
Will E-Cigarette Modified Risk Messages with a Nicotine Warning Polarize Smokers’ Beliefs about the Efficacy of Switching Completely to E-Cigarettes in Reducing Smoking-Related Risks?


Abstract
:1. Introduction
1.1. Background
1.2. Biased Assimilation and Opinion Polarization
1.3. Need for Closure
2. Materials and Methods
2.1. Design, Participants, and Procedure
2.2. Message Stimuli
2.3. Key Measures
2.4. Analysis Plan
3. Results
3.1. Sample Characteristics
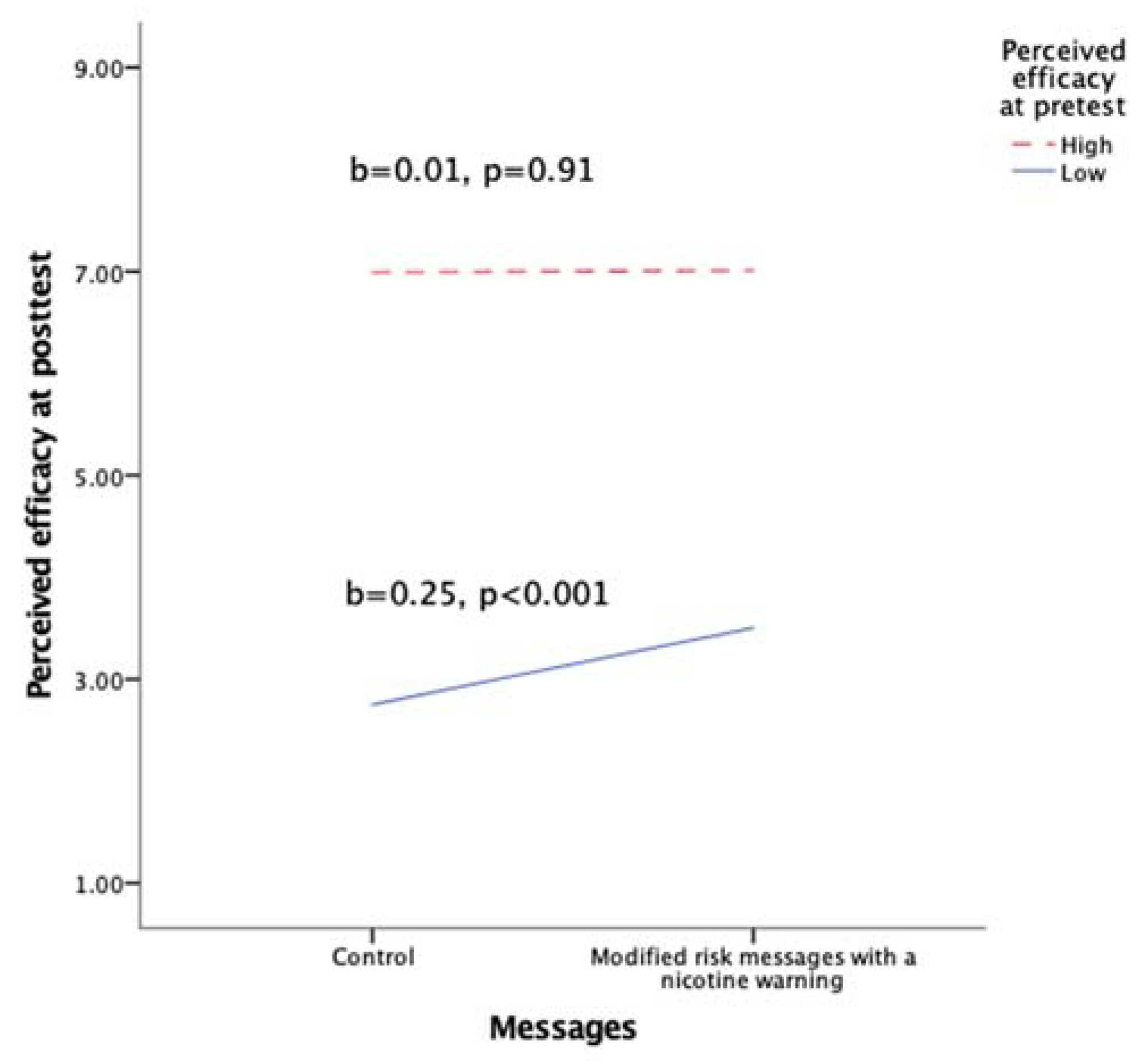
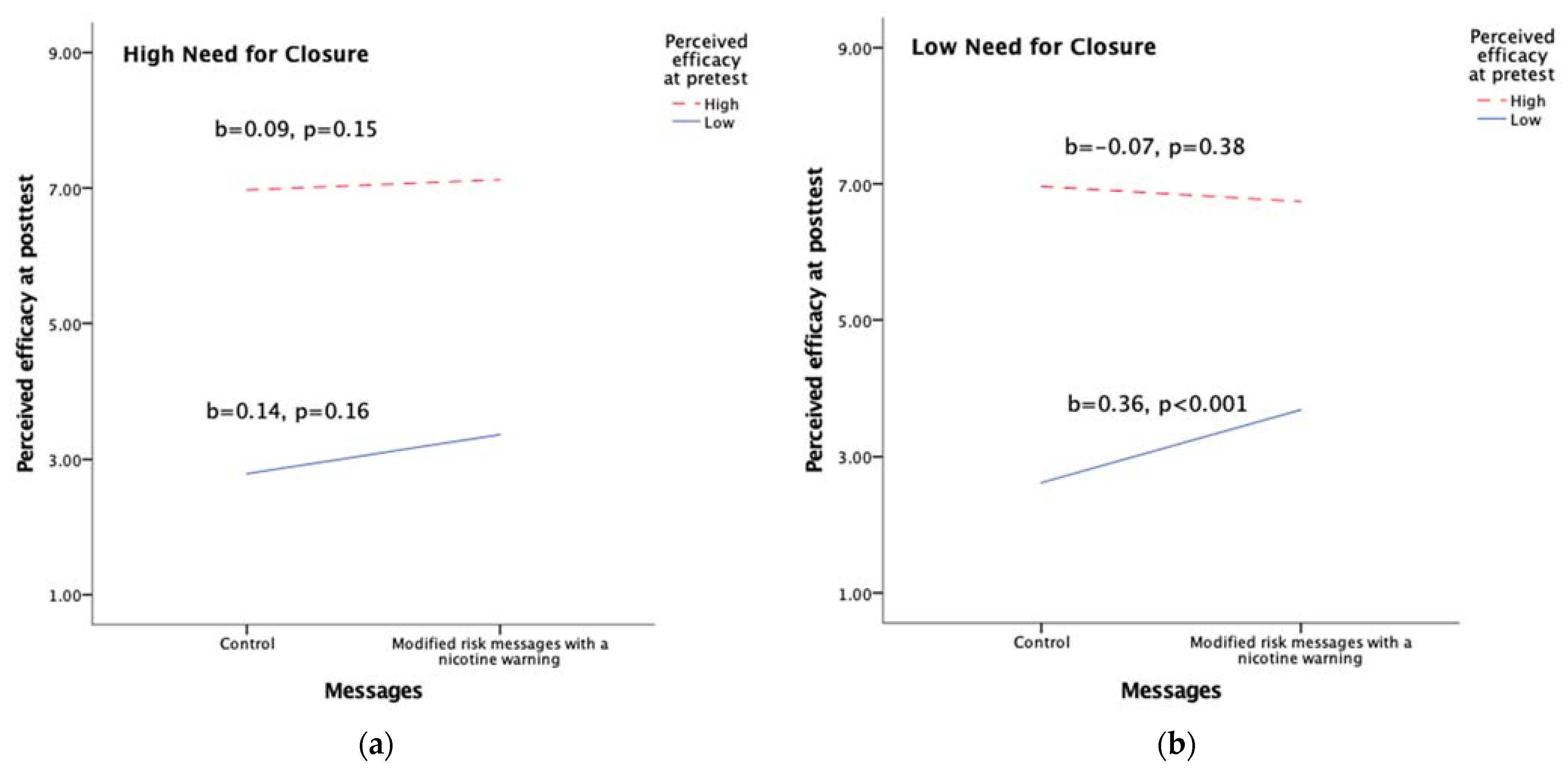
3.2. Hypothesis Testing
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- National Academies of Sciences, Engineering, and Medicine. Public Health Consequences of E-Cigarettes; The National Academies Press: Washington, DC, USA, 2018. [Google Scholar]
- McNeill, A.; Brose, L.S.; Calder, R.; Bauld, L.; Robson, D. Evidence Review of e-Cigarettes and Heated Tobacco Products 2018. A Report Commissioned by Public Health England; Public Health England: London, UK, 2018. [Google Scholar]
