
Evaluation of Clinical, Biochemical and Microbiological Markers Related to Dental Caries

 , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participant Selection Process
2.2. Clinical Examination and Sample Collection
2.3. Determination of Salivary pH
2.4. Determination of Biofilm pH and Lactate Content
2.5. Count of S. mutans, S. dentisani, and Total Bacterial Count
2.6. Statistical Analysis
3. Results
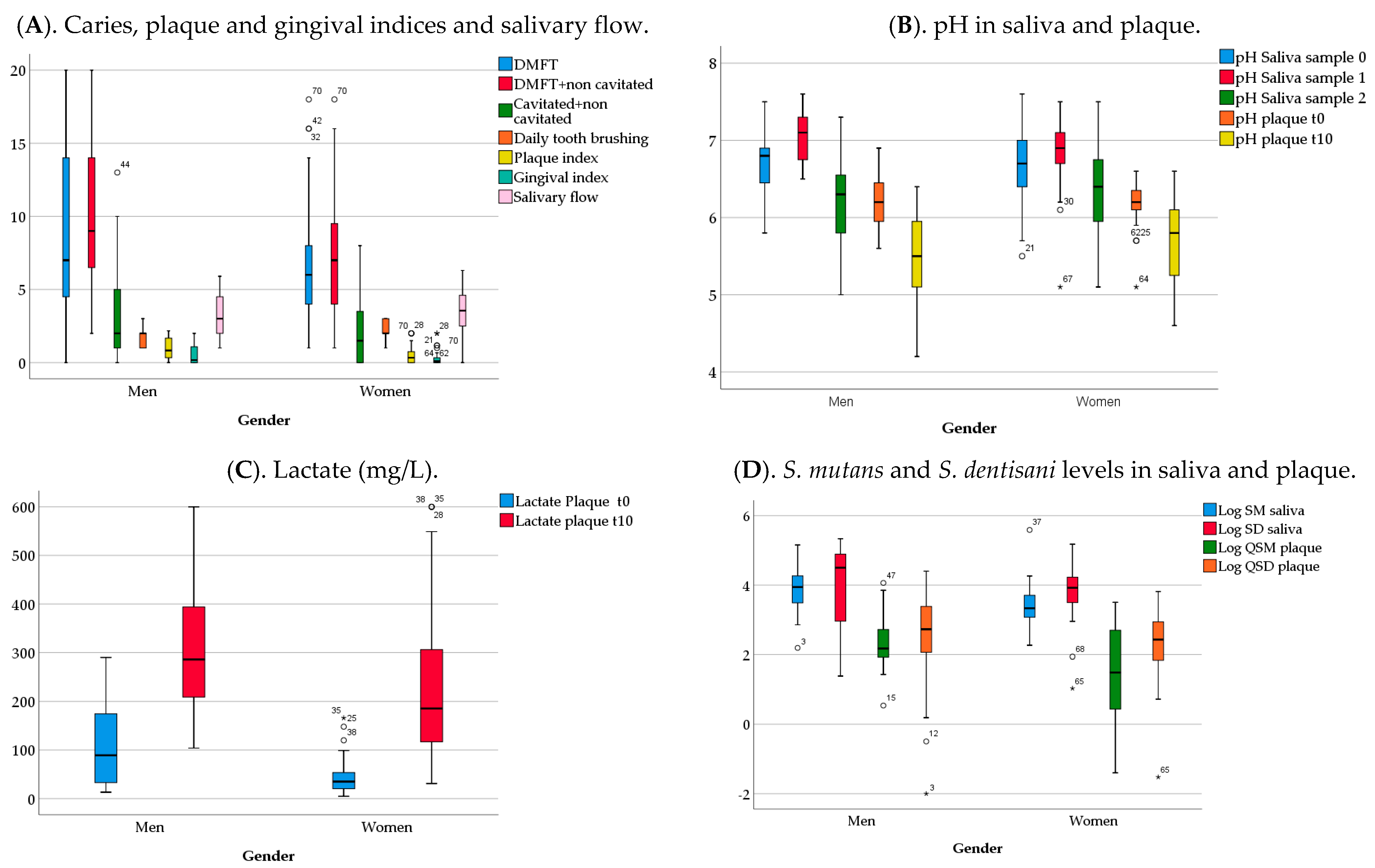
3.1. Analysis of Clinical, Biochemical and Microbiological Variables by Gender
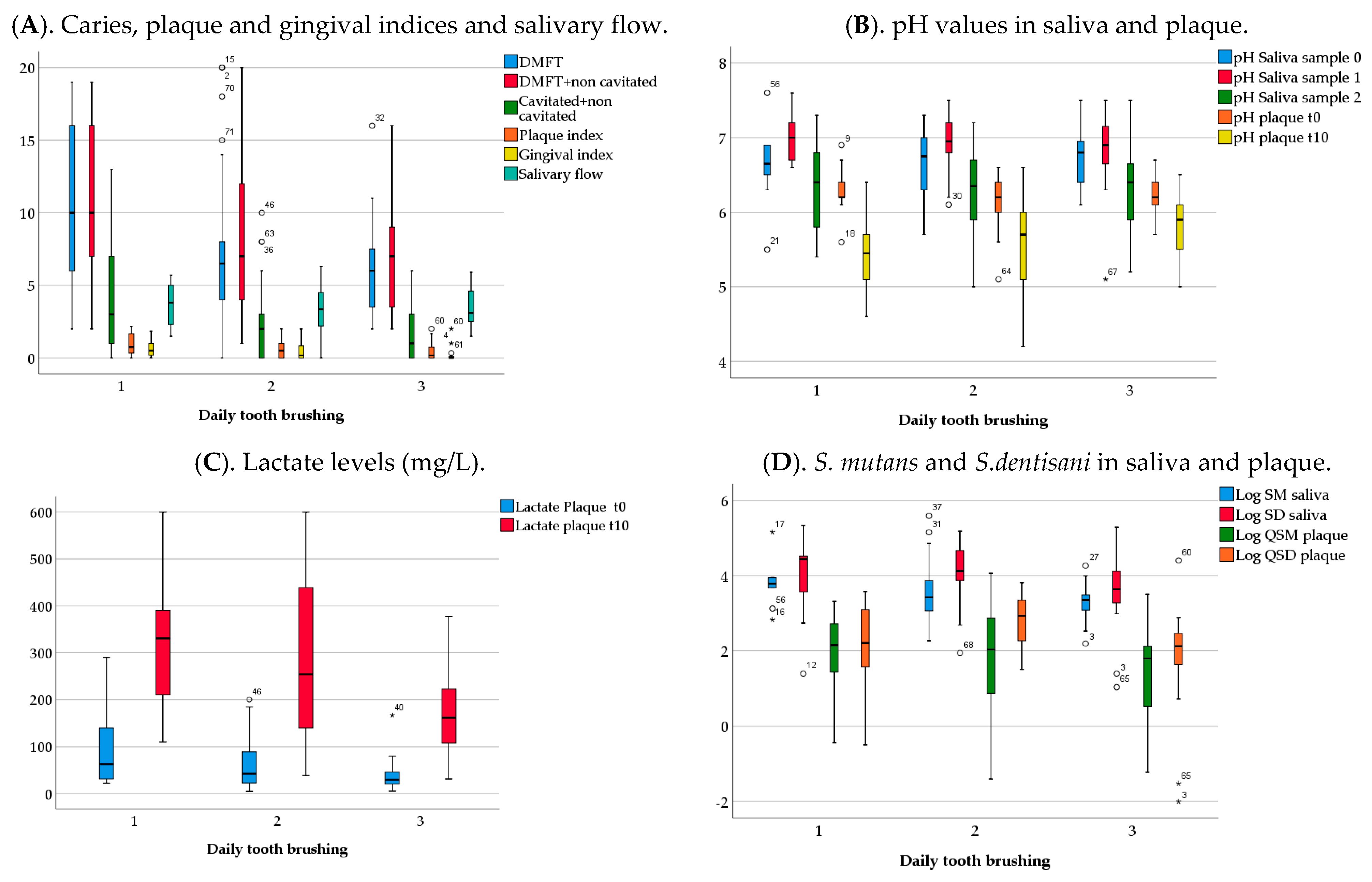
3.2. Analysis of Clinical, Biochemical and Microbiological Variables by Tooth-Brushing Frequency
3.3. Analysis of Clinical and Biochemical Variables
3.4. Microbiological Parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Machiulskiene, V.; Campus, G.; Carvalho, J.C.; Dige, I.; Ekstrand, K.R.; Jablonski-Momeni, A.; Maltz, M.; Manton, D.J.; Martignon, S.; Martinez-Mier, E.A.; et al. Terminology of Dental Caries and Dental Caries Management: Consensus Report of a Workshop Organized by ORCA and Cariology Research Group of IADR. Caries Res. 2020, 54, 7–14. [Google Scholar] [CrossRef]
- Morou-Bermudez, E.; Elias-Boneta, A.; Billings, R.J.; Burne, R.A.; Garcia-Rivas, V.; Brignoni-Nazario, V.; Suarez Perez, E. Urease activity in dental plaque and saliva of children during a three-year study period and its relationship with other caries risk factors. Arch. Oral Biol. 2011, 56, 1282–1289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simon-Soro, A.; Mira, A. Solving the etiology of dental caries. Trends Microbiol. 2015, 23, 76–82. [Google Scholar] [CrossRef]
- Simon-Soro, A.; Guillen-Navarro, M.; Mira, A. Metatranscriptomics reveals overall active bacterial composition in caries lesions. J. Oral Microbiol. 2014, 6, 25443. [Google Scholar] [CrossRef] [Green Version]
- Marsh, P.D. Are dental diseases examples of ecological catastrophes? Microbiology 2003, 149, 279–294. [Google Scholar] [CrossRef] [PubMed]
- Paes Leme, A.F.; Koo, H.; Bellato, C.M.; Bedi, G.; Cury, J.A. The role of sucrose in cariogenic dental biofilm formation—New insight. J. Dent. Res. 2006, 85, 878–887. [Google Scholar] [CrossRef] [PubMed]
- Sheng, J.; Baldeck, J.D.; Nguyen, P.T.; Quivey, R.G., Jr.; Marquis, R.E. Alkali production associated with malolactic fermentation by oral streptococci and protection against acid, oxidative, or starvation damage. Can. J. Microbiol. 2010, 56, 539–547. [Google Scholar] [CrossRef] [PubMed]
