
Speaking Softly and Listening Hard: The Process of Involving Young Voices from a Culturally and Linguistically Diverse School in Child Health Research

 , , , ,
, , , ,  ,
,  and
and 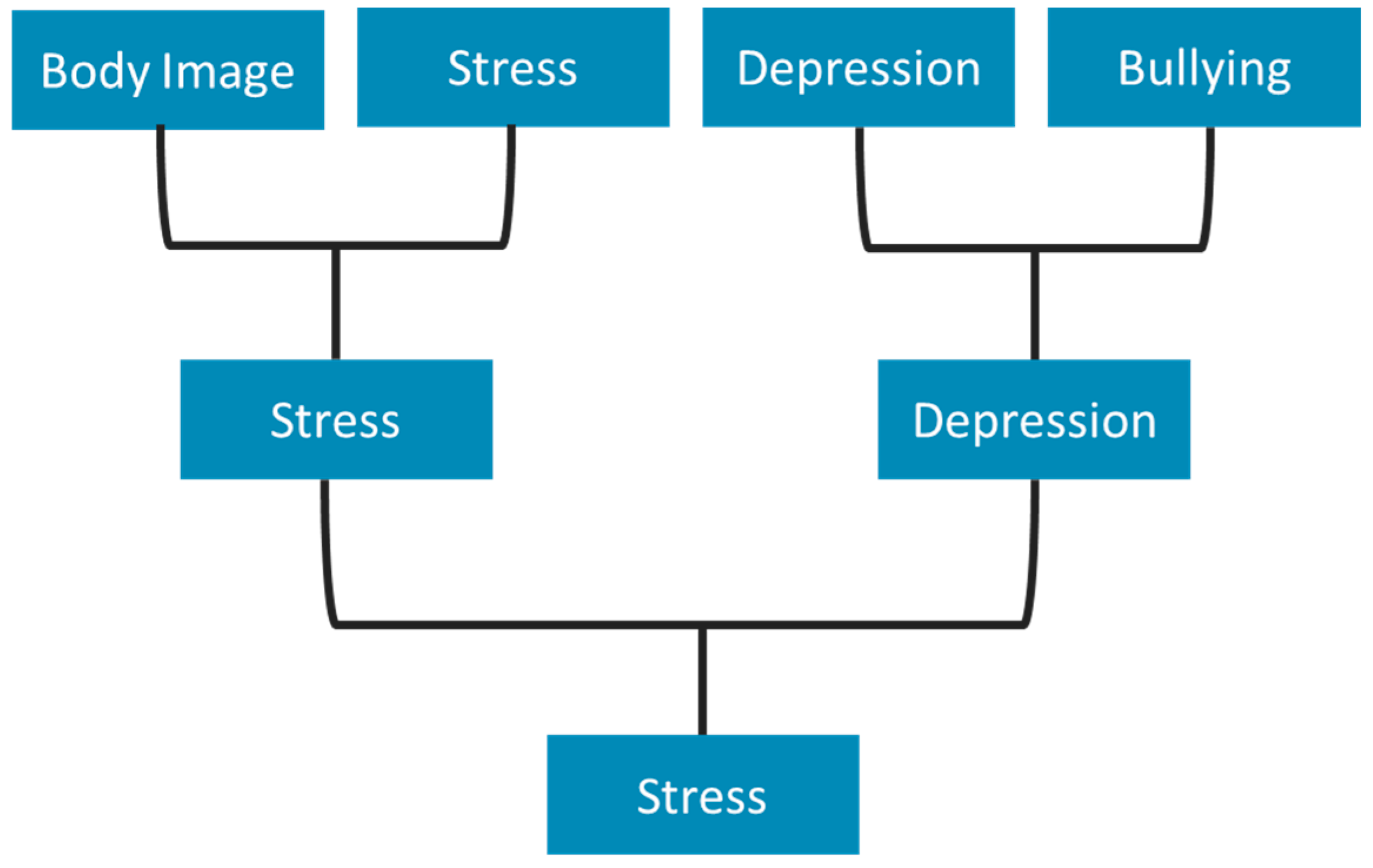{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics
2.2. Participants
2.3. Data Collection
2.4. Data Analysis
3. Themes
3.1. Approaching the Schools and Setting up the Groups
3.1.1. Strategies in Approaching Schools
3.1.2. Strategies to Approach Students
3.1.3. Strategies in Managing Regulatory Approval
3.2. Establishing and Running the Groups
3.2.1. Fostering Trust with Students
3.2.2. (Re)negotiating School Access
3.3. Exploring Health Priorities: The Emergence of Mental Health as a Priority Area
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Grace, R.; Knight, J.; Baird, K.; Ng, J.; Shier, H.; Wise, S.; Fattore, T.; McClean, T.; Bonser, G.; Judd-Lam, S.; et al. Where are the silences? A scoping review of child participatory research literature in the context of the Australian service system. Child. Aust. 2019, 44, 172–186. [Google Scholar] [CrossRef] [Green Version]
- Byers, V. The challenges of leading change in health-care delivery from the front-line. J. Nurs. Manag. 2015, 25, 449–456. [Google Scholar] [CrossRef] [Green Version]
- Agency for Clinical Innovation. A Guide to Build Co-Design Capability: Consumers and Staff Coming Together to Improve Healthcare, in Patient Experience and Consumer Engagement; Agency for Clinical Innovation: Chatswood, Australia, 2019. [Google Scholar]
- Sanders, E.B.-N.; Stappers, P.J. Co-creation and the new landscapes of design. Co-Design 2008, 4, 5–18. [Google Scholar] [CrossRef] [Green Version]
- Hawkins, J.; Madden, K.; Fletcher, A.; Midgley, L.; Grant, A.; Cox, G.; Moore, L.; Campbell, R.; Murphy, S.; Bonell, C.; et al. Development of a framework for the co-production and prototyping of public health interventions. BMC Public Health 2017, 17, 689. [Google Scholar] [CrossRef]
- Millstein, S.G.; Ozer, E.J.; Ozer, E.M.; Brindis, C.D.; Knopf, D.K.; Irwin, C.E., Jr. Research Priorities in Adolescent Health: An Analysis and Synthesis of Research Recommendations. 1999. Available online: https://eric.ed.gov/?id=ED449456 (accessed on 16 March 2021).
