
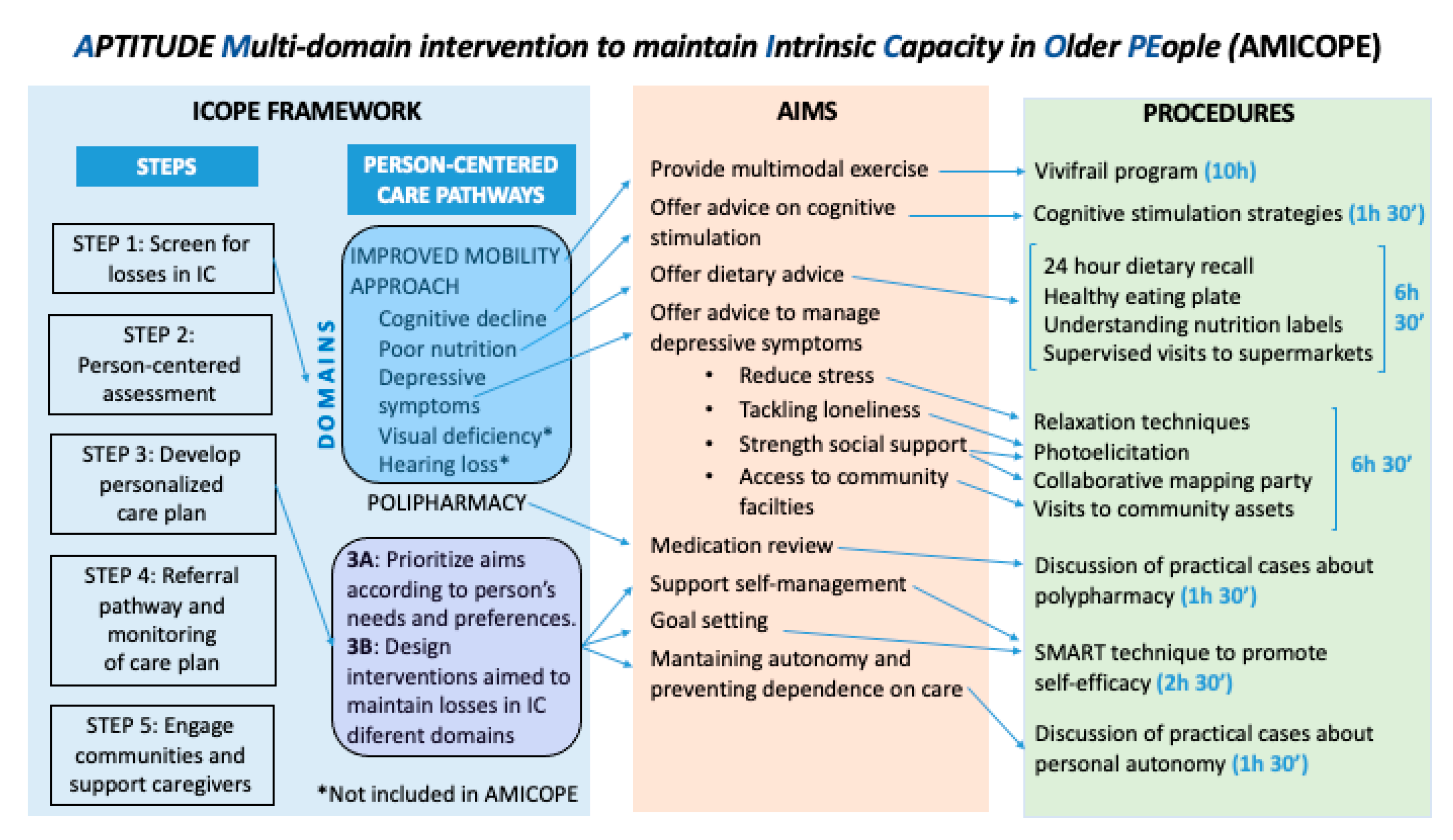
A Multi-Domain Group-Based Intervention to Promote Physical Activity, Healthy Nutrition, and Psychological Wellbeing in Older People with Losses in Intrinsic Capacity: AMICOPE Development Study

 , , , , ,
, , , , ,  , , and
, , and {kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chatterji, S.; Byles, J.; Cutler, D.; Seeman, T.; Verdes, E. Health, functioning, and disability in older adults—Present status and future implications. Lancet 2015, 385, 563–575. [Google Scholar] [CrossRef] [Green Version]
- Marengoni, A.; Angleman, S.; Melis, R.; Mangialasche, F.; Karp, A.; Garmen, A.; Meinow, B.; Fratiglioni, L. Aging with multimorbidity: A systematic review of the literature. Ageing Res. Rev. 2011, 10, 430–439. [Google Scholar] [CrossRef] [PubMed]
- Arokiasamy, P.; Uttamacharya, U.; Jain, K.; Biritwum, R.B.; Yawson, A.E.; Wu, F.; Guo, Y.; Maximova, T.; Espinoza, B.M.; Rodríguez, A.S.; et al. The impact of multimorbidity on adult physical and mental health in low- and middle-income countries: What does the study on global ageing and adult health (SAGE) reveal? BMC Med. 2015, 13, 178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Inouye, S.K.; Studenski, S.; Tinetti, M.E.; Kuchel, G.A. Geriatric syndromes: Clinical, research, and policy implications of a core geriatric concept. J. Am. Geriatr. Soc. 2007, 55, 780–791. [Google Scholar] [CrossRef] [PubMed]
- Fried, L.P.; Ferrucci, L.; Darer, J.; Williamson, J.D.; Anderson, G. Untangling the concepts of disability, frailty, and comorbidity: Implications for improved targeting and care. J. Gerontol. 2004, 59, 255–263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clegg, A.; Young, J.; Iliffe, S.; Rikkert, M.O.; Rockwood, K. Frailty in elderly people. Lancet 2013, 381, 752–762. [Google Scholar] [CrossRef] [Green Version]
- Harttgen, K.; Kowal, P.; Strulik, H.; Chatterji, S.; Vollmer, S. Patterns of frailty in older adults: Comparing results from higher and lower income countries using the Survey of Health, Ageing and Retirement in Europe (SHARE) and the Study on Global AGEing and Adult Health (SAGE). PLoS ONE 2013, 8, e75847. [Google Scholar] [CrossRef] [Green Version]
- Beard, J.R.; Officer, A.; de Carvalho, I.A.; Sadana, R.; Pot, A.M.; Michel, J.P.; Lloyd-Sherlock, P.; Epping-Jordan, J.E.; Peeters, G.; Mahanani, W.R.; et al. The World report on ageing and health: A policy framework for healthy ageing. Lancet 2016, 387, 2145–2154. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Active Ageing: A Policy Framework; WHO: Geneva, Switzerland, 2002. [Google Scholar]
- Stuck, A.E.; Siu, A.L.; Wieland, G.D.; Adams, J.; Rubenstein, L.Z. Comprehensive geriatric assessment: A meta-analysis of controlled trials. Lancet 1993, 342, 1032–1036. [Google Scholar] [CrossRef]