- Huang, X.; Exterkate, R.A.; ten Cate, J.M. Factors associated with alkali production from arginine in dental biofilms. J. Dent. Res. 2012, 91, 1130–1134. [Google Scholar] [CrossRef] [Green Version]
- Simón-Soro, A.; Tomás, I.; Cabrera-Rubio, R.; Catalan, M.D.; Nyvad, B.; Mira, A. Microbial geography of the oral cavity. J. Dent. Res. 2013, 92, 616–621. [Google Scholar] [CrossRef] [PubMed]
- Alcaraz, L.D.; Belda-Ferre, P.; Cabrera-Rubio, R.; Romero, H.; Simón-Soro, A.; Pignatelli, M.; Mira, A. Identifying a healthy oral microbiome through metagenomics. Clin. Microbiol. Infect. 2012, 18 (Suppl. S4), 54–57. [Google Scholar] [CrossRef] [Green Version]
- Benítez-Páez, A.; Belda-Ferre, P.; Simón-Soro, A.; Mira, A. Microbiota diversity and gene expression dynamics in human oral biofilms. BMC Genom. 2014, 15, 311. [Google Scholar] [CrossRef] [PubMed]
- Belda-Ferre, P.; Alcaraz, L.D.; Cabrera-Rubio, R.; Romero, H.; Simon-Soro, A.; Pignatelli, M.; Mira, A. The oral metagenome in health and disease. ISME J. 2012, 6, 46–56. [Google Scholar] [CrossRef] [Green Version]
- Camelo-Castillo, A.; Benitez-Paez, A.; Belda-Ferre, P.; Cabrera-Rubio, R.; Mira, A. Streptococcus dentisani sp. a novel member of the mitis group. Int. J. Syst. Evol. Microbiol. 2014, 64, 60–65. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Lopez, A.; Camelo-Castillo, A.; Ferrer, M.D.; Simon-Soro, A.; Mira, A. Health-Associated Niche Inhabitants as Oral Probiotics: The Case of Streptococcus dentisani. Front. Microbiol. 2017, 8, 379. [Google Scholar] [CrossRef] [PubMed]
- Rosier, B.T.; Buetas, E.; Moya-Gonzalvez, E.M.; Artacho, A.; Mira, A. Nitrate as a potential prebiotic for the oral microbiome. Sci. Rep. 2020, 10, 12895. [Google Scholar] [CrossRef]
- Nascimento, M.M.; Gordan, V.V.; Garvan, C.W.; Browngardt, C.M.; Burne, R.A. Correlations of oral bacterial arginine and urea catabolism with caries experience. Oral Microbiol. Immunol. 2009, 24, 89–95. [Google Scholar] [CrossRef] [Green Version]
- Gordan, V.V.; Garvan, C.W.; Ottenga, M.E.; Schulte, R.; Harris, P.A.; McEdward, D.; Magnusson, L. Could alkali production be considered an approach for caries control? Caries Res. 2010, 44, 547–554. [Google Scholar] [CrossRef]
- Nascimento, M.M.; Liu, Y.; Kalra, R.; Perry, S.; Adewumi, A.; Xu, X.; Primosch, R.E.; Burne, R.A. Oral arginine metabolism may decrease the risk for dental caries in children. J. Dent Res. 2013, 92, 60460–60468. [Google Scholar] [CrossRef]
