
Impact of Nutrition-Based Interventions on Athletic Performance during Menstrual Cycle Phases: A Review

Abstract
:1. Introduction
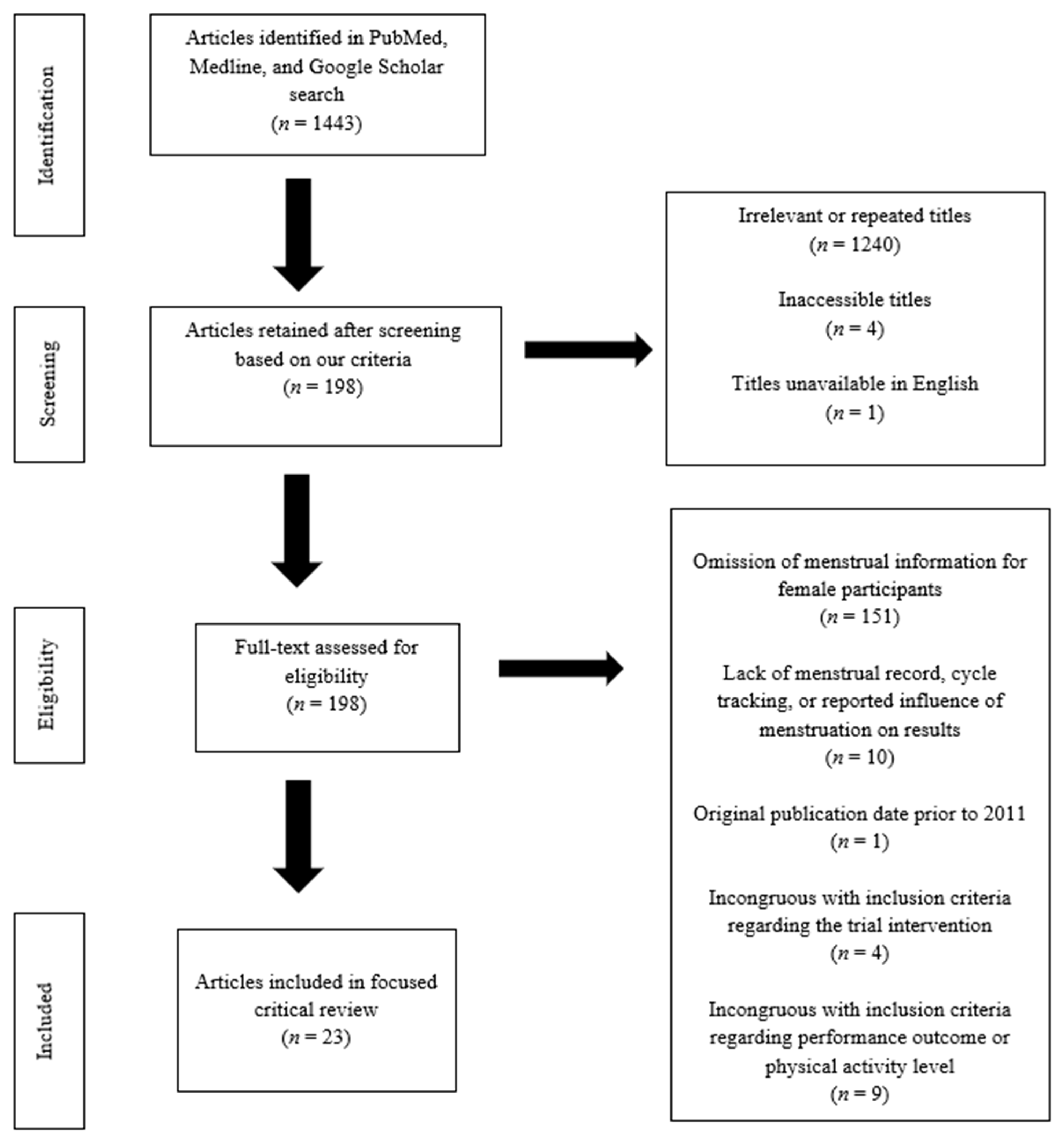
2. Materials and Methods
3. Results
3.1. Hydration Interventions
3.2. Micronutrient Interventions
3.3. Omega-3-Fatty Acids and Phytochemical-Based Dietary Supplement Interventions
4. Discussion
4.1. Hydration Interventions
4.2. Micronutrient Interventions
4.3. Omega-3-Fatty Acids and Phytochemical-Based Dietary Supplement Interventions
4.4. Strengths and Limitations
4.5. Future Directions
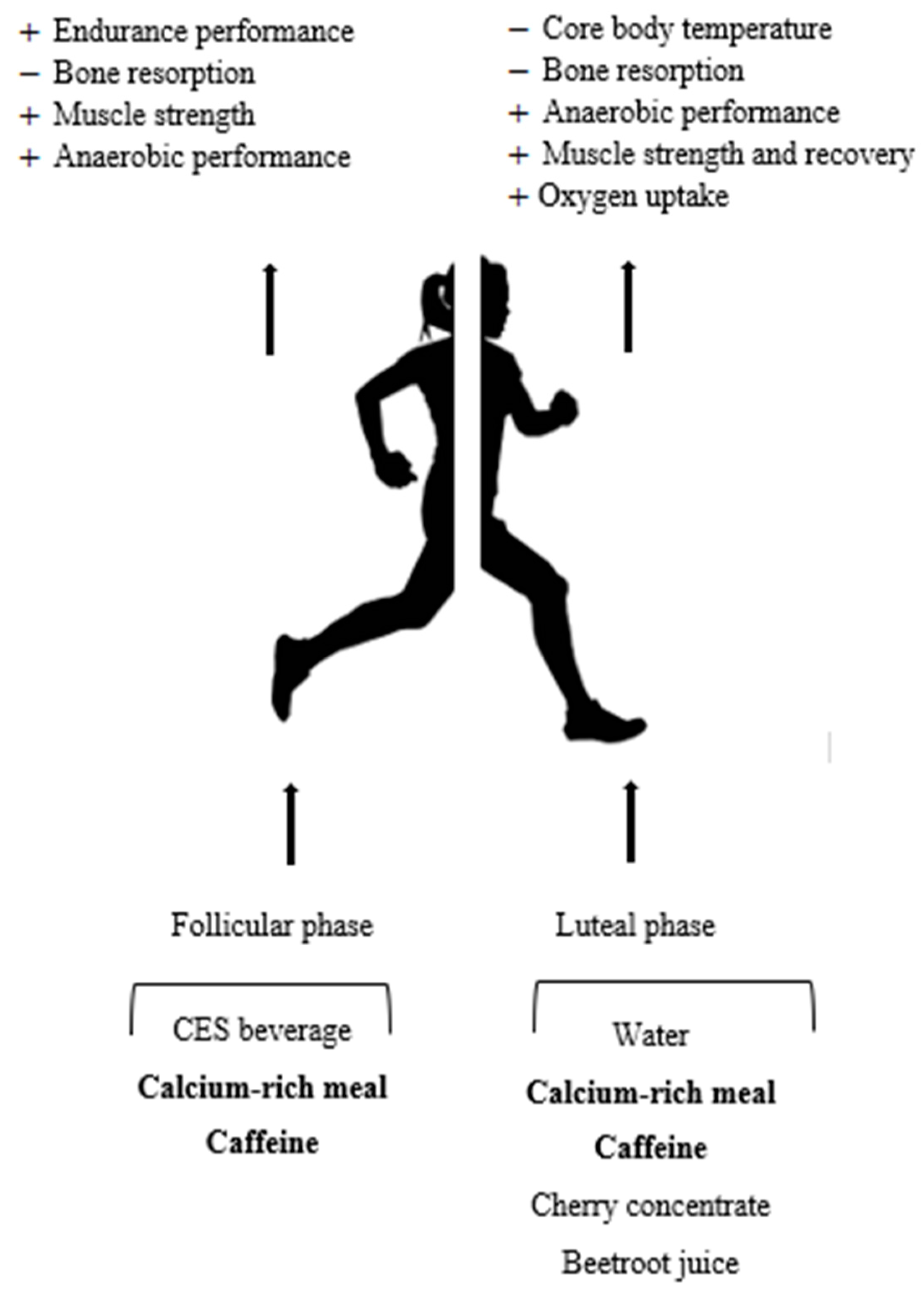
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Fink, J.S. Female athletes, women’s sport, and the sport media commercial complex: Have we really ‘come a long way, baby’? Sport Manag. Rev. 2015, 18, 331–342. [Google Scholar] [CrossRef]
- Smith, M.; Wrynn, A. Women in the Olympic and Paralympic Games. 2013. Available online: http://sharp.research.umich.edu/wp-content/uploads/2017/03/olympic_report_2012_final-4-11-13.pdf (accessed on 21 February 2021).
- Freemas, J.A.; Baranauskas, M.N.; Constantini, K.; Constantini, N.; Greenshields, J.T.; Mickleborough, T.D.; Raglin, J.S.; Schlader, Z.J. Exercise Performance Is Impaired during the Mid-Luteal Phase of the Menstrual Cycle. Med. Sci. Sports Exerc. 2020, 3, 442–452. [Google Scholar] [CrossRef] [PubMed]
- Lebrun, C.M.; McKenzie, D.C.; Prior, J.C.; Taunton, J.E. Effects of menstrual cycle phase on athletic performance. Med. Sci. Sports Exerc. 1995, 27, 437–444. [Google Scholar] [CrossRef]
- Oosthuyse, T.; Bosch, A.N. The effect of the menstrual cycle on exercise metabolism: Implications for exercise performance in eumenorrhoeic women. Sports Med. 2010, 40, 207–227. [Google Scholar] [CrossRef] [PubMed]
- Giersch, G.E.W.; Charkoudian, N.; Stearns, R.L.; Casa, D.J. Fluid Balance and Hydration Considerations for Women: Review and Future Directions. Sports Med. 2020, 50, 253–261. [Google Scholar] [CrossRef]
- De Jonge, X.A.K.J. Effects of the menstrual cycle on exercise performance. Sports Med. 2003, 33, 833–851. [Google Scholar] [CrossRef] [PubMed]
- Bruinvels, G.; Burden, R.J.; McGregor, A.J.; Ackerman, K.E.; Dooley, M.; Richards, T.; Pedlar, C. Sport, exercise and the menstrual cycle: Where is the research? Br. J. Sports Med. 2017, 51, 487–488. [Google Scholar] [CrossRef] [PubMed]
- Giersch, G.E.; Morrissey, M.C.; Katch, R.K.; Colburn, A.T.; Sims, S.T.; Stachenfeld, N.S.; Casa, D.J. Menstrual cycle and thermoregulation during exercise in the heat: A systematic review and meta-analysis. J. Sci. Med. Sport 2020, 23, 1134–1140. [Google Scholar] [CrossRef] [PubMed]
- Aguree, S.; Bethancourt, H.J.; Taylor, L.A.; Rosinger, A.Y.; Gernand, A.D. Plasma volume variation across the menstrual cycle among healthy women of reproductive age: A prospective cohort study. Physiol. Rep. 2020, 8, e14418. [Google Scholar] [CrossRef]
- Wenner, M.M.; Stachenfeld, N.S. Blood pressure and water regulation: Understanding sex hormone effects within and between men and women. J. Physiol. 2012, 590, 5949–5961. [Google Scholar] [CrossRef] [Green Version]
- Sawka, M.N.; Burke, L.M.; Eichner, E.R.; Maughan, R.J.; Montain, S.J.; Stachenfeld, N.S. Exercise and fluid replacement. Med. Sci. Sports Exerc. 2007, 39, 377–390. [Google Scholar] [CrossRef] [Green Version]
- MacLeod, H.; Sunderland, C. Previous-day hypohydration impairs skill performance in elite female field hockey players. Scand. J. Med. Sci. Sport 2012, 22, 430–438. [Google Scholar] [CrossRef] [PubMed]
