
The ACTyourCHANGE in Teens Study Protocol: An Acceptance and Commitment Therapy-Based Intervention for Adolescents with Obesity: A Randomized Controlled Trial

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
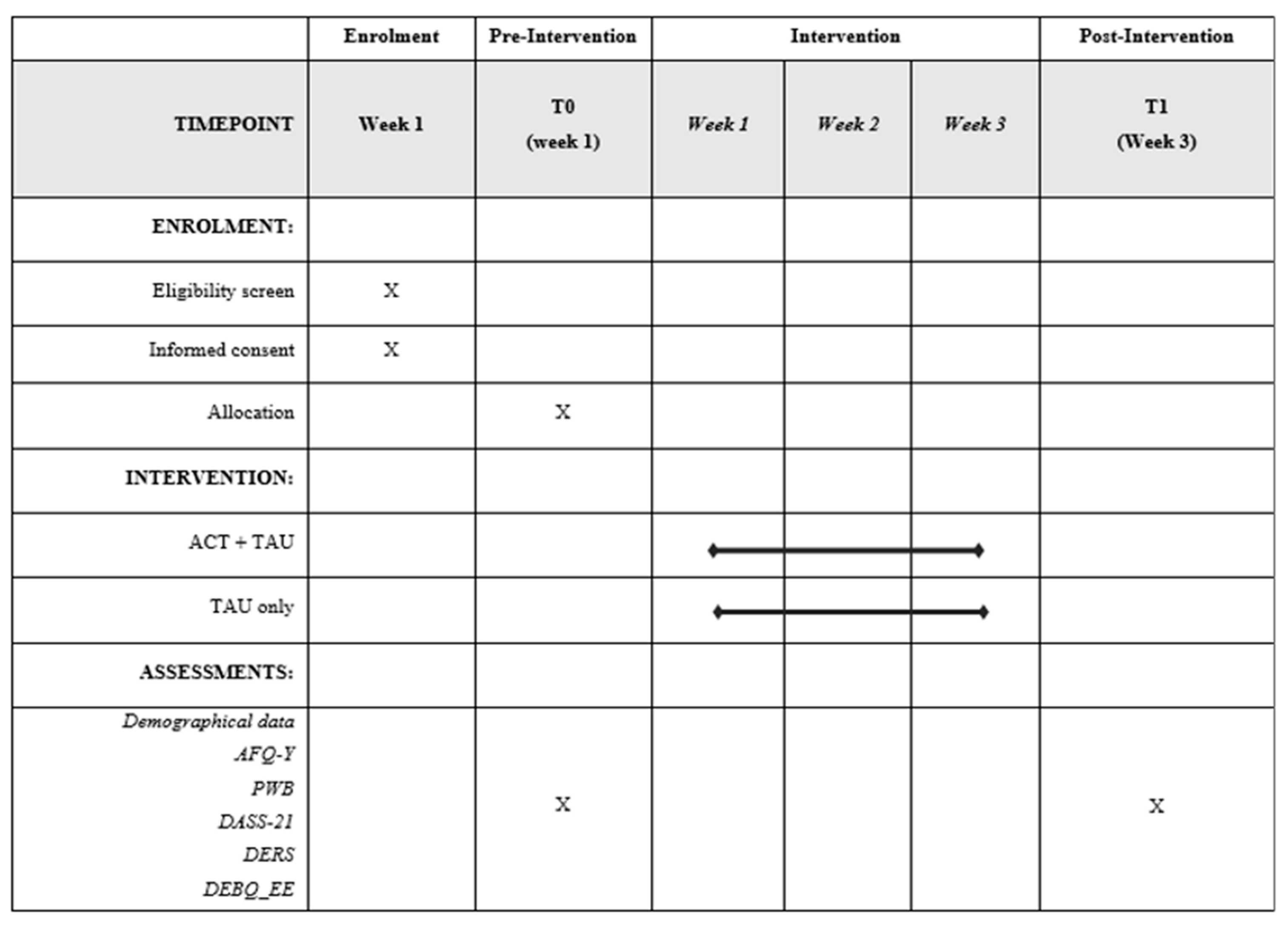
2.1. Study Design
2.2. Participants
2.3. Measures
2.3.1. Primary Outcomes
2.3.2. Secondary Outcomes
2.4. Randomization Procedure
2.5. Procedures
2.6. The ACT-Based Intervention
2.7. Treatment Fidelity
2.8. Sample Size Calculation
2.9. Statistical Analysis
3. Discussion
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bentham, J.; Di Cesare, M.; Bilano, V.; Bixby, H.; Zhou, B.; Stevens, G.A.; Riley, L.M.; Taddei, C.; Hajifathalian, K.; Lu, Y.; et al. Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: A pooled analysis of 2416 population-based measurement studies in 128·9 million children, adolescents, and adults. Lancet 2017, 390, 2627–2642. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization (WHO). Obesity and Overweight; WHO: Geneva, Switzerland, 2017; Available online: http://www.who.int/mediacentre/factsheets/fs311/en/ (accessed on 25 October 2017).