- Goniewicz, M.L.; Gawron, M.; Smith, D.M.; Peng, M.; Jacob, P.; Benowitz, N.L. Exposure to nicotine and selected toxicants in cigarette smokers who switched to electronic cigarettes: A longitudinal within-subjects observational study. Nicotine Tob. Res. 2017, 19, 160–167. [Google Scholar] [CrossRef] [Green Version]
- Jay, J.; Pfaunmiller, E.L.; Huang, N.J.; Cohen, G.; Graff, D.W. Five-day changes in biomarkers of exposure among adult smokers after completely switching from combustible cigarettes to a nicotine-salt pod system. Nicotine Tob. Res. 2020, 22, 1285–1293. [Google Scholar] [CrossRef] [Green Version]
- Pulvers, K.; Nollen, N.L.; Rice, M.; Schmid, C.H.; Qu, K.; Benowitz, N.L.; Ahluwalia, J.S. Effect of pod e-cigarettes vs cigarettes on carcinogen exposure among African American and latinx smokers: A randomized clinical trial. JAMA Netw. Open 2020, 3, e2026324. [Google Scholar] [CrossRef]
- Lindblom, E.N. Should FDA try to move smokers to e-cigarettes and other less-harmful tobacco products and, if so, how? Food Drug Law J. 2018, 73, 276–318. [Google Scholar]
- Abrams, D.B.; Glasser, A.M.; Pearson, J.L.; Villanti, A.C.; Collins, L.K.; Niaura, R.S. Harm minimization and tobacco control: Reframing societal views of nicotine use to rapidly save lives. Annu. Rev. Public Health 2018, 39, 