- World Health Organization. Integrated Care for older People (ICOPE): Guidance for Person-Centered Assessment and Pathways in Primary Care; WHO: Geneva, Switzerland, 2019. [Google Scholar]
- van Het Bolscher-Niehuis, M.J.; den Ouden, M.E.; de Vocht, H.M.; Francke, A.L. Effects of self-management support programmes on activities of daily living of older adults: A systematic review. Int. J. Nurs. Stud. 2016, 61, 230–247. [Google Scholar] [CrossRef] [Green Version]
- Pescheny, J.V.; Randhawa, G.; Pappas, Y. The impact of social prescribing services on service users: A systematic review of the evidence. Eur. J. Public Health 2020, 30, 664–673. [Google Scholar] [CrossRef]
- Cesari, M.; Araujo de Carvalho, I.; Thiyagarajan, J.A.; Cooper, C.; Martin, F.C.; Reginster, J.Y.; Vellas, B.; Beard, J.R. Evidence for the Domains Supporting the Construct of Intrinsic Capacity. J. Gerontol. 2018, 73, 1653–1660. [Google Scholar] [CrossRef] [Green Version]
- Nestola, T.; Orlandini, L.; Beard, J.R.; Cesari, M. COVID-19 and Intrinsic Capacity. J. Nutr. Health Aging 2020, 24, 692–695. [Google Scholar] [CrossRef]
- Apóstolo, J.; Cooke, R.; Bobrowicz-Campos, E.; Santana, S.; Marcucci, M.; Cano, A.; Vollenbroek-Hutten, M.; Germini, F.; D’Avanzo, B.; Gwyther, H.; et al. Effectiveness of interventions to prevent pre-frailty and frailty progression in older adults: A systematic review. JBI Database Syst. Rev. Implement. Rep. 2018, 16, 140–232, Erratum in 2018, 16, 1282–1283. [Google Scholar] [CrossRef] [PubMed]
- Landi, F.; Abbatecola, A.M.; Provinciali, M.; Corsonello, A.; Bustacchini, S.; Manigrasso, L.; Cherubini, A.; Bernabei, R.; Lattanzio, F. Moving against frailty: Does physical activity matter? Biogerontology 2010, 11, 537–545. [Google Scholar] [CrossRef]
- Dent, E.; Morley, J.E.; Cruz-Jentoft, A.J.; Woodhouse, L.; Rodríguez-Mañas, L.; Fried, L.P.; Woo, J.; Aprahamian, I.; Sanford, A.; Lundy, J.; et al. Physical Frailty: ICFSR International Clinical Practice Guidelines for Identification and Management. J. Nutr. Health Aging 2019, 23, 771–787. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Casas Herrero, Á.; Cadore, E.L.; Martínez Velilla, N.; Izquierdo Redin, M. El ejercicio físico en el anciano frágil: Una actualización [Physical exercise in the frail elderly: An update]. Rev. Esp. Geriatr. Gerontol. 2015, 50, 74–81. [Google Scholar] [CrossRef]
- Tarazona-Santabalbina, F.J.; Gómez-Cabrera, M.C.; Pérez-Ros, P.; Martínez-Arnau, F.M.; Cabo, H.; Tsaparas, K.; Salvador-Pascual, A.; Rodriguez-Mañas, L.; Viña, J.A. Multicomponent Exercise Intervention that Reverses Frailty and Improves Cognition, Emotion, and Social Networking in the Community-Dwelling Frail Elderly: A Randomized Clinical Trial. J. Am. Med. Dir. Assoc. 2016, 17, 426–433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martínez-Velilla, N.; Casas-Herrero, A.; Zambom-Ferraresi, F.; Sáez de Asteasu, M.L.; Lucia, A.; Galbete, A.; García-Baztán, A.; Alonso-Renedo, J.; González-Glaría, B.; Gonzalo-Lázaro, M.; et al. Effect of Exercise Intervention on Functional Decline in Very Elderly Patients during Acute Hospitalization: A Randomized Clinical Trial. JAMA Intern. Med. 2019, 179, 28–36. [Google Scholar] [CrossRef]