- Hassan, H.; Lingstrom, P.; Carlen, A. Plaque pH in caries-free and caries-active young individuals before and after frequent rinses with sucrose and urea solution. Caries Res. 2015, 49, 18–25. [Google Scholar] [CrossRef]
- Dawes, C. What is the critical pH and why does a tooth dissolve in acid? J. Can. Dent. Assoc. 2003, 69, 722–724. [Google Scholar] [PubMed]
- Kleinberg, I. A mixed-bacteria ecological approach to understanding the role of the oral bacteria in dental caries causation: An alternative to Streptococcus mutans and the specific-plaque hypothesis. Crit. Rev. Oral Biol. Med. 2002, 13, 108–125. [Google Scholar] [CrossRef]
- Aminabadi, N.A.; Najafpour, E.; Razavi Rohani, Z.; Sighari Deljavan, A.; Ghojazadeh, M.; Jamali, Z. Linear reciprocal interaction between dental caries and salivary characteristics. J. Oral Sci. 2013, 55, 337–342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lenander-Lumikari, M.; Loimaranta, V. Saliva and dental caries. Adv. Dent Res. 2000, 14, 40–47. [Google Scholar] [CrossRef]
- Löe, H. The gingival index, the plaque index and the retention index systems. J. Periodontol. 1967, 38, 610–616. [Google Scholar] [CrossRef]
- Ekstrand, K.R.; Gimenez, T.; Ferreira, F.R.; Mendes, F.M.; Braga, M.M. The International Caries Detection and Assessment System—ICDAS: A Systematic Review. Caries Res. 2018, 52, 406–419. [Google Scholar] [CrossRef]
- Dzidic, M.; Collado, M.C.; Abrahamsson, T.; Artacho, A.; Stensson, M.; Jenmalm, M.C.; Mira, A. Oral microbiome development during childhood: An ecological succession influenced by postnatal factors and associated with tooth decay. ISME J. 2018, 12, 2292–2306. [Google Scholar] [CrossRef] [PubMed]
- Yano, A.; Kaneko, N.; Ida, H.; Yamaguchi, T.; Hanada, N. Real-time PCR for quantification of Streptococcus mutans. FEMS Microbiol. Lett. 2002, 217, 23–30. [Google Scholar] [CrossRef] [PubMed]
- Caporaso, J.G.; Lauber, C.L.; Walters, W.A.; Berg-Lyons, D.; Lozupone, C.A.; Turnbaugh, P.J.; Fierer, N.; Knight, R. Global patterns of 16S rRNA diversity at a depth of millions of sequences per sample. Proc. Natl. Acad. Sci. USA 2011, 108, 4516–4522. [Google Scholar] [CrossRef] [Green Version]
- Cruaud, P.; Vigneron, A.; Lucchetti-Miganeh, C.; Ciron, P.E.; Godfroy, A.; Cambon-Bonavita, M.A. Influence of DNA extraction method, 16S rRNA targeted hypervariable regions, and sample origin on microbial diversity detected by 454 pyrosequencing in marine chemosynthetic ecosystems. Appl. Environ. Microbiol. 2014, 80, 4626–4639. [Google Scholar] [CrossRef] [Green Version]