193–213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gottlieb, S.; Zeller, M. A nicotine-focused framework for public health. N. Engl. J. Med. 2017, 377, 1111–1114. [Google Scholar] [CrossRef] [PubMed]
- Electronic Cigarettes: What’s the Bottom Line? Available online: https://www.cdc.gov/tobacco/basic_information/e-cigarettes/pdfs/Electronic-Cigarettes-Infographic-p.pdf (accessed on 3 June 2021).
- Draft Guidance for Industry: Modified Risk Tobacco Product Applications; U.S. Food and Drug Administration: Washington, DC, USA, 2012.
- Modified Risk Tobacco Products. Available online: https://www.fda.gov/tobacco-products/advertising-and-promotion/modified-risk-tobacco-products (accessed on 3 June 2021).
- Modified Risk Orders. Available online: https://www.fda.gov/tobacco-products/advertising-and-promotion/modified-risk-orders (accessed on 3 June 2021).
- “Covered” Tobacco Products and Roll-Your-Own/Cigarette Tobacco Labeling and Warning Statement Requirements. Available online: https://www.fda.gov/tobacco-products/labeling-and-warning-statements-tobacco-products/covered-tobacco-products-and-roll-your-own-cigarette-tobacco-labeling-and-warning-statement (accessed on 3 June 2021).
