
Association between Shift Work and Reflux Esophagitis: The Kangbuk Samsung Health Study


Abstract
:1. Introduction
2. Materials and Methods
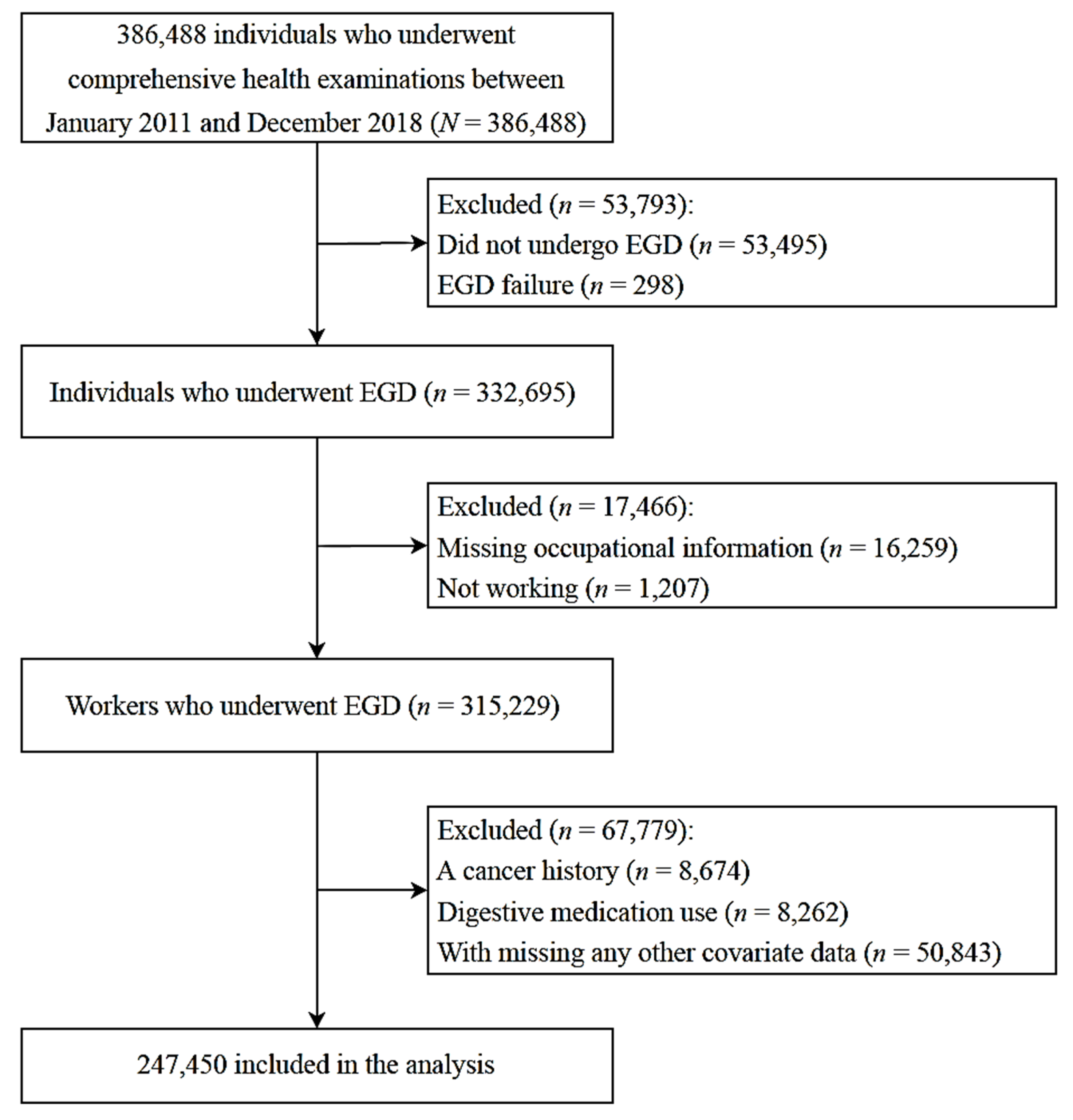
2.1. Study Design and Participants
2.2. Measurement of Types of Shift Work
- Fixed evening shift (between 2 PM and 12 AM);
- Fixed night shift (between 9 PM and next day AM);
- Regular day and night shifts;
- 24 h shifts;
- Split shift;
- Irregular shift work.