- Sáez de Asteasu, M.L.; Martínez-Velilla, N.; Zambom-Ferraresi, F.; Casas-Herrero, Á.; Cadore, E.L.; Galbete, A.; Izquierdo, M. Assessing the impact of physical exercise on cognitive function in older medical patients during acute hospitalization: Secondary analysis of a randomized trial. PLoS Med. 2019, 16, e1002852. [Google Scholar] [CrossRef]
- Sáez de Asteasu, M.L.; Martínez-Velilla, N.; Zambom-Ferraresi, F.; Casas-Herrero, Á.; Cadore, E.L.; Ramirez-Velez, R.; Izquierdo, M. Inter-individual variability in response to exercise intervention or usual care in hospitalized older adults. J. Cachexia Sarcopenia Muscle 2019, 10, 1266–1275. [Google Scholar] [CrossRef] [Green Version]
- Sáez de Asteasu, M.L.; Martínez-Velilla, N.; Zambom-Ferraresi, F.; Ramírez-Vélez, R.; García-Hermoso, A.; Cadore, E.L.; Casas-Herrero, Á.; Galbete, A.; Izquierdo, M. Changes in muscle power after usual care or early structured exercise intervention in acutely hospitalized older adults. J. Cachexia Sarcopenia Muscle 2019, 11, 997–1006. [Google Scholar] [CrossRef] [Green Version]
- Sáez de Asteasu, M.L.; Martínez-Velilla, N.; Zambom-Ferraresi, F.; Casas-Herrero, Á.; Millor, N.; Izquierdo, M. Quantifying physical functional trajectory in hospitalized older adults using body worn inertial sensors. J. Biomech. 2019, 92, 105–111. [Google Scholar] [CrossRef] [PubMed]
- Sáez de Asteasu, M.L.; Martínez-Velilla, N.; Zambom-Ferraresi, F.; Casas-Herrero, Á.; Lucía, A.; Galbete, A.; Izquierdo, M. Physical Exercise Improves Function in Acutely Hospitalized Older Patients: Secondary Analysis of a Randomized Clinical Trial. J. Am. Med. Dir. Assoc. 2019, 20, 866–873. [Google Scholar] [CrossRef]
- Sáez de Asteasu, M.L.; Martínez-Velilla, N.; Zambom-Ferraresi, F.; Ramirez-Vélez, R.; Izquierdo, M. Role of muscle power output as a mediator between gait variability and gait velocity in hospitalized older adults. Exp. Gerontol. 2019, 124, 110631. [Google Scholar] [CrossRef]
- Martínez-Velilla, N.; Valenzuela, P.L.; Zambom-Ferraresi, F.; Sáez de Asteasu, M.L.; Ramírez-Vélez, R.; García-Hermoso, A.; Lucia, A.; Izquierdo, M. Tailored exercise is safe and beneficial for acutely hospitalised older adults with COPD. Eur. Respir. J. 2020, 56, 2001048. [Google Scholar] [CrossRef] [PubMed]
- Sáez de Asteasu, M.L.; Martínez-Velilla, N.; Zambom-Ferraresi, F.; Ramírez-Vélez, R.; García-Hermoso, A.; Izquierdo, M. Cognitive Function Improvements Mediate Exercise Intervention Effects on Physical Performance in Acutely Hospitalized Older Adults. J. Am. Med. Dir. Assoc. 2020, 22, 787–791. [Google Scholar] [CrossRef] [PubMed]
