
mHealth Interventions to Address Physical Activity and Sedentary Behavior in Cancer Survivors: A Systematic Review

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Inclusion Criteria
2.1.1. Study Designs
2.1.2. Participants
2.1.3. Interventions
2.1.4. Comparator(s)
2.1.5. Outcomes
2.2. Search Strategy
2.3. Study Selection
2.4. Data Extraction
2.5. Risk of Bias Appraisal
2.6. Analysis
- (1)
- Strong evidence: at least 66% (2/3) of controlled trials with low/some risk of bias show effect in the same direction;
- (2)
- Moderate evidence: 50% to 65% of controlled trials with low/some risk of bias show effect in the same direction;
- (3)
- Limited evidence: less than three low/some concerns risk of bias controlled trials available;
- (4)
- Inconclusive evidence: other findings not applicable to strong, moderate, or limited. For example, inconsistent findings in multiple studies (two of five or 40% low-risk studies show effect in the same direction).
3. Results
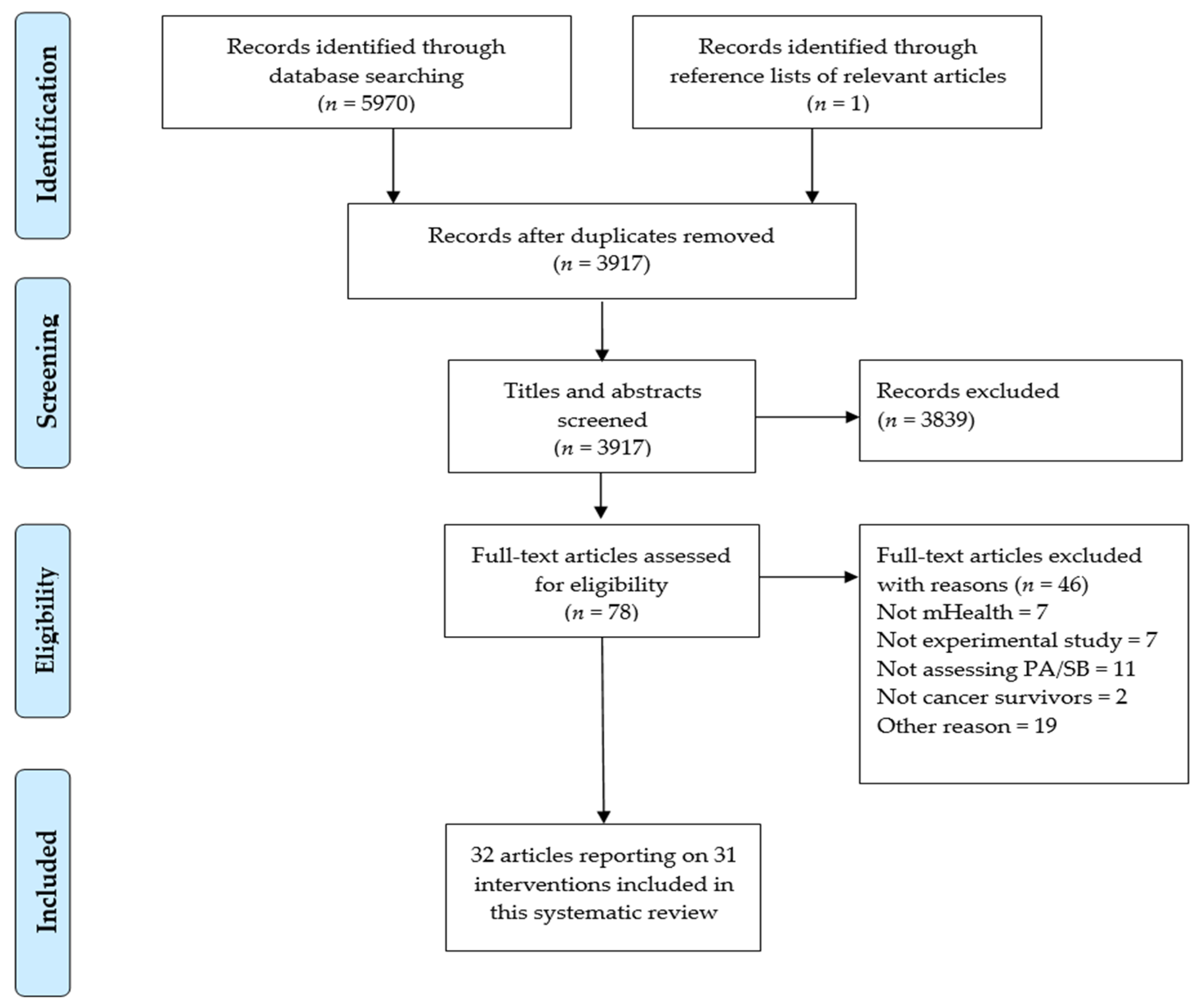
3.1. Study Selection
3.2. Study Characteristics
3.3. Participant Characteristics
3.4. Intervention Characteristics
3.5. Intervention Effects on PA Outcomes
3.5.1. Intervention Effects on PA Outcomes in Controlled Trials
3.5.2. Effects on PA Outcomes in Non-Controlled Trials
3.6. Intervention Effects on SB Outcomes
3.7. Risk of Bias Assessment
3.8. Best Evidence Synthesis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021. [Google Scholar] [CrossRef]
- Allemani, C.; Matsuda, T.; Di Carlo, V.; Harewood, R.; Matz, M.; Nikšić, M.; Bonaventure, A.; Valkov, M.; Johnson, C.J.; Estève, J. Global Surveillance of Trends in Cancer Survival 2000–14 (CONCORD-3): Analysis of Individual Records for 37 513 025 Patients Diagnosed with One of 18 Cancers from 322 Population-Based Registries in 71 Countries. Lancet 2018, 391, 1023–1075. [Google Scholar] [CrossRef] [Green Version]
- Kleckner, I.R.; Dunne, R.F.; Asare, M.; Cole, C.; Fleming, F.; Fung, C.; Lin, P.-J.; Mustian, K.M. Exercise for Toxicity Management in Cancer-A Narrative Review. Oncol. Hematol. Rev. 2018, 14, 28–37. [Google Scholar] [CrossRef]
- Weaver, K.E.; Forsythe, L.P.; Reeve, B.B.; Alfano, C.M.; Rodriguez, J.L.; Sabatino, S.A.; Hawkins, N.A.; Rowland, J.H. Mental and Physical Health–Related Quality of Life among US Cancer Survivors: Population Estimates from the 2010 National Health Interview Survey. Cancer Epidemiol. Biomark. Prev. 2012, 21, 2108–2117. [Google Scholar] [CrossRef] [Green Version]
- Demark-Wahnefried, W.; Pinto, B.M.; Gritz, E.R. Promoting Health and Physical Function among Cancer Survivors: Potential for Prevention and Questions That Remain. J. Clin. Oncol. 2006, 24, 5125–5131. [Google Scholar] [CrossRef]
- World Health Organization. Available online: https://www.who.int/news-room/fact-sheets/detail/physical-activity (accessed on 18 May 2021).