2.3. Mesasurement and Classification of Reflux Esophagitis
- LA-M: no esophageal mucosal injury, but white turbidity of the mucosa or redness with unclear boundaries that cannot be said to be mucosal damage.
- LA-A: mucosal injury with a major axis not exceeding 5 mm, limited to the mucosal folds.
- LA-B: at least one mucosal injury with a major axis of 5 mm or more; mucosal injuries on different mucosal folds are not continuous with each other.
- LA-C: mucosal injury in at least one place that spreads continuously to two or more folds but involves less than 75% of the circumference.
- LA-D: continuous mucosal injury involving at least 75% of the esophageal circumference.
2.4. Mesasurement of Covariates
2.5. Statistical Analysis
3. Results
3.1. Participant Characteristics
3.2. The Distribution of Endoscopic Findings of Reflux Esophagitis
3.3. Association between Shift Work and Reflux Esophagitis
3.4. Association between Shift Work Schedules and Types of Reflux Esophagitis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Harrington, J.M. Health effects of shift work and extended hours of work. Occup. Environ. Med. 2001, 58, 68–72. [Google Scholar] [CrossRef] [Green Version]
- Eurofound. Sixth European Working Conditions Survey—Overview Report (2017 update); Publications Office of the European Union: Luxembourg, 2017. [Google Scholar]
- Maestas, N.; Mullen, K.J.; Powell, D.; von Wachter, T.; Wenger, J.B. Working Conditions in the United States: Results of the 2015 American Working Conditions Survey; RAND Corporation: Santa Monica, CA, USA, 2017; Available online: https://www.rand.org/pubs/research_reports/RR2014.html (accessed on 31 January 2021).
- Korean Working Environment Survey. Occupational Safety and Health Research Institute, Korea Safety and Health Agency. Korea Social Sciences Archive (KOSSDA). 2017. Available online: http://hdl.handle.net/20.500.12236/23243 (accessed on 31 January 2021).
- Vyas, M.V.; Garg, A.X.; Iansavichus, A.V.; Costella, J.; Donner, A.; Laugsand, L.E.; Janszky, I.; Mrkobrada, M.; Parraga, G.; Hackam, D.G. Shift work and vascular events: Systematic review and meta-analysis. BMJ 2012, 345, e4800. [Google Scholar] [CrossRef] [Green Version]
- Anothaisintawee, T.; Reutrakul, S.; Van Cauter, E.; Thakkinstian, A. Sleep disturbances compared to traditional risk factors for diabetes development: Systematic review and meta-analysis. Sleep Med. Rev. 2015, 30, 11–24. [Google Scholar] [CrossRef]
- Proper, K.I.; van de Langenberg, D.; Rodenburg, W.; Vermeulen, R.C.; van der Beek, A.J.; van Steeg, H.; van Kerkhof, L.W. The relationship between shift work and metabolic risk factors: A systematic review of longitudinal studies. Am. J. Prev. Med. 2016, 50, e147–e157. [Google Scholar] [CrossRef]
- Ijaz, S.; Verbeek, J.; Seidler, A.; Lindbohm, M.L.; Ojajärvi, A.; Orsini, N.; Costa, G.; Neuvonen, K. Night-shift work and breast cancer—a systematic review and meta-analysis. Scand. J. Work Environ. Health 2013, 39, 431–447. [Google Scholar] [CrossRef]
- Wang, X.; Ji, A.; Zhu, Y.; Liang, Z.; Wu, J.; Li, S.; Meng, S.; Zheng, X.; Xie, L. A meta-analysis including dose-response relationship between night shift work and the risk of colorectal cancer. Oncotarget 2015, 6, 25046–25060. [Google Scholar] [CrossRef] [Green Version]
- Rao, D.; Yu, H.; Bai, Y.; Zheng, X.; Xie, L. Does night-shift work increase the risk of prostate cancer? A systematic review and meta-analysis. OncoTargets Ther. 2015, 8, 2817–2826. [Google Scholar]