- Braga, M.M.; Oliveira, L.B.; Bonini, G.A.; Bönecker, M.; Mendes, F.M. Feasibility of the International Caries Detection and Assessment System (ICDAS-II) in epidemiological surveys and comparability with standard World Health Organization criteria. Caries Res. 2009, 43, 245–249. [Google Scholar] [CrossRef]
- Bravo Perez, M.; Almerich Silla, J.M.; Canorea Díaz, E.; Casals, P.; Cortes Martinicorena, F.J.; Expósito Delgado, A.; Gómez Santos, G.; Hidalgo Olivares, G.; Lamas Oliveira, M.; Martínez Beneyto, Y.; et al. Oral Health Survey in Spain 2020. RCOE 2020, 25, 12–69. [Google Scholar]
- Eustaquio, M.V.; Montiel, J.M.; Almerich, J.M. Oral health survey of the adult population of the Valencia region (Spain). Med. Oral Patol. Oral Cir. Bucal. 2010, 15, e538–e544. [Google Scholar] [CrossRef] [Green Version]
- Zeng, L.; Peng, Y.; Xu, T.; Wen, J.; Wan, L.; Ou, X.; Zhou, X. Dental caries and associated factors among adolescents aged 12 to 15 in Jiangxi Province, China. Public Health Dent. 2020, 80, 217–226. [Google Scholar] [CrossRef] [PubMed]
- Carta, G.; Cagetti, M.G.; Cocco, F.; Sale, S.; Lingstrom, P.; Campus, G. Caries-risk profiles in Italian adults using computer caries assessment system and ICDAS. Braz. Oral Res. 2015, 29, 1–8. [Google Scholar] [CrossRef]
- Broadbent, J.M.; Zeng, J.; Foster Page, L.A.; Baker, S.R.; Ramrakha, S.; Thomson, W.M. Oral Health-Related Beliefs, Behaviors, and Outcomes through the Life Course. J. Dent Res. 2016, 95, 808–813. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arrica, M.; Carta, G.; Cocco, F.; Cagetti, M.G.; Campus, G.; Ierardo, G.; Ottolenghi, L.; Salee, S.; Strohmenger, L. Does a social/behavioural gradient in dental health exist among adults? A cross-sectional study. J. Int. Med. Res. 2017, 45, 451–461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vano, M.; Gennai, S.; Karapetsa, D.; Miceli, M.; Giuca, M.R.; Gabriele, M.; Graziani, F. The influence of educational level and oral hygiene behaviours on DMFT index and CPITN index in an adult Italian population: An epidemiological study. Int. J. Dent. Hyg. 2015, 13, 151–157. [Google Scholar] [CrossRef]
- Marsh, P.D.; Head, D.A. Ecological approaches to oral biofilms: Control without killing. Caries Res. 2015, 49, 46–54. [Google Scholar] [CrossRef] [Green Version]
- Tanner, A.C.; Kressirer, C.A.; Faller, L.L. Understanding Caries from the Oral Microbiome Perspective. J. Calif Dent. Assoc. 2016, 44, 437–446. [Google Scholar]