- Sagar, R.; Gupta, T. Psychological Aspects of Obesity in Children and Adolescents. Indian J. Pediatr. 2018, 85, 554–559. [Google Scholar] [CrossRef]
- Quek, Y.H.; Tam, W.W.S.; Zhang, M.W.B.; Ho, R.C.M. Exploring the association between childhood and adolescent obesity and depression: A meta-analysis. Obes. Rev. 2017, 18, 742–754. [Google Scholar] [CrossRef]
- Waring, M.E.; Lapane, K.L. Overweight in children and adolescents in relation to attention-deficit/ hyperactivity disorder: Results from a national sample. Pediatrics 2008, 122. [Google Scholar] [CrossRef]
- Morrison, K.M.; Shin, S.; Tarnopolsky, M.; Taylor, V.H. Association of depression & health related quality of life with body composition in children and youth with obesity. J. Affect. Disord. 2015, 172, 18–23. [Google Scholar] [CrossRef] [PubMed]
- Beck, A.R. Psychosocial Aspects of Obesity. NASN Sch. Nurse 2016, 31, 23–27. [Google Scholar] [CrossRef]
- Halfon, N.; Larson, K.; Slusser, W. Associations between obesity and comorbid mental health, developmental, and physical health conditions in a nationally representative sample of us children aged 10 to 17. Acad. Pediatr. 2013, 13, 6–13. [Google Scholar] [CrossRef]
- Rankin, J.; Matthews, L.; Cobley, S.; Han, A.; Sanders, R.; Wiltshire, H.D.; Baker, J.S. Psychological consequences of childhood obesity: Psychiatric comorbidity and prevention. Adolesc. Health Med. Ther. 2016, 7, 125–146. [Google Scholar] [CrossRef] [Green Version]
- Wang, F.; Veugelers, P.J. Self-esteem and cognitive development in the era of the childhood obesity epidemic. Obes. Rev. 2008, 9, 615–623. [Google Scholar] [CrossRef]
- Anderson, Y.C.; Wynter, L.E.; Treves, K.F.; Grant, C.C.; Stewart, J.M.; Cave, T.L.; Wouldes, T.A.; Derraik, J.G.B.; Cutfield, W.S.; Hofman, P.L. Assessment of health-related quality of life and psychological well-being of children and adolescents with obesity enrolled in a New Zealand community-based intervention programme: An observational study. BMJ Open 2017, 7, e015776. [Google Scholar] [CrossRef] [Green Version]
- Carter, F.A.; Jansen, A. Improving psychological treatment for obesity. Which eating behaviours should we target? Appetite 2012, 58, 1063–1069. [Google Scholar] [CrossRef]
- Giusti, E.M.; Spatola, C.; Brunani, A.; Kumbhare, D.; Oral, A.; Ilieva, E.; Kiekens, C.; Pietrabissa, G.; Manzoni, G.M.; Imamura, M.; et al. ISPRM/ESPRM Guidelines on Physical and Rehabilitation Medicine (PRM) professional practice for adults with obesity and related comorbidities. Eur. J. Phys. Rehabil. Med. 2020, 56, 496–507. [Google Scholar] [CrossRef]
- Keller, C.; Siegrist, M. Ambivalence toward palatable food and emotional eating predict weight fluctuations. Results of a longitudinal study with four waves. Appetite 2015, 85, 138–145. [Google Scholar] [CrossRef]
- Sainsbury, K.; Evans, E.H.; Pedersen, S.; Marques, M.M.; Teixeira, P.J.; Lähteenmäki, L.; Stubbs, R.J.; Heitmann, B.L.; Sniehotta, F.F. Attribution of weight regain to emotional reasons amongst European adults with overweight and obesity who regained weight following a weight loss attempt. Eat. Weight Disord. 2019, 24, 351–361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frayn, M.; Knäuper, B. Emotional Eating and Weight in Adults: A Review. Curr. Psychol. 2018, 37, 924–933. [Google Scholar] [CrossRef]
- Gratz, K.L.; Roemer, L. Multidimensional Assessment of Emotion Regulation and Dysregulation: Development, Factor Structure, and Initial Validation of the Difficulties in Emotion Regulation Scale. J. Psychopathol. Behav. Assess. 2004, 26, 41–54. [Google Scholar] [CrossRef]
- Van Strien, T.; Peter Herman, C.; Verheijden, M.W. Eating style, overeating and weight gain. A prospective 2-year follow-up study in a representative Dutch sample. Appetite 2012, 59, 782–789. [Google Scholar] [CrossRef]