- Friedenreich, C.M.; Stone, C.R.; Cheung, W.Y.; Hayes, S.C. Physical Activity and Mortality in Cancer Survivors: A Systematic Review and Meta-Analysis. JNCI Cancer Spectrum. 2020, 4. [Google Scholar] [CrossRef]
- Patel, A.V.; Friedenreich, C.M.; Moore, S.C.; Hayes, S.C.; Silver, J.K.; Campbell, K.L.; Winters-Stone, K.; Gerber, L.H.; George, S.M.; Fulton, J.E. American College of Sports Medicine Roundtable Report on Physical Activity, Sedentary Behavior, and Cancer Prevention and Control. Med. Sci. Sports Exerc. 2019, 51, 2391–2402. [Google Scholar] [CrossRef] [Green Version]
- Jung, A.Y.; Behrens, S.; Schmidt, M.; Thoene, K.; Obi, N.; Hüsing, A.; Benner, A.; Steindorf, K.; Chang-Claude, J. Pre-to Postdiagnosis Leisure-Time Physical Activity and Prognosis in Postmenopausal Breast Cancer Survivors. Breast Cancer Res. 2019, 21, 117. [Google Scholar] [CrossRef] [Green Version]
- Van Blarigan, E.L.; Fuchs, C.S.; Niedzwiecki, D.; Zhang, S.; Saltz, L.B.; Mayer, R.J.; Mowat, R.B.; Whittom, R.; Hantel, A.; Benson, A.; et al. Association of Survival With Adherence to the American Cancer Society Nutrition and Physical Activity Guidelines for Cancer Survivors After Colon Cancer Diagnosis: The CALGB 89803/Alliance Trial. JAMA Oncol. 2018, 4, 783–790. [Google Scholar] [CrossRef]
- Brown, J.C.; Winters-Stone, K.; Lee, A.; Schmitz, K.H. Cancer, Physical Activity, and Exercise. Compr. Physiol. 2012, 2, 2775–2809. [Google Scholar] [CrossRef] [Green Version]
- Tremblay, M.S.; Aubert, S.; Barnes, J.D.; Saunders, T.J.; Carson, V.; Latimer-Cheung, A.E.; Chastin, S.F.M.; Altenburg, T.M.; Chinapaw, M.J.M. Sedentary Behavior Research Network (SBRN)—Terminology Consensus Project Process and Outcome. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 75. [Google Scholar] [CrossRef] [Green Version]
- Ehlers, D.K.; Fanning, J.; Sunderlage, A.; Severson, J.; Kramer, A.F.; McAuley, E. Influence of Sitting Behaviors on Sleep Disturbance and Memory Impairment in Breast Cancer Survivors. Cancer Med. 2020, 9, 3417–3424. [Google Scholar] [CrossRef] [Green Version]
- Sabiston, C.M.; Lacombe, J.; Faulkner, G.; Jones, J.; Trinh, L. Profiling Sedentary Behavior in Breast Cancer Survivors: Links with Depression Symptoms during the Early Survivorship Period. Psychooncology 2018, 27, 569–575. [Google Scholar] [CrossRef]
- Swain, C.T.; Nguyen, N.H.; Eagles, T.; Vallance, J.K.; Boyle, T.; Lahart, I.M.; Lynch, B.M. Postdiagnosis Sedentary Behavior and Health Outcomes in Cancer Survivors: A Systematic Review and Meta-analysis. Cancer 2020, 126, 861–869. [Google Scholar] [CrossRef]
- Rock, C.L.; Doyle, C.; Demark-Wahnefried, W.; Meyerhardt, J.; Courneya, K.S.; Schwartz, A.L.; Bandera, E.V.; Hamilton, K.K.; Grant, B.; McCullough, M. Nutrition and Physical Activity Guidelines for Cancer Survivors. CA Cancer J. Clin. 2012, 62, 242–274. [Google Scholar] [CrossRef] [Green Version]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.-P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 Guidelines on Physical Activity and Sedentary Behaviour. Br. J. Sports Med. 2020, 54, 1451. [Google Scholar] [CrossRef]
- Kim, R.B.; Phillips, A.; Herrick, K.; Helou, M.; Rafie, C.; Anscher, M.S.; Mikkelsen, R.B.; Ning, Y. Physical Activity and Sedentary Behavior of Cancer Survivors and Non-Cancer Individuals: Results from a National Survey. PLoS ONE 2013, 8, e57598. [Google Scholar] [CrossRef] [Green Version]
- Marcolino, M.S.; Oliveira, J.A.Q.; D’Agostino, M.; Ribeiro, A.L.; Alkmim, M.B.M.; Novillo-Ortiz, D. The Impact of mHealth Interventions: Systematic Review of Systematic Reviews. JMIR Mhealth Uhealth 2018, 6, e23. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Available online: https://www.who.int/goe/publications/goe_mhealth_web.pdf (accessed on 12 April 2020).
- Müller, A.M.; Maher, C.A.; Vandelanotte, C.; Hingle, M.; Middelweerd, A.; Lopez, M.L.; DeSmet, A.; Short, C.E.; Nathan, N.; Hutchesson, M.J.; et al. Physical Activity, Sedentary Behavior, and Diet-Related eHealth and mHealth Research: Bibliometric Analysis. J. Med. Internet Res. 2018, 20, e8954. [Google Scholar] [CrossRef]
- Vandelanotte, C.; Müller, A.M.; Short, C.E.; Hingle, M.; Nathan, N.; Williams, S.L.; Lopez, M.L.; Parekh, S.; Maher, C.A. Past, Present, and Future of eHealth and mHealth Research to Improve Physical Activity and Dietary Behaviors. J. Nutr. Educ. Behav. 2016, 48, 219–228.e1. [Google Scholar] [CrossRef]
- Direito, A.; Carraça, E.; Rawstorn, J.; Whittaker, R.; Maddison, R. MHealth Technologies to Influence Physical Activity and Sedentary Behaviors: Behavior Change Techniques, Systematic Review and Meta-Analysis of Randomized Controlled Trials. Ann. Behav. Med. 2017, 51, 226–239. [Google Scholar] [CrossRef] [Green Version]
- Haberlin, C.; O’Dwyer, T.; Mockler, D.; Moran, J.; O’Donnell, D.M.; Broderick, J.; O’Dwyer, T.; O’Donnell, D.M. The Use of EHealth to Promote Physical Activity in Cancer Survivors: A Systematic Review. Support. Care Cancer 2018, 26, 3323–3336. [Google Scholar] [CrossRef] [PubMed]
- Roberts, A.L.; Fisher, A.; Smith, L.; Heinrich, M.; Potts, H.W. Digital Health Behaviour Change Interventions Targeting Physical Activity and Diet in Cancer Survivors: A Systematic Review and Meta-Analysis. J. Cancer Surviv. 2017, 11, 704–719. [Google Scholar] [CrossRef]
- Coughlin, S.S.; Caplan, L.S.; Stone, R. Use of Consumer Wearable Devices to Promote Physical Activity among Breast, Prostate, and Colorectal Cancer Survivors: A Review of Health Intervention Studies. J. Cancer Surviv. 2020, 14, 386–392. [Google Scholar] [CrossRef]
- Corbett, T.; Cheetham, T.; Müller, A.M.; Slodkowska-Barabasz, J.; Wilde, L.; Krusche, A.; Richardson, A.; Foster, C.; Watson, E.; Little, P.; et al. Exploring Cancer Survivors’ Views of Health Behaviour Change: “Where Do You Start, Where Do You Stop with Everything?”. Psychooncology 2018, 27, 1816–1824. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Denlinger, C.S.; Carlson, R.W.; Are, M.; Baker, K.S.; Davis, E.; Edge, S.B.; Friedman, D.L.; Goldman, M.; Jones, L.; King, A. Survivorship: Introduction and Definition. J. Natl. Compr. Cancer Netw. 2014, 12, 34–45. [Google Scholar] [CrossRef] [Green Version]
- Ganesan, A.N.; Louise, J.; Horsfall, M.; Bilsborough, S.A.; Hendriks, J.; McGavigan, A.D.; Selvanayagam, J.B.; Chew, D.P. International Mobile-Health Intervention on Physical Activity, Sitting, and Weight: The Stepathlon Cardiovascular Health Study. J. Am. Coll. Cardiol. 2016, 67, 2453–2463. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 6.1 (Updated September 2020). Cochrane. 2020. Available online: www.training.cochrane.org/handbook (accessed on 23 April 2021).
