
Systematic Review to Update ‘Value of a Statistical Life’ Estimates for Australia



Abstract
:1. Introduction
2. Methods
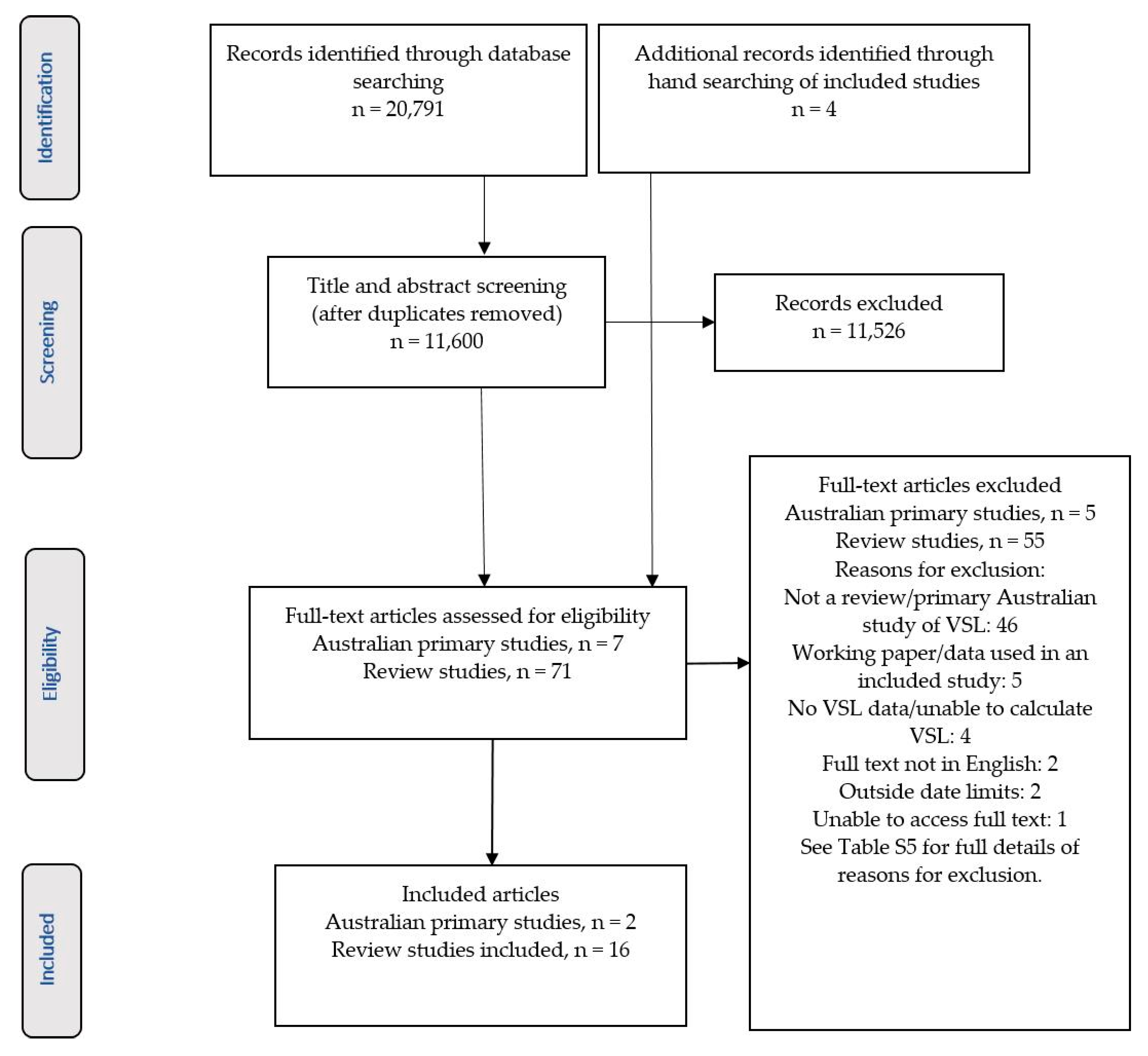
2.1. Search Strategy and Selection of Studies
2.2. Quality Assessment

{kind=link}
| Review Studies | ||||||
|---|---|---|---|---|---|---|
| Study | VSL Elicitation Methods and Publication Years of Included Studies | Search Strategy/Data Sources | Country and VSL Context | Number of Studies/VSL Estimates | SANRA Score (Total 12) (See S6) [28] | |
| Anderson & Treich 2008 [29] | RP: 1972–1999; SP: 1982–2005 | Not clearly reported—many estimates from a previous review | International; Transport | 32 studies; 48 estimates (RP: 12; SP: 36); Results not reported in Table 2 as included studies published prior to 2007 | 6 | |
| Bahamonde-Birke et al., 2015 [30] | RP: 1976–1991; SP (contingent valuation): 1984–1999; SP (stated choice): 2003–2013 | RP studies from previous reviews and a literature review of SP studies using stated choice methodology (no search strategy) | International; Transport | 50 studies; 66 estimates (RP: 21; SP continent valuation: 32; SP stated choice: 13) | 5 | |
| Bellavance et al., 2009 [31] | RP: 1974–2004 | Key word search of 5 databases and 3 previous literature reviews. Key words not specified | International; Labour market | 37 studies; 32 estimates for primary analysis, 39 in sensitivity analysis. Results not reported in Table 2 as included studies published prior to 2007 | 10 | |
| Dekker et al., 2011 [32] | SP (contingent valuation):1983–2008 | Key word search using EconLit, Google scholar and EVRI databases | International; Transport; Environment | 26 studies; 47 estimates reported (77 estimates from original studies used in the meta-analysis) | 10 | |
| Doucouliagos et al., 2012 [33] | RP: 1974–2004 | Studies included in Bellavance et al. [31] | International; Labour market | See Bellavance et al. [31]; Results not reported in Table 2 as included studies published prior to 2007 | 9 | |
| Hein et al., 2016 [18] | SP: 1996–2011 | Key word search using Scopus database | Europe; Environment | 7 studies; 22 estimates | 10 | |
| Hultkrantz & Svensson 2012 [34] | RP: 2005–2009; SP: 1996–2010 | EconLit and Pubmed databases and Google Scholar (search strategy not specified) | Sweden; All contexts | 12 studies; 48 estimates | 10 | |