- Braet, C.; Claus, L.; Goossens, L.; Moens, E.; Van Vlierberghe, L.; Soetens, B. Differences in eating style between overweight and normal-weight youngsters. J. Health Psychol. 2008, 13, 733–743. [Google Scholar] [CrossRef] [PubMed]
- Forman, E.; Butryn, M. A new look at the science of weight control: How acceptance and commitment strategies can address the challenge of self-regulation. Appetite 2015. [Google Scholar] [CrossRef] [Green Version]
- Hayes, S.C.; Luoma, J.B.; Bond, F.W.; Masuda, A.; Lillis, J. Acceptance and Commitment Therapy: Model, processes and outcomes. Behav. Res. Ther. 2006. [Google Scholar] [CrossRef] [Green Version]
- Kashdan, T.B.; Rottenberg, J. Psychological flexibility as a fundamental aspect of health. Clin. Psychol. Rev. 2010, 30, 865–878. [Google Scholar] [CrossRef] [Green Version]
- Lillis, J.; Niemeier, H.M.; Ross, K.M.; Graham Thomas, J.; Leahey, T.; Unick, J.; Kendra, K.E.; Wing, R.R. Weight loss intervention for individuals with high internal disinhibition: Design of the Acceptance Based Behavioral Intervention (ABBI) randomized controlled trial. BMC Psychol. 2015, 3, 17. [Google Scholar] [CrossRef] [Green Version]
- Hayes, S.C.; Strosahl, K.D.; Wilson, K.G. Acceptance and Commitment Therapy: The Process and Practice of Mindful Change, 2nd ed.; The Guilford Press: New York, NY, USA, 2012; ISBN 9781609189624/9781609189648. [Google Scholar]
- Casier, A.; Goubert, L.; Theunis, M.; Huse, D.; De Baets, F.; Matthys, D.; Crombez, G. Acceptance and well-being in adolescents and young adults with cystic fibrosis: A prospective study. J. Pediatr. Psychol. 2011, 36, 476–487. [Google Scholar] [CrossRef] [Green Version]
- Gauntlett-Gilbert, J.; Connell, H.; Clinch, J.; Mccracken, L.M. Acceptance and values-based treatment of adolescents with chronic pain: Outcomes and their relationship to acceptance. J. Pediatr. Psychol. 2013, 38, 72–81. [Google Scholar] [CrossRef] [Green Version]
- Murrell, A.R.; Kapadia, V. Brief report on experiential avoidance and valuing in at-risk adolescents. Behav. Dev. Bull. 2011, 17, 38–42. [Google Scholar] [CrossRef] [Green Version]
- Luciano, C.; Ruiz, F.J.; Torres, R.M.V.; Martín, V.S.; Martínez, O.G.; López, J.C.L. A relational frame analysis of defusion interactions in acceptance and commitment therapy. A preliminary and quasi-experimental study with at-risk adolescents. Int. J. Psychol. Psychol. Ther. 2011, 11, 165–182. [Google Scholar]
- Hayes, L.; Boyd, C.P.; Sewell, J. Acceptance and Commitment Therapy for the Treatment of Adolescent Depression: A Pilot Study in a Psychiatric Outpatient Setting. Mindfulness 2011, 2, 86–94. [Google Scholar] [CrossRef]
- Kemani, M.K.; Kanstrup, M.; Jordan, A.; Caes, L.; Gauntlett-Gilbert, J. Evaluation of an intensive interdisciplinary pain treatment based on acceptance and commitment therapy for adolescents with chronic pain and their parents: A nonrandomized clinical trial. J. Pediatr. Psychol. 2018, 43, 981–994. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Woidneck, M.R.; Morrison, K.L.; Twohig, M.P. Acceptance and Commitment Therapy for the Treatment of Posttraumatic Stress Among Adolescents. Behav. Modif. 2014, 38, 451–476. [Google Scholar] [CrossRef] [Green Version]
- Tronieri, J.S.; Wadden, T.A.; Leonard, S.M.; Berkowitz, R.I. A pilot study of acceptance-based behavioural weight loss for adolescents with obesity. Behav. Cogn. Psychother. 2019, 47, 686–696. [Google Scholar] [CrossRef] [PubMed]
- Tanner, J. Foetus into Man: Physical Growth from Conception to Maturity; Harvard University Press: Cambridge, UK, 1990. [Google Scholar]