- Higgins, J.P.; Sterne, J.A.; Savovic, J.; Page, M.J.; Hróbjartsson, A.; Boutron, I.; Reeves, B.; Eldridge, S. A Revised Tool for Assessing Risk of Bias in Randomized Trials. Cochrane Database Syst. Rev. 2016, 10, 29–31. [Google Scholar]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I. ROBINS-I: A Tool for Assessing Risk of Bias in Non-Randomised Studies of Interventions. BMJ 2016, 355. [Google Scholar] [CrossRef] [Green Version]
- Slavin, R.E. Best Evidence Synthesis: An Intelligent Alternative to Meta-Analysis. J. Clin. Epidemiol. 1995, 48, 9–18. [Google Scholar] [CrossRef]
- Fanchini, M.; Steendahl, I.B.; Impellizzeri, F.M.; Pruna, R.; Dupont, G.; Coutts, A.J.; Meyer, T.; McCall, A. Exercise-Based Strategies to Prevent Muscle Injury in Elite Footballers: A Systematic Review and Best Evidence Synthesis. Sports Med. 2020, 50, 1653–1666. [Google Scholar] [CrossRef]
- Kuijer, P.P.F.M.; Gouttebarge, V.; Brouwer, S.; Reneman, M.F.; Frings-Dresen, M.H.W. Are Performance-Based Measures Predictive of Work Participation in Patients with Musculoskeletal Disorders? A Systematic Review. Int. Arch. Occup. Environ. Health 2012, 85, 109–123. [Google Scholar] [CrossRef] [Green Version]
- van Tulder, M.; Furlan, A.; Bombardier, C.; Bouter, L. Updated Method Guidelines for Systematic Reviews in the Cochrane Collaboration Back Review Group. Spine 2003, 28, 1290–1299. [Google Scholar] [CrossRef] [Green Version]
- Lynch, B.M.; Nguyen, N.H.; Moore, M.M.; Reeves, M.M.; Rosenberg, D.E.; Boyle, T.; Vallance, J.K.; Milton, S.; Friedenreich, C.M.; English, D.R. A Randomized Controlled Trial of a Wearable Technology-Based Intervention for Increasing Moderate to Vigorous Physical Activity and Reducing Sedentary Behavior in Breast Cancer Survivors: The ACTIVATE Trial. Cancer 2019, 125, 2846–2855. [Google Scholar] [CrossRef]
- Lynch, B.M.; Nguyen, N.H.; Moore, M.M.; Reeves, M.M.; Rosenberg, D.E.; Boyle, T.; Milton, S.; Friedenreich, C.M.; Vallance, J.K.; English, D.R. Maintenance of Physical Activity and Sedentary Behavior Change, and Physical Activity and Sedentary Behavior Change after an Abridged Intervention: Secondary Outcomes from the ACTIVATE Trial. Cancer 2019, 125, 2856–2860. [Google Scholar] [CrossRef] [PubMed]
- Mendoza, J.A.; Baker, K.S.; Moreno, M.A.; Whitlock, K.; Abbey-Lambertz, M.; Waite, A.; Colburn, T.; Chow, E.J. A Fitbit and Facebook MHealth Intervention for Promoting Physical Activity among Adolescent and Young Adult Childhood Cancer Survivors: A Pilot Study. Pediatr. Blood Cancer 2017, 64. [Google Scholar] [CrossRef] [PubMed]
- Le, A.; Mitchell, H.; Zheng, D.J.; Rotatori, J.; Fahey, J.T.; Ness, K.K.; Kadan-Lottick, N.S.; Mitchell, H.-R.; Kadan-Lottick, N.S. A Home-Based Physical Activity Intervention Using Activity Trackers in Survivors of Childhood Cancer: A Pilot Study. Pediatr. Blood Cancer 2017, 64, 387–394. [Google Scholar] [CrossRef] [PubMed]
- Cadmus-Bertram, L.; Tevaarwerk, A.J.; Sesto, M.E.; Gangnon, R.; Van Remortel, B.; Date, P. Building a Physical Activity Intervention into Clinical Care for Breast and Colorectal Cancer Survivors in Wisconsin: A Randomized Controlled Pilot Trial. J. Cancer Surviv. 2019, 13, 593–602. [Google Scholar] [CrossRef]
- Gell, N.; Grover, K.; Humble, M.; Sexton, M.; Dittus, K.; Gell, N.M.; Grover, K.W. Efficacy, Feasibility, and Acceptability of a Novel Technology-Based Intervention to Support Physical Activity in Cancer Survivors. Support. Care Cancer 2017, 25, 1291–1300. [Google Scholar] [CrossRef]
- Gell, N.M.; Grover, K.W.; Savard, L.; Dittus, K. Outcomes of a Text Message, Fitbit, and Coaching Intervention on Physical Activity Maintenance among Cancer Survivors: A Randomized Control Pilot Trial. J. Cancer Surviv. 2020, 14, 80–88. [Google Scholar] [CrossRef]
- Ovans, J.A.; Hooke, M.C.; Bendel, A.E.; Tanner, L.R. Physical Therapist Coaching to Improve Physical Activity in Children With Brain Tumors: A Pilot Study. Pediatr. Phys. Ther. 2018, 30, 310–317. [Google Scholar] [CrossRef] [PubMed]
- Mayer, D.K.; Landucci, G.; Awoyinka, L.; Atwood, A.K.; Carmack, C.L.; Demark-Wahnefried, W.; McTavish, F.; Gustafson, D.H. SurvivorCHESS to Increase Physical Activity in Colon Cancer Survivors: Can We Get Them Moving? J. Cancer Surviv. 2018, 12, 82–94. [Google Scholar] [CrossRef]
- Kenfield, S.; Van Blarigan, E.; Ameli, N.; Lavaki, E.; Cedars, B.; Paciorek, A.; Monroy, C.; Tantum, L.; Newton, R.; Signorell, C.; et al. Feasibility, Acceptability, and Behavioral Outcomes from a Technology-Enhanced Behavioral Change Intervention (Prostate 8): A Pilot Randomized Controlled Trial in Men with Prostate Cancer. Eur. Urol. 2019. [Google Scholar] [CrossRef] [PubMed]
- Haggerty, A.; Hagemann, A.; Barnett, M.; Thornquist, M.; Neuhouser, M.; Horowitz, N.; Colditz, G.; Sarwer, D.; Ko, E.; Allison, K. A Randomized, Controlled, Multicenter Study of Technology-Based Weight Loss Interventions among Endometrial Cancer Survivors. Obesity 2017, 25 (Suppl. 2), S102–S108. [Google Scholar] [CrossRef] [Green Version]
- Pope, Z.C.; Zeng, N.; Zhang, R.; Lee, H.Y.; Gao, Z. Effectiveness of Combined Smartwatch and Social Media Intervention on Breast Cancer Survivor Health Outcomes: A 10-Week Pilot Randomized Trial. J. Clin. Med. 2018, 7, 140. [Google Scholar] [CrossRef] [Green Version]
- McCarroll, M.L.; Armbruster, S.; Pohle-Krauza, R.J.; Lyzen, A.M.; Min, S.; Nash, D.W.; Roulette, G.D.; Andrews, S.J.; von Gruenigen, V.E. Feasibility of a Lifestyle Intervention for Overweight/Obese Endometrial and Breast Cancer Survivors Using an Interactive Mobile Application. Gynecol. Oncol. 2015, 137, 508–515. [Google Scholar] [CrossRef]
- Valle, C.G.; Deal, A.M.; Tate, D.F. Preventing Weight Gain in African American Breast Cancer Survivors Using Smart Scales and Activity Trackers: A Randomized Controlled Pilot Study. J. Cancer Surviv. 2017, 11, 133–148. [Google Scholar] [CrossRef] [PubMed]
- Hartman, S.J.; Nelson, S.H.; Myers, E.; Natarajan, L.; Sears, D.D.; Palmer, B.W.; Weiner, L.S.; Parker, B.A.; Patterson, R.E. Randomized Controlled Trial of Increasing Physical Activity on Objectively Measured and Self-Reported Cognitive Functioning among Breast Cancer Survivors: The Memory & Motion Study. Cancer 2018, 124, 192–202. [Google Scholar] [CrossRef]