- Ramírez-Vélez, R.; García-Hermoso, A.; Martínez-Velilla, N.; Zambom-Ferraresi, F.; Sáez de Asteasu, M.L.; Recarey, A.E.; Izquierdo, M. Effects of Exercise Interventions on Inflammatory Parameters in Acutely Hospitalized Older Patients: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Clin. Med. 2021, 10, 290. [Google Scholar] [CrossRef]
- Sáez de Asteasu, M.L.; Martínez-Velilla, N.; Zambom-Ferraresi, F.; Ramírez-Vélez, R.; García-Hermoso, A.; Cadore, E.L.; Izquierdo, M. Exercise Effects on Brain and Muscle Function in Acutely Hospitalized Older Patients Assessed by Functional Near-Infrared Spectroscopy. J. Am. Med. Dir. Assoc. 2021, 22, 875–876. [Google Scholar] [CrossRef]
- Ramírez-Vélez, R.; Sáez de Asteasu, M.L.; Martínez-Velilla, N.; Zambom-Ferraresi, F.; García-Hermoso, A.; Izquierdo, M. Handgrip Strength as a Complementary Test for Mobility Limitations Assessment in Acutely Hospitalized Oldest Old. Rejuvenation Res. 2021. [Google Scholar] [CrossRef]
- Martínez-Velilla, N.; Valenzuela, P.L.; Sáez de Asteasu, M.L.; Zambom-Ferraresi, F.; Ramírez-Vélez, R.; García-Hermoso, A.; Librero-López, J.; Gorricho, J.; Pérez, F.E.; Lucia, A.; et al. Effects of a Tailored Exercise Intervention in Acutely Hospitalized Oldest Old Diabetic Adults: An Ancillary Analysis. J. Clin. Endocrinol. Metab. 2021, 106, e899–e906. [Google Scholar] [CrossRef]
- Martínez-Velilla, N.; Sáez de Asteasu, M.L.; Ramírez-Vélez, R.; Zambom-Ferraresi, F.; García-Hermoso, A.; Izquierdo, M. Recovery of the decline in activities of daily living after hospitalization through an individualized exercise programme: Secondary Analysis of a Randomized Clinical Trial. J. Gerontol. 2021. [Google Scholar] [CrossRef]
- Martínez Velilla, N.; Ramírez-Vélez, R.; Sáez de Asteasu, M.L.; Zambom-Ferraresi, F.; Garcia Hermoso, A.; Marín Epelde, I.; Izquierdo, M. Red Cell Distribution Width (RDW) Trajectory During a Multicomponent Exercise in Hospitalized Older Adults: A Secondary Analysis of a Randomized Clinical Trial. Rejuvenation Res. 2021. [Google Scholar] [CrossRef]
- Vásquez-Araneda, E.; Solís-Vivanco, R.I.; Mahecha-Matsudo, S.; Zapata-Lamana, R.; Cigarroa, I. Characteristics of Physical Exercise Programs for Older Adults in Latin America: A Systematic Review of Randomized Controlled Trials. Int. J. Environ. Res. Public Health 2021, 18, 2812. [Google Scholar] [CrossRef] [PubMed]
- Cadore, E.L.; Casas-Herrero, A.; Zambom-Ferraresi, F.; Idoate, F.; Millor, N.; Gómez, M.; Rodriguez-Mañas, L.; Izquierdo, M. Multicomponent exercises including muscle power training enhance muscle mass, power output, and functional outcomes in institutionalized frail nonagenarians. Age 2014, 36, 773–785. [Google Scholar] [CrossRef] [Green Version]
