
Protecting Nurses from Mistreatment by Patients: A Cross-Sectional Study on the Roles of Emotional Contagion Susceptibility and Emotional Regulation Ability



Abstract
:1. Introduction
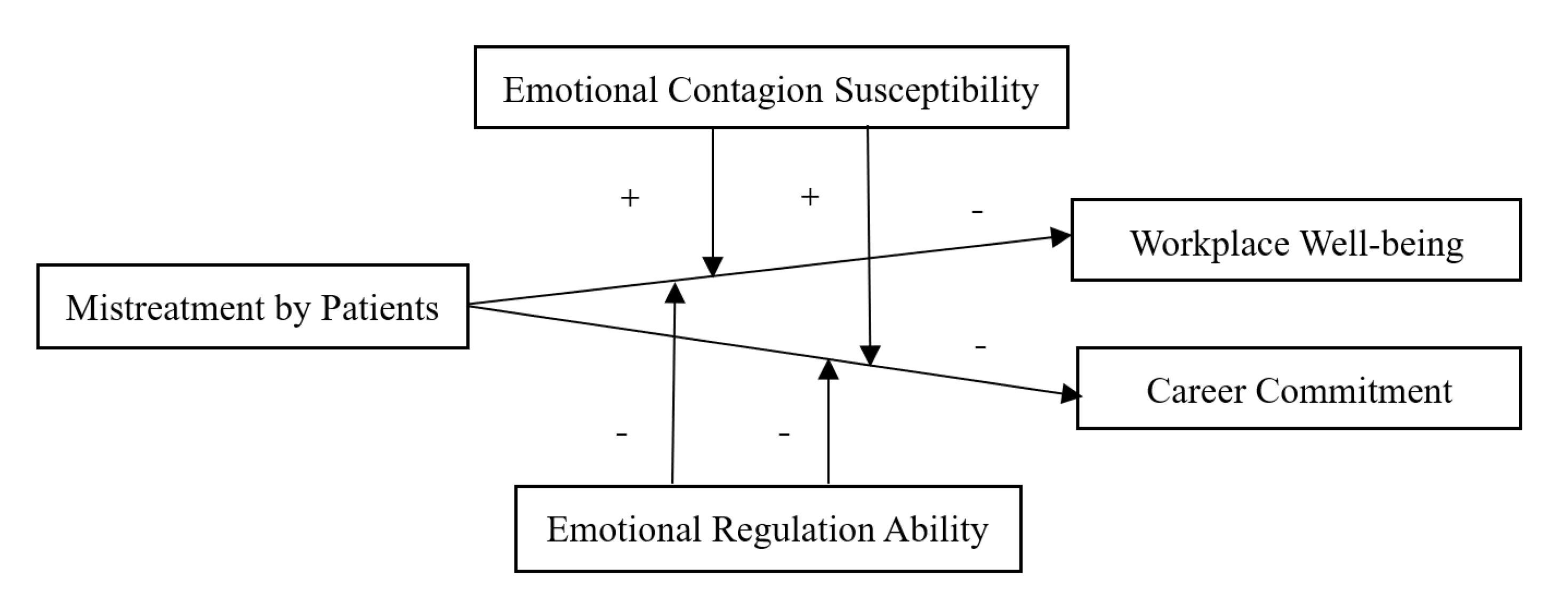
2. Theories and Hypotheses
2.1. Mistreatment by Patients, Workplace Well-Being, and Career Commitment