- Cacciari, E.; Milani, S.; Balsamo, A.; Spada, E.; Bona, G.; Cavallo, L.; Cerutti, F.; Gargantini, L.; Greggio, N.; Tonini, G.; et al. Italian cross-sectional growth charts for height, weight and BMI (2 to 20 yr). J. Endocrinol. Investig. 2006, 29, 581–593. [Google Scholar] [CrossRef]
- Ryff, C.D. Happiness is everything, or is it? Explorations on the meaning of psychological well-being. J. Pers. Soc. Psychol. 1989, 57, 1069–1081. [Google Scholar] [CrossRef]
- Ruini, C.; Ottolini, F.; Rafanelli, C.; Ryff, C.; Fava, G.A. La validazione italiana delle Psychological Well-being Scales (PWB). Riv. Psichiatr. 2003, 38, 117–130. [Google Scholar]
- Sirigatti, S.; Stefanile, C.; Giannetti, E.; Iani, L.; Penzo, I.; Mazzeschi, A. Assessment of factor structure of Ryff’s Psychological Well-Being Scales in Italian adolescents. Boll. Psicol. Appl. 2009, 259, 30–50. [Google Scholar]
- Greco, L.A.; Lambert, W.; Baer, R.A. Psychological Inflexibility in Childhood and Adolescence: Development and Evaluation of the Avoidance and Fusion Questionnaire for Youth. Psychol. Assess. 2008, 20, 93–102. [Google Scholar] [CrossRef]
- Schweiger, M.; Ristallo, A.; Oppo, A.; Pergolizzi, F.; Presti, G.; Moderato, P. Ragazzi in lotta con emozioni e pensieri: La validazione della versione italiana dell’avoidance and fusion questionnaire for youth (I-AFQ-Y). Psicoter. Cogn. Comport. 2017, 23, 141–162. [Google Scholar]
- Lovibond, S.; Lovibond, P. Manual for the Depression Anxiety Stress Scales; Psychology Foundation of Australia: Sydney, Australia, 1996. [Google Scholar]
- Cosenza, M.; Ciccarelli, M.; Nigro, G. Decision-Making Styles, Negative Affectivity, and Cognitive Distortions in Adolescent Gambling. J. Gambl. Stud. 2019, 35, 517. [Google Scholar] [CrossRef]
- Nigro, G.; Cosenza, M.; Ciccarelli, M. The blurred future of adolescent gamblers: Impulsivity, time horizon, and emotional distress. Front. Psychol. 2017, 8, 486. [Google Scholar] [CrossRef] [Green Version]
- Bottesi, G.; Ghisi, M.; Altoè, G.; Conforti, E.; Melli, G.; Sica, C. The Italian version of the Depression Anxiety Stress Scales-21: Factor structure and psychometric properties on community and clinical samples. Compr. Psychiatry 2015, 60, 170–181. [Google Scholar] [CrossRef]
- Giromini, L.; Velotti, P.; De Campora, G.; Bonalume, L.; Cesare Zavattini, G. Cultural Adaptation of the Difficulties in Emotion Regulation Scale: Reliability and Validity of an Italian Version. J. Clin. Psychol. 2012, 68, 989–1007. [Google Scholar] [CrossRef] [Green Version]
- Somma, A.; Sharp, C.; Borroni, S.; Fossati, A. Borderline personality disorder features, emotion dysregulation and non-suicidal self-injury: Preliminary findings in a sample of community-dwelling Italian adolescents. Pers. Ment. Health 2017, 11, 23–32. [Google Scholar] [CrossRef] [PubMed]
- Fossati, A.; Gratz, K.L.; Maffei, C.; Borroni, S. Impulsivity dimensions, emotion dysregulation, and borderline personality disorder features among Italian nonclinical adolescents. Bord. Personal. Disord. Emot. Dysregul. 2014, 1, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Strien, T.; Frijters, J.E.R.; Bergers, G.P.A.; Defares, P.B. The Dutch Eating Behavior Questionnaire (DEBQ) for assessment of restrained, emotional, and external eating behavior. Int. J. Eat. Disord. 1986, 5, 295–315. [Google Scholar] [CrossRef]
- Dakanalis, A.; Zanetti, M.A.; Clerici, M.; Madeddu, F.; Riva, G.; Caccialanza, R. Italian version of the Dutch Eating Behavior Questionnaire. Psychometric proprieties and measurement invariance across sex, BMI-status and age. Appetite 2013, 71, 187–195. [Google Scholar] [CrossRef]