- Fiatarone, M.A.; O’Neill, E.F.; Ryan, N.D.; Clements, K.M.; Solares, G.R.; Nelson, M.E.; Roberts, S.B.; Kehayias, J.J.; Lipsitz, L.A.; Evans, W.J. Exercise training and nutritional supplementation for physical frailty in very elderly people. N. Engl. J. Med. 1994, 330, 1769–1775. [Google Scholar] [CrossRef] [Green Version]
- Woo, J. Nutrition and Frailty. J. Nutr. Health Ageing 2018, 22, 1025–1027. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zak, M.; Swine, C.; Grodzicki, T. Combined effects of functionally-oriented exercise regimens and nutritional supplementation on both the institutionalised and free-living frail elderly (double-blind, randomised clinical trial). BMC Public Health 2009, 9, 39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nilsson, M.I.; Mikhail, A.; Lan, L.; Di Carlo, A.; Hamilton, B.; Barnard, K.; Hettinga, B.P.; Hatcher, E.; Tarnopolsky, M.G.; Nederveen, J.P.; et al. A Five-Ingredient Nutritional Supplement and Home-Based Resistance Exercise Improve Lean Mass and Strength in Free-Living Elderly. Nutrients 2020, 12, 2391. [Google Scholar] [CrossRef]
- Zhou, X.; Perez-Cueto, F.; Santos, Q.D.; Monteleone, E.; Giboreau, A.; Appleton, K.M.; Bjørner, T.; Bredie, W.; Hartwell, H. A Systematic Review of Behavioural Interventions Promoting Healthy Eating among Older People. Nutrients 2018, 10, 128. [Google Scholar] [CrossRef] [Green Version]
- Hollon, S.D.; Stewart, M.O.; Strunk, D. Enduring effects for cognitive behavior therapy in the treatment of depression and anxiety. Annu. Rev. Psychol. 2006, 57, 285–315. [Google Scholar] [CrossRef] [Green Version]
- Krishna, M.; Jauhari, A.; Lepping, P.; Turner, J.; Crossley, D.; Krishnamoorthy, A. Is group psychotherapy effective in older adults with depression? A systematic review. Int. J. Geriatr. Psychiatry 2011, 26, 331–340. [Google Scholar] [CrossRef]
- Coll-Planas, L.; Nyqvist, F.; Puig, T.; Urrútia, G.; Solà, I.; Monteserín, R. Social capital interventions targeting older people and their impact on health: A systematic review. J. Epidemiol. Community Health 2017, 71, 663–672. [Google Scholar] [CrossRef] [PubMed]
- French, D.P.; Olander, E.K.; Chisholm, A.; Mc Sharry, J. Which behaviour change techniques are most effective at increasing older adults’ self-efficacy and physical activity behaviour? A systematic review. Ann. Behav. Med. 2014, 48, 225–234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lachman, M.E.; Lipsitz, L.; Lubben, J.; Castaneda-Sceppa, C.; Jette, A.M. When Adults Don’t Exercise: Behavioral Strategies to Increase Physical Activity in Sedentary Middle-Aged and Older Adults. Innov. Aging 2018, 2. [Google Scholar] [CrossRef]
- Chase, J.A. Physical activity interventions among older adults: A literature review. Res. Theory Nurs. Pract. 2013, 27, 53–80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoddinott, P.; Allan, K.; Avenell, A.; Britten, J. Group interventions to improve health outcomes: A framework for their design and delivery. BMC Public Health 2010, 10, 800. [Google Scholar] [CrossRef] [Green Version]