- Singh, B.; Spence, R.R.; Sandler, C.X.; Tanner, J.; Hayes, S.C. Feasibility and Effect of a Physical Activity Counselling Session with or without Provision of an Activity Tracker on Maintenance of Physical Activity in Women with Breast Cancer—A Randomised Controlled Trial. J. Sci. Med. Sport 2020, 23, 283–290. [Google Scholar] [CrossRef] [Green Version]
- Spark, L.C.; Fjeldsoe, B.S.; Eakin, E.G.; Reeves, M.M. Efficacy of a Text Message-Delivered Extended Contact Intervention on Maintenance of Weight Loss, Physical Activity, and Dietary Behavior Change. JMIR Mhealth Uhealth 2015, 3, e88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Short, C.E.; Finlay, A.; Sanders, I.; Maher, C. Development and Pilot Evaluation of a Clinic-Based MHealth App Referral Service to Support Adult Cancer Survivors Increase Their Participation in Physical Activity Using Publicly Available Mobile Apps. BMC Health Serv. Res. 2018, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maxwell-Smith, C.; Hince, D.; Cohen, P.A.; Bulsara, M.K.; Boyle, T.; Platell, C.; Tan, P.; Levitt, M.; Salama, P.; Tan, J.; et al. A Randomized Controlled Trial of WATAAP to Promote Physical Activity in Colorectal and Endometrial Cancer Survivors. Psychooncology 2019, 28, 1420–1429. [Google Scholar] [CrossRef]
- Uhm, K.; Yoo, J.; Chung, S.; Lee, J.; Lee, I.; Kim, J.; Lee, S.; Nam, S.; Park, Y.; Lee, J.; et al. Effects of Exercise Intervention in Breast Cancer Patients: Is Mobile Health (MHealth) with Pedometer More Effective than Conventional Program Using Brochure? Breast Cancer Res. Treat. 2017, 161, 443–452. [Google Scholar] [CrossRef] [PubMed]
- Chung, I.Y.; Jung, M.; Park, Y.R.; Cho, D.; Chung, H.; Min, Y.H.; Park, H.J.; Lee, M.; Lee, S.B.; Chung, S.; et al. Exercise Promotion and Distress Reduction Using a Mobile App-Based Community in Breast Cancer Survivors. Front. Oncol. 2019, 9, 1505. [Google Scholar] [CrossRef] [PubMed]
- Cheong, I.Y.; An, S.Y.; Cha, W.C.; Rha, M.Y.; Kim, S.T.; Chang, D.K.; Hwang, J.H. Efficacy of Mobile Health Care Application and Wearable Device in Improvement of Physical Performance in Colorectal Cancer Patients Undergoing Chemotherapy. Clin. Colorectal Cancer 2018, 17, e353–e362. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Seo, J.; An, S.-Y.; Sinn, D.H.; Hwang, J.H. Efficacy and Safety of an MHealth App and Wearable Device in Physical Performance for Patients With Hepatocellular Carcinoma: Development and Usability Study. JMIR Mhealth Uhealth 2020, 8, e14435. [Google Scholar] [CrossRef]
- McNeil, J.; Brenner, D.R.; Stone, C.R.; O’Reilly, R.; Ruan, Y.; Vallance, J.K.; Courneya, K.S.; Thorpe, K.E.; Klein, D.J.; Friedenreich, C.M. Activity Tracker to Prescribe Various Exercise Intensities in Breast Cancer Survivors. Med. Sci. Sports Exerc. 2019, 51, 930–940. [Google Scholar] [CrossRef]
- Trinh, L.; Arbour-Nicitopoulos, K.P.; Sabiston, C.M.; Berry, S.R.; Loblaw, A.; Alibhai, S.M.H.; Jones, J.M.; Faulkner, G.E. RiseTx: Testing the Feasibility of a Web Application for Reducing Sedentary Behavior among Prostate Cancer Survivors Receiving Androgen Deprivation Therapy. Int. J. Behav. Nutr. Phys. Act. 2018, 15. [Google Scholar] [CrossRef] [Green Version]
- Delrieu, L.; Pialoux, V.; Perol, O.; Morelle, M.; Martin, A.; Friedenreich, C.; Febvey-Combes, O.; Perol, D.; Belladame, E.; Clemencon, M.; et al. Feasibility and Health Benefits of an Individualized Physical Activity Intervention in Women With Metastatic Breast Cancer: Intervention Study. JMIR Mhealth Uhealth 2020, 8, e12306. [Google Scholar] [CrossRef]
- Villaron, C.; Cury, F.; Eisinger, F.; Cappiello, M.-A.; Marqueste, T. Telehealth Applied to Physical Activity during Cancer Treatment: A Feasibility, Acceptability, and Randomized Pilot Study. Support. Care Cancer 2018, 26, 3413–3421. [Google Scholar] [CrossRef]
- Ormel, H.L.; van der Schoot, G.G.F.; Westerink, N.-D.L.; Gietema, J.A.; Walenkamp, A.M.E.; Sluiter, W.J. Self-Monitoring Physical Activity with a Smartphone Application in Cancer Patients: A Randomized Feasibility Study (SMART-Trial). Support. Care Cancer 2018, 26, 3915–3923. [Google Scholar] [CrossRef] [Green Version]
- Götte, M.; Kesting, S.V.; Gerss, J.; Rosenbaum, D.; Boos, J. Feasibility and Effects of a Home-Based Intervention Using Activity Trackers on Achievement of Individual Goals, Quality of Life and Motor Performance in Patients with Paediatric Cancer. BMJ Open Sport Exerc. Med. 2018, 4, e000322. [Google Scholar] [CrossRef] [Green Version]
- Lozano-Lozano, M.; Cantarero-Villanueva, I.; Martin-Martin, L.; Galiano-Castillo, N.; Sanchez, M.-J.; Fernandez-Lao, C.; Postigo-Martin, P.; Arroyo-Morales, M. A Mobile System to Improve Quality of Life Via Energy Balance in Breast Cancer Survivors (BENECA MHealth): Prospective Test-Retest Quasiexperimental Feasibility Study. JMIR Mhealth Uhealth 2019, 7, e14136. [Google Scholar] [CrossRef]
- Puszkiewicz, P.; Roberts, A.L.; Smith, L.; Wardle, J.; Fisher, A. Assessment of Cancer Survivors’ Experiences of Using a Publicly Available Physical Activity Mobile Application. JMIR Cancer 2016, 2, e7. [Google Scholar] [CrossRef] [PubMed]
- Van Blarigan, E.L.; Chan, H.; Van Loon, K.; Kenfield, S.A.; Chan, J.M.; Mitchell, E.; Zhang, L.; Paciorek, A.; Joseph, G.; Laffan, A.; et al. Self-Monitoring and Reminder Text Messages to Increase Physical Activity in Colorectal Cancer Survivors (Smart Pace): A Pilot Randomized Controlled Trial. BMC Cancer 2019, 19, 218. [Google Scholar] [CrossRef] [Green Version]
- Dorri, S.; Asadi, F.; Olfatbakhsh, A.; Kazemi, A. A Systematic Review of Electronic Health (eHealth) Interventions to Improve Physical Activity in Patients with Breast Cancer. Breast Cancer 2020, 27, 25–46. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.H.; Wallington, S.F.; Makambi, K.H.; Adams-Campbell, L.L. Social Networks and Physical Activity Behaviors among Cancer Survivors: Data from the 2005 Health Information National Trends Survey. J. Health Commun. 2015, 20, 656–662. [Google Scholar] [CrossRef] [PubMed]