- Garcia, A.M.C.; Lacerda, M.G.; Fonseca, I.A.T.; Reis, F.M.; Rodrigues, L.O.C.; Silami-Garcia, E. Luteal phase of the menstrual cycle increases sweating rate during exercise. Brazilian J. Med. Biol. Res. 2006, 39, 1255–1261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, I.; Yetley, E.A.; Calvo, M.S. Variations menstrual during the menstrual cycle. Am. J. Clin. Nutr. 1993, 58, 705–709. [Google Scholar] [CrossRef] [PubMed]
- Woods, A.; Garvican-Lewis, L.A.; Saunders, P.U.; Lovell, G.; Hughes, D.; Fazakerley, R.; Anderson, B.; Gore, C.J.; Thompson, K.G. Four weeks of iv iron supplementation reduces perceived fatigue and mood disturbance in distance runners. PLoS ONE 2014, 9. [Google Scholar] [CrossRef] [PubMed]
- Vaucher, P.; Druais, P.L.; Waldvogel, S.; Favrat, B. Effect of iron supplementation on fatigue in nonanemic menstruating women with low ferritin: A randomized controlled trial. CMAJ 2012, 184, 1247–1254. [Google Scholar] [CrossRef] [Green Version]
- Brown, D.M.Y.; Graham, J.D.; Innes, K.I.; Harris, S.; Flemington, A.; Bray, S.R. Effects of Prior Cognitive Exertion on Physical Performance: A Systematic Review and Meta-Analysis; Springer International Publishing: Berlin/Heidelberg, Germany, 2020; Volume 50. [Google Scholar]
- Peinado, A.; Alfaro-Magallanes, V.; Romero-Parra, N.; Barba-Moreno, L.; Rael, B.; Maestre-Cascales, C.; Rojo-Tirado, M.; Castro, E.; Benito, P.; Ortega-Santos, C.; et al. Methodological Approach of the Iron and Muscular Damage: Female Metabolism and Menstrual Cycle during Exercise Project (IronFEMME Study). Int. J. Environ. Res. Public Health 2021, 18, 735. [Google Scholar] [CrossRef]
- Papageorgiou, M.; Elliott-Sale, K.J.; Parsons, A.; Tang, J.C.; Greeves, J.P.; Fraser, W.D.; Sale, C. Effects of reduced energy availability on bone metabolism in women and men. Bone 2017, 105, 191–199. [Google Scholar] [CrossRef] [Green Version]
- Levers, K.; Dalton, R.; Galvan, E.; O’Connor, A.; Goodenough, C.; Simbo, S.; Mertens-Talcott, S.U.; Rasmussen, C.; Greenwood, M.; Riechman, S.; et al. Effects of powdered Montmorency tart cherry supplementation on acute endurance exercise performance in aerobically trained individuals. J. Int. Soc. Sports Nutr. 2016, 13, 22. [Google Scholar] [CrossRef] [Green Version]
- García-Flores, L.A.; Medina, S.; Cejuela-Anta, R.; Martínez-Sanz, J.M.; Abellán, Á.; Genieser, H.G.; Ferreres, F.; Gil-Izquierdo, Á. DNA catabolites in triathletes: Effects of supplementation with an aronia-citrus juice (polyphenols-rich juice). Food Funct. 2016, 7, 2084–2093. [Google Scholar] [CrossRef] [Green Version]
- McAnulty, S.R.; Nieman, D.C.; McAnulty, L.S.; Lynch, W.S.; Jin, F.; Henson, D.A. Effect of mixed flavonoids, n-3 fatty acids, and vitamin C on oxidative stress and antioxidant capacity before and after intense cycling. Int. J. Sport Nutr. Exerc. Metab. 2011, 21, 328–337. [Google Scholar] [CrossRef] [PubMed]
- Mestre-Alfaro, A.; Ferrer, M.D.; Sureda, A.; Tauler, P.; Martínez, E.; Bibiloni, M.M.; Micol, V.; Tur, J.A.; Pons, A. Phytoestrogens enhance antioxidant enzymes after swimming exercise and modulate sex hormone plasma levels in female swimmers. Eur. J. Appl. Physiol. 2011, 111, 2281–2294. [Google Scholar] [CrossRef]
- Martin-Rincon, M.; Gelabert-Rebato, M.; Galvan-Alvarez, V.; Gallego-Selles, A.; Martinez-Canton, M.; Lopez-Rios, L.; Wiebe, J.C.; Martin-Rodriguez, S.; Arteaga-Ortiz, R.; Dorado, C.; et al. Supplementation with a mango leaf extract (Zynamite ®) in combination with quercetin attenuated muscle damage and pain and accelerates recovery after strenuous damaging exercise. Nutrients. 2020, 12, 614. [Google Scholar] [CrossRef] [Green Version]