- Zaura, E.; Brandt, B.W.; Prodan, A.; Teixeira de Mattos, M.J.; Imangaliyev, S.; Kool, J.; Buijs, M.J.; Jagers, F.L.; Hennequin-Hoenderdos, N.L.; Slot, D.E.; et al. On the ecosystemic network of saliva in healthy young adults. ISME J. 2017, 11, 1218–1231. [Google Scholar] [CrossRef] [PubMed]
- Struzycka, I. The oral microbiome in dental caries. Pol. J. Microbiol. 2014, 63, 127–135. [Google Scholar] [CrossRef]
- Firestone, A.R.; Graves, C.; Caufield, P.W.; Feagin, F.F. Root surface caries subsequent to gingivectomy in rats inoculated with Streptococcus sobrinus, mutans and Actinomyces viscosus. J. Dent. Res. 1987, 66, 1583–1586. [Google Scholar] [CrossRef]
- Elgamily, H.M.; Gamal, A.A.; Saleh, S.A.A.; Abdel Wahab, W.A.; Hashem, A.M.; Esawy, M.A. Microbiological and environmental assessment of human oral dental plaque isolates. Microb. Pathog. 2019, 135, 103626. [Google Scholar] [CrossRef] [PubMed]
- Tanner, A.C.R.; Kressirer, C.A.; Rothmiller, S.; Johansson, I.; Chalmers, N.I. The Caries Microbiome: Implications for Reversing Dysbiosis. Adv. Dent. Res. 2018, 29, 78–85. [Google Scholar] [CrossRef] [Green Version]
- Moncada, G.; Maureira, J.; Neira, M.; Reyes, E.; Oliveira Junior, O.B.; Faleiros, S.; Palma, P.; Corsini, G.; Ugalde, C.; Gordan, V.V.; et al. Salivary Urease and ADS Enzymatic Activity as Endogenous Protection against Dental Caries in Children. J. Clin. Pediatr. Dent. 2015, 39, 358–363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferrer, M.D.; López-López, A.; Nicolescu, T.; Salavert, A.; Méndez, I.; Cuñé, J.; Llena, C.; Mira, A. A pilot study to assess oral colonization and pH buffering by the probiotic Streptococcus dentisani under different dosing regimens. Odontology 2020, 108, 180–187. [Google Scholar] [CrossRef]
- Ferrer, M.D.; López-López, A.; Nicolescu, T.; Perez-Vilaplana, S.; Boix-Amorós, A.; Dzidic, M.; Garcia, S.; Artacho, A.; Llena, C.; Mira, A. Topic Application of the Probiotic Streptococcus dentisani Improves Clinical and Microbiological Parameters Associated with Oral Health. Front. Cell Infect. Microbiol. 2020, 10, 465. [Google Scholar] [CrossRef]