- Caccialanza, R.; Nicholls, D.; Cena, H.; Maccarini, L.; Rezzani, C.; Antonioli, L.; Dieli, S.; Roggi, C. Validation of the Dutch Eating Behaviour Questionnaire parent version (DEBQ-P) in the Italian population: A screening tool to detect differences in eating behaviour among obese, overweight and normal-weight preadolescents. Eur. J. Clin. Nutr. 2004, 58, 1217–1222. [Google Scholar] [CrossRef]
- Rigamonti, A.E.; Tringali, G.; De Micheli, R.; De Col, A.; Tamini, S.; Saezza, A.; Cella, S.G.; Sartorio, A. Impact of a three-week in-hospital multidisciplinary body weight reduction program on body composition, muscle performance and fatigue in a pediatric obese population with or without metabolic syndrome. Nutrients 2020, 12, 208. [Google Scholar] [CrossRef] [Green Version]
- Lazzer, S.; Bravo, G.; Tringali, G.; De Micheli, R.; De Col, A.; Sartorio, A. A 3-Week Multidisciplinary Body Weight Reduction Program Improves Body Composition and Lower Limb Power Output in 3,778 Severely Obese Children and Adolescents. Front. Physiol. 2020, 11, 548. [Google Scholar] [CrossRef]
- Pietrabissa, G.; Volpi, C.; Bottacchi, M.; Bertuzzi, V.; Guerrini Usubini, A.; Löffler-Stastka, H.; Prevendar, T.; Rapelli, G.; Cattivelli, R.; Castelnuovo, G.; et al. The impact of social isolation during the covid-19 pandemic on physical and mental health: The lived experience of adolescents with obesity and their caregivers. Int. J. Environ. Res. Public Health 2021, 18, 3026. [Google Scholar] [CrossRef]
- Nutrition ISO. Recommended Levels of Energy and Nutrients Intake for the Italian Population (LARN); Edra Medical Publishing and New Media: Milano, Italy, 1996. [Google Scholar]
- Halliburton, A.E.; Cooper, L.D. Applications and adaptations of Acceptance and Commitment Therapy (ACT) for adolescents. J. Context. Behav. Sci. 2015, 4, 1–11. [Google Scholar] [CrossRef]
- Turrell, S.L.; Bell, M. ACT for Adolescents: Treating Teens and Adolescents in Individual and Group Therapy; New Harbinger Publications: Oakland, CA, USA, 2016. [Google Scholar]
- Harris, R. ACT Made Simple; New Harbinger Publications: Oakland, CA, USA, 2009; pp. 9–13. [Google Scholar]
- Strosahl, K.; Robinson, P.; Gustavsson, T. Brief Interventions for Radical Change: Principles and Practice of Focused Acceptance and Commitment Therapy; New Harbinger Publications: Oakland, CA, USA, 2012; ISBN 9781608823451/9781608823475/9781608823468. [Google Scholar]
- Stoddard, J.A.; Afari, N. The Big Book of ACT Metaphors: A Practitioner’s Guide to Experiential Exercises and Metaphors in Acceptance and Commitment Therapy; New Harbinger Publications: Oakland, CA, USA, 2014. [Google Scholar]
- Villatte, J.L.; Vilardaga, R.; Villatte, M.; Plumb Vilardaga, J.C.; Atkins, D.C.; Hayes, S.C. Acceptance and Commitment Therapy modules: Differential impact on treatment processes and outcomes. Behav. Res. Ther. 2016, 77, 52–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cattivelli, R.; Castelnuovo, G.; Musetti, A.; Varallo, G.; Spatola, C.A.M.; Riboni, F.V.; Usubini, A.G.; Tosolin, F.; Manzoni, G.M.; Capodaglio, P.; et al. ACTonHEALTH study protocol: Promoting psychological flexibility with activity tracker and mHealth tools to foster healthful lifestyle for obesity and other chronic health conditions. Trials 2018, 19, 659. [Google Scholar] [CrossRef] [PubMed]
- Pietrabissa, G.; Castelnuovo, G.; Jackson, J.B.; Rossi, A.; Manzoni, G.M.; Gibson, P. Brief strategic therapy for bulimia nervosa and binge eating disorder: A clinical and research protocol. Front. Psychol. 2019, 10, 373. [Google Scholar] [CrossRef] [PubMed]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Associates, L.E., Ed.; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 1988. [Google Scholar]
- The Jamovi Project. Jamovi (Version 1.6) [Computer Software]. 2021. Available online: https://www.jamovi.org (accessed on 4 June 2021).