- Lin, X.; Chen, W.; Wei, F.; Ying, M.; Wei, W.; Xie, X. Night-shift work increases morbidity of breast cancer and all-cause mortality: A meta-analysis of 16 prospective cohort studies. Sleep Med. 2015, 16, 1381–1387. [Google Scholar] [CrossRef]
- Kecklund, G.; Axelsson, J. Health consequences of shift work and insufficient sleep. BMJ 2016, 355, i5210. [Google Scholar] [CrossRef] [PubMed]
- Konturek, P.C.; Brzozowski, T.; Konturek, S.J. Gut clock: Implication of circadian rhythms in the gastrointestinal tract. J. Physiol. Pharmacol. 2011, 62, 139–150. [Google Scholar]
- Vakil, N.; Van Zanten, S.V.; Kahrilas, P.; Dent, J.; Jones, R. The Montreal definition and classification of gastroesophageal reflux disease: A global evidence-based consensus. Am. J. Gastroenterol. 2006, 101, 1900–1920. [Google Scholar]
- Jones, R.; Galmiche, J.P. What do we mean by GERD?–definition and diagnosis. Aliment. Pharmacol. Ther. 2005, 22, 2–10. [Google Scholar] [CrossRef]
- Xue, J.; Zhao, Y.; Wang, Z.; Ren, N.; Zhou, C.; Qin, S. Rotating night shift work is associated with an increased risk of gastroesophageal reflux disease (GERD) symptoms among workers in China: A cross-sectional study. Int. J. Clin. Pract. 2021, 75, e13848. [Google Scholar] [CrossRef]
- Li, Y.M.; Du, J.; Zhang, H.; Yu, C.H. Epidemiological investigation in outpatients with symptomatic gastroesophageal reflux from the Department of Medicine in Zhejiang Province, east China. J. Gastroenterol. Hepatol. 2008, 23, 283–289. [Google Scholar] [CrossRef] [PubMed]
- Wong, B.C.; Kinoshita, Y. Systematic review on epidemiology of gastroesophageal reflux disease in Asia. Clin. Gastroenterol. Hepatol. 2006, 4, 398–407. [Google Scholar] [CrossRef]
- Savarino, E.; De Bortoli, N.; De Cassan, C.; Coletta, M.D.; Bartolo, O.; Furnari, M.; Ottonello, A.; Marabotto, E.; Bodini, G.; Savarino, V. The natural history of gastro-esophageal reflux disease: A comprehensive review. Dis. Esophagus 2017, 30. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Lancet 2007, 370, 1453–1457. [Google Scholar] [CrossRef]
- Iwakiri, K.; Kawami, N.; Nomura, T.; Hoshihara, Y. Tips for the diagnosis and treatment of reflux esophagitis. Gastroenterol. Endosc. 2015, 57, 1641–1647. [Google Scholar]
- Eusebi, L.H.; Ratnakumaran, R.; Yuan, Y.; Solaymani-Dodaran, M.; Bazzoli, F.; Ford, A.C. Global prevalence of, and risk factors for, gastro-oesophageal reflux symptoms: A meta-analysis. Gut 2018, 67, 430–440. [Google Scholar] [CrossRef]
- Richter, J.E.; Rubenstein, J.H. Presentation and epidemiology of gastroesophageal reflux disease. Gastroenterology 2018, 154, 267–276. [Google Scholar] [CrossRef]
- Nam, K.; Shin, J.E.; Kim, S.E.; Baik, G.H.; Choi, S.H.; Lee, J.Y.; Park, K.S.; Joo, Y.E.; Myung, D.S.; Kim, H.J.; et al. Prevalence and risk factors for upper gastrointestinal diseases in health check-up subjects: A nationwide multicenter study in Korea. Scand. J. Gastroenterol. 2018, 53, 910–916. [Google Scholar] [CrossRef] [PubMed]
- Depner, C.M.; Stothard, E.R.; Wright, K.P. Metabolic consequences of sleep and circadian disorders. Curr. Diabetes Rep. 2014, 14, 1–9. [Google Scholar] [CrossRef]