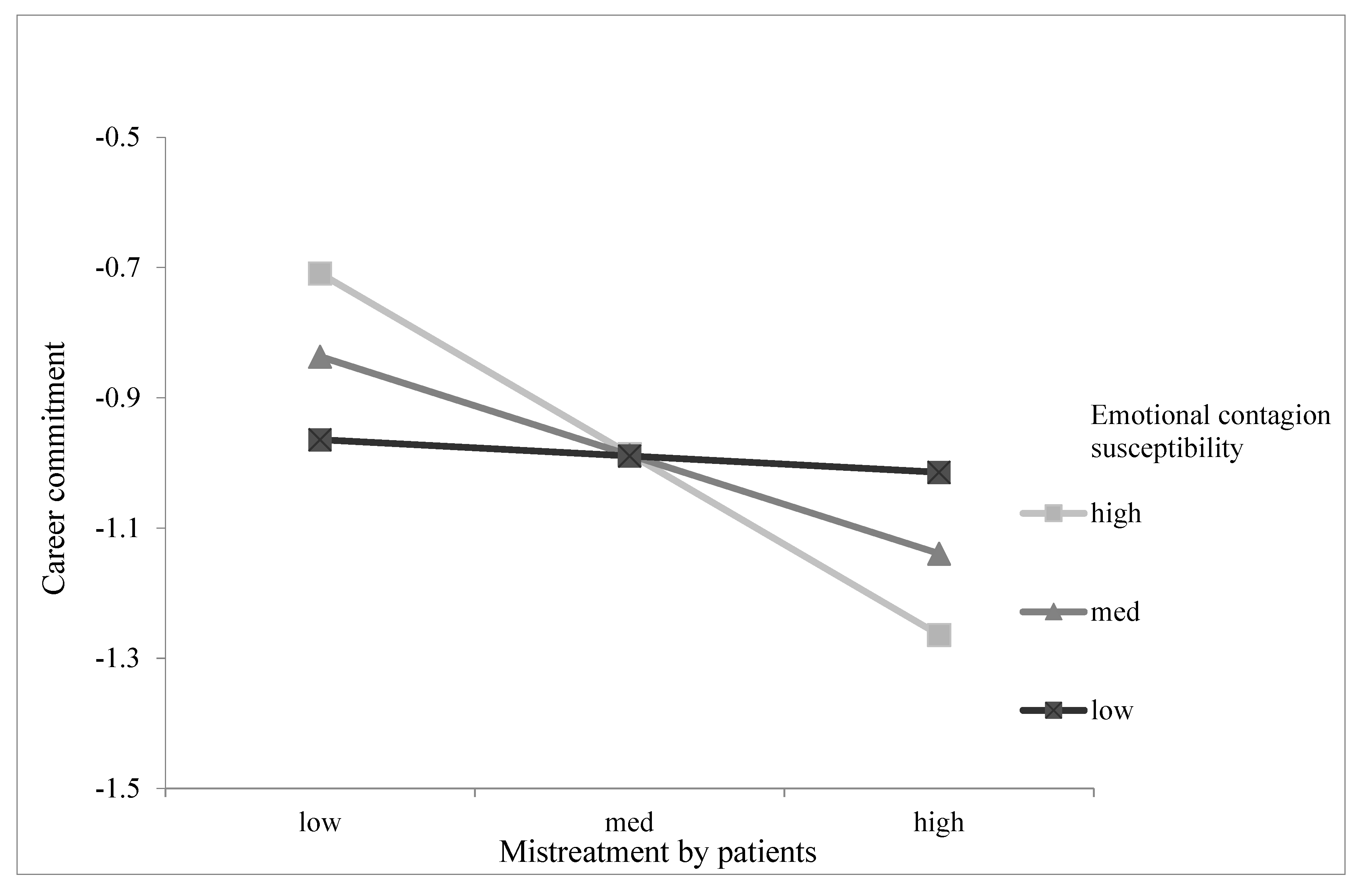
2.2. The Moderating Role of Emotional Contagion Susceptibility
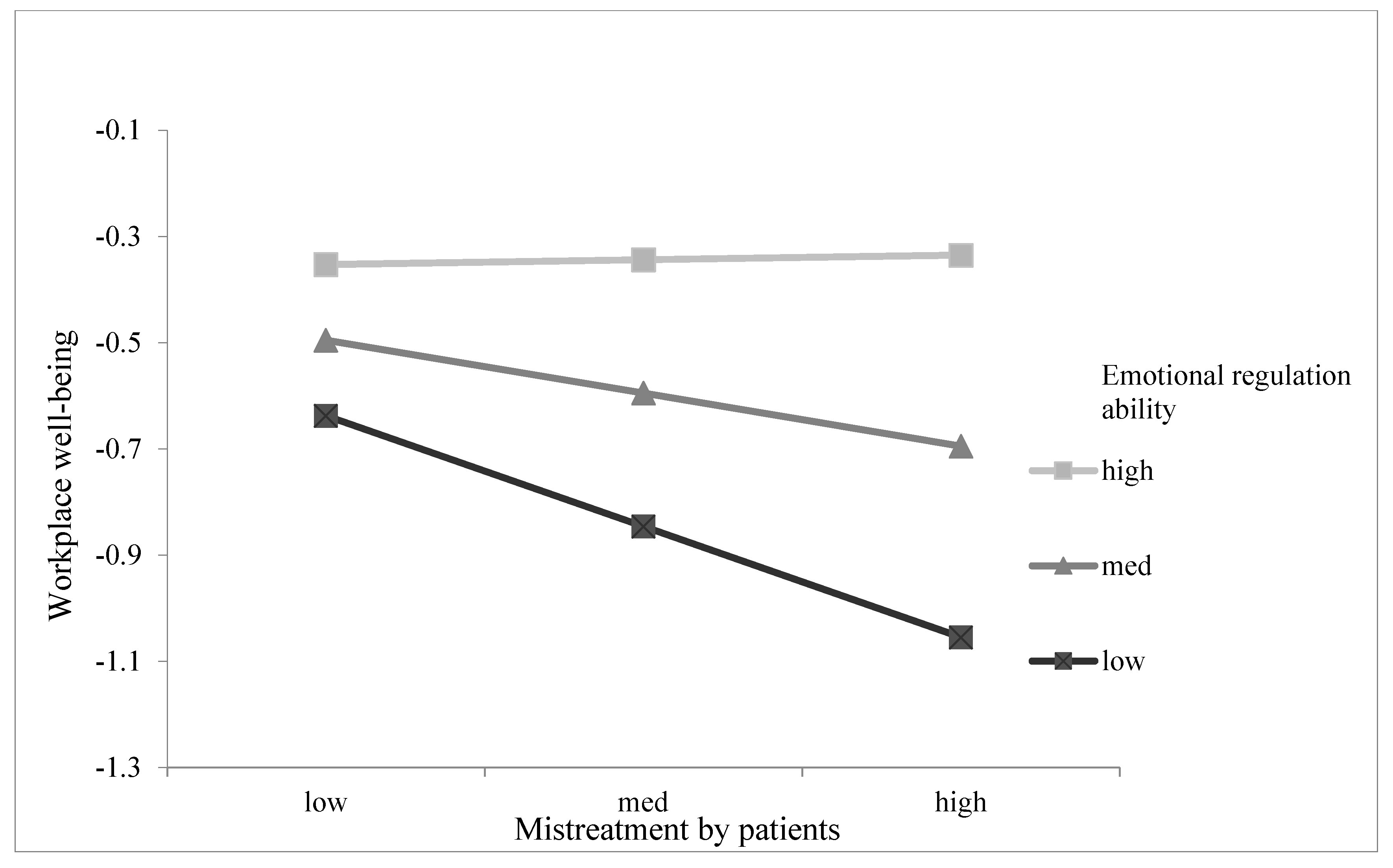
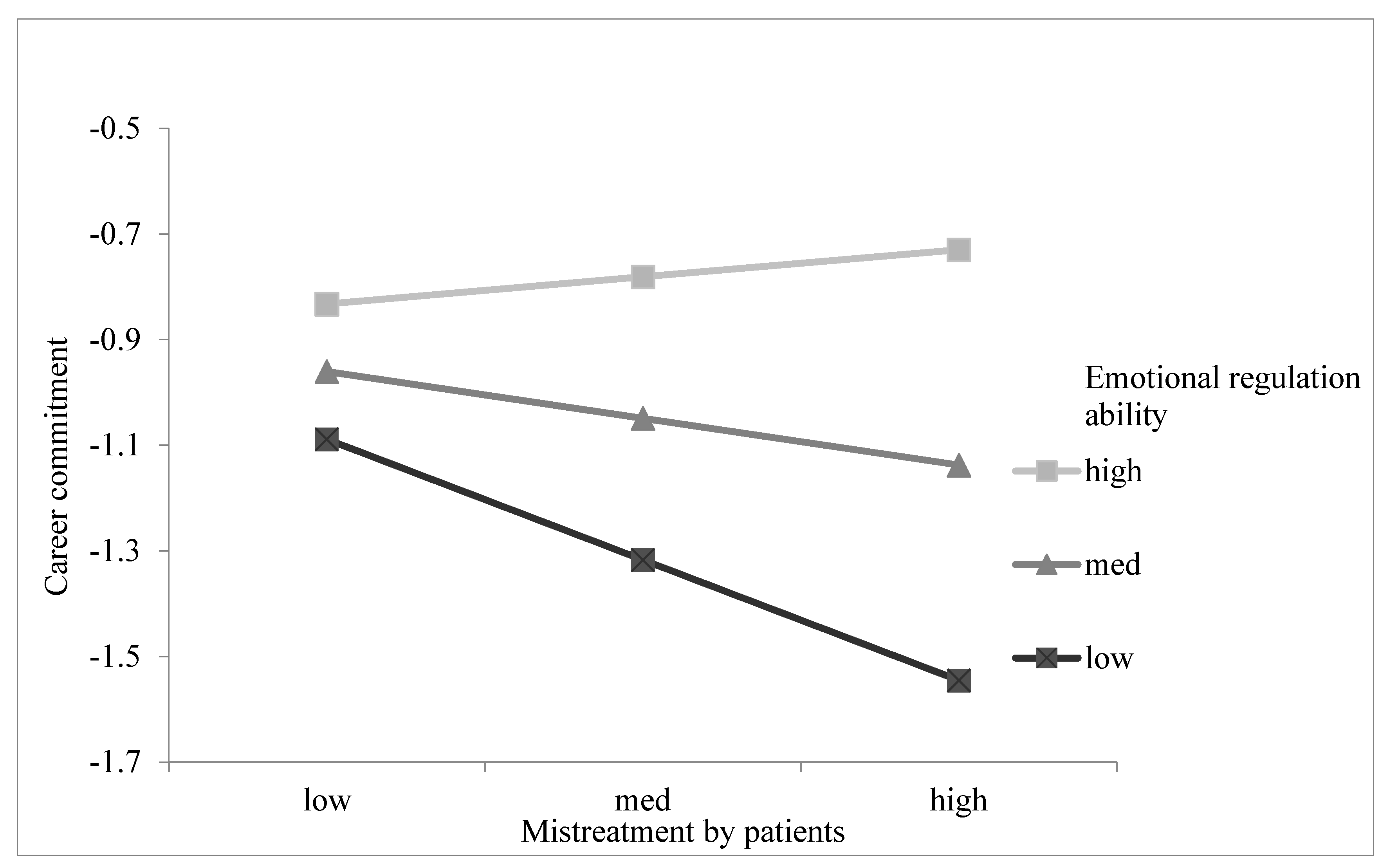
2.3. The Moderating Role of Emotional Regulation Ability
3. Materials and Methods
3.1. Participants and Procedure
3.2. Measures
3.2.1. Mistreatment by Patients
3.2.2. Workplace Well-Being
3.2.3. Career Commitment
3.2.4. Emotional Contagion Susceptibility
3.2.5. Emotional Regulation Ability
3.3. Data Analysis
3.4. Ethics Considerations
4. Results
4.1. Descriptive Statistics
4.2. Harman’s One-Factor Test
4.3. Confirmatory Factor Analysis
4.4. Hypothesis Testing
5. Discussion
5.1. Theoretical Implications
5.2. Practical Implications
5.3. Limitations and Future Research Directions
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Stopping Verbally Abusive Patients in Their Tracks. Available online: https://canadian-nurse.com/en/articles/issues/2012/may-2012/stopping-verbally-abusive-patients-in-their-tracks (accessed on 7 May 2021).