- Toscano, L.T.; Tavares, R.L.; Toscano, L.T.; Da Silva, C.S.O.; De Almeida, A.E.M.; Biasoto, A.; Gonçalves, M.D.C.R.; Silva, A.S. Potential ergogenic activity of grape juice in runners. Appl. Physiol. Nutr. Metab. 2015, 40, 899–906. [Google Scholar] [CrossRef] [Green Version]
- Trexler, E.T.; Smith-Ryan, A.E.; Melvin, M.N.; Roelofs, E.J.; Wingfield, H.L. The effects of pomegranate extract on blood flow and running time to exhaustion. Appl. Physiol. Nutr. Metab. 2014, 39, 1038–1042. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodriguez-Giustiniani, P.; Galloway, S.D. Influence of Peak Menstrual Cycle Hormonal Changes on Restoration of Fluid Balance After Induced Dehydration. Int. J. Sport Nutr. Exerc. Metab. 2019, 29, 651–657. [Google Scholar] [CrossRef] [PubMed]
- Harris, P.R.; Keen, D.A.; Constantopoulos, E.; Weninger, S.N.; Hines, E.; Koppinger, M.P.; Khalpey, Z.I.; Konhilas, J.P. Fluid type influences acute hydration and muscle performance recovery in human subjects. J. Int. Soc. Sports Nutr. 2019, 16, 15. [Google Scholar] [CrossRef] [Green Version]
- Miller, K.C. Electrolyte and Plasma Responses After Pickle Juice, Mustard, and Deionized Water Ingestion in Dehydrated Humans. J. Athl. Train. 2014, 49, 360–367. [Google Scholar] [CrossRef] [Green Version]
- Chryssanthopoulos, C.; Ziaras, C.; Oosthuyse, T.; Lambropoulos, I.; Giorgios, P.P.; Zacharogiannis, E.; Philippou, A.; Maridaki, M. Carbohydrate mouth rinse does not affect performance during a 60-min running race in women. J. Sports Sci. 2017, 36, 824–833. [Google Scholar] [CrossRef]
- Konishi, K.; Kimura, T.; Yuhaku, A.; Kurihara, T.; Fujimoto, M.; Hamaoka, T.; Sanada, K. Mouth rinsing with a carbohydrate solution attenuates exercise-induced decline in executive function. J. Int. Soc. Sports Nutr. 2017, 14, 45. [Google Scholar] [CrossRef] [Green Version]
- Gui, Z.; Sun, F.; Si, G.; Chen, Y. Effect of protein and carbohydrate solutions on running performance and cognitive function in female recreational runners. PLoS ONE 2017, 12, e0185982. [Google Scholar] [CrossRef] [Green Version]
- Sun, F.-H.; Wong, S.H.-S.; Chen, S.-H.; Poon, T.-C. Carbohydrate electrolyte solutions enhance endurance capacity in active females. Nutrients 2015, 7, 3739–3750. [Google Scholar] [CrossRef] [Green Version]
- Ramos-Jiménez, A.; Hernández-Torres, R.P.; Wall-Medrano, A.; Torres-Durán, P.V.; Juárez-Oropeza, M.A.; Viloria, M.; Villalobos-Molina, R. Respuestas fisiológicas asociadas al género e hidratación durante el spinning. Nutr. Hosp. 2014, 29, 644–651. [Google Scholar] [CrossRef] [PubMed]
- Logan-Sprenger, H.M.; Spriet, L.L. The Acute Effects of Fluid Intake on Urine Specific Gravity and Fluid Retention in a Mildly Dehydrate State. J. Strength Cond. Res. 2013, 27, 1002–1008. [Google Scholar] [CrossRef]
- West, J.S.; Ayton, T.; Wallman, K.E.; Guelfi, K.J. The effect of 6 days of sodium phosphate supplementation on appetite, energy intake, and aerobic capacity in trained men and women. Int. J. Sport Nutr. Exerc. Metab. 2012, 22, 422–429. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ali, A.; Gardiner, R.; Foskett, A.; Gant, N. Fluid balance, thermoregulation and sprint and passing skill performance in female soccer players. Scand. J. Med. Sci. Sports 2011, 21, 437–445. [Google Scholar] [CrossRef] [PubMed]
- Haakonssen, E.C.; Ross, M.L.; Knight, E.J.; Cato, L.E.; Nana, A.; Wluka, A.; Cicuttini, F.M.; Wang, B.H.; Jenkins, D.G.; Burke, L.M. The effects of a calcium-rich pre-exercise meal on biomarkers of calcium homeostasis in competitive female cyclists a randomised crossover trial. PLoS ONE 2015, 10, e0123302. [Google Scholar] [CrossRef] [Green Version]