- Carpenter, D.M.; Geryk, L.L.; Chen, A.T.; Nagler, R.H.; Dieckmann, N.F.; Han, P.K. Conflicting health information: A critical research need. Health Expect. 2016, 19, 1173–1182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katz, S.J.; Lindgren, B.; Hatsukami, D. E-cigarettes warning labels and modified risk statements: Tests of messages to reduce recreational use. Tob. Regul. Sci. 2017, 3, 445–458. [Google Scholar] [CrossRef]
- Owusu, D.; Lawley, R.; Yang, B.; Henderson, K.; Bethea, B.; LaRose, C.; Stallworth, S.; Popova, L. ‘The lesser devil you don’t know’: A qualitative study of smokers’ responses to messages communicating comparative risk of electronic and combusted cigarettes. Tob. Control 2020, 29, 217–223. [Google Scholar] [CrossRef]
- Wackowski, O.A.; Rashid, M.; Greene, K.L.; Lewis, M.J.; O’Connor, R.J. Smokers’ and young adult non-smokers’ perceptions and perceived impact of snus and e-cigarette modified risk messages. Int. J. Environ. Res. Public Health 2020, 17, 6807. [Google Scholar] [CrossRef]
- Katz, S.J.; Erkkinen, M.; Lindgren, B.; Hatsukami, D. Assessing the impact of conflicting health warning information on intentions to use e-cigarettes—An application of the heuristic-systematic model. J. Health Commun. 2018, 23, 874–885. [Google Scholar] [CrossRef] [PubMed]
- Nagler, R.H.; LoRusso, S.M. Conflicting information and message competition in health and risk messaging. In The Oxford Encyclopedia of Health and Risk Message Design and Processing; Parrott, R.L., Ed.; Oxford University Press: New York, NY, USA, 2017. [Google Scholar]
- Nagler, R.H.; Yzer, M.C.; Rothman, A.J. Effects of Media Exposure to Conflicting Information about Mammography: Results from a population-based survey experiment. Ann. Behav. Med. 2019, 53, 896–908. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.-j.; Nagler, R.H.; Wang, N. Source-specific exposure to contradictory nutrition information: Documenting prevalence and effects on adverse cognitive and behavioral outcomes. Health Commun. 2018, 33, 453–461. [Google Scholar] [CrossRef] [PubMed]
- Chang, C. Motivated processing: How people perceive news covering novel or contradictory health research findings. Sci. Commun. 2015, 37, 602–634. [Google Scholar] [CrossRef]
- Tan, A.S.; Lee, C.-J.; Bigman, C.A. Public support for selected e-cigarette regulations and associations with overall information exposure and contradictory information exposure about e-cigarettes: Findings from a national survey of US adults. Prev. Med. 2015, 81, 268–274. [Google Scholar] [CrossRef]
- Tan, A.S.; Lee, C.-J.; Nagler, R.H.; Bigman, C.A. To vape or not to vape? Effects of exposure to conflicting news headlines on beliefs about harms and benefits of electronic cigarette use: Results from a randomized controlled experiment. Prev. Med. 2017, 105, 97–103. [Google Scholar] [CrossRef]
- Yang, Q.; Herbert, N.; Yang, S.; Alber, J.; Ophir, Y.; Cappella, J.N. The role of information avoidance in managing uncertainty from conflicting recommendations about electronic cigarettes. Commun. Monogr. 2020, 1–23. [Google Scholar] [CrossRef]