- Smith, L.; Croker, H.; Fisher, A.; Williams, K.; Wardle, J.; Beeken, R.J. Cancer Survivors’ Attitudes towards and Knowledge of Physical Activity, Sources of Information, and Barriers and Facilitators of Engagement: A Qualitative Study. Eur. J. Cancer Care 2017, 26, e12641. [Google Scholar] [CrossRef] [Green Version]
- McNeill, L.H.; Kreuter, M.W.; Subramanian, S.V. Social Environment and Physical Activity: A Review of Concepts and Evidence. Soc. Sci. Med. 2006, 63, 1011–1022. [Google Scholar] [CrossRef] [PubMed]
- Yardley, L.; Spring, B.J.; Riper, H.; Morrison, L.G.; Crane, D.H.; Curtis, K.; Merchant, G.C.; Naughton, F.; Blandford, A. Understanding and Promoting Effective Engagement With Digital Behavior Change Interventions. Am. J. Prev. Med. 2016, 51, 833–842. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Panahi, S.; Tremblay, A. Sedentariness and Health: Is Sedentary Behavior More than Just Physical Inactivity? Front. Public Health 2018, 6, 258. [Google Scholar] [CrossRef] [Green Version]
- Keadle, S.K.; Conroy, D.E.; Buman, M.P.; Dunstan, D.W.; Matthews, C.E. Targeting Reductions in Sitting Time to Increase Physical Activity and Improve Health. Med. Sci. Sports Exerc. 2017, 49, 1572–1582. [Google Scholar] [CrossRef]
- Craft, L.L.; Zderic, T.W.; Gapstur, S.M.; Vaniterson, E.H.; Thomas, D.M.; Siddique, J.; Hamilton, M.T. Evidence That Women Meeting Physical Activity Guidelines Do Not Sit Less: An Observational Inclinometry Study. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 122. [Google Scholar] [CrossRef] [Green Version]
- Cho, Y.-M.; Lee, S.; Islam, S.M.S.; Kim, S.-Y. Theories Applied to M-Health Interventions for Behavior Change in Low-and Middle-Income Countries: A Systematic Review. Telemed. J. E Health 2018, 24, 727–741. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Müller, A.M.; Alley, S.; Schoeppe, S.; Vandelanotte, C. The Effectiveness of E-& MHealth Interventions to Promote Physical Activity and Healthy Diets in Developing Countries: A Systematic Review. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 1–14. [Google Scholar]


{kind=link}
| First Author, Year, Country | Study Design | Sample Size; Age Group; Cancer Type(s) | Intervention Group | Control Group | PA/SB Outcome | Other Outcome |
|---|---|---|---|---|---|---|
| Cadmus-Bertram, 2019, United States [42] | 12 weeks RCT (Pilot) | Baseline: n = 50 Analyzed: n = 47; Adults/older adults; Breast, colorectal | mHealth: Activity tracker non-mHealth component: Printed material, in-person session, social support, email-based coaching and electronic health record linked to an activity tracker | Printed material and email | PA | Weight |
| Cheong, 2018, Republic of Korea [59] | 12 weeks pre-post | Baseline/analyzed: n = 75; Adults/older adults; Colorectal | mHealth: app providing daily exercise program and activity tracker to record activity | Not applicable | PA | Muscle strength, cardiorespiratory fitness, QoL |
| Chung, 2019, Republic of Korea [58] | 12 weeks Quasi-experimental | Baseline: n = 54 Analyzed: n = 37; Adults/older adults; Breast | mHealth: WalkOn R app to promote healthy activities in a mobile community | No intervention | PA | Not applicable |
| Delrieu, 2020, France [63] | 6 months Pre-Post | Baseline: n = 49 Analyzed: n = 44; Adults/ older adults; Breast | mHealth: Activity tracker and affiliated app non-mHealth component: In-person or phone sessions on performance feedback or recommendations of PA and SB | Not applicable | PA, SB | Cardiorespiratory fitness, strength, anthropometry, QoL, fatigue |
| Gell, 2017, United States [43] | 4 weeks pre-post (Pilot) | Baseline/Analyzed: n = 24; Adults/ older adults; Various | mHealth: Activity tracker and text messages non-mHealth component: Health coaching phone calls | Not applicable | PA | Self-regulation, fatigue, depression, acceptability |
| Gell, 2020, United States [44] | 8 weeks RCT (Pilot) | Baseline: n = 66 Analyzed: n = 59; Adults/older adults; Various | mHealth: Activity tracker and text messages non-mHealth component: Phone calls from health coach | No intervention | PA, SB | Adherence wearing activity tracker, intervention satisfaction |
| Götte, 2018, Germany [66] | 10 weeks Quasi-experimental | Baseline: n = 40 Analyzed: n = 39; Children/adolescents; pediatric | mHealth: Activity tracker non-mHealth component: Supervised exercise intervention during and after acute cancer treatment | Exercise intervention after acute cancer treatment | PA | QoL, motor performance, acceptability |
| Haggerty, 2017, United States [48] | 6 months RCT (Pilot) | Baseline: n = 41 Analyzed: n = 32; Adults/older adults; Endometrial | mHealth: Text messages to support weight loss non-mHealth component: Conventional weighing scale | Telemedicine (active CG) and no intervention (inactive CG) | PA | Weight loss, anthropometry, QoL |
| Hartman, 2018, United States [52] | 12 weeks RCT | Baseline/Analyzed: n = 87; Adults/ older adults; Breast | mHealth: Activity tracker non-mHealth component: In- person session to set PA goals | No intervention | PA | BMI, neurocognitive functioning |
| Kenfield, 2019, United States [47] | 12 weeks RCT (Pilot) | Baseline: n = 76 Analyzed: n = 65; Adults/older adults; Prostate | mHealth: Activity tracker and text messages non-mHealth component: Website providing behavioral and social support information | No intervention | PA | Acceptability |
| Kim, 2020, Republic of Korea [60] | 12 weeks pre-post | Baseline/Analyzed: n = 31; Adults/older adults; Hepatocellular carcinoma | mHealth: Care app and activity tracker prescribing exercise program | Not applicable | PA | Cardiorespiratory fitness, strength, anthropometry, QoL |
| Le, 2017, United States [41] | 6 months Pre-post (pilot) | Baseline: n = 19 Analyzed: n = 15; Adolescents/young adults; Various | mHealth: Activity tracker to record PA non-mHealth component: Website and instruction to adhere to exercise recommendations | Not applicable | PA | Cardiorespiratory fitness, barriers to exercise |
| Lozano-Lozano, 2019, Spain [67] | 8 weeks pre-post | Baseline: n = 80 Analyzed: n = 76; Adults/older adults; Breast | mHealth: BENECA mHealth app to monitor and provide feedback on healthy eating and PA | Not applicable | PA | QoL, self-efficacy, anthropometry |