- Dellavalle, D.M.; Haas, J.D. Iron supplementation improves energetic efficiency in iron-depleted female rowers. Med. Sci. Sports Exerc. 2014, 46, 1204–1215. [Google Scholar] [CrossRef]
- McKinley-Barnard, S.K.; Andre, T.L.; Gann, J.J.; Hwang, P.S.; Willoughby, D.S. Effectiveness of fish oil supplementation in attenuating exercise-induced muscle damage in women during midfollicular and midluteal menstrual phases. J. Strength Cond. Res. 2018, 32, 1601–1612. [Google Scholar] [CrossRef]
- Hiles, A.M.; Flood, T.R.; Lee, B.J.; Wheeler, L.E.; Costello, R.; Walker, E.F.; Ashdown, K.M.; Kuennen, M.R.; Willems, M.E. Dietary supplementation with New Zealand blackcurrant extract enhances fat oxidation during submaximal exercise in the heat. J. Sci. Med. Sport 2020, 23, 908–912. [Google Scholar] [CrossRef]
- Lara, B.; Hellín, J.G.; Ruíz-Moreno, C.; Romero-Moraleda, B.; del Coso, J. Acute caffeine intake increases performance in the 15-s Wingate test during the menstrual cycle. Br. J. Clin. Pharmacol. 2020, 86, 745–752. [Google Scholar] [CrossRef] [Green Version]
- Romero-Moraleda, B.; del Coso, J.; Gutiérrez-Hellín, J.; Lara, B. The effect of caffeine on the velocity of half-squat exercise during the menstrual cycle: A randomized controlled trial. Nutrients 2019, 11, 2662. [Google Scholar] [CrossRef] [Green Version]
- Brown, M.A.; Stevenson, E.J.; Howatson, G. Montmorency tart cherry (Prunus cerasus L.) supplementation accelerates recovery from exercise-induced muscle damage in females. Eur. J. Sport Sci. 2019, 19, 95–102. [Google Scholar] [CrossRef] [PubMed]
- Gutiérrez-Hellín, J.; del Coso, J. Effects of p -Synephrine and Caffeine Ingestion on Substrate Oxidation during Exercise. Med. Sci. Sports Exerc. 2018, 50, 1899–1906. [Google Scholar] [CrossRef]
- Strauss, J.A.; Willems, M.E.T.; Shepherd, S.O. New Zealand blackcurrant extract enhances fat oxidation during prolonged cycling in endurance-trained females. Eur. J. Appl. Physiol. 2018, 118, 1265–1272. [Google Scholar] [CrossRef] [Green Version]
- Buck, C.; Guelfi, K.; Dawson, B.; McNaughton, L.; Wallman, K. Effects of sodium phosphate and caffeine loading on repeated-sprint ability. J. Sports Sci. 2015, 33, 1971–1979. [Google Scholar] [CrossRef] [PubMed]
- Buck, C.L.; Henry, T.; Guelfi, K.; Dawson, B.; McNaughton, L.R.; Wallman, K. Effects of sodium phosphate and beetroot juice supplementation on repeated-sprint ability in females. Eur. J. Appl. Physiol. 2015, 115, 2205–2213. [Google Scholar] [CrossRef]
- Braakhuis, A.J.; Hopkins, W.G.; Lowe, T.E. Effects of dietary antioxidants on training and performance in female runners. Eur. J. Sport Sci. 2014, 14, 160–168. [Google Scholar] [CrossRef]
- Wiecek, M.; Szymura, J.; Maciejczyk, M.; Cempla, J.; Szygula, Z. Effect of sex and menstrual cycle in women on starting speed, anaerobic endurance and muscle power. Acta Physiol. Hung. 2016, 103, 127–132. [Google Scholar] [CrossRef] [Green Version]
- Brener, W.; Hendrix, T.R.; McHugh, P.R. Regulation of the Gastric Emptying of Glucose. Gastroenterology 1983, 85, 76–82. [Google Scholar] [CrossRef]
- Billich, C.O.; Levitan, R. Effects of sodium concentration and osmolality on water and electrolyte absorption form the intact human colon. J. Clin. Investig. 1969, 48, 1336–1347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamilton, M.T.; Gonzalez-Alonso, J.; Montain, S.J.; Coyle, E.F. Fluid replacement and glucose infusion during exercise prevent cardiovascular drift. J. Appl. Physiol. 1991, 71, 871–877. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caballero-Plasencia, A.M.; Valenzuela-Barranco, M.; Martín-Ruiz, J.L.; Herrerías-Gutiérrez, J.M.; Esteban-Carretero, J.M. Are there changes in gastric emptying during the menstrual cycle? Scand. J. Gastroenterol. 1999, 34, 772–776. [Google Scholar] [CrossRef]