- Leeper, T.J.M.; Kevin, J. Motivated reasoning. In Oxford Biliographices, 22 February 2018 ed.; Oxford University Press: New York, NY, USA, 2018. [Google Scholar]
- Lord, C.G.; Taylor, C.A. Biased assimilation: Effects of assumptions and expectations on the interpretation of new evidence. Soc. Personal. Psychol. Compass 2009, 3, 827–841. [Google Scholar] [CrossRef]
- Kahan, D.M.; Braman, D.; Cohen, G.L.; Gastil, J.; Slovic, P. Who fears the hpv vaccine, who doesn’t, and why? An experimental study of the mechanisms of cultural cognition. Law Hum. Behav. 2010, 34, 501–516. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nan, X.; Daily, K. Biased assimilation and need for closure: Examining the effects of mixed blogs on vaccine-related beliefs. J. Health Commun. 2015, 20, 462–471. [Google Scholar] [CrossRef] [PubMed]
- Lord, C.G.; Ross, L.; Lepper, M.R. Biased assimilation and attitude polarization: The effects of prior theories on subsequently considered evidence. J. Personal. Soc. Psychol. 1979, 37, 2098–2109. [Google Scholar] [CrossRef]
- Kahan, D.M.; Braman, D. Cultural cognition and public policy. Yale Law Policy Rev. 2006, 24, 149–172. [Google Scholar]
- Greitemeyer, T.; Fischer, P.; Frey, D.; Schulz-Hardt, S. Biased assimilation: The role of source position. Eur. J. Soc. Psychol. 2009, 39, 22–39. [Google Scholar] [CrossRef]
- Mafael, A.; Gottschalk, S.A.; Kreis, H. Examining biased assimilation of brand-related online reviews. J. Interact. Mark. 2016, 36, 91–106. [Google Scholar] [CrossRef]
- Boysen, G.A.; Vogel, D.L. Biased assimilation and attitude polarization in response to learning about biological explanations of homosexuality. Sex Roles 2007, 57, 755–762. [Google Scholar] [CrossRef]
- Corner, A.; Whitmarsh, L.; Xenias, D. Uncertainty, scepticism and attitudes towards climate change: Biased assimilation and attitude polarisation. Clim. Chang. 2012, 114, 463–478. [Google Scholar] [CrossRef]
- Ofori-Parku, S.S. Fifty years after surgeon general’s report: Cultural cognition, biased assimilation, and cigarette smoking risk perceptions among college students. HealthRisk Soc. 2020, 22, 156–176. [Google Scholar] [CrossRef]
- Boysen, G.A.; Vogel, D.L. Education and mental health stigma: The effects of attribution, biased assimilation, and attitude polarization. J. Soc. Clin. Psychol. 2008, 27, 447–470. [Google Scholar] [CrossRef] [Green Version]
- Lopes, L.; Hamel, L.; Kearney, A.; Brodie, M. Data Note: Public Views on Vaping and e-Cigarettes; Henry Kaiser Family Foundation: San Franscisco, CA, USA, 2019. [Google Scholar]
- Kahan, D.M.; Slovic, P.; Braman, D.; Gastil, J.; Cohen, G.L.; Kysar, D.A. Biased assimilation, polarization, and cultural credibility: An experimental study of nanotechnology risk perceptions. Harv. Law Sch. Program Risk Regul. Res. Pap. 2008. [Google Scholar] [CrossRef] [Green Version]
- FDA Authorizes Marketing of iqos Tobacco Heating System with ‘Reduced Exposure’ Information. Available online: https://www.fda.gov/news-events/press-announcements/fda-authorizes-marketing-iqos-tobacco-heating-system-reduced-exposure-information (accessed on 9 May 2021).