- Tribble, G.D.; Angelov, N.; Weltman, R.; Wang, B.Y.; Eswaran, S.V.; Gay, I.C.; Parthasarathy, K.; Dao, D.V.; Richardson, K.N.; Ismail, N.M.; et al. Frequency of Tongue Cleaning Impacts the Human Tongue Microbiome Composition and Enterosalivary Circulation of Nitrate. Front. Cell Infect. Microbiol. 2019, 9, 39. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Age | D_Cavitated 1 | D_non Cavitated 2 | M 3 | F 4 | DMFT 5 | DMFT + Non Cavitated 6 | PI 7 | GI 8 | Salivary Flow | pH_Saliva (Sample 0) 9 | pH_Saliva (Sample 1) 10 | pH_Saliva (Sample 2) 11 | pH_Plaque_t0 12 | pH_Plaque_t10 13 | Lactate_ Plaque_t0 14 | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| D_cavitated | CC | 0.11 | |||||||||||||||
| p | 0.34 | ||||||||||||||||
| D_non cavitated | CC | −0.17 | −0.20 | ||||||||||||||
| p | 0.13 | 0.07 | |||||||||||||||
| M | CC | 0.60 | 0.08 | −0.02 | |||||||||||||
| p | 0.00 | 0.48 | 0.80 | ||||||||||||||
| F | CC | 0.17 | −0.32 | −0.14 | 0.20 | ||||||||||||
| p | 0.14 | 0.00 | 0.23 | 0.08 | |||||||||||||
| DMFT | CC | 0.33 | 0.262 | −0.23 | 0.50 | 0.69 | |||||||||||
| p | 0.00 | 0.02 | 0.04 | 0.00 | 0.00 | ||||||||||||
| DMFT + non cavitated | CC | 0.27 | 0.19 | 0.15 | 0.54 | 0.61 | 0.887 | ||||||||||
| p | 0.01 | 0.10 | 0.19 | 0.00 | 0.00 | 0.00 | |||||||||||
| D cavitated + non cavitated | CC | −0.03 | 0.72 | 0.42 | 0.06 | −0.32 | 0.15 | 0.36 | |||||||||
| p | 0.79 | 0.00 | 0.00 | 0.59 | 0.00 | 0.17 | 0.00 | ||||||||||
| PI | CC | 0.21 | 0.39 | −0.13 | 0.26 | −0.09 | 0.23 | 0.20 | |||||||||
| p | 0.06 | 0.00 | 0.26 | 0.02 | 0.39 | 0.03 | 0.07 | ||||||||||
| GI | CC | 0.18 | 0.16 | −0.13 | 0.24 | −0.07 | 0.17 | 0.14 | 0.53 | ||||||||
| P | 0.11 | 0.16 | 0.24 | 0.03 | 0.51 | 0.14 | 0.23 | 0.00 | |||||||||
| Salivary flow | CC | −0.03 | 0.08 | 0.08 | 0.09 | 0.06 | 0.16 | 0.15 | −0.15 | 0.07 | |||||||
| p | 0.77 | 0.46 | 0.46 | 0.42 | 0.58 | 0.14 | 0.18 | 0.19 | 0.51 | ||||||||
| pH_saliva (sample 0) | CC | −0.15 | −0.12 | 0.07 | 0.01 | −0.06 | −0.09 | −0.10 | −0.10 | 0.05 | 0.07 | ||||||
| p | 0.19 | 0.27 | 0.53 | 0.93 | 0.58 | 0.41 | 0.39 | 0.36 | 0.66 | 0.52 | |||||||
| pH_saliva (sample 1) | CC | −0.08 | −0.05 | 0.15 | 0.05 | −0.20 | −0.12 | −0.07 | 0.00 | 0.02 | 0.03 | 0.56 | |||||
| p | 0.47 | 0.63 | 0.17 | 0.65 | 0.08 | 0.28 | 0.53 | 0.98 | 0.84 | 0.75 | 0.00 | ||||||
| pH_saliva (sample 2) | CC | −0.25 | 0.05 | 0.15 | −0.15 | −0.21 | −0.21 | −0.17 | −0.09 | 0.00 | 0.18 | 0.32 | 0.39 | ||||
| p | 0.02 | 0.66 | 0.19 | 0.17 | 0.06 | 0.06 | 0.13 | 0.41 | 0.94 | 0.10 | 0.00 | 0.00 | |||||
| pH_plaque_t0 | CC | −0.03 | −0.03 | 0.04 | 0.06 | 0.15 | 0.08 | 0.11 | −0.24 | −0.07 | 0.03 | −0.02 | 0.00 | −0.04 | |||
| p | 0.79 | 0.79 | 0.68 | 0.56 | 0.18 | 0.48 | 0.32 | 0.03 | 0.54 | 0.78 | 0.81 | 0.99 | 0.72 | ||||