- Zhou, Z.; Bian, C.; Luo, Z.; Guille, C.; Ogunrinde, E.; Wu, J.; Zhao, M.; Fitting, S.; Kamen, D.L.; Oates, J.C.; et al. Progesterone decreases gut permeability through upregulating occludin expression in primary human gut tissues and Caco-2 cells. Sci. Rep. 2019, 9, 8367. [Google Scholar] [CrossRef] [Green Version]
- Stone, T.; Earley, R.L.; Burnash, S.G.; Wingo, J.E. Menstrual cycle effects on cardiovascular drift and maximal oxygen uptake during exercise heat stress. Eur. J. Appl. Physiol. 2021, 121, 561–572. [Google Scholar] [CrossRef]
- Stoffel, N.U.; von Siebenthal, H.K.; Moretti, D.; Zimmermann, M.B. Oral iron supplementation in iron-deficient women: How much and how often? Mol. Aspects Med. 2020, 75, 100865. [Google Scholar] [CrossRef]
- Trumbo, P.; Yates, A.A.; Schlicker, S.; Poos, M. Dietary reference intakes: Vitamin A, vitamin K, arsenic, boron, chromium, copper, iodine, iron, manganese, molybdenum, nickel, silicon, vanadium, and zinc. J. Am. Diet. Assoc. 2001, 101, 294–301. [Google Scholar] [CrossRef]
- Davies, K.J.A.; Maguire, J.J.; Brooks, G.A. Muscle mitochondrial bioenergetics, oxygen supply, and work capacity during dietary iron deficiency and repletion. Am. J. Physiol. Endocrinol. Metab. 1982, 5. [Google Scholar] [CrossRef]
- Keller, M.F.; Harrison, M.L.; Lalande, S. Impact of Menstrual Blood Loss and Oral Contraceptive Use on Oxygen-carrying Capacity. Med. Sci. Sports Exerc. 2020, 52, 1414–1419. [Google Scholar] [CrossRef]
- Institute of Medicine (US). Committee to Review Dietary Reference Intakes for Vitamin D and Calcium; Ross, A., Taylor, C., Yaktine, A., Eds.; National Academy Press: Washington, DC, USA, 2011; p. 5. [Google Scholar]
- Gardinier, J.D.; Mohamed, F.; Kohn, D.H. PTH signaling during exercise contributes to bone adaptation. J. Bone Miner. Res. 2015, 30, 1053–1063. [Google Scholar] [CrossRef] [Green Version]
- Raisz, L.G. Bone Resorption in Tissue Culture. Factors Influencing the Response To Parathyroid Hormone. J. Clin. Investig. 1965, 44, 103–116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fox, J.; Miller, M.A.; Stroup, G.B.; Nemeth, E.F.; Miller, S.C. Plasma levels of parathyroid hormone that induce anabolic effects in bone of ovariectomized rats can be achieved by stimulation of endogenous hormone secretion. Bone 1997, 21, 163–169. [Google Scholar] [CrossRef]
- Chiu, K.M.; Ju, J.; Mayes, D.; Bacchetti, P.; Weitz, S.; Arnaud, C.D. Changes in bone resorption during the menstrual cycle. J. Bone Miner. Res. 1999, 14, 609–615. [Google Scholar] [CrossRef]
- Kuo, I.Y.; Ehrlich, B.E. Signaling in muscle contraction. Cold Spring Harb. Perspect. Biol. 2015, 7. [Google Scholar] [CrossRef]
- Weber, A.; Herz, R. The relationship between caffeine contracture of intact muscle and the effect of caffeine on reticulum. J. Gen. Physiol. 1968, 52, 750–759. [Google Scholar] [CrossRef] [Green Version]
- Allen, D.G.; Westerblad, H. The effects of caffeine on intracellular calcium, force and the rate of relaxation of mouse skeletal muscle. J. Physiol. 1995, 487, 331–342. [Google Scholar] [CrossRef]
- Kotsopoulos, J.; Eliassen, A.H.; Missmer, S.A.; Hankinson, S.E.; Tworoger, S.S. Relationship between caffeine intake and plasma sex hormone concentrations in premenopausal and postmenopausal women. Cancer 2009, 115, 2765–2774. [Google Scholar] [CrossRef] [Green Version]
- Tsuda, T.; Ueno, Y.; Kojo, H.; Yoshikawa, T.; Osawa, T. Gene expression profile of isolated rat adipocytes treated with anthocyanins. Biochim. Biophys. Acta Mol. Cell Biol. Lipids 2005, 1733, 137–147. [Google Scholar] [CrossRef]