| Lynch, 2019, Australia [38,39] | 12 weeks RCT | Baseline: n = 83 Analyzed: n = 80; Adults/older adults; Breast | mHealth: Activity tracker and affiliated app non-mHealth component: In-person session and telephone-health coaching sessions | No intervention | PA, SB | Not applicable |
| Maxwell–Smith, 2019, Australia [56] | 12 weeks RCT | Baseline: n = 68 Analyzed: n = 67; Adults/older adults; Colorectal, gynecologic (at risk of cardiovascular disease) | mHealth: Activity tracker non-mHealth component: Dashboard to collect PA engagement data, printed material, group sessions and phone call at Week 8 | Printed material | PA, SB | BMI, blood pressure |
| Mayer, 2018, United States [46] | 6 months RCT | Baseline: n = 284 Analyzed: n = 227; Adults/older adults; Colon | mHealth: SurvivorCHESS app to help increase daily activity levels non-mHealth component: Printed material, self-learning audio program for cancer survival and pedometer | Printed material, self-learning program for cancer survival and pedometer | PA | QoL, distress |
| McCarroll, 2015, United States [50] | 4 weeks pre-post | Baseline: n = 50 Analyzed: n = 35; Adults/older adults; Breast, endometrial | mHealth: LoseIt! app to support weight-loss non-mHealth component: Weighing scale to track weight | Not applicable | PA | QoL, self-efficacy, anthropometry |
| McNeil, 2019, Canada [61] | 12 weeks RCT (Pilot) | Baseline: n = 45 Analyzed: n = 41; Adults/older adults; Breast | mHealth: Activity tracker and app to prescribe exercise non-mHealth component: Diary and phone call or e-mail | No intervention | PA, SB | Anthropometry, cardiorespiratory fitness |
| Mendoza, 2017, United States [40] | 10 weeks RCT (Pilot) | Baseline/analyzed: n = 59; Children/adolescents; Various | mHealth: Activity tracker with app and text messages non-mHealth component: Facebook support group and phone call to set a daily step goal | No intervention | PA, SB | QoL, acceptability |
| Ormel, 2018, Netherlands [65] | 12 weeks RCT | Baseline/analyzed: n = 32; Adults/older adults; Various | mHealth: RunKeeper app for self-monitoring PA | No intervention | PA, SB | Usability of app |
| Ovans, 2018, United States [45] | 12 weeks Pre-post (pilot) | Baseline/analyzed: n = 15; Children/ adolescents; Brain tumor | mHealth: Activity tracker non-mHealth component: Phone or in-person coaching to encourage PA | Not applicable | PA | Cardiorespiratory fitness, QoL, fatigue |
| Pope, 2018, United States [49] | 10 weeks RCT | Baseline: n = 30 Analyzed: n = 20; Adults/older adults; Breast | mHealth: Activity tracker non-mHealth component: Facebook group providing PA tips | Facebook group | PA, SB | Anthropometry, cardiorespiratory fitness |
| Puszkiewic, 2016, United Kingdom [68] | 6 weeks pre-Post | Baseline/Analyzed: n = 11; Adults/older adults; Various | mHealth: GAINFitness app that provides a PA program | Not applicable | PA | Anthropometry, QoL, sleep quality, app engagement |
| Short, 2018, Australia [55] | 2 weeks pre-post (pilot) | Baseline/analyzed: n = 10; Adults/older adults; Various | mHealth: app to support PA. non-mHealth component: In- person consultation, handout, and telephone or email. | Not applicable | PA | Acceptability |
| Singh, 2020, Australia [53] | 12 weeks RCT | Baseline: n = 52 Analyzed: n = 50; Adults/older adults; Breast (after completed supervised exercise intervention) | mHealth: Activity tracker non-mHealth component: Counselling session and printed material | Counselling session and printed material | PA | Acceptability |
| Spark, 2015, Australia [54] | 6 months pre-post | Baseline: n = 25 Analyzed: n = 23; Adults/older adults; Breast | mHealth: Text messages to promote weight loss, PA and dietary behavior change non-mHealth component: Phone call to tailor self-regulation strategies | Not applicable | PA | Weight |
| Trinh, 2018, Canada [62] | 12 weeks pre-post (pilot) | Baseline/Analyzed: n = 46, Adults/older adults; Prostate | mHealth: Activity tracker non-mHealth component: Web-based SB intervention | Not applicable | PA, SB | QoL, feasibility |
| Uhm, 2017, Republic of Korea [57] | 12 weeks Quasi-experimental | Baseline: n = 356 Analyzed: n = 339; Adults/older adults; Breast | mHealth: Smart After Care exercise app non-mHealth component: Pedometer | Printed material | PA | BMI, blood pressure, heart rate, strength, cardiorespiratory fitness, QoL, user satisfaction |
| Valle, 2017, United States [51] | 6 months RCT (Pilot) | Baseline: n = 35 Analyzed: n = 33; Adults/older adults; Breast | mHealth: Activity tracker interfaced with app non-mHealth component: In-person session, wireless weighing scale, and email-delivered behavioral lessons | Self-regulation intervention group and wireless weighing scale | PA | BMI |
| Van Blarigan, 2019, United States [69] | 12 weeks RCT (Pilot) | Baseline: n = 41 Analyzed: n = 39; Adults/older adults; Colorectal | mHealth: Activity tracker and daily text messages non-mHealth component: Printed material on PA after cancer | Printed material on PA after cancer | PA | Feasibility and acceptability |
| Villaron, 2018, France [64] | 8 weeks RCT (Pilot) | Baseline/Analyzed: n = 43; Adults/older adults; Various | mHealth: Weekly PA encouraging text messages non-mHealth component: PA recommendations, pedometer and printed material | Pedometer | PA | QoL, fatigue |
| mHealth Only Interventions | |||||||
| First Author, Year | mHealth Intervention | Control | Effects | Risk of Bias | |||
| PA | SB | Results Summary | |||||
| Chung, 2019 [58] | App to motivate and provide information on PA, healthy diet and distress | Inactive | Significant effect Step counts (steps/w) O | Not applicable | Significant between-group increase in step count favoring the intervention group | No information ** (NI,?,+,+,?,?,+) | |
| Ormel, 2018 [65] | App for PA self-monitoring | Inactive | No significant effect Total PA (min/w) S, Physical activity scale for the elderly (sum score) S | No significant effect Sitting time (min/w) S | No significant between-group change in either outcome | Some concerns * (+,+,+,?,+) | |