| pH_plaque_t10 | CC | −0.18 | −0.14 | 0.05 | −0.22 | 0.04 | −0.10 | −0.10 | −0.39 | −0.27 | 0.12 | −0.08 | −0.26 | −0.03 | 0.53 | ||
| p | 0.11 | 0.21 | 0.61 | 0.05 | 0.67 | 0.38 | 0.37 | 0.00 | 0.01 | 0.28 | 0.44 | 0.02 | 0.79 | 0.00 | |||
| Lactate_plaque_t0 | CC | 0.31 | 0.17 | −0.16 | 0.27 | 0.03 | 0.16 | 0.16 | 0.44 | 0.35 | −0.17 | −0.05 | 0.01 | −0.10 | −0.018 | −0.59 | |
| p | 0.00 | 0.13 | 0.16 | 0.01 | 0.75 | 0.16 | 0.16 | 0.00 | 0.00 | 0.13 | 0.65 | 0.87 | 0.39 | 0.11 | 0.00 | ||
| Lactate_plaque_t10 15 | CC | 0.29 | 0.28 | −0.11 | 0.29 | −0.07 | 0.17 | 0.15 | 0.39 | 0.34 | −0.03 | 0.02 | 0.17 | 0.01 | −0.19 | −0.67 | 0.75 |
| p | 0.01 | 0.01 | 0.33 | 0.00 | 0.53 | 0.13 | 0.17 | 0.00 | 0.00 | 0.77 | 0.83 | 0.14 | 0.88 | 0.10 | 0.00 | 0.00 | |
| S. mutans Saliva | S. dentisani Saliva | S. dentisani norm. in Plaque | S. mutans norm. in Plaque | % S. dentisani in Plaque | % S. Mutans in Plaque | ||
|---|---|---|---|---|---|---|---|
| Age | CC | 0.154 | 0.311 | 0.220 | −0.105 | 0.254 | −0.084 |
| p | 0.200 | 0.008 | 0.065 | 0.385 | 0.033 | 0.486 | |
| PI 1 | CC | 0.27 | 0.412 | 0.226 | 0.098 | 0.246 | 0.040 |
| p | 0.020 | 0.000 | 0.058 | 0.415 | 0.039 | 0.742 | |
| GI 2 | CC | 0.168 | 0.108 | 0.088 | 0.046 | 0.098 | 0.000 |
| p | 0.162 | 0.370 | 0.467 | 0.706 | 0.415 | 0.998 | |
| Salivary flow | CC | −0.034 | −0.197 | −0.036 | 0.048 | −0.142 | −0.015 |
| p | 0.777 | 0.100 | 0.763 | 0.688 | 0.236 | 0.899 | |
| D_cavitated 3 | CC | 0.242 | 0.349 | 0.107 | −0.046 | 0.159 | −0.045 |
| p | 0.042 | 0.003 | 0.373 | 0.705 | 0.185 | 0.709 | |
| D_cavitaed + non cavitated 4 | CC | 0.210 | 0.260 | 0.186 | 0.068 | 0.245 | 0.027 |
| p | 0.079 | 0.119 | 0.574 | 0.039 | 0.823 | ||
| M 5 | CC | 0.149 | 0.150 | 0.068 | 0.085 | 0.018 | 0.114 |
| p | 0.214 | 0.211 | 0.574 | 0.479 | 0.882 | 0.346 | |
| F 6 | CC | −0.123 | −0.234 | −0.120 | 0.003 | −0.128 | 0.040 |
| p | 0.308 | 0.049 | 0.320 | 0.981 | 0.287 | 0.738 | |
| DMFT 7 | CC | 0.084 | 0.044 | −0.049 | 0.007 | −0.074 | 0.058 |
| p | 0.488 | 0.718 | 0.688 | 0.951 | 0.539 | 0.633 | |
| DMFT_with non cavitated 8 | CC | 0.110 | 0.037 | −0.001 | 0.053 | −0.012 | 0.084 |
| p | 0.363 | 0.760 | 0.993 | 0.659 | 0.919 | 0.484 | |
| S. mutans in saliva | CC | 0.594 | 0.116 | 0.488 | 0.013 | 0.460 | |
| p | 0.000 | 0.335 | 0.000 | 0.913 | 0.000 | ||
| S. dentisani in saliva | CC | 0.594 | 0.399 | 0.181 | 0.429 | 0.179 | |
| p | 0.000 | 0.001 | 0.131 | 0.000 | 0.136 | ||
| S. dentisaninorm. in plaque | CC | 0.116 | 0.399 | 0.300 | 0.893 | 0.160 | |
| p | 0.335 | 0.001 | 0.011 | 0.000 | 0.182 | ||
| S. mutansnorm. in plaque | CC | 0.488 | 0.181 | 0.300 | 0.151 | 0.922 | |
| p | 0.000 | 0.131 | 0.011 | 0.208 | 0.000 | ||
| % S. dentisani in plaque | CC | 0.013 | 0.429 | 0.893 | 0.151 | 0.079 | |
| p | 0.913 | 0.000 | 0.000 | 0.208 | 0.512 | ||
| % S. mutans in plaque | CC | 0.460 | 0.179 | 0.160 | 0.922 | 0.079 | |
| p | 0.000 | 0.136 | 0.182 | 0.000 | 0.512 | ||
| pH_saliva (sample 0) 9 | CC | −0.177 | −0.238 | −0.103 | −0.111 | −0.124 | −0.154 |
| p | 0.139 | 0.046 | 0.392 | 0.359 | 0.302 | 0.201 | |
| pH_saliva (sample 1) 10 | CC | 0.146 | −0.131 | −0.044 | 0.132 | −0.113 | 0.125 |
| p | 0.223 | 0.278 | 0.715 | 0.273 | 0.348 | 0.298 | |
| pH_saliva (sample 2) 11 | CC | −0.167 | −0.216 | −0.020 | −0.111 | −0.018 | −0.172 |
| p | 0.165 | 0.071 | 0.867 | 0.357 | 0.879 | 0.152 | |
| pH_plaque_t0 12 | CC | −0.207 | −0.351 | −0.411 | −0.289 | −0.296 | −0.230 |
| p | 0.084 | 0.003 | 0.000 | 0.015 | 0.012 | 0.053 | |
| pH_plaque_t10 13 | CC | −0.368 | −0.286 | −0.286 | −0.427 | −0.177 | −0.394 |
| p | 0.002 | 0.016 | 0.016 | 0.000 | 0.141 | 0.001 | |
| Lactate_plaque t0 14 | CC | 0.333 | 0.324 | 0.045 | 0.249 | 0.112 | 0.332 |
| p | 0.005 | 0.006 | 0.710 | 0.036 | 0.353 | 0.005 | |
| Lactate_plaque t10 15 | CC | 0.362 | 0.402 | 0.137 | 0.246 | 0.148 | 0.293 |
| p | 0.002 | 0.001 | 0.254 | 0.039 | 0.218 | 0.012 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ferrer, M.D.; Pérez, S.; Lopez, A.L.; Sanz, J.L.; Melo, M.; Llena, C.; Mira, A. Evaluation of Clinical, Biochemical and Microbiological Markers Related to Dental Caries. Int. J. Environ. Res. Public Health 2021, 18, 6049. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18116049
Ferrer MD, Pérez S, Lopez AL, Sanz JL, Melo M, Llena C, Mira A. Evaluation of Clinical, Biochemical and Microbiological Markers Related to Dental Caries. International Journal of Environmental Research and Public Health. 2021; 18(11):6049. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18116049
Chicago/Turabian StyleFerrer, Maria D, Salvadora Pérez, Aránzazu López Lopez, José Luis Sanz, Maria Melo, Carmen Llena, and Alejandro Mira. 2021. "Evaluation of Clinical, Biochemical and Microbiological Markers Related to Dental Caries" International Journal of Environmental Research and Public Health 18, no. 11: 6049. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18116049