- McMurray, A. Community Health and Wellness: A Socio-Ecological Approach; Elsevier: Amsterdam, The Netherlands, 2007. [Google Scholar]
- Goodhew, M.; Stein-Parbury, J.; Dawson, A. Consumer participation in drug treatment: A systematic review. Drugs Alcohol Today 2019, 19, 97–112. [Google Scholar] [CrossRef] [Green Version]
- Nathan, S.; Braithwaite, J.; Stephenson, N. Sidestepping questions of legitimacy: How community representatives manoeuvre to effect change in a health service. Health 2014, 18, 23–40. [Google Scholar] [CrossRef] [PubMed]
- Nathan, S.; Braithwaite, J.; Stephenson, N. The scope and impact of community participation: The views of community representatives in an Australian health service. J. Health Organ. Manag. 2014, 28, 405–421. [Google Scholar] [CrossRef]
- Shé, É.N.; Cassidy, J.; Davies, C.; De Brún, A.; Donnelly, S.; Dorris, E.; Dunne, N.; Egan, K.; Foley, M.; Galvin, M.; et al. Minding the gap: Identifying values to enable public and patient involvement at the pre-commencement stage of research projects. Res. Involv. Engag. 2020, 6, 46. [Google Scholar] [CrossRef] [PubMed]
- Swist, T.; Collin, P.; Nguyen, B.; Steinbeck, K.; Dawson, A. Wellbeing Health & Youth Engagement Framework; WH&Y Centre of Research Excellence: Sydney, Australia, 2019. [Google Scholar]
- Powers, J.L.; Tiffany, J.S. Engaging Youth in Participatory Research and Evaluation. J. Public Health Manag. Pract. 2006, 12, S79–S87. [Google Scholar] [CrossRef]
- Jenkins, E.K.; Bungay, V.; Patterson, A.; Saewyc, E.M.; Johnson, J.L. Assessing the impacts and outcomes of youth driven mental health promotion: A mixed-methods assessment of the Social Networking Action for Resilience study. J. Adolesc. 2018, 67, 1–11. [Google Scholar] [CrossRef]
- Vaughn, L.M.; Wagner, E.; Jacquez, F. A Review of Community-Based Participatory Research in Child Health. MCN Am. J. Matern. Nurs. 2013, 38, 48–53. [Google Scholar] [CrossRef] [PubMed]
- Coad, J.; Lewis, A. Engaging Children and Young People in Research; The National Evaluation of the Children’s Fund: London, UK, 2004. [Google Scholar]
- Thomas, N.; O’Kane, C. The ethics of participatory research with children. Child. Soc. 1998, 12, 336–348. [Google Scholar] [CrossRef]
- Christensen, P.; James, A. Research with Children: Perspectives and Practices; Routledge: London, UK, 2008. [Google Scholar]
- Garth, B.; Aroni, R. ‘I Value What You have to Say’. Seeking the Perspective of Children with a Disability, Not Just their Parents. Disabil. Soc. 2003, 18, 561–576. [Google Scholar] [CrossRef]
- Fleming, J. Young People’s Involvement in Research: Still a Long Way to Go? Qual. Soc. Work 2010, 10, 207–223. [Google Scholar] [CrossRef]
- Involve, U.K. Involving Children and Young People in Research: Top Tips and Essential Key Issues for Researchers; Eastleigh: Eastleigh, UK, 2016. [Google Scholar]
- South Western Sydney Local Health District. Vision, Mission and Principles of Your Health District; South Western Sydney Local Health District: Liverpool, Australia, 2017. [Google Scholar]
- Horobin, A.; Hall, D. No Research about Me without Me—Why Researchers Should Welcome the Patient’s Voice. 2018. Available online: http://0-blogs-biomedcentral-com.brum.beds.ac.uk/blog/author/adelehall/ (accessed on 18 March 2021).