- Kruglanski, A.W. Lay epistemic theory in social-cognitive psychology. Psychol. Inq. 1990, 1, 181–197. [Google Scholar] [CrossRef]
- Briñol, P.; Petty, R.E. Individual differences in attitude change. In The Handbook of Attitudes; Albarracín, B.T.J., Zanna, M.P., Eds.; Psychology Press: New York, NY, USA, 2014; pp. 575–615. [Google Scholar]
- Kruglanski, A.W.; Webster, D.M. Motivated closing of the mind: “Seizing” and “freezing”. Psychol. Rev. 1996, 103, 263–283. [Google Scholar] [CrossRef] [PubMed]
- O’Keefe, D.J. Persuasion: Theory and Research; Sage Publications: Thousand Oaks, CA, USA, 2016. [Google Scholar]
- Webster, D.M.; Kruglanski, A.W. Individual differences in need for cognitive closure. J. Personal. Soc. Psychol. 1994, 67, 1049–1062. [Google Scholar] [CrossRef]
- Webster, D.M.; Kruglanski, A.W. Cognitive and social consequences of the need for cognitive closure. Eur. Rev. Soc. Psychol. 1997, 8, 133–173. [Google Scholar] [CrossRef]
- Sweeny, K.; Melnyk, D.; Miller, W.; Shepperd, J.A. Information avoidance: Who, what, when, and why. Rev. Gen. Psychol. 2010, 14, 340–353. [Google Scholar] [CrossRef]
- Hart, W.; Adams, J.M.; Burton, K.A.; Shreves, W.; Hamilton, J.C. Shaping reality vs hiding from reality: Reconsidering the effects of trait need for closure on information search. J. Res. Personal. 2012, 46, 489–496. [Google Scholar] [CrossRef]
- Hiel, A.V.; Mervielde, I. Effects of ambiguity and need for closure on the acquisition of information. Soc. Cogn. 2002, 20, 380–408. [Google Scholar] [CrossRef]
- Yang, B.; Popova, L. Communicating risk differences between electronic and combusted cigarettes: The role of the FDA-mandated addiction warning and a nicotine fact sheet. Tob. Control 2020, 29, 663–671. [Google Scholar] [CrossRef]
- Yang, B.; Owusu, D.; Popova, L. Effects of a nicotine fact sheet on perceived risk of nicotine and e-cigarettes and intentions to seek information about and use e-cigarettes. Int. J. Environ. Res. Public Health 2020, 17, 131. [Google Scholar] [CrossRef] [Green Version]
- Popova, L.; Ling, P.M. Nonsmokers’ responses to new warning labels on smokeless tobacco and electronic cigarettes: An experimental study. BMC Public Health 2014, 14, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Padon, A.A.; Lochbuehler, K.; Maloney, E.K.; Cappella, J.N. A randomized trial of the effect of youth appealing e-cigarette advertising on susceptibility to use e-cigarettes among youth. Nicotine Tob. Res. 2018, 20, 954–961. [Google Scholar] [CrossRef]
- Sangalang, A.; Volinsky, A.C.; Liu, J.; Yang, Q.; Lee, S.J.; Gibson, L.A.; Hornik, R.C. Identifying potential campaign themes to prevent youth initiation of e-cigarettes. Am. J. Prev. Med. 2019, 56, S65–S75. [Google Scholar] [CrossRef] [Green Version]
- Clawson, A.H.; McQuaid, E.L.; Dunsiger, S.; Borrelli, B. Smokers with children with asthma: Parental perceptions about prototype intervention messages focused on reducing child tobacco exposure and use. J. Child Health Care 2018, 24, 106–122. [Google Scholar] [CrossRef] [PubMed]
- Global Community Panel Book. Available online: https://tolunacorporate.com/wp-content/uploads/2021/04/Global-Community-Panel-Book.pdf (accessed on 3 June 2021).