- Reiter, R.J.; Tan, D.X.; Mayo, J.C.; Sainz, R.M.; Leon, J.; Czarnocki, Z. Melatonin as an antioxidant: Biochemical mechanisms and pathophysiological implications in humans. Acta Biochim. Pol. 2003, 50, 1129–1146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Konturek, S.J.; Zayachkivska, O.; Havryluk, X.O.; Brzozowski, T.; Sliwowski, Z.; Pawlik, M.; Konturek, P.C.; Czesnikiewicz-Guzik, M.; Gzhegotsky, M.R.; Pawlik, W.W. Protective influence of melatonin against acute esophageal lesions involves prostaglandins, nitric oxide and sensory nerves. J. Physiol. Pharmacol. 2007, 58, 361–377. [Google Scholar]
- Kato, K.; Murai, I.; Asai, S.; Takahashi, Y.; Matsuno, Y.; Komuro, S.; Kurosaka, H.; Iwasaki, A.; Ishikawa, K.; Arakawa, Y. Central nervous system action of melatonin on gastric acid and pepsin secretion in pylorusligated rats. Neuroreport 1998, 9, 2447–2450. [Google Scholar] [CrossRef]
- Bubenik, G.A. Gastrointestinal melatonin: Localization, function, and clinical relevance. Dig. Dis. Sci. 2002, 47, 2336–2348. [Google Scholar] [CrossRef]
- Bang, C.S.; Yang, Y.J.; Baik, G.H. Melatonin for the treatment of gastroesophageal reflux disease; protocol for a systematic review and meta-analysis. Medicine 2019, 98, e14241. [Google Scholar] [CrossRef] [PubMed]
- Souza, R.V.D.; Sarmento, R.A.; Almeida, J.C.D.; Canuto, R. The effect of shift work on eating habits: A systematic review. Scand. J. Work Environ. Health 2019, 45, 7–21. [Google Scholar] [CrossRef]
- Lowden, A.; Moreno, C.; Holmbäck, U.; Lennernäs, M.; Tucker, P. Eating and shift work—Effects on habits, metabolism, and performance. Scand. J. Work Environ. Health 2010, 150–162. [Google Scholar] [CrossRef]
- Fujiwara, Y.; Machida, A.; Watanabe, Y.; Shiba, M.; Tominaga, K.; Watanabe, T.; Oshitani, N.; Higuchi, K.; Arakawa, T. Association between dinner-to-bed time and gastro-esophageal reflux disease. Am. J. Gastroenterol. 2005, 100, 2633–2636. [Google Scholar] [CrossRef]
- Esmaillzadeh, A.; Keshteli, A.H.; Feizi, A.; Zaribaf, F.; Feinle-Bisset, C.; Adibi, P. Patterns of diet-related practices and prevalence of gastro-esophageal reflux disease. Neurogastroenterol. Motil. 2013, 25, 831-e638. [Google Scholar]
- Yamamichi, N.; Mochizuki, S.; Asada-Hirayama, I.; Mikami-Matsuda, R.; Shimamoto, T.; Konno-Shimizu, M.; Takahashi, Y.; Takeuchi, C.; Niimi, K.; Ono, S.; et al. Lifestyle factors affecting gastroesophageal reflux disease symptoms: A cross-sectional study of healthy 19864 adults using FSSG scores. BMC Med. 2012, 10, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Vandelanotte, C.; Short, C.; Rockloff, M.; Di Millia, L.; Ronan, K.; Happell, B.; Duncan, M.J. How do different occupational factors influence total, occupational, and leisure-time physical activity? J. Phys. Act. Health 2015, 12, 200–207. [Google Scholar] [CrossRef] [PubMed]
- van Amelsvoort, L.G.; Jansen, N.W.; Kant, I. Among shift workers: More than a confounding factor. Chronobiol. Int. 2006, 23, 1105–1113. [Google Scholar] [CrossRef]
- Richter, K.; Peter, L.; Rodenbeck, A.; Weess, H.G.; Riedel-Heller, S.G.; Hillemacher, T. Shiftwork and alcohol consumption: A systematic review of the literature. Eur. Addict. Res. 2021, 27, 9–15. [Google Scholar] [CrossRef]
- Pyo, J.H.; Kim, J.W.; Kim, T.J.; Lee, H.; Min, Y.W.; Min, B.H.; Lee, J.H.; Rhee, P.L.; Jung, S.H.; Cha, K.M.; et al. Physical activity protects against the risk of erosive esophagitis on the basis of body mass index. J. Clin. Gastroenterol. 2019, 53, 102–108. [Google Scholar] [CrossRef]
- Gong, Y.; Zeng, Q.; Yan, Y.; Han, C.; Zheng, Y. Association between lifestyle and gastroesophageal reflux disease questionnaire scores: A cross-sectional study of 37 442 Chinese adults. Gastroenterol. Res. Pract. 2019, 5753813. [Google Scholar] [CrossRef]
- Pan, J.; Cen, L.; Chen, W.; Yu, C.; Li, Y.; Shen, Z. Alcohol consumption and the risk of gastroesophageal reflux disease: A systematic review and meta-analysis. Alcohol Alcohol. 2019, 54, 62–69. [Google Scholar] [CrossRef]
- Ness-Jensen., E.; Lagergren, J. Tobacco smoking, alcohol consumption and gastro-oesophageal reflux disease. Best Pract. Res. Clin. Gastroenterol. 2017, 31, 501–508. [Google Scholar] [CrossRef] [Green Version]
- Wang, F.; Zhang, L.; Zhang, Y.; Zhang, B.A.; He, Y.; Xie, S.; Li, M.; Miao, X.; Chan, E.Y.Y.; Tang, J.L.; et al. Meta-analysis on night shift work and risk of metabolic syndrome. Obes. Rev. 2014, 15, 709–720. [Google Scholar] [CrossRef]
- Park, J.H.; Park, D.I.; Kim, H.J.; Cho, Y.K.; Sohn, C.I.; Jeon, W.K.; Kim, B.I. Metabolic syndrome is associated with erosive esophagitis. World J. Gastroenterol. 2008, 14, 5442. [Google Scholar] [CrossRef]
- Mancio, J.; Leal, C.; Ferreira, M.; Norton, P.; Lunet, N. Does the association of prostate cancer with night-shift work differ according to rotating vs. fixed schedule? A systematic review and meta-analysis. Prostate Cancer Prostatic Dis. 2018, 21, 337–344. [Google Scholar] [CrossRef] [Green Version]
- Gupta, C.C.; Coates, A.M.; Dorrian, J.; Banks, S. The factors influencing the eating behaviour of shiftworkers: What, when, where and why. Ind. Health 2019, 57, 419–453. [Google Scholar] [CrossRef] [Green Version]
- Azer, S.A.; Reddivari, A.K.R. Reflux Esophagitis. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2021; PMID: 32119349. [Google Scholar]
- Chung, T.H.; Lee, J.; Kim, M.C. Impact of night-shift work on the prevalence of erosive esophagitis in shipyard male workers. Int. Arch. Occup. Environ. Health 2016, 89, 961–966. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zografos, G.N.; Georgiadou, D.; Thomas, D.; Kaltsas, G.; Digalakis, M. Drug-induced esophagitis. Dis Esophagus 2009, 22, 633–637. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Reflux Esohpagitis | ||||
|---|---|---|---|---|
| Variable Category | Total | (−) | (+) | p-Value |
| N (%) | 247,450 (100) | 197,683 (79.9) | 49,767 (20.1) | |
| Age, years | 36 (31–42) | 36 (31–42) | 35 (30–41) | <0.001 |
| Sex, % male | 65.0 | 61.9 | 77.5 | <0.001 |
| Current smoker, % yes | 23.7 | 21.9 | 30.6 | <0.001 |
| Alcohol intake, g/day | 7 (3–20) | 7 (3–20) | 10 (3–26) | <0.001 |
| Exercise, % yes | 39.9 | 39.3 | 42.0 | <0.001 |
| Glucose, mg/dL | 93 (88–99) | 93 (88–98) | 94 (89–100) | <0.001 |
| BMI, kg/m2 | 23.4 (21.2–25.6) | 23.2 (21.0–25.4) | 24.1 (21.8–26.4) | <0.001 |
| Waist circumference, cm | 82 (75–89) | 82 (74–88) | 85 (78–91) | <0.001 |
| Total cholesterol, mg/dL | 190 (169–214) | 190 (169–213) | 192 (171–216) | <0.001 |
| HDL-C, mg/dL | 57 (47–68) | 57 (48–69) | 55 (46–66) | <0.001 |
| LDL-C, mg/dL | 120 (99–143) | 119 (99–142) | 123 (101–146) | <0.001 |
| Triglycerides, mg/dL | 91 (64–137) | 89 (63–132) | 103 (71–156) | <0.001 |
| Marital status, % married | 74.1 | 74.4 | 72.8 | <0.001 |
| Education, % college or more | 84.6 | 84.4 | 85.6 | <0.001 |
| Shift work (%) | 23,178 (9.4) * | 18,223 (9.2) | 4955 (10.0) | <0.001 |