- Stafford, L. ‘What about my voice’: Emancipating the voices of children with disabilities through participant-centred methods. Child. Geogr. 2017, 15, 600–613. [Google Scholar] [CrossRef] [Green Version]
- Tisdall, E.K.M. The Challenge and Challenging of Childhood Studies? Learning from Disability Studies and Research with Disabled Children. Child. Soc. 2012, 26, 181–191. [Google Scholar] [CrossRef] [Green Version]
- Beazley, H.; Bessell, S.; Ennew, J.; Waterson, R. The right to be properly researched: Research with children in a messy, real world. Child. Geogr. 2009, 7, 365–378. [Google Scholar] [CrossRef]
- O’Mara-Eves, A.; Brunton, G.; McDaid, D.; Oliver, S.; Kavanagh, J.; Jamal, F.; Matosevic, T.; Hardenberg, A.; Thomas, J. Community engagement to reduce inequalities in health: A systematic review, meta-analysis and economic analysis. Public Health Res. 2013, 1. [Google Scholar] [CrossRef] [Green Version]
- Cyril, S.; Smith, B.J.; Possamai-Inesedy, A.; Renzaho, A.M.N. Exploring the role of community engagement in improving the health of disadvantaged populations: A systematic review. Glob. Health Action 2015, 8, 29842. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferrera, M.J.; Sacks, T.K.; Perez, M.; Nixon, J.P.; Asis, D.; Coleman, R.W. Empowering immigrant youth in Chicago: Utilizing CBPR to document the impact of a Youth Health Service Corps program. Fam. Community Health 2015, 38, 12–21. [Google Scholar] [CrossRef] [PubMed]
- Spyrou, S. The limits of children’s voices: From authenticity to critical, reflexive representation. Childhood 2011, 18, 151–165. [Google Scholar] [CrossRef] [Green Version]
- MH:2K Oldham a Youth-Led Approach to Exploring Mental Health. 2017. Available online: https://www.involve.org.uk/sites/default/files/uploads/MH2K-Oldham-Summary-Report.pdf (accessed on 26 March 2021).
- MH:2K Final Evaluation Report. 2017. Available online: https://www.involve.org.uk/sites/default/files/uploads/MH2K-Oldham-final-evaluation-report.pdf (accessed on 2 April 2021).
- Irby, M.; Moore, K.; Mann-Jackson, L.; Hamlin, D.; Randall, I.; Summers, P.; Skelton, J.; Daniel, S.; Rhodes, S. Community-Engaged Research: Common Themes and Needs Identified by Investigators and Research Teams at an Emerging Academic Learning Health System. Int. J. Environ. Res. Public Health 2021, 18, 3893. [Google Scholar] [CrossRef] [PubMed]
- Hayes, H.; Buckland, S.; Tarpey, M. Briefing Notes for Researchers: Public Involvement in NHS, Public Health and Social Care Research; Involve Coordinating Centre: Eastleigh, UK, 2012. [Google Scholar]
- Brett, J.; Staniszewska, S.; Mockford, C.; Herron-Marx, S.; Hughes, J.; Tysall, C.; Suleman, R. Mapping the impact of patient and public involvement on health and social care research: A systematic review. Health Expect. 2014, 17, 637–650. [Google Scholar] [CrossRef] [PubMed]
- Nierse, C.J.; Abma, T.A. Developing voice and empowerment: The first step towards a broad consultation in research agenda setting. J. Intellect. Disabil. Res. 2011, 55, 411–421. [Google Scholar] [CrossRef]
- McLaughlin, M.W.; Talbert, J.E. Building School-Based Teacher Learning Communities: Professional Strategies to Improve Student Achievement; Teachers College Press: New York, NY, USA, 2006. [Google Scholar]
- Bishop, K. Challenging Research: Completing Participatory Social Research with Children and Adolescents in a Hospital Setting. HERD Health Environ. Res. Des. J. 2014, 7, 76–91. [Google Scholar] [CrossRef]
- Clark, M.; Glasby, J.; Lester, H. Cases for change: User involvement in mental health services and research. Res. Policy Plan. 2004, 22, 31–38. [Google Scholar]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Samir, N.; Diaz, A.M.; Hodgins, M.; Matic, S.; Bawden, S.; Khoury, J.; Eapen, V.; Lingam, R. Speaking Softly and Listening Hard: The Process of Involving Young Voices from a Culturally and Linguistically Diverse School in Child Health Research. Int. J. Environ. Res. Public Health 2021, 18, 5808. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115808
Samir N, Diaz AM, Hodgins M, Matic S, Bawden S, Khoury J, Eapen V, Lingam R. Speaking Softly and Listening Hard: The Process of Involving Young Voices from a Culturally and Linguistically Diverse School in Child Health Research. International Journal of Environmental Research and Public Health. 2021; 18(11):5808. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115808
Chicago/Turabian StyleSamir, Nora, Antonio Mendoza Diaz, Michael Hodgins, Simone Matic, Samira Bawden, Jessica Khoury, Valsamma Eapen, and Raghu Lingam. 2021. "Speaking Softly and Listening Hard: The Process of Involving Young Voices from a Culturally and Linguistically Diverse School in Child Health Research" International Journal of Environmental Research and Public Health 18, no. 11: 5808. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115808