- Toseland, R.W.; Rossiter, C.M.; Peak, T.; Smith, G.C. Comparative effectiveness of individual and group interventions to support family caregivers. Soc. Work 1990, 35, 209–217. [Google Scholar]
- Paul-Ebhohimhen, V.; Avenell, A. A systematic review of the effectiveness of group versus individual treatments for adult obesity. Obes. Facts 2009, 2, 17–24. [Google Scholar] [CrossRef]
- Chi, Y.C.; Sha, F.; Yip, P.S.F.; Chen, J.L.; Chen, Y.Y. Randomized comparison of group versus individual educational interventions for pregnant women to reduce their secondhand smoke exposure. Medicine 2016, 95, e5072. [Google Scholar] [CrossRef] [Green Version]
- Booth, A.; Cantrell, A.; Preston, L.; Chambers, D.; Goyder, E. What is the evidence for the effectiveness, appropriateness and feasibility of group clinics for patients with chronic conditions? A systematic review. Health Serv. Deliv. Res. 2015, 3, 1–194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haslam, C.; Haslam, S.A.; Jetten, J.; Bevins, A.; Ravenscroft, S.; Tonks, J. The social treatment: The benefits of group interventions in residential care settings. Psychol. Aging 2010, 25, 157–167. [Google Scholar] [CrossRef] [PubMed]
- Borek, A.J.; Abraham, C. How do small groups promote behaviour change? An integrative conceptual review of explanatory mechanisms. Appl. Psychol. Health Well Being 2018, 10, 30–61. [Google Scholar] [CrossRef] [Green Version]
- Greaves, C.J.; Campbell, J.L. Supporting self-care in general practice. Br. J. Gen. Pract. 2007, 57, 814–821. [Google Scholar] [PubMed]
- Duncan, E.; O’Cathain, A.; Rousseau, N.; Croot, L.; Sworn, K.; Turner, K.M.; Yardley, L.; Hoddinott, P. Guidance for reporting intervention development studies in health research (GUIDED): An evidence-based consensus study. BMJ Open 2020, 10, e033516. [Google Scholar] [CrossRef] [Green Version]
- Hoffmann, T.C.; Glasziou, P.P.; Boutron, I.; Milne, R.; Perera, R.; Moher, D.; Altman, D.G.; Barbour, V.; Macdonald, H.; Johnston, M.; et al. Better reporting of interventions: Template for intervention description and replication (TIDieR) checklist and guide. Br. Med. J. 2014, 348, g1687. [Google Scholar] [CrossRef] [Green Version]
- APTITUDE. Un Réseau Transpyrénéen au Service des Personnes Âgées. Available online: http://www.aptitude-net.com (accessed on 18 March 2021).
- Bases Conceptuals i Model D’atenció Per a Les Persones Fràgils, Amb Cronicitat Complexa (PCC) o Avançada (MACA). Department of Health, Government of Catalonia. Available online: https://salutweb.gencat.cat/web/.content/_ambits-actuacio/Linies-dactuacio/Estrategies-de-salut/Cronicitat/Documentacio-cronicitat/arxius/Model-de-Bases-de-Cronicitat.pdf (accessed on 18 March 2021).