- Yang, B.; Owusu, D.; Popova, L. Testing messages about comparative risk of electronic cigarettes and combusted cigarettes. Tob. Control 2019, 28, 440–448. [Google Scholar] [CrossRef] [PubMed]
- Witte, K. Predicting risk behaviors: Development and validation of a diagnostic scale. J. Health Commun. 1996, 1, 317–342. [Google Scholar] [CrossRef]
- Roets, A.; Van Hiel, A. Item selection and validation of a brief, 15-item version of the need for closure scale. Personal. Individ. Differ. 2011, 50, 90–94. [Google Scholar] [CrossRef] [Green Version]
- Carpenter, M.J.; Hughes, J.R.; Solomon, L.J.; Callas, P.W. Both smoking reduction with nicotine replacement therapy and motivational advice increase future cessation among smokers unmotivated to quit. J. Consult. Clin. Psychol. 2004, 72, 371–381. [Google Scholar] [CrossRef]
- Heatherton, T.F.; Kozlowski, L.T.; Frecker, R.C.; Fagerstrom, K.O. The Fagerström test for nicotine dependence: A revision of the fagerstrom tolerance questionnaire. Br. J. Addict. 1991, 86, 1119–1127. [Google Scholar] [CrossRef] [PubMed]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach, 2nd ed.; Guilford Press: New York, NY, USA, 2018. [Google Scholar]
- Schumpe, B.M.; Brizi, A.; Giacomantonio, M.; Panno, A.; Kopetz, C.; Kosta, M.; Mannetti, L. Need for cognitive closure decreases risk taking and motivates discounting of delayed rewards. Personal. Individ. Differ. 2017, 107, 66–71. [Google Scholar] [CrossRef]
- Huang, J.; Feng, B.; Weaver, S.R.; Pechacek, T.F.; Slovic, P.; Eriksen, M.P. Changing perceptions of harm of e-cigarette vs cigarette use among adults in 2 US national surveys from 2012 to 2017. JAMA Netw. Open 2019, 2, e191047. [Google Scholar] [CrossRef] [Green Version]
- Strickland, A.A.; Taber, C.S.; Lodge, M. Motivated reasoning and public opinion. J. Health Politics Policy Law 2011, 36, 935–944. [Google Scholar] [CrossRef]
- Willson, V.L.; Kim, E.S. Pretest sensitization. In Encyclopedia of Research Design; Salkind, N.J., Ed.; Sage Publications: Thousand Oaks, CA, USA, 2012; pp. 1092–1094. [Google Scholar]
- Jackson, S.; Jacobs, S. Generalizing about messages: Suggestions for design and analysis of experiments. Hum. Commun. Res. 1983, 9, 169–191. [Google Scholar] [CrossRef]
- Rains, S.A.; Levine, T.R.; Weber, R. Sixty years of quantitative communication research summarized: Lessons from 149 meta-analyses. Ann. Int. Commun. Assoc. 2018, 42, 105–124. [Google Scholar] [CrossRef]
- Snyder, L.B. How effective are mediated health campaigns. Public Commun. Campaign. 2001, 3, 181–190. [Google Scholar] [CrossRef]
- Stiff, J.B.; Mongeau, P.A. Persuasive Communication, 3rd ed.; Guilford Press: New York, NY, USA, 2016. [Google Scholar]
- Cole-Lewis, H.; Pugatch, J.; Sanders, A.; Varghese, A.; Posada, S.; Yun, C.; Schwarz, M.; Augustson, E. Social listening: A content analysis of e-cigarette discussions on twitter. J. Med. Internet Res. 2015, 17, e243. [Google Scholar] [CrossRef] [Green Version]
- Kim, K.; Gibson, L.A.; Williams, S.; Kim, Y.; Binns, S.; Emery, S.L.; Hornik, R.C. Valence of media coverage about electronic cigarettes and other tobacco products from 2014 to 2017: Evidence from automated content analysis. Nicotine Tob. Res. 2020, 22, 1891–1900. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Overall (n = 761) | |