- Nursing Trends and Salary Survey Results 2020. Available online: https://www.myamericannurse.com/2020-nursing-trends-and-salary-survey-results/ (accessed on 7 May 2021).
- Goussinsky, R.; Livne, Y. Coping with Interpersonal Mistreatment: The Role of Emotion Regulation Strategies and Supervisor Support. J. Nurs. Manag. 2016, 24, 1109–1118. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Zheng, J.; Liu, K.; Liu, X.; Wu, Y.; Wang, J.; You, L. Workplace Violence against Nurses, Job Satisfaction, Burnout and Patient Safety in Chinese Hospitals. Nurs. Outlook 2019, 67, 558–566. [Google Scholar] [CrossRef] [PubMed]
- Lin, W.-Q.; Wu, J.; Yuan, L.-X.; Zhang, S.-C.; Jing, M.-J.; Zhang, H.-S.; Luo, J.-L.; Lei, Y.-X.; Wang, P.-X. Workplace Violence and Job Performance among Community Healthcare Workers in China: The Mediator Role of Quality of Life. Int. J. Environ. Res. Public Health 2015, 12, 14872–14886. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, K. Exploring the Influence of Workplace Violence and Bystander Behavior on Patient Safety in Korea: A Pilot Study. J. Nurs. Manag. 2020, 28, 735–743. [Google Scholar] [CrossRef] [PubMed]
- Gunawan, J.; Aungsuroch, Y.; Fisher, M.; Marzilli, C.; Liu, Y. Factors Related to the Clinical Competence of Registered Nurses: Systematic Review and Meta-Analysis. J. Nurs. Scholarsh. 2020, 52, 623–633. [Google Scholar] [CrossRef]
- Alameddine, M.; Baroud, M.; Kharroubi, S.; Hamadeh, R.; Ammar, W.; Shoaib, H.; Khodr, H. Investigating the Job Satisfaction of Healthcare Providers at Primary Healthcare Centres in Lebanon: A National Cross-Sectional Study. Health Soc. Care Community 2017, 25, 1805–1816. [Google Scholar] [CrossRef]
- González-Gancedo, J.; Fernández-Martínez, E.; Rodríguez-Borrego, M.A. Relationships among General Health, Job Satisfaction, Work Engagement and Job Features in Nurses Working in a Public Hospital: A Cross-Sectional Study. J. Clin. Nurs. 2019, 28, 1273–1288. [Google Scholar] [CrossRef]
- Motlagh, F.; Nobahar, M.; Raiesdana, N. The Relationship of Moral Intelligence and Social Capital with Job Satisfaction among Nurses Working in the Emergency Department. Int. Emerg. Nurs. 2020, 52, 100911. [Google Scholar] [CrossRef]
- Lotfi, Z.; Atashzadeh-Shoorideh, F.; Mohtashami, J.; Nasiri, M. Relationship between Ethical Leadership and Organisational Commitment of Nurses with Perception of Patient Safety Culture. J. Nurs. Manag. 2018, 26, 726–734. [Google Scholar] [CrossRef]
- Caldas, M.; Ostermeier, K.; Cooper, D. When Helping Hurts: COVID-19 Critical Incident Involvement and Resource Depletion in Health Care Workers. J. Appl. Psychