
Application of a Scorecard Tool for Assessing and Engaging Media on Responsible Reporting of Suicide-Related News in India

 , , , , and
, , , , and
Abstract
:1. Introduction
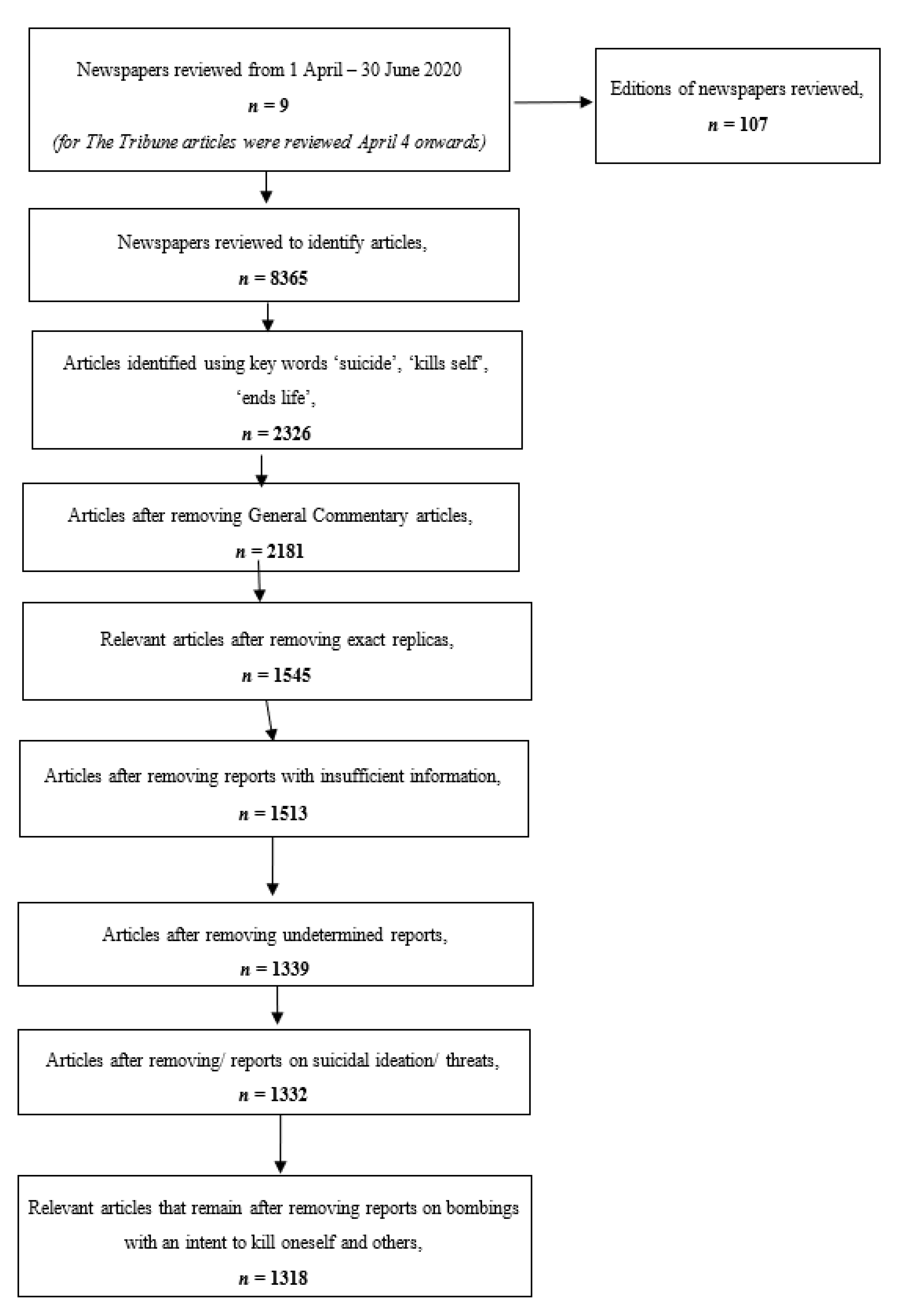
2. Methodology
2.1. Review of Existing Assessment Tools on Suicide Reporting
2.2. Development of Assessment Tool for Scoring Suicide Reports
3. Results
Assessment of Reports on The Positive and Negative Scorecard
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
| Positive Scorecard | ||
|---|---|---|
| Positive Parameter | Description | Example |
| Presence of help seeking information | Provides information of national or state-level support services that includes suicide prevention centers, emergency units in hospitals, 24/7 crisis helplines, self-help groups, mental health professionals’ general physicians, community resources, rehabilitation centers. | “Those in distress or having suicidal tendencies could seek help and counselling by call Sneha - 044- 24640050” |
| Information is up to date and operational | The information and contact details provided should be accurate and reliable. By operational we mean it should be relevant to where the article is published. This can be verified through a Google search. | Placed at the bottom of the article. |
| Links to poor mental health | The report establishes a link between suicidal behavior and a mental illness, by making a clear reference to the individual’s struggle with a mental illness, its effect on their mental state. Inappropriate language such as “crazy” or “mental” is not accepted. Neither are mood qualifiers like “stressed”, “unhappy” etc. | “Before ending his life, the deceased, who was said to be depressed” |
| Links to drug/ alcohol abuse | The report acknowledges the link between the suicide and the substance and alcohol use. The report clearly refers to the person’s ongoing struggle with alcohol or drug addiction. A reference to the person’s intoxicated state at the time of suicide does not qualify. | “Owing to the liquor ban, Suneesh was in a state of alcohol withdrawal and took his life” |
| Comments from mental health and suicide prevention experts | The article contains a quote or comment from a mental health professional or suicide prevention expert. | “Dr. Singh, a psychiatrist at KEM Hospital encourages reaching out to family members or friends who are disconnected, alone and have expressed distress.” |
| Reduces stigma highlights suicides are preventable | The article highlights that suicides are preventable by taking preventive measures and identifying risks in time and contains information that reduces stigma around talking about suicide and mental health concerns. | “Suicides can be prevented and it’s okay to talk about how you are feeling,” |
| Credible population-level suicide statistics and/ or other research findings | The article reports on suicide-related statistical data. It may also provide findings from studies conducted on suicide and suicide prevention. | “The Ministry of Agriculture reported 127 farmers who died by suicide during the period of the lockdown.” |
| Challenges popular myths | The report challenges popular myths and reinforces false nature of such myths:
| “Socially, mental illness and thoughts about suicide are not something we talk about… what we have learnt from the mental health partners and academics we have worked with is that being connected is a protective factor in suicide prevention.” |
| Links to hopeful stories | The report should have links to or snippets of reports that contain hopeful stories of people who have overcome suicidal thoughts and feelings. | “Mohammad Shami has spoken about suicidal thoughts he faced in the past and has opened up about the help he received to overcome those thoughts in this article.” |
| Verified information and facts from official source | Information and facts are verified by official sources that include police officers, healthcare professionals or a government authority in the area. | “Police confirmed, Harish jumped off the bridge at 1am last night” |
| Negative Scorecard | ||
|---|---|---|
| Negative Parameter | Description | Example |
| Use of criminalizing language | The article uses phrases that associates suicide with a crime or sin, ‘committed suicide’. | “He committed suicide by jumping off the balcony from his residence”. |
| Attention-grabbing headlines | The headline includes the word ‘suicide’, mentions a life event, the method or the reason for the suicide or attempted suicide. | “Man jumps to death on testing positive for COVID-19” “Woman commits suicide by hanging after marriage failure” |
| Describes method in detail | The article provides at least two specific details about the suicide/ attempted suicide method. | “… jumped from the third floor balcony by hoisting themselves off the grill” “… attempted to hang herself from a ceiling fan using her dupatta” |
| Method of suicide or attempted suicide is mentioned in the article | The article mentions the method of suicide or attempted suicide. | “He was found hanging in his room.” |
| Discloses details of the suicide site | The report provides enough information to clearly identify the location and it is somewhat accessible to at least some members of the public. | “The deceased took their life in their residence at Prestige Luxe Complex in Koramangala.” “After her test results came back negative, she took her life by jumping from the window of KEM Hospital.” |
| Reduces reason to a single factor or event | The article clearly articulates that the suicide incident had just one motive, cause or trigger. It over-simplifies the complex realities of suicide by reducing it to a single factor.The causal relationship is NOT subject to speculation. | “Upon losing his job, Prakash ended his life.” “Police said that he was under severe financial stress and therefore took this extreme step.” |
| Accompanying photos | The report publishes photographs or video footage of the deceased, bereaved members, the location of the suicide and the method as well as other dramatic/emotional images (e.g., a noose, slit wrists, person standing on the ledge, etc.). | |
| Contains information on grieving persons | The article reports on the effects of a suicide on bereaved persons or contains interview with bereaved persons. Relatives, friends of the victim and other private persons involved in the suicidal act or affected by the suicide are defined as bereaved persons. | “After no response from banging her door, her father kicked down the door and was shocked to find her hanging from the fan.” |
| Publishes note, text and social media post | The report publishes suicide notes, text messages, social media posts and emails of the deceased person and/or their family members. | “In his suicide note, the deceased said “I am ending my life because I see no point in living. No one is to blame for my death.” |
| Article is on the front page of the newspaper | The article is published on the first page. This includes articles that commence on the first page and are then continued in later pages. | |
References
- WHO Statistics on Suicide. Available online: https://www.who.int/mental_health/prevention/suicide/suicideprevent/en/ (accessed on 30 March 2021).
- National Crime Records Bureau (Accidental Deaths and Suicide in India) 2019. Available online: https://ncrb.gov.in/sites/default/files/Chapter-2-Suicides_2019.pdf (accessed on 30 March 2021).
- Reporting on Suicide during COVID19 Pandemic. Available online: https://www.iasp.info/pdf/2020_Briefing_Statement_Reporting_on_Suicide_During_COVID19.pdf (accessed on 30 March 2021).
- Dandona, R.; Kumar, G.A.; Dhaliwal, R.S.; Naghavi, M.; Vos, T.; Shukla, D.K.; Vijayakumar, L.; Gururaj, G.; Thakur, J.S.; Ambekar, A.; et al. Gender differentials and state variations in suicide deaths in India: The Global Burden of Disease Study 1990–2016. Lancet Public Health 2018, 3, e478–e489. [Google Scholar] [CrossRef] [Green Version]
- Niederkrotenthaler, T.; Voracek, M.; Herberth, A.; Till, B.; Strauss, M.; Etzersdorfer, E.; Eisenwort, B.; Sonneck, G. Role of media reports in completed and prevented suicide: Werther v. Papageno effects. Br. J. Psychiatry J. Ment. Sci. 2010, 197, 234–243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bilsen, J. Suicide and Youth: Risk Factors. Front. Psychiatry 2018, 9, 540. [Google Scholar] [CrossRef]
- Pirkis, J.; Blood, R.W. Suicide and the media. Part I: Reportage in nonfictional media. Crisis 2001, 22, 146–154. [Google Scholar] [CrossRef]
- Zalsman, G.; Hawton, K.; Wasserman, D.; van Heeringen, K.; Arensman, E.; Sarchiapone, M.; Carli, V.; Höschl, C.; Barzilay, R.; Balazs, J.; et al. Suicide prevention strategies revisited: 10-year systematic review. Lancet Psychiatry 2016, 3, 646–659. [Google Scholar] [CrossRef]
- Turecki, G.; Brent, D.A. Suicide and suicidal behaviour. Lancet 2016, 387, 1227–1239. [Google Scholar] [CrossRef]
- Niederkrotenthaler, T.; Braun, M.; Pirkis, J.; Till, B.; Stack, S.; Sinyor, M.; Tran, U.S.; Voracek, M.; Cheng, Q.; Arendt, F.; et al. Association between suicide reporting in the media and suicide: Systematic re-view and meta-analysis. BMJ 2020, 368, m575. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Armstrong, G.; Vijayakumar, L.; Niederkrotenthaler, T.; Jayaseelan, M.; Kannan, R.; Pirkis, J.; Jorm, A.F. Assessing the quality of media reporting of suicide news in India against World Health Organization guidelines: A content analysis study of nine major newspapers in Tamil Nadu. Aust. N. Z. J. Psychiatry 2018, 52, 856–863. [Google Scholar] [CrossRef]
- Armstrong, G.; Haregu, T.; Arya, V.; Vijayakumar, L.; Sinyor, M.; Niederkrotenthaler, T.; Spittal, M.J. Suicide-related Internet search queries in India following media reports of a celebrity suicide: An interrupted time series analysis. World Psychiatry 2021, 20, 143–144. [Google Scholar] [CrossRef]
- Armstrong, G.; Vijayakumar, L.; Pirkis, J.; Jayaseelan, M.; Cherian, A.; Soerensen, J.B.; Arya, V.; Niederkrotenthaler, T. Mass media representation of suicide in a high suicide state in India: An epidemiological comparison with suicide deaths in the population. BMJ Open 2019, 9, e030836. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organisation (WHO). Preventing Suicides: A Resource Guide for Media Professionals (2008). Available online: https://www.who.int/mental_health/prevention/suicide/resource_media.pdf (accessed on 30 March 2021).
- Preventing Suicide: A Resource for Media Professionals; World Health Organization: Geneva, Switzerland, 2017; (WHO/MSD/MER/17.5). Licence: CC BY-NC-SA 3.0 IGO.
- Preventing Suicide: A Technical Package of Policy, Programs, and Practices, Centre for Disease Control and Prevention. Available online: https://www.cdc.gov/violenceprevention/pdf/suicidetechnicalpackage.pdf (accessed on 30 March 2021).
- Samaritans Media Guidelines for Reporting Suicide. 2020. Available online: https://media.samaritans.org/documents/Media_Guidelines_FINAL.pdf (accessed on 7 June 2021).
- Press Council of India Guidelines for reporting on Mental Illness and Suicide. 2019. Available online: http://presscouncil.nic.in/WriteReadData/Pdf/PRtennineteentwenty.pdf (accessed on 30 March 2021).
- Mental Healthcare Act. 2017. Available online: http://egazette.nic.in/WriteReadData/2017/175248.pdf (accessed on 30 March 2021).
- Armstrong, G.; Vijayakumar, L.; Cherian, A.; Krishnaswamy, K.; Pathare, S. Indian media professionals’ perspectives regarding the role of media in suicide prevention and receptiveness to media guidelines: A qualitative study. BMJ Open 2021, 11, e047166. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, G.; Vijayakumar, L.; Cherian, A.V.; Krishnaswamy, K. “It’s a battle for eyeballs and suicide is clickbait”: The media experience of suicide reporting in India. PLoS ONE 2020, 15, e0239280. [Google Scholar] [CrossRef] [PubMed]
- Nutt, R.; Kidd, B.; Matthews, K. Assessing the Adherence to Guidelines of Media Reporting of Suicide Using a Novel Instrument—the “Risk of Imitative Suicide Scale” (RISc). Suicide Life-Threat. Behav. 2015, 45, 360–375. [Google Scholar] [CrossRef] [PubMed]
- John, A.; Hawton, K.; Gunnell, D.; Lloyd, K.; Scourfield, J.; Jones, P.A.; Luce, A.; Marchant, A.; Platt, S.; Price, S.; et al. Newspaper Reporting on a Cluster of Suicides in the UK. Crisis 2016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Indian Readership Survey. 2019. Available online: https://mruc.net/studies (accessed on 25 May 2020).

| No. | Positive Parameter | Description |
|---|---|---|
| 1 | Presence of help-seeking information | Provides information of national- or state-level support services that includes suicide prevention centers, emergency units in hospitals, 24/7 crisis helplines, self-help groups, mental health professionals, general physicians, community resources, rehabilitation centers. |
| 2 | Help-seeking information is up to date and operational | The information and contact details provided should be accurate and reliable. By operational we mean it should be relevant to where the article is published. This can be verified through a Google search. |
| 3 | Links to poor mental health | The report establishes a link between suicidal behavior and a mental illness, by making a clear reference to the individual’s struggle with a mental illness, its effect on their mental state. Inappropriate language such as “crazy” or “mental” is not accepted. Neither are mood qualifiers like “stressed”, “unhappy” etc. Acceptable terms that qualify include “depressed”, “anxious”, “panic”, “trauma”, “disturbed”, “distraught” or names of specific mental disorders. |
| 4 | Links to drug/ alcohol abuse | The report acknowledges the link between the suicide and substance and alcohol use. The report clearly refers to the person’s ongoing struggle with alcohol or drug addiction. A reference to the person’s intoxicated state at the time of suicide does not qualify. |
| 5 | Comments from mental health and suicide prevention experts | The article contains a quote or comment from a mental health professional or suicide prevention expert. |
| 6 | Reduces stigma highlights suicides are preventable | The article highlights that suicides are preventable by taking preventive measures and identifying risks in time and contains information that reduces stigma around talking about suicide and mental health concerns. |
| 7 | Credible population-level suicide statistics and/ or other research findings | The article reports on suicide-related statistical data. It may also provide findings from studies conducted on suicide and suicide prevention. |
| 8 | Challenges popular myths | The report challenges popular myths and reinforces their false nature. Examples of myths are (1) talking about suicide will lead to and encourage suicide; (2) people who talk about suicide do not mean to do it; (3) there are no preceding warning signs; and (4) there is nothing you can do to prevent suicide. |
| 9 | Links to hopeful stories | The report should have links to or snippets of reports that contain hopeful stories of people who have overcome suicidal thoughts and feelings. |
| 10 | Verified information and facts from official source | Information and facts are verified by official sources that include police officers, healthcare professionals or a government authority in the area. It has to be from a specific source if it simply says “sources”, that does not qualify. It could be likely that the information in the report is from an official source however, it may have not been acknowledged. It is important that reported information is corroborated, the absence of which may fuel speculation surrounding the story which in turn increases the likelihood of sensationalizing the report. |
| No. | Negative Parameter | Description |
|---|---|---|
| 1 | Use of criminalizing language | The article uses phrases that associate suicide with a crime or sin, e.g., ‘committed suicide’. |
| 2 | Attention-grabbing headlines | The headline includes the word ‘suicide’, the method or the reason for the suicide |
| 3 | Method of suicide or attempted suicide is mentioned in the article | The article mentions the method of suicide or attempted suicide. |
| 4 | Describes method in detail | The article provides at least two specific details about the suicide/ attempted suicide method. The detail may include objects used in the suicide or specific names of substance used e.g., kerosene, ‘celphos’ tablets. |
| 5 | Discloses details of the suicide site | The report provides enough information to clearly identify the location and it is somewhat accessible to at least some members of the public. |
| 6 | Reduces reason to a single factor or event | The article clearly articulates that the suicide incident had just one motive, cause or trigger. It over-simplifies the complex realities of suicide by reducing it to a single factor. The causal relationship is NOT subject to speculation. Speculation about the cause is indicated by phrases such as ‘the reason may be’, ‘some uncertainties about the cause remain’. |
| 7 | Accompanying photos | The report publishes photographs or video footage of the deceased, bereaved members, the location of the suicide and the method as well as other dramatic/ emotional images (e.g., a noose, slit wrists, person standing on the ledge, etc.). |
| 8 | Contains information on grieving persons | The article reports on the effects of a suicide on bereaved persons or contains interview with bereaved persons. Relatives, friends of the victim and other private persons involved in the suicidal act or affected by the suicide are defined as bereaved persons. |
| 9 | Publishes note or text | The report publishes suicide notes, text messages, social media posts and emails of the deceased person and/or their family members. |
| 10 | Article is on the front page of the newspaper | The article is published on the first page. This includes articles that commence on the first page and are then continued in later pages. |
| Newspaper Name | Positive Score | Negative Score |
|---|---|---|
| The Times of India | 1.12 (0.66) * | 3.37 (1.27) |
| Hindustan Times | 1.31 (0.69) | 3.28 (1.22) |
| The New Indian Express | 1.07 (0.91) | 3.42 (1.18) |
| The Telegraph | 1.03 (0.55) | 3.37 (1.31) |
| The Hindu | 2.71 (0.92) | 2.35 (1.15) |
| The Indian Express | 1.32 (0.68) | 3.32 (1.33) |
| Mirror | 1.32 (0.73) | 4.13 (1.35) |
| The Tribune | 1.00 (0.62) | 4.04 (0.98) |
| The Economic Times | 1.13 (0.83) | 3.25 (1.83) |
| Total | 1.32 (0.87) | 3.31 (1.31) |
| Positive Scoring Criteria | No. of Articles | |
|---|---|---|
| 1 | Verified information and facts from official source | 1084 (82.25%) |
| 2 | Links to poor mental health | 286 (21.70%) |
| 3 | Presence of help seeking information | 139 (10.55%) |
| 4 | Help-seeking information is up to date and operational | 139 (10.55%) |
| 5 | Links to drug/alcohol abuse | 61 (4.63%) |
| 6 | Comments from mental health and suicide prevention experts | 13 (0.99%) |
| 7 | Credible population-level suicide statistics | 6 (0.46%) |
| 8 | Reduces stigma highlights suicides are preventable | 4 (0.30%) |
| 9 | Challenges popular myths | 2 (0.15%) |
| 10 | Links to hopeful stories | 0 (0.00%) |
| Negative Scoring Criteria | No. of Articles | |
| 1 | Method of suicide or attempted suicide is mentioned in the article | 1140 (86.49%) |
| 2 | Attention-grabbing headlines | 992 (75.27%) |
| 3 | Use of criminalizing language | 859 (65.17%) |
| 4 | Reduces reason to a single factor or event | 541 (41.05%) |
| 5 | Discloses details of the suicide site | 228 (17.05%) |
| 6 | Describes method in detail | 194 (14.72%) |
| 7 | Accompanying photos | 148 (11.23%) |
| 8 | Contains information on grieving persons | 126 (9.56%) |
| 9 | Article is on the front page of the newspaper | 79 (5.99%) |
| 10 | Publishes note, text and social media post | 61 (4.63%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vijayakumar, L.; Shastri, M.; Fernandes, T.N.; Bagra, Y.; Pathare, A.; Patel, A.; Jain, P.; Merchant, Y.; Armstrong, G.; Pathare, S. Application of a Scorecard Tool for Assessing and Engaging Media on Responsible Reporting of Suicide-Related News in India. Int. J. Environ. Res. Public Health 2021, 18, 6206. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18126206
Vijayakumar L, Shastri M, Fernandes TN, Bagra Y, Pathare A, Patel A, Jain P, Merchant Y, Armstrong G, Pathare S. Application of a Scorecard Tool for Assessing and Engaging Media on Responsible Reporting of Suicide-Related News in India. International Journal of Environmental Research and Public Health. 2021; 18(12):6206. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18126206
Chicago/Turabian StyleVijayakumar, Lakshmi, Manisha Shastri, Tanya Nicole Fernandes, Yash Bagra, Aaryaman Pathare, Arpita Patel, Padam Jain, Yesha Merchant, Gregory Armstrong, and Soumitra Pathare. 2021. "Application of a Scorecard Tool for Assessing and Engaging Media on Responsible Reporting of Suicide-Related News in India" International Journal of Environmental Research and Public Health 18, no. 12: 6206. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18126206