|---|---|
| Gender | |
| Male | 48.0 |
| Female | 51.5 |
| Transgender | 0.5 |
| Age | |
| 18–29 | 22.5 |
| 30–44 | 33.0 |
| 45–59 | 25.1 |
| 60+ | 19.4 |
| Race | |
| White | 73.9 |
| Black or African American | 15.2 |
| American Indian or Alaska Native | 1.4 |
| Asian | 3.8 |
| Other | 5.7 |
| Ethnicity | |
| Hispanic | 12.4 |
| Non-Hispanic | 87.6 |
| Education | |
| Less than high school | 8.1 |
| High school | 31.5 |
| Some college | 33.0 |
| Bachelor or higher degree | 27.3 |
| Daily Smoker | |
| Yes | 63.3 |
| No | 36.7 |
| E-Cigarette Use | |
| Current | 46.4 |
| Former | 24.4 |
| Never | 29.2 |
| Current Cigarette Smoking | |
| Yes | 95.9 |
| No, former smoker | 4.1 |
| Tried to Quit in the Past 12 Months | |
| Yes | 52.6 |
| No | 47.4 |
| Predictors | Unstandardized Coefficient | Standard Error | Part Correlation | p Value |
|---|---|---|---|---|
| Male (vs. other) | −0.07 | 0.12 | −0.01 | 0.56 |
| Age | −0.01 | 0.00 | −0.06 | 0.01 |
| Non-Hispanic White (vs. Non-Hispanic other) | −0.25 | 0.23 | −0.03 | 0.28 |
| Non-Hispanic Black (vs. Non-Hispanic other) | −0.10 | 0.27 | −0.01 | 0.70 |
| Hispanic (vs. Non-Hispanic other) | −0.29 | 0.27 | −0.03 | 0.29 |
| Below college education (vs. other) | −0.05 | 0.12 | −0.01 | 0.68 |
| Current e-cigarette users (vs. never) | 0.15 | 0.16 | 0.02 | 0.35 |
| Ever but not current e-cigarette users (vs. never) | 0.09 | 0.16 | 0.01 | 0.57 |
| Nicotine dependence | 0.10 | 0.04 | 0.05 | 0.02 |
| Past quit attempt (vs. no) | 0.19 | 0.13 | 0.03 | 0.14 |
| Ever switch to a lower tar or nicotine cigarette (vs. no) | 0.34 | 0.13 | 0.06 | 0.01 |
| Modified risk messages with a nicotine warning (MRMs vs. control) | 0.12 | 0.04 | 0.07 | 0.00 |
| Pretest perceived efficacy (Efficacy) | 0.78 | 0.05 | 0.38 | 0.00 |
| Need for closure (NC) | 0.07 | 0.12 | 0.01 | 0.57 |
| Efficacy × MRMs | −0.04 | 0.02 | −0.06 | 0.01 |
| Efficacy × NC | −0.06 | 0.05 | −0.03 | 0.19 |
| MRMs × NC | −0.01 | 0.04 | −0.00 | 0.86 |
| Efficacy × MRMs × NC | 0.04 | 0.02 | 0.06 | 0.01 |
| Total R2 | 0.60 | |||
| Adjusted R2 | 0.59 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, B.; Barbati, J.L.; Choi, Y. Will E-Cigarette Modified Risk Messages with a Nicotine Warning Polarize Smokers’ Beliefs about the Efficacy of Switching Completely to E-Cigarettes in Reducing Smoking-Related Risks? Int. J. Environ. Res. Public Health 2021, 18, 6094. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18116094
Yang B, Barbati JL, Choi Y. Will E-Cigarette Modified Risk Messages with a Nicotine Warning Polarize Smokers’ Beliefs about the Efficacy of Switching Completely to E-Cigarettes in Reducing Smoking-Related Risks? International Journal of Environmental Research and Public Health. 2021; 18(11):6094. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18116094
Chicago/Turabian StyleYang, Bo, Juliana L. Barbati, and Yunjin Choi. 2021. "Will E-Cigarette Modified Risk Messages with a Nicotine Warning Polarize Smokers’ Beliefs about the Efficacy of Switching Completely to E-Cigarettes in Reducing Smoking-Related Risks?" International Journal of Environmental Research and Public Health 18, no. 11: 6094. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18116094