| Lindhjem et al., 2011 [27] | SP: 1970–2008 | Search covering academic journal databases and the grey literature | International; Transport; Environment; Health | 75 studies; 856 estimates | 10 | |
| Masterman & Viscusi 2018 [35] | SP: Not reported | Data from 2 studies (Lindhjem et al. [27] and Robinson et al. [22]) | International; All contexts | 92 studies; 1145 estimates; The results are not reported in Table 2 due to significant overlap between this dataset and other included studies | 9 | |
| Milligan et al., 2014 [36] | SP: 1970–2013 | Uses the SP database reported by Lindhjem et al. [27]. Search strategy for additional studies not specified | International; All contexts | 79 studies; 862 estimates. There is significant overlap between this dataset and other included studies. Table 2 reports the results from the three additional studies not included in other included reviews | 9 | |
| Robinson & Hammitt 2016 [37] | RP: 2003–2014 SP: 2001–2013 | Studies from previous reviews and contacts with VSL researchers supplemented with an EconLit database search (strategy not specified) | USA; All contexts | 9 studies; 14 estimates | 10 | |
| Robinson et al., 2019 [22] | RP: 2007–2014 SP: 2003–2014 | Studies from previous reviews and contacts with VSL researchers supplemented with a literature search (databases not specified) | International; All contexts | 26 studies; 27 estimates (18 SP; 9 RP) | 8 | |
| Viscusi & Masterman 2017 [38] | RP: 1974–2016 | Data from 3 previous studies (Bellavance et al. [31], Viscusi [23] and Viscusi & Aldy [39]) supplemented with a keyword EconLit database search | International; Labour market | 68 Studies; 1025 estimates; Table 2 reports estimates from the international studies and a summary of the CFOI dataset | 10 | |
| Viscusi 2015 [23] | RP: 2003–2014 | VSL estimates derived from CFOI data. Search strategy not specified | USA (supplemented with international studies); Labour market | 17 studies; 550 estimates. The results are not reported in Table 2 due to significant overlap between this dataset and Viscusi & Masterman 2017 [38] | 9 | |
| Wheeler & Dockins 2013 [40] | RP: Not reported | RP dataset from the EPA [41]. Search strategy not specified | USA; Labour market | 35 studies; 386 estimates | 7 | |
| Yaduma et al., 2013 [42] | RP & SP: 1974–2009 | Data from 2 previous reviews (Viscusi & Aldy [39] and Miller [43]) supplemented with key word search of 3 databases | International; All contexts | 83 studies; 83 estimates (21 SP; 62 RP) | 10 | |
| Primary Australian Studies | ||||||
| Author | Survey Year | Population and Risk Context | WTP Elicitation Method | Mortality Risk Attribute | Payment Vehicle | ISPOR 10 Item Checklist [26] (See S6) |
| Hensher et al., 2009 [44] | 2007 | NSW car drivers n = 213; Choice of car based road route based on following attributes: fatality/injury numbers, cost of the trip, travel time, number of speed cameras & speed limit; Public good | Stated choice experiment using face to face interviews to complete a computer survey | Number of deaths per year (range between 0–5) | Car running costs and tolls | Fully compliant on 5 criteria; Mostly compliant on 5 criteria |
| Hensher et al., 2011 [45] | 2007 | NSW pedestrians n = 99; Choice of pedestrian route based on the following attributes: fatality/injury numbers, cost, travel time, number of lanes of traffic, road speed limit & crossing type (zebra, lights etc.); Public good | Increase in monthly council rates/rent | Fully compliant on 6 criteria; Mostly compliant on 2 criteria; Somewhat compliant on 2 criteria | ||
| Study | Australian Studies Included | Minimum VSL Estimate a | Maximum VSL Estimate a | Median VSL a | Median VSL Estimate Using Income Elasticity of 0.5 b | VSLY Estimate a,c | ||
|---|---|---|---|---|---|---|---|---|
| 3% Discount Rate | 7% Discount Rate | 10% Discount Rate | ||||||
| Stated Preference Studies | ||||||||
| Anderson & Treich 2008 [29] | All VSL estimates from studies published prior to 2007 | |||||||
| Bahamonde-Birke et al., 2015 [30]-CV studies | ||||||||
| Bahamonde-Birke et al., 2015 [30]–SC studies | Hensher et al., 2011 [45]; Hensher et al., 2009 [44] | 3,665,233 | 116,716,019 | 7,581,962 d | 7,581,962 d | 328,014 | 568,716 | 775,327 |
| Dekker et al., 2011 [32] | 1,704,668 | 3,344,120 | 1,878,772 | 2,088,128 | 90,337 | 156,629 | 213,531 | |
| Hein et al., 2016 [18] | - | - | - | - | 88,136 (minimum: 37,118; maximum: 468,272) e | |||
| Hultkrantz & Svensson 2012 [34] | 2,514,675 | 24,564,302 | 7,369,291 | 8,707,750 | 376,718 | 653,161 | 890,449 | |
| Lindhjem et al., 2011 [27] | 284,209 | 10,231,524 | 4,717,651 | 6,114,775 | 264,540 | 458,664 | 625,293 | |
| Robinson & Hammitt 2016 [37] | 9,451,322 | 15,799,226 | 15,415,350 | 13,944,413 | 603,268 | 1045,958 | 1425,948 | |
| Robinson et al., 2019 [22] | 583,468 | 28,202,141 | 11,532,035 | 2,410,916 | 104,302 | 180,841 | 246,539 | |
| Milligan et al., 2014 [36] | 1,399,051 | 17,899,440 | 15,094,617 | 16,306,529 | 705,459 | 1,223,139 | 1,667,496 | |
| Median SP VSL | 1,399,051 | 17,899,440 | 7,581,962 | 7,581,962 | 328,014 | 568,716 | 775,327 | |
| Mean SP VSL | 2,755,655 | 30,965,253 | 9,084,240 | 8,370,241 | 353,234 | 612,444 | 834,940 | |
| Revealed Preference Studies | ||||||||
| Anderson & Treich 2008 [29] | All VSL estimates from RP studies published prior to 2007 | |||||||
| Bahamonde-Birke et al., 2015 [30]-CV | Kniesner & Leeth 1991 [46] | |||||||
| Bellavance et al., 2009 [31] | Kniesner & Leeth 1991 [46] Miller et al., 1997 [47] | |||||||
| Doucouliagos et al., 2012 [33] | ||||||||
| Hultkrantz & Svensson 2012 [34] | 4,049,761 | 7,043,063 | 5,546,412 | 6,026,316 | 260,713 | 452,029 | 616,248 | |
| Robinson & Hammitt 2016 [37] | 3,808,498 | 37,722,267 | 15,596,707 | 14,108,465 | 610,366 | 1,058,264 | 1442,723 | |
| Robinson et al., 2019 [22] | 1,642,971 | 111,900,063 | 17,101,389 | 7,014,189 | 303,450 | 526,128 | 717,267 | |
| Viscusi & Masterman 2017 [38] f | Kniesner & Leeth 1991 [46] Miller et al., 1997 [47] | 189,912 | 20,074,339 | 3,536,095 | 3,715,149 | 160,726 | 278,670 | 379,909 |
| 17,964,045 | 17,399,366 | 752,738 | 1,305,111 | 1799,249 | ||||
| Wheeler & Dockins 2013 [40] g | 10,842,282 | 8,229,684 | 10,757,518 | 465,396 | 806,912 | 1,100,058 | ||
| Median RP VSL | 2,725,735 | 20,074,339 | 11,913,195 | 8,885,852 | 384,423 | 666,520 | 908,662 | |
| Mean RP VSL | 2,422,786 | 37,516,403 | 11,329,055 | 9,836,834 | 425,565 | 737,852 | 1,005,909 | |
| Yaduma et al., 2013 [42] | Kniesner & Leeth 1991 [46] Miller et al., 1997 [47] | 990,572 | 8,464,034 | 2,261,696 | 1,007,897 | 43,604 | 75,601 | 103,067 |
| Median all studies VSL | 1,521,011 | 17,899,440 | 7,905,823 | 7,298,074 | 315,732 | 547,422 | 746,297 | |
| Mean all studies VSL | 2,497,608 | 31,754,063 | 9,603,764 | 8,370,241 | 362,117 | 627,845 | 855,936 | |
2.3. Data Extraction and Analysis
2.4. VSLY Calculation
2.5. Value Transfer Calculation
3. Results
4. Discussion
5. Conclusions/Policy Recommendations
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Australian Goverment. The Australian Government Guide to Regulation; Department of Prime Minister and Cabinet, Ed.; Commonwealth of Australia: Canberra, Australia, 2014.
- Office of Health Economics. Measuring and Valuing Outcomes; Office of Health Economics: London, UK, 2020; Available online: https://www.ohe.org/research/measuring-and-valuing-outcomes (accessed on 24 April 2020).
- Organisation for Economic Cooperation and Development (OECD). Mortality Risk Valuation in Environment, Health and Transport Policies; Organisation for Economic Cooperation and Development (OECD): Paris, France, 2012; pp. 1–139. ISBN 9789264130807. [Google Scholar]
- Department of Health (Ed.) Guidelines for Preparing a Submission to the Pharmaceutical Benefits Advisory Committee; Version 5.0; Commonwealth of Australia: Canberra, Australia, 2016. [Google Scholar]
- Department of Health. Technical Guidelines for Preparing Assessment Reports for the Medical Services Advisory Committee—Service Type: Investigative (Version 3.0), 3rd ed.; Department of Health, Ed.; Commonwealth of Australia: Canberra, Australia, 2017. [Google Scholar]
- Nyborg, K. Project evaluation with democratic decision-making: What does cost–benefit analysis really measure? Ecol. Econ. 2014, 106, 124–131. [Google Scholar] [CrossRef] [Green Version]
- Dobes, L. A Century of Australian Cost-Benefit Analysis; Department of Finance and Deregulation, Ed.; Commonwealth Government: Canberra, Australia, 2007. [Google Scholar]
- Swinburn, B.A.; Sacks, G.; Hall, K.D.; McPherson, K.; Finegood, D.T.; Moodie, M.L.; Gortmaker, S.L. The global obesity pandemic: Shaped by global drivers and local environments. Lancet 2011, 378, 804–814. [Google Scholar] [CrossRef]
- Gortmaker, S.L.; Swinburn, B.A.; Levy, D.; Carter, R.; Mabry, P.L.; Finegood, D.T.; Huang, T.; Marsh, T.; Moodie, M.L. Changing the future of obesity: Science, policy, and action. Lancet 2011, 378, 838–847. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Health in All Policies (HiAP) Framework for Country Action; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Wijnen, W.; Wesemann, P.; de Blaeij, A. Valuation of road safety effects in cost-benefit analysis. Eval. Program Plan. 2009, 32, 326–331. [Google Scholar] [CrossRef]
- Robinson, L.A. Estimating the values of mortality risk reductions in low- and middle-income countries. J. Benefit Cost Anal. 2017, 8, 205–214. [Google Scholar] [CrossRef] [Green Version]
- Majumder, A.; Madheswaran, S. Meta-analysis of value of statistical life estimates. IIM Kozhikode Soc. Manag. Rev. 2017, 6, 110–120. [Google Scholar] [CrossRef]
- Simon, N.B.; Dockins, C.; Maguire, K.B.; Newbold, S.C.; Krupnick, A.; Taylor, L.O. Policy Brief—What’s in a Name? A Search for Alternatives to “VSL”. Rev. Environ. Econ. Policy 2019, 13, 155–161. [Google Scholar] [CrossRef] [Green Version]
- Viscusi, W.K. Pricing lives: International guideposts for safety. Econ. Rec. 2018, 94, 1–10. [Google Scholar] [CrossRef]
- Abelson, P. Establishing a Monetary Value for Lives Saved: Issues and Controversies; WP 2008-02; Office of Best Practice Regulation, Department of Finance and Deregulation: Canberra, Australia, 2008. [Google Scholar]
- Abelson, P. The value of life and health for pubic policy. Econ. Rec. 2003, 79, S2–S13. [Google Scholar] [CrossRef]
- Hein, L.; Roberts, P.; Gonzalez, L. Valuing a statistical life year in relation to clean air. J. Environ. Assess. Policy Manag. 2016, 18, 1650025. [Google Scholar] [CrossRef] [Green Version]
- Desaigues, B.; Ami, D.; Bartczak, A.; Braun-Kohlová, M.; Chilton, S.; Czajkowski, M.; Farreras, V.; Hunt, A.; Hutchison, M.; Jeanrenaud, C.; et al. Economic valuation of air pollution mortality: A 9-country contingent valuation survey of value of a life year (VOLY). Ecol. Indic. 2011, 11, 902–910. [Google Scholar] [CrossRef]
- Access Economics. The Health of Nations: The Value of a Statistical Life; Commonwealth of Australia: Canberra, Australia, 2007. [Google Scholar]
- Office of Best Practice Regulation. Best Practice Regulation Guidance Note: Value of Statistical Life; Department of the Prime Minister and Cabinet, Ed.; Australian Government: Canberra, Australia, 2014.
- Robinson, L.A.; Hammitt, J.K.; O’Keeffe, L. Valuing mortality risk reductions in global benefit-cost analysis. J. Benefit Cost Anal. 2019, 10, 15–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Viscusi, W.K. The role of publication selection bias in estimates of the value of a statistical life. Am. J. Health Econ. 2015, 1, 27–52. [Google Scholar] [CrossRef]
- Alberini, A. Revealed versus Stated Preferences: What Have We Learned About Valuation and Behavior? Rev. Environ. Econ. Policy 2019, 13, 283–298. [Google Scholar] [CrossRef]
- Whitty, J.A.; Lancsar, E.; Rixon, K.; Golenko, X.; Ratcliffe, J. A systematic review of stated preference studies reporting public preferences for healthcare priority setting. Patient Patient Cent. Outcomes Res. 2014, 7, 365–386. [Google Scholar] [CrossRef] [PubMed]
- Bridges, J.F.P.; Hauber, A.B.; Marshall, D.; Lloyd, A.; Prosser, L.A.; Regier, D.A.; Johnson, F.R.; Mauskopf, J. Conjoint analysis applications in health—A Checklist: A report of the ISPOR Good Research Practices for Conjoint Analysis task force. Value Health 2011, 14, 403–413. [Google Scholar] [CrossRef] [Green Version]
- Lindhjem, H.; Navrud, S.; Braathen, N.A.; Biausque, V. Valuing mortality risk reductions from environmental, transport, and health policies: A global meta-analysis of stated preference studies. Risk Anal. Int. J. 2011, 31, 1381–1407. [Google Scholar] [CrossRef] [PubMed]
- Baethge, C.; Goldbeck-Wood, S.; Mertens, S. SANRA—A scale for the quality assessment of narrative review articles. Res. Integr. Peer Rev. 2019, 4, 5. [Google Scholar] [CrossRef] [Green Version]
- Andersson, H.; Treich, N. The Value of a Statistical Life; Federal Reserve Bank of St Louis: St. Louis, MO, USA, 2008. [Google Scholar]
- Bahamonde-Birke, F.J.; Kunert, U.; Link, H. The value of a statistical life in a road safety context—A review of the current literature. Transp. Rev. 2015, 35, 488–511. [Google Scholar] [CrossRef]
- Bellavance, F.; Dionne, G.; Lebeau, M. The value of a statistical life: A meta-analysis with a mixed effects regression model. J. Health Econ. 2009, 28, 444–464. [Google Scholar] [CrossRef] [PubMed]
- Dekker, T.; Brouwer, R.; Hofkes, M.; Moeltner, K. The effect of risk context on the value of a statistical life: A Bayesian meta-model. Environ. Resour. Econ. 2011, 49, 597–624. [Google Scholar] [CrossRef] [Green Version]
- Doucouliagos, C.; Stanley, T.D.; Giles, M. Are estimates of the value of a statistical life exaggerated? J. Health Econ. 2012, 31, 197–206. [Google Scholar] [CrossRef] [Green Version]
- Hultkrantz, L.; Svensson, M. The value of a statistical life in Sweden: A review of the empirical literature. Health Policy 2012, 108, 302–310. [Google Scholar] [CrossRef] [PubMed]
- Masterman, C.J.; Kip Viscusi, W. The income elasticity of global values of a statistical life: Stated preference evidence. J. Benefit Cost Anal. 2018, 9, 407–434. [Google Scholar] [CrossRef] [Green Version]
- Milligan, C.; Kopp, A.; Dahdah, S.; Montufar, J. Value of a statistical life in road safety: A benefit-transfer function with risk-analysis guidance based on developing country data. Accid. Anal. Prev. 2014, 71, 236–247. [Google Scholar] [CrossRef] [Green Version]
- Robinson, L.A.; Hammitt, J.K. Valuing reductions in fatal illness risks: Implications of recent research. Health Econ. 2016, 25, 1039–1052. [Google Scholar] [CrossRef]
- Viscusi, W.K.; Masterman, C. Anchoring biases in international estimates of the value of a statistical life. J. Risk Uncertain. 2017, 54, 103–128. [Google Scholar] [CrossRef]
- Viscusi, W.K.; Aldy, J.E. The value of a statistical life: A critical review of market estimates throughout the world. J. Risk Uncertain. 2003, 27, 5–76. [Google Scholar] [CrossRef]
- Wheeler, W.; Dockins, C. Meta-Analysis and Publication Bias in the Hedonic Wage Literature; Federal Reserve Bank of St Louis: St. Louis, MO, USA, 2013. [Google Scholar]
- U.S. Environmental Protection Agency, National Center for Environmental Economics (Ed.) Valuing Mortality Risk Reductions for Environmental Policy: A White Paper; U.S. Environmental Protection Agency: Washington, DC, USA, 2010.
- Yaduma, N.; Kortelainen, M.; Wossink, A. Estimating mortality and economic costs of particulate air pollution in developing countries: The case of Nigeria. Environ. Resour. Econ. 2013, 54, 361–387. [Google Scholar] [CrossRef] [Green Version]
- Miller, T.R. Variations between countries in values of statistical life. J. Transp. Econ. Policy 2000, 34, 169–188. [Google Scholar]
- Hensher, D.A.; Rose, J.M.; Ortuzar, J.d.D.; Rizzi, L.I. Estimating the willingness to pay and value of risk reduction for car occupants in the road environment. Transp. Res. Part A Policy Pract. 2009, 43, 692–707. [Google Scholar] [CrossRef] [Green Version]
- Hensher, D.A.; Rose, J.M.; De Dios Ortúzar, J.; Rizzi, L.I. Estimating the value of risk reduction for pedestrians in the road environment: An exploratory analysis. J. Choice Model. 2011, 4, 70–94. [Google Scholar] [CrossRef] [Green Version]
- Kniesner, T.; Leeth, J.D. Compensating wage differentials for fatal injury risk in Australia, Japan, and the United States. J. Risk Uncertain. 1991, 4, 75–90. [Google Scholar] [CrossRef]
- Miller, P.; Mulvey, C.; Norris, K. Compensating differentials for risk of death in Australia. Econ. Rec. 1997, 73, 363–372. [Google Scholar] [CrossRef]
- The World Bank. GNI per Capita, Atlas Method (Current US$). 2019. Available online: https://data.worldbank.org/indicator/NY.GNP.PCAP.CD?end=2017&name_desc=false&start=2005 (accessed on 26 April 2019).
- Organisation for Economic Cooperation and Development (OECD). PPPs and Exchange Rates. 2014. Available online: https://0-www-oecd--ilibrary-org.brum.beds.ac.uk/content/data/data-00004-en (accessed on 26 April 2019).
- Australian Institute of Health and Welfare. Health Expenditure Australia 2015–16; Cat. No. HWE 68; Australian Institute of Health and Welfare: Canberra, Australia, 2017; Volume 58. [Google Scholar]
- Dobes, L.; Leung, J.; Argyrous, G. Social Cost-Benefit Analysis in Australia and New Zealand: The State of Current Practice and What Needs to Be Done; ANU Press: Canberra, Australia, 2016. [Google Scholar]
- Australian Goverment. Cost-Benefit—Guidance Note; Department of Prime Minister and Cabinet, Ed.; Commonwealth of Australia: Canberra, Australia, 2016.
- Organisation for Economic Cooperation and Development (OECD). Gross National Income. 2019. Available online: https://data.oecd.org/natincome/gross-national-income.htm (accessed on 26 April 2019).
- Viscusi, W.K.; Masterman, C.J. Income elasticities and global values of a statistical life. J. Benefit Cost Anal. 2017, 8, 226–250. [Google Scholar] [CrossRef] [Green Version]
- Doucouliagos, H.; Stanley, T.D.; Viscusi, W.K. Publication selection and the income elasticity of the value of a statistical life. J. Health Econ. 2014, 33, 67–75. [Google Scholar] [CrossRef]
- Australian Institute of Health and Welfare. Health Expenditure Australia 2016–17; Cat. No. HWE 74; Australian Institute of Health and Welfare: Canberra, Australia, 2018; Volume 64. [Google Scholar]
- Clough, P.; Guria, J.; Bealing, M. Approaches To Valuing Injury and Mortality Risk in Transport Assessments; New Zealand Transport Agency: Wellington, New Zealand, 2015; 78p, ISBN 9780478445152. [Google Scholar]
- Kniesner, T.J.; Leeth, J.D. Hedonic wage equilibrium: Theory, evidence and policy. Found. Trends Microecon. 2010, 5, 229–299. [Google Scholar] [CrossRef]
- Cowgill, M. Which Countries Are Most Similar to Australia? Some Answers Might Surprise You; Grattan Institute: Melbourne, Australia, 2019; Available online: https://blog.grattan.edu.au/2019/04/which-countries-are-most-similar-to-australia-some-answers-might-surprise-you/ (accessed on 4 May 2020).
- Ministry of Transport (Ed.) Social Cost of Road Crashes And Injuries 2018 Update; New Zealand Government: Wellington, New Zealand, 2019.
- Chestnut, L.G.; De Civita, P. Economic Valuation of Mortality Risk Reduction: Review and Recommendations for Policy and Regulatory Analysis; Government of Canada: Ottawa, ON, Canada, 2009.
- Organisation for Economic Cooperation and Development (OECD). Valuing Mortality Risk Reduction in Regulatory Ananlysis of Environmental, Health and Transport Policies: Poliy Implications; OECD: Paris, France, 2011. [Google Scholar]
- Braathen, N.; Lindhjem, H.; Navrud, S. Valuing Lives Saved from Environmental, Transport and Health Policies: A Meta-Analysis of Stated Preference Studies. In Proceedings of the Managing the Social Impacts of Change from a Risk Perspective, Beijing, China, 15–17 April 2009. [Google Scholar]
- Hammitt, J.K. Valuing changes in mortality risk: Lives saved versus life years saved. Rev. Environ. Econ. Policy 2007, 1, 228–240. [Google Scholar] [CrossRef]
- Australian Bureau of Statistics. 3302.0.55.001—Life Tables, States, Territories and Australia, 2016–2018. Available online: https://www.abs.gov.au/ausstats/[email protected]/mf/3302.0.55.001 (accessed on 30 April 2020).
- Ryen, L.; Svensson, M. The Willingness to Pay for a Quality Adjusted Life Year: A Review of the Empirical Literature. Health Econ. 2015, 24, 1289–1301. [Google Scholar] [CrossRef]
- Hammitt, J.K.; Haninger, K. Valuing nonfatal health risk as a function of illness severity and duration: Benefit transfer using QALYs. J. Environ. Econ. Manag. 2017, 82, 17–38. [Google Scholar] [CrossRef]
- George, B.; Harris, A.; Mitchell, A. Cost-effectiveness analysis and the consistency of decision making. Pharmacoeconomics 2001, 19, 1103–1109. [Google Scholar] [CrossRef] [PubMed]

| Author | Sample Size | Number of VSL Estimates | Minimum VSL Estimate | Maximum VSL Estimate | Mean/Median VSL Estimate | VSLY Estimate a | ||
|---|---|---|---|---|---|---|---|---|
| 3% Discount Rate | 7% Discount Rate | 10% Discount Rate | ||||||
| Hensher et al., 2009 [44] | 213 | 2 | 7,524,566 | 7,610,102 | 7,567,334 | 327,381 | 567,619 | 773,831 |
| Hensher et al., 2011 [45] | 99 | 3 | 5,071,123 | 6,394,432 | 5,829,987 | 252,219 | 437,302 | 596,171 |
| Weighted mean VSL from primary studies b | 7,016,060 | 303,531 | 526,269 | 717,458 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ananthapavan, J.; Moodie, M.; Milat, A.J.; Carter, R. Systematic Review to Update ‘Value of a Statistical Life’ Estimates for Australia. Int. J. Environ. Res. Public Health 2021, 18, 6168. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18116168
Ananthapavan J, Moodie M, Milat AJ, Carter R. Systematic Review to Update ‘Value of a Statistical Life’ Estimates for Australia. International Journal of Environmental Research and Public Health. 2021; 18(11):6168. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18116168
Chicago/Turabian StyleAnanthapavan, Jaithri, Marj Moodie, Andrew J. Milat, and Rob Carter. 2021. "Systematic Review to Update ‘Value of a Statistical Life’ Estimates for Australia" International Journal of Environmental Research and Public Health 18, no. 11: 6168. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18116168