| Fixed evening shift (%) | 2132 (0.9) | 1749 (0.9) | 383 (0.8) | 0.01 |
| Fixed night shift (%) | 577 (0.2) | 472 (0.2) | 105 (0.2) | 0.25 |
| Regular day and night shifts (%) | 7442 (3.0) | 5723 (2.9) | 1719 (3.5) | <0.001 |
| 24 h shifts (%) | 3232 (1.3) | 2534 (1.3) | 698 (1.4) | 0.03 |
| Split shift (%) | 1127 (0.5) | 911 (0.5) | 216 (0.4) | 0.43 |
| Irregular shift (%) | 3788 (1.5) | 2934 (1.5) | 854 (1.7) | <0.001 |
| RE Classification | ||||||
|---|---|---|---|---|---|---|
| Total N | Normal | LA-M | LA-A | LA-B | ≥LA-C | |
| N (%) | 247,450 (100) | 197,683 (79.9) | 31,132 (12.6) | 16,213 (6.6) | 2333 (0.9) | 89 (0.04) |
| Sex | ||||||
| Male, n (%) | 160,829 (100) | 122,269 (76.0) | 21,356 (13.3) | 14,906 (9.3) | 2210 (1.4) | 88 (0.1) |
| Female, n (%) | 86,621 (100) | 75,414 (87.1) | 9776 (11.3) | 1307 (1.5) | 123 (0.1) | 1 (0.001) |
| Age | ||||||
| 18–29, n (%) | 42,249 (100) | 33,435 (79.1) | 6096 (14.4) | 2470 (5.8) | 238 (0.6) | 10 (0.02) |
| 30–39, n (%) | 12,2301 (100) | 96,949 (79.3) | 15,954 (13.0) | 8298 (6.8) | 1072 (0.9) | 28 (0.02) |
| 40–49, n (%) | 59,243 (100) | 47,646 (80.4) | 6931 (11.7) | 3946 (6.7) | 684 (1.2) | 36 (0.1) |
| 50–59, n (%) | 18,710 (100) | 15,499 (82.8) | 1766 (9.4) | 1184 (6.3) | 248 (1.3) | 13 (0.1) |
| ≥60, n (%) | 4947 (100) | 4154 (84.0) | 385 (7.8) | 315 (6.4) | 91 (1.8) | 2 (0.04) |
| Work Type | Crude Model | Age and Sex Adjusted Model | Multivariate-Adjusted Models | |
|---|---|---|---|---|
| Model 1 | Model 2 | |||
| Fixed day work | 1.00 (Ref.) | 1.00 (Ref.) | 1.00 (Ref.) | 1.00 (Ref.) |
| Shift work | 1.09 (1.05–1.13) | 1.18 (1.14–1.22) | 1.15 (1.11–1.20) | 1.15 (1.11–1.19) |
| RE Classification | ||||
|---|---|---|---|---|
| Work Type | Overall | LA-M | LA-A | ≥LA-B |
| Fixed day work | 1.00 (Ref.) | 1.00 (Ref.) | 1.00 (Ref.) | 1.00 (Ref.) |
| Shift work | 1.15 (1.11–1.19) | 1.17 (1.12–1.21) | 1.11 (1.05–1.18) | 1.14 (0.98–1.33) |
| Fixed evening shift | 1.10 (0.98–1.23) | 1.10 (0.97–1.25) | 1.08 (0.88–1.33) | 1.25 (0.78–2.00) |
| Fixed night shift | 0.94 (0.76–1.17) | 0.85 (0.64–1.11) | 1.09 (0.78–1.53) | 1.32 (0.65–2.68) |
| Regular day and night shifts | 1.20 (1.13–1.27) | 1.22 (1.14–1.31) | 1.14 (1.03–1.26) | 1.24 (0.97–1.58) |
| 24 h shifts | 1.17 (1.07–1.28) | 1.20 (1.09–1.33) | 1.12 (0.96–1.31) | 1.03 (0.66–1.59) |
| Split shift | 1.08 (0.93–1.26) | 1.13 (0.95–1.34) | 1.02 (0.77–1.35) | 0.94 (0.44–1.98) |
| Irregular shift | 1.17 (1.08–1.26) | 1.14 (1.03–1.25) | 1.26 (1.11–1.44) | 1.05 (0.73–1.53) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mun, E.; Kim, D.; Lee, Y.; Lee, W.; Park, S. Association between Shift Work and Reflux Esophagitis: The Kangbuk Samsung Health Study. Int. J. Environ. Res. Public Health 2021, 18, 6189. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18126189
Mun E, Kim D, Lee Y, Lee W, Park S. Association between Shift Work and Reflux Esophagitis: The Kangbuk Samsung Health Study. International Journal of Environmental Research and Public Health. 2021; 18(12):6189. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18126189
Chicago/Turabian StyleMun, Eunchan, Daehoon Kim, Yesung Lee, Woncheol Lee, and Soyoung Park. 2021. "Association between Shift Work and Reflux Esophagitis: The Kangbuk Samsung Health Study" International Journal of Environmental Research and Public Health 18, no. 12: 6189. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18126189