021. "Know-Me: A Toolkit for Designing Personalised Dementia Care" International Journal of Environmental Research and Public Health 18, no. 11: 5662. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115662