- Ignarro, L.J.; Lippton, H.; Edwards, J.C.; Baricos, W.H.; Hyman, A.L.; Kadowitz, P.J.; Gruetter, C.A. Mechanism of vascular smooth muscle relaxation by organic nitrates, nitrites, nitroprusside and nitric oxide: Evidence for the involvement of S-Nitrosothiols as active intermediates. J. Pharmacol. Exp. Ther. 1981, 218, 739–749. [Google Scholar]
- Mason, D.T. Afterload reduction and cardiac performance. Am. J. Med. 1978, 65, 106–125. [Google Scholar] [CrossRef]
- Hashimoto, M.; Akishita, M.; Eto, M.; Ishikawa, M.; Kozaki, K.; Toba, K.; Sagara, Y.; Taketani, Y.; Orimo, H.; Ouchi, Y. Modulation of Endoethelium-Dependent Flow-Mediated Dilation of the BRachial Artery by Sex and Menstrual Cycle. Circulation 1995, 92, 3431–3435. [Google Scholar] [CrossRef]
- Zhang, Z.; Fulgoni, V.L.; Kris-Etherton, P.M.; Mitmesser, S.H. Dietary intakes of EPA and DHA omega-3 fatty acids among US childbearing-age and pregnant women: An analysis of NHANES 2001–2014. Nutrients 2018, 10, 416. [Google Scholar] [CrossRef] [Green Version]
- Gray, P.; Chappell, A.; Jenkinson, A.M.E.; Thies, F.; Gray, S.R. Fish oil supplementation reduces markers of oxidative stress but not muscle soreness after eccentric exercise. Int. J. Sport Nutr. Exerc. Metab. 2014, 24, 206–214. [Google Scholar] [CrossRef] [Green Version]
- Carter, A.; Dodbridge, J.; Hackney, A.C. Influence of Estrogen on Markers of Muscle Tissue Damage Following Eccentric Exercise. Hum. Physiol. 2001, 27, 626–630. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Authors, Year (Country) | Study Design | Participants | Menstrual Cycle Reported | Nutrition-Based Intervention and Duration | Assessment of Athletic Outcome |
|---|---|---|---|---|---|
| Rodriguez-Giustiniani and Galloway, 2019 (United Kingdom) [28] | Crossover study | Women (n = 10) Age: 25 ± 7 years | LFP: between days 10 and 13 MLP: between days 18 and 23 | 100% body mass loss volume: 6.4% CHO, 25 mM Na+, 3.5 mM K+ beverage Consumed in four equal phases over 30 min | ↑ Fluid retention in LFP (trivial effect) ∅ Menstrual phase on degree of dehydration, urine volume, net fluid balance, electrolyte balance, urine osmolality, thirst intensity |
| Harris et al., 2019 (United States) [29] | Randomized counterbalanced crossover study | Women (n = 8) Age: 21 ± 2 years | Early in cycle | 100% body mass loss volume: Deep-ocean mineral water 59.2 g/L CHO, 450.9 mg/L Na+, 408.3 mg/L Cl−, 126.8 mg/L K+ beverage Spring water Consumed in two phases 30 min apart | Rehydrating with deep-ocean mineral water: ↑ Peak torque ↓ Salivary osmolality |
| Chryssanthopoulos et al., 2018 (Greece) [31] | Double-blind placebo-controlled RCT | Women (n = 15) Age: 43 ± 2 years | FP: between days 3 and 10 | 25 mL 6.4% CHO beverage Rinsed in mouth for 5 s prior to exercise and at minute 15, 30, and 45 | ∅ Distance traveled, HR, fluid loss |
| Konishi et al., 2017 (Japan) [32] | Single-blind RCT | Women (n = 4) Age: 24 ± 2 years | FP | 25 mL 6.4% maltodextrin solution Rinsed in mouth for 5 s prior to exercise | ↓ Reaction time, RPE plasma E and NE ∅ Executive function accuracy, plasma ACTH |
| Gui et al., 2017 (Hong Kong) [33] | Randomized, placebo-controlled crossover study | Women (n = 11) Age: 32 ± 7 years | Within 10 days after menses ended | 150 mL 6% CES or 150 mL 4% CHO + 2% PRO CES-P Consumed every 2.5 km for 21 km run | CES: ↓ 21 km time CES-P: ∅ 21 km time CES and CES-P: ∅ USG, RPE, cognitive reaction time |
| Sun et al., 2015 (China) [34] | Double-blind placebo-controlled RCT | Women (n = 8) Age: 28 ± 2 years | FP | 3 mL·kg−1 body mass 6% CES Consumed every 20 min until exhaustion | ↑ Exercise time to exhaustion, plasma glucose from 15 min mark ∅ RER, blood glucose, lactate levels, HR, RPE, PTS, PAS |