- Barlow, S.E. Expert committee recommendations regarding the prevention, assessment, and treatment of child and adolescent overweight and obesity: Summary report. Pediatrics 2007, 120 (Suppl. 4). [Google Scholar] [CrossRef] [Green Version]
- Sanyaolu, A.; Okorie, C.; Qi, X.; Locke, J.; Rehman, S. Childhood and Adolescent Obesity in the United States: A Public Health Concern. Glob. Pediatr. Health 2019, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aparicio, E.; Canals, J.; Arija, V.; De Henauw, S.; Michels, N. The role of emotion regulation in childhood obesity: Implications for prevention and treatment. Nutr. Res. Rev. 2016, 29, 17–29. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Session Number | Domains | Goals and Therapeutic Processes | Experiential Activities and Metaphors |
|---|---|---|---|
| Session 1 Week 1 | Openness | The purpose of this session is to develop the willingness to experiencing distress and undesirable private events as part of human experience, without judgment or attempts to avoid or control internal states, even if they are unpleasant. | Experiential exercise: “How would my life be if…” In this experiential activity, young patients are guided to answer the key question: “How would my life be if I didn’t have … [my problem that I have]”. The problem could be their weight or anything else related to their condition of obesity or any other perceived problem in their life. Participants are encouraged to describe what they desire to do if they did not have obesity, in order to take distance, observe and accept their conditions and related thoughts and feelings. |
| Session 2 Week 2 | Awareness | The purpose of this session is to promote the ability to be present at the moment and face events as contextually situated. To be aware means stepping back from suffering situations and seeing them in the context where they occur. | Metaphor: “The sky and weather metaphor” [58]. In this metaphor, personal thoughts and feelings are presented as the weather and the self as the sky. The weather naturally changes. Despite that, it can never harm or change the sky. No matter how bad the weather, the sky always has room for it. Sometimes, we forget that the sky is there, but it is still there. In the same way, difficult thoughts and feelings can occur. No matter how harmful they are, the self is still there. We can always learn how to access this part of us. It is a safe space that contains difficult thought and feelings. |
| Session 3 Week 3 | Engagement | The purpose of this session is to foster values clarification and engagement in actions linked to personal values, such as relationships and personal growth. If a person engages himself in committed actions driven by chosen life directions, they can pursue a meaningful and coherent life. | Experiential exercise: “The treasure hunt”. In this experiential exercise, young patients are asked to draw a treasure hunt in which the treasure is a value in their life and the route is made of behaviors that need to be engaged to reach a meaningful life. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guerrini Usubini, A.; Cattivelli, R.; Bertuzzi, V.; Varallo, G.; Rossi, A.A.; Volpi, C.; Bottacchi, M.; Tamini, S.; De Col, A.; Pietrabissa, G.; et al. The ACTyourCHANGE in Teens Study Protocol: An Acceptance and Commitment Therapy-Based Intervention for Adolescents with Obesity: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2021, 18, 6225. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18126225
Guerrini Usubini A, Cattivelli R, Bertuzzi V, Varallo G, Rossi AA, Volpi C, Bottacchi M, Tamini S, De Col A, Pietrabissa G, et al. The ACTyourCHANGE in Teens Study Protocol: An Acceptance and Commitment Therapy-Based Intervention for Adolescents with Obesity: A Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2021; 18(12):6225. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18126225
Chicago/Turabian StyleGuerrini Usubini, Anna, Roberto Cattivelli, Vanessa Bertuzzi, Giorgia Varallo, Alessandro Alberto Rossi, Clarissa Volpi, Michela Bottacchi, Sofia Tamini, Alessandra De Col, Giada Pietrabissa, and et al. 2021. "The ACTyourCHANGE in Teens Study Protocol: An Acceptance and Commitment Therapy-Based Intervention for Adolescents with Obesity: A Randomized Controlled Trial" International Journal of Environmental Research and Public Health 18, no. 12: 6225. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18126225