- O’Cathain, A.; Croot, L.; Duncan, E.; Rousseau, N.; Sworn, K.; Turner, K.M.; Yardley, L.; Hoddinott, P. Guidance on how to develop complex interventions to improve health and healthcare. BMJ Open 2019, 9, e029954. [Google Scholar] [CrossRef] [Green Version]
- Blancafort Alias, S.; Monteserín Nadal, R.; Moral, I.; Roqué Fígols, M.; Rojano Luque, X.; Coll-Planas, L. Promoting social capital, self-management and health literacy in older adults through a group-based intervention delivered in low-income urban areas: Results of the randomized trial AEQUALIS. BMC Public Health 2021, 21, 84. [Google Scholar] [CrossRef]
- Izquierdo, M.; Casas-Herrero, A.; Zambom-Ferraresi, F.; Martínez-Velilla, N.; Alonso-Bouzón, C.; Rodríguez-Mañas, L. Multicomponent Physical Exercise Program VIVIFRAIL. 2017. Available online: http://vivifrail.com/resources/ (accessed on 8 March 2021).
- Coll-Planas, L.; Blancafort, S.; Rojano, X.; Roqué, M.; Monteserín, R. Promoting self-management, health literacy and social capital to reduce health inequalities in older adults living in urban disadvantaged areas: Protocol of the randomised controlled trial AEQUALIS. BMC Public Health 2018, 18, 345. [Google Scholar] [CrossRef]
- Intervención Multi-Componente AMICOPE. Available online: https://www.aptitude-net.com/es/intervencion-multi-componente-amicope (accessed on 8 May 2021).
- de Moraes, M.B.; Avgerinou, C.; Fukushima, F.B.; Vidal, E. Nutritional interventions for the management of frailty in older adults: Systematic review and meta-analysis of randomized clinical trials. Nutr. Rev. 2020. [Google Scholar] [CrossRef]
- Chiu, H.L.; Chu, H.; Tsai, J.C.; Liu, D.; Chen, Y.R.; Yang, H.L.; Chou, K.R. The effect of cognitive-based training for the healthy older people: A meta-analysis of randomized controlled trials. PLoS ONE 2017, 12, e0176742. [Google Scholar] [CrossRef] [PubMed]
- George, J.; Elliott, R.A.; Stewart, D.C. A systematic review of interventions to improve medication taking in elderly patients prescribed multiple medications. Drugs Aging 2008, 25, 307–324. [Google Scholar] [CrossRef] [PubMed]
- Boulos, C.; Salameh, P.; Barberger-Gateau, P. Social isolation and risk for malnutrition among older people. Geriatr. Gerontol. Int. 2017, 17, 286–294. [Google Scholar] [CrossRef] [PubMed]
- Epton, T.; Currie, S.; Armitage, C.J. Unique effects of setting goals on behavior change: Systematic review and meta-analysis. J. Consult. Clin. Psychol. 2017, 85, 1182–1198. [Google Scholar] [CrossRef]
- Shilts, M.K.; Horowitz, M.; Townsend, M.S. Goal setting as a strategy for dietary and physical activity behavior change: A review of the literature. Am. J. Health Promot. 2004, 19, 81–93. [Google Scholar] [CrossRef]
- Vermunt, N.; Harmsen, M.; Westert, G.P.; Olde Rikkert, M.; Faber, M.J. Collaborative goal setting with elderly patients with chronic disease or multimorbidity: A systematic review. BMC Geriatr. 2017, 17, 167. [Google Scholar] [CrossRef]
- Sagar-Ouriaghli, I.; Godfrey, E.; Graham, S.; Brown, J. Improving Mental Health Help-Seeking Behaviours for Male Students: A Framework for Developing a Complex Intervention. Int. J. Environ. Res. Public Health 2020, 17, 4965. [Google Scholar] [CrossRef]
- Steed, L.; Heslop-Marshall, K.; Sohanpal, R.; Saqi-Waseem, S.; Kelly, M.; Pinnock, H.; Taylor, S. Developing a complex intervention whilst considering implementation: The TANDEM (Tailored intervention for ANxiety and DEpression Management) intervention for patients with chronic obstructive pulmonary disease (COPD). Trials 2021, 22, 252. [Google Scholar] [CrossRef] [PubMed]