| Miller, 2014 (United States) [30] | Randomized, crossover study | Women (n = 6) Age: 25 ± 2 years | FP | 1 mL·kg−1 body mass pickle juice Bolus of mustard with similar [Na+] to pickle juice Consumed in full in 2.5 min | ∅ Plasma Na+ or K+ concentration, plasma osmolality, plasma volume |
| Ramos-Jiménez et al., 2014 (Mexico) [35] | RCT | Women (n = 9) Age: 24 ± 5 years | FP | 100% of body mass loss: Plain water hydration or 324 mmol/L CHO, 19.9 mmol/L Na+, 3.2 mmol/L K+ beverage Consumed every 15 min for 90 min | Both water and CHO-based beverage: ↓ Loss of body mass, body temperature, mean blood pressure, HR ∅ Distance traveled, resistance applied to ergometer |
| Logan-Sprenger and Spriet, 2013 (Canada) [36] | Randomized, crossover study | Women (n = 6) Age: 25 ± 1 years | FP | 600 mL of each: Water 40 mM Na+ salt water 3% CES 6% CES Consumed in two phases 15 min apart | Starting in a hypohydrated state, all 4 beverages: ↓ USG ↓ Urine volume |
| West et al., 2012 (Australia) [37] | Double-blind placebo-controlled counterbalanced RCT | Women (n = 9) Age: 23 ± 3 years | FP: between days 1 and 5 | 50 mL·kg−1 fat-free mass of sodium phosphate Consumed daily for 6 days with fluid | ∅ VO2peak, running speed, HR |
| Ali et al., 2011 (New Zealand) [38] | Randomized, crossover study | Women (n = 10) Age: 26 ± 5 | LP | 3 mL·kg−1 body mass water Consumed every 15 min for 90 min | ↓ Change in body mass, core body temperature, HR, blood lactate concentration, RPE ∅ Sprint performance |
| Authors, Year (Country) | Study Design | Participants | Menstrual Cycle Reported | Nutrition-Based Intervention and Duration | Assessment of Athletic Outcome |
|---|---|---|---|---|---|
| Haakonssen et al., 2015 (Japan) [39] | Randomized counterbalanced crossover study | Women (n = 32) Age: 24 ± 4 years | LP or FP | Pre-exercise meal with 1352 ± 53 mg calcium Consumed 2 h before exercise | ↓ Exercise-induced bone resorption markers, hematocrit percentage ∅ Sweat calcium levels, 10 min time trial |
| Dellavalle and Haas, 2013 (United States) [40] | Double-blind placebo-controlled RCT | Women (n = 31) Age: 20 ± 1 years | Menstrual status quantified daily | 50 mg iron sulfate Consumed twice per day for 6 weeks | ↑ Gross efficiency, absolute VO2peak, maximal work rate ↓ Energy expenditure, maximal blood lactate concentration ∅ Endurance time trial, relative VO2peak, HR maximum, RER |
| Authors, Year (Country) | Study Design | Participants | Menstrual Cycle Reported | Nutrition-Based Intervention and Duration | Assessment of Athletic Outcome |
|---|---|---|---|---|---|
| Hiles et al., 2020 (United Kingdom) [42] | Randomized, placebo-controlled double-blind crossover study | Women (n = 6) Age: 21 ± 2 years | MLP | 300 mg New Zealand BC extract Consumed twice daily for 7 days | ↑ Fat oxidation ↓ RER, CHO oxidation ∅ HR, VO2, VCO2; rectal, skin, body temperature; whole body sweat rate |
| Lara et al., 2020 (Spain) [43] | Double-blind, placebo-controlled, crossover RCT | Women (n = 13) Age: 31 ± 6 years | EFP, preovulatory phase, MLP | 3 mg·kg−1 body mass caffeine Consumed 60 min prior to exercise | In EFP, preovulatory phase, MLP: ↑ 15 s Wingate peak power |
| Romero-Moraleda et al., 2019 (Spain) [44] | Double-blind placebo-controlled crossover RCT | Women (n = 13) Age: 31 ± 6 years | EFP LFP MLP | 3 mg·kg−1 body mass caffeine Consumed 45 min prior to exercise | In EFP and LFP: ↑ Peak velocity at 60% 1-RM |