| Multicomponent interventions with mHealth component | |||||||
| First Author, Year | Intervention | Control | Effects | Risk of Bias | |||
| mHealth | Non-mHealth Component | PA | SB | Results Summary | |||
| Multicomponent intervention without personal contact (e.g., No phone and in-person contact) | |||||||
| Haggerty, 2017 [48] | Daily text messages providing feedback, support, and strategies to adhere to behavior change | Conventional weighing scale | Active and inactive | Significant effect Walking activity, vigorous PA (METs/w) S No significant effect Total PA (METs/w) S | Not applicable | Significant between-group increase in walking favoring intervention group with a significant increase of vigorous PA in favor of the inactive control group | High * (+,+,?,?,+) |
| Kenfield, 2019 [47] | Activity tracker and text messages to motivate behavioral changes following recommendations | Website | Inactive | No significant effect MVPA (min/d) O, Step counts (steps/d) O | Not applicable | No significant between-group changes in either outcome | Low * (+,+,+,+,+) |
| Mayer, 2018 [46] | Apps providing information and support to increase daily activity levels | Printed material, self-learning audio program and pedometer | Active | No significant effect MVPA (min/w) S | Not applicable | No significant between-group changes in outcome | Some concerns * (?,+,+,+,+) |
| Pope, 2018 [49] | Activity tracker monitoring PA and health metrics | Facebook group | Active | No significant effect Light PA, MVPA (min/d) O, Energy expenditure (kcal/d) O, Step counts (Steps/d) O | No significant effect SB (min/d) O | No significant between-group changes in either outcome | Low * (+,+,+,+,+) |
| Uhm, 2017 [57] | Apps providing information and monitor the prescribed exercises | Pedometer and printed material | Active | No significant effect Total metabolic equivalent (METs/w) S | Not applicable | No significant between-group changes in outcome | Serious ** (/,?,+,+,+,?,+) |
| Van Blarigan, 2019 [69] | Activity tracker to assess PA and daily text messages providing PA information | Printed material | Active | No significant effect MVPA, moderate PA, vigorous PA (min/d) O, Step counts (steps/d) O | Not applicable | No significant between-group changes in either outcome | Low * (+,+,+,+,+) |
| Villaron, 2018 [64] | Text messages on recommendations to increase PA | Printed material | Active | No significant effect Step counts (steps/w) O | Not applicable | No significant between-group changes in outcome | High * (?,+,+,+,?) |
| Multicomponent intervention with personal contact | |||||||
| Cadmus-Bertram, 2019 [42] | Activity tracker for self-monitoring PA and developing self-regulatory skills | Printed material, in-person session, social support and email | Active | Significant effect MVPA, moderate PA (min/w)O, MVPA in bouts (min/d) O, Step counts (steps/d) O No significant effect Total PA, vigorous PA, light PA (min/w) O | Not applicable | Significant between-group increase in MVPA, moderate PA and step counts favoring the intervention group | Low * (+,+,+,+,+) |
| Gell, 2020 [44] | Activity tracker for self-monitoring PA level and text messages to support PA engagement | Phone call | Inactive | Significant effect MVPA (min/w) O No significant effect Light PA (min/d) O, Adjusted light intensity time (% of day) O | No significant effect Sedentary time (min/d O) Adjusted sedentary time (% of day O) | Significant between-group increase in MVPA favoring the intervention group | Some concerns * (+,+,+,+,?) |
| Götte, 2018 [66] | Activity trackers assessing and providing feedback on PA during and after cancer treatment | In-person session | Active | No significant effect Daily step goal, active time goal (Goals achievement percentage,?) O | Not applicable | No significant between-group changes in either outcome | High ** (?,?,?,+,+,?,+) |
| Hartman, 2018 [52] | Activity tracker promoting behavior change | Phone calls and emails | Inactive | Significant effect MVPA, total activity (min/d) O, ?Number of participants meeting 150 min/w (n,?) | Not applicable | Significant between-group increase in MVPA, total activity and number of participant meeting 150 min/w favoring the intervention group | Low * (+,+,+,+,+) |
| Lynch, 2019 [38,39] | Activity tracker with the app providing inactivity alerts and assess PA | In-person session and phone call coaching | Inactive | Significant effect MVPA (min/w) O | Significant effect Sitting time (min/d) O | Significant between-group increase MVPA and decrease sitting time favoring the intervention group | Low * (+,+,+,+,+) |
| Maxwell–Smith, 2019 [56] | Activity tracker to record the daily activity and as an encouragement to increase PA target | Printed material, group sessions and phone call | Active | Significant effect MVPA, moderate PA (min/w) O No significant effect Proportion of MV10: MVPA accrued in bouts of at least 10 min (min/d) O | No significant effect SB (hours/w) O | Significant between-group increase in MVPA and moderate PA favoring the intervention group | Low * (+,+,+,+,+) |
| Mcneil, 2019 [61] | Activity tracker with app prescribing exercise intensity either lower or higher-intensity IG | Diary and phone call or email | Inactive | Significant effect MVPA (min/d) O No significant effect Total PA, Light–intensity PA (min/d) O | Significant effect Sedentary time (min/d) O | Significant between-group increase in MVPA and decrease in sedentary time favoring the low-intensity intervention group | Low * (+,+,+,+,+) |
| Mendoza, 2017 [40] | Activity tracker with an app to show goal progression and text messages for PA encouragement | Facebook group and phone call | Inactive | No significant effect MVPA (min/d) O | No significant effect SB (min/d) O | No significant between-group changes in outcome | Low * (+,+,+,+,+) |
| Singh, 2020 [53] | Activity tracker for self-monitoring and manage PA maintenance following supervised exercise intervention | In-person session and printed material | Active | Significant effect Walking, moderate PA, MVPA, total activity (min/w) S, Vigorous PA and MVPA (min/w) O No significant effect Vigorous PA (min/w) S, Moderate PA (min/w) O, Step counts (steps/d) O | Not applicable | Significant between-group increase in MVPA S, total activity S, moderate PA S, walking S, MVPA O and vigorous PA O favoring the intervention group | Some concerns * (+,+,+,?,+) |
| Valle, 2017 [51] | Activity tracker interfaced with an app to assess PA and providing feedback on PA | In-person session, wireless weighing scale and email | Active | No significant effect Energy expenditure (kcal/w) S | Not applicable | No significant between-group changes in outcome | Low * (+,+,+,+,+) |
| mHealth Only Intervention | ||||||
| First Author, Year | mHealth Intervention | Effects | Risk of Bias | |||
| PA | SB | Results Summary | ||||
| Cheong, 2018 [59] | Activity tracker with an app providing exercise program | No significant effect Total metabolic equivalent (METs/w) S | Not applicable | No significant change pre to post-intervention in an outcome | High * (?,?,?,?,?,?,+) | |
| Kim, 2020 [60] | Activity tracker with app prescribing exercise program | Significant effect Total metabolic equivalent (METs/w) S | Not applicable | Significant increase of METs pre to post-intervention | No information * (NI,?,+,+,?,?,+) | |
| Lozano-Lozano, 2019 [67] | App to monitor and provide feedback on health behaviors | Significant effect MVPA weekday (min/d) O No significant effect MVPA weekend, MVPA global (min/d) O Steps weekday, steps weekend, steps global (steps/d) O | Not applicable | Significant increase of MVPA weekday pre to post-intervention | No information * (NI,?,+,+,+,?,+) | |
| Puszkiewicz, 2016 [68] | App to provide PA program | Significant effect Strenuous PA, mild PA (min/w)S No significant effect Moderate PA (min/w) S | Not applicable | Significant increase in strenuous PA and a significant decrease in mild PA pre to post-intervention | High * (?,?,+,+,+,?,+) | |
| mHealth and multicomponent intervention | ||||||
| First Author, Year | mHealth intervention | Non-mHealth Intervention | Effects | Risk of Bias | ||
| PA | SB | Results Summary | ||||
| mHealth without personal contact intervention | ||||||
| Le, 2017 [41] | Motivational activity tracker to record PA | Website and exercise recommendations | No significant effect MVPA (min/d, min/wk) O Proportion of average total daily time doing MVPA and MVPA for at least 10 min day/w S | No significant effect Proportion of average screen time/day watching TV and days playing computer, video games, surfing the Internet S | No significant change pre to post-intervention in either outcome | No information * (NI,?,?,?,?,?,+) |
| McCarroll, 2015 [50] | App giving motivational feedback | Weighing scale | No significant effect PA times (min/w) S, Caloric expenditure (kcals/w) S | Not applicable | No significant change pre to post-intervention in either outcome | No information * (NI,?,+,+,+,?,+) |
| Trinh, 2018 [62] | Activity tracker to assess PA and provide alert to decrease SB | Web-based intervention | Significant effect MVPA (min/w) S, Step counts (steps/w) O No significant effect Light PA (min/w) O, Number of bouts spent in MVPA ≥ 10 min | Significant effect Sedentary time (min/w) S No significant effect Total time spent in SB bouts of ≥30 min (min/w) O, Number of breaks in time spent in SB bouts of ≥30 min | Significant increase of MVPA and step counts with significant reduction of sedentary time pre to post-intervention | No information * (NI,?,+,+,?,?,+) |
| mHealth with personal contact intervention | ||||||
| Delrieu, 2020 [63] | Activity tracker and app to monitor activity level | In-person or phone sessions | Significant effect Domestic PA (min/w) S No significant effect Total PA, recreational PA, moderate PA, vigorous PA, walking PA (MET-min/w) S, Participants proportions in low, moderate, and vigorous PA, n (%) | Significant effect Sitting time (min/w) S | Significant decrease in sitting time with significantly favoring a decrease in domestic PA pre to post-intervention | High * (-,?,+,+,+,?,+) |
| Gell, 2017 [43] | Activity tracker for self-monitoring activity and text messages to support PA | Phone call | No significant effect MVPA (min/w) O, Step counts (steps/d) O | Not applicable | No significant change pre to post-intervention in either outcome | No information * (NI,?,+,+,+,?,+) |
| Ovans, 2018 [45] | Activity tracker to show feedback and progress toward a goal | In-person or phone coaching | No significant effect Step counts (steps/d) O, Leisure score index S | Not applicable | No significant change pre to post-intervention in either outcome | High * (?,?,+,+,?,?,+) |
| Short, 2018 [55] | Recommended app according to individual characteristics | In-person session, printed material and a phone call or email | No significant effect MVPA, walking, moderate PA, vigorous PA (min/w) S | Not applicable | No significant change pre- to post-intervention in either outcome | No information * (NI,?,+,+,+,?,+) |
| Spark, 2015 [54] | Text messages for promoting behavioral change. | Phone call | No significant effect MVPA (min/d) O | Not applicable | No significant change pre to post-intervention in an outcome | High * (?,?,+,+,+,?,+) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khoo, S.; Mohbin, N.; Ansari, P.; Al-Kitani, M.; Müller, A.M. mHealth Interventions to Address Physical Activity and Sedentary Behavior in Cancer Survivors: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 5798. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115798
Khoo S, Mohbin N, Ansari P, Al-Kitani M, Müller AM. mHealth Interventions to Address Physical Activity and Sedentary Behavior in Cancer Survivors: A Systematic Review. International Journal of Environmental Research and Public Health. 2021; 18(11):5798. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115798
Chicago/Turabian StyleKhoo, Selina, Najihah Mohbin, Payam Ansari, Mahfoodha Al-Kitani, and Andre Matthias Müller. 2021. "mHealth Interventions to Address Physical Activity and Sedentary Behavior in Cancer Survivors: A Systematic Review" International Journal of Environmental Research and Public Health 18, no. 11: 5798. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115798