- Surgey, A.; Disbeschl, S.; Lewis, R.; Hiscock, J.; Nafees, S.; Law, J.; Roberts, J.L.; Hendry, A.; Hoare, Z.; Goulden, N.; et al. ThinkCancer! The multi-method development of a complex behavior change intervention to improve the early diagnosis of cancer in primary care. medRxiv 2020. [Google Scholar] [CrossRef]
- Walsh, K.A.; Byrne, S.; Mc Sharry, J.; Browne, J.; Irving, K.; Hurley, E.; Rochford-Brennan, H.; Geoghegan, C.; Presseau, J.; Timmons, S. Developing a complex intervention targeting antipsychotic prescribing to nursing home residents with dementia. HRB Open Res. 2021, 4, 23. [Google Scholar] [CrossRef]
- Carswell, C. Development and Feasibility of an Arts-Based Intervention for Patients with End-Stage Kidney Disease Whilst Receiving Haemodialysis. Ph.D. Thesis, Queen’s University, Belfast, Northern Ireland, 17 September 2020. [Google Scholar]
- Slade, S.C.; Dionne, C.E.; Underwood, M.; Buchbinder, R.; Beck, B.; Bennell, K.; Brosseau, L.; Costa, L.; Cramp, F.; Cup, E.; et al. Consensus on Exercise Reporting Template (CERT): Modified Delphi Study. Phys Ther. 2016, 96, 1514–1524. [Google Scholar] [CrossRef] [PubMed]
- Braun, T.; Grüneberg, C.; Süßmilch, K.; Wiessmeier, M.; Schwenk, I.; Eggert, S.; Machleit-Ebner, A.; Harras, I.; Thiel, C. An augmented prescribed exercise program (APEP) to improve mobility of older acute medical patients-a randomized, controlled pilot and feasibility trial. BMC Geriatr. 2019, 19, 240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Slade, S.C.; Carey, D.L.; Hill, A.M.; Morris, M.E. Effects of falls prevention interventions on falls outcomes for hospitalised adults: Protocol for a systematic review with meta-analysis. BMJ Open 2017, 7, e017864. [Google Scholar] [CrossRef] [PubMed] [Green Version]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Blancafort Alias, S.; Cuevas-Lara, C.; Martínez-Velilla, N.; Zambom-Ferraresi, F.; Soto, M.E.; Tavassoli, N.; Mathieu, C.; Heras Muxella, E.; Garibaldi, P.; Anglada, M.; et al. A Multi-Domain Group-Based Intervention to Promote Physical Activity, Healthy Nutrition, and Psychological Wellbeing in Older People with Losses in Intrinsic Capacity: AMICOPE Development Study. Int. J. Environ. Res. Public Health 2021, 18, 5979. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115979
Blancafort Alias S, Cuevas-Lara C, Martínez-Velilla N, Zambom-Ferraresi F, Soto ME, Tavassoli N, Mathieu C, Heras Muxella E, Garibaldi P, Anglada M, et al. A Multi-Domain Group-Based Intervention to Promote Physical Activity, Healthy Nutrition, and Psychological Wellbeing in Older People with Losses in Intrinsic Capacity: AMICOPE Development Study. International Journal of Environmental Research and Public Health. 2021; 18(11):5979. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115979
Chicago/Turabian StyleBlancafort Alias, Sergi, César Cuevas-Lara, Nicolás Martínez-Velilla, Fabricio Zambom-Ferraresi, Maria Eugenia Soto, Neda Tavassoli, Céline Mathieu, Eva Heras Muxella, Pablo Garibaldi, Maria Anglada, and et al. 2021. "A Multi-Domain Group-Based Intervention to Promote Physical Activity, Healthy Nutrition, and Psychological Wellbeing in Older People with Losses in Intrinsic Capacity: AMICOPE Development Study" International Journal of Environmental Research and Public Health 18, no. 11: 5979. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115979