| Brown et al., 2019 (United Kingdom) [45] | Double-blind placebo-controlled RCT | Women (n = 20) Age: 19 ± 1 years | ELP to MLP or 14 days before withdrawal bleed | 30 mL Montmorency cherry concentrate Consumed twice daily for 8 days | ↑ Pain pressure threshold at rectus femoris, CMJ muscle recovery ↓ Rating of muscle soreness ∅ Hamstring stiffness and flexibility, maximum voluntary isometric contraction, 30 m sprint time, repeated sprint time, RPE |
| McKinley-Barnard et al., 2018 (United States) [41] | Double-blind placebo-controlled RCT | Women (n = 22) Age: 21 ± 1 years | MFP: day 6 MLP: day 21 | 2.4 g EPA and 1.8 g DHA (FO) Consumed daily for 21 days | FO: ↑ Perceived muscle soreness, serum estradiol FO during MFP: ↓ Serum myoglobin FO and cycle phase: ∅ Muscular strength Cycle phase: ∅ Perceived muscle soreness |
| Gutierrez-Hellin and Del Coso, 2018 (Spain) [46] | Double-blind placebo-controlled RCT | Women (n = 2) Age: 25 ± 7 years | LP | 3 mg·kg−1 caffeine 3 mg·kg−1 p-synephrine Consumed 60 min prior to exercise | Caffeine: ↑ Fat oxidation at 30–70% VO2max Caffeine + p-synephrine: ↑ Fat oxidation at 40% and 70% VO2max Caffeine: ↑ Muscle power and endurance perception Caffeine: ↓ CHO oxidation at 70% VO2max Caffeine: ↓ Perceived exertion p-synephrine: ↓ CHO oxidation at 60% VO2max ∅ Energy expenditure |
| Strauss et al., 2018 (United Kingdom) [47] | Randomized, placebo-controlled double-blind crossover study | Women (n = 16) Age: 28 ± 8 years | FP: between days 9 and 11 | 600 mg·day−1 New Zealand BC extract Consumed daily for 7 days | ↑ Fat oxidation ↓ CHO oxidation ∅ HR, VO2, VCO2 |
| Buck et al., June 2015 (Australia) [49] | Randomized, placebo-controlled double-blind Latin-square design | Women (n = 13) Age: 26 ± 2 years | FP | 50 mg·L−1 SP Consumed daily for 6 days 70 mL concentrated BJ Consumed 3 h prior to exercise | SP: ↓ Set 1, 2, overall total sprint time, best sprint time SP + BJ: ↓ Set 2 total sprint time vs. placebo BJ: ∅ total sprint time, best sprint time ∅ HR, RPE, blood lactate |
| Buck et al., March 2015 (Australia) [48] | Randomized, placebo-controlled double-blind Latin-square design | Women (n = 12) Age: 26 ± 2 years | FP | 50 mg·L−1 SP Consumed daily for 6 days 6 mg·kg−1 body mass caffeine Consumed 1 h prior to exercise | SP + Caffeine: ↓ Set 1, 2, 3, and overall total sprint time vs. placebo SP + Caffeine: ↓ Set 3 and overall total sprint time vs. Caffeine and vs. SP SP: ↓ Set 1 and 3 total sprint time vs. placebo SP + Caffeine: ↓ Best sprint time ∅ HR, RPE |
| Braakhuis et al., 2014 (Australia) [50] | Randomized, placebo-controlled crossover study | Women (n = 23) Age: 31 ± 8 years | Cycle recorded over 3 weeks | 0.5 L VC juice or BC juice Consumed daily for 21 days | VC: ↓ Training speed VC and BC: ↑ Running times BC: ↓ 5 km time trial in fast runners |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Helm, M.M.; McGinnis, G.R.; Basu, A. Impact of Nutrition-Based Interventions on Athletic Performance during Menstrual Cycle Phases: A Review. Int. J. Environ. Res. Public Health 2021, 18, 6294. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18126294
Helm MM, McGinnis GR, Basu A. Impact of Nutrition-Based Interventions on Athletic Performance during Menstrual Cycle Phases: A Review. International Journal of Environmental Research and Public Health. 2021; 18(12):6294. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18126294
Chicago/Turabian StyleHelm, Macy M., Graham R. McGinnis, and Arpita Basu. 2021. "Impact of Nutrition-Based Interventions on Athletic Performance during Menstrual Cycle Phases: A Review" International Journal of Environmental Research and Public Health 18, no. 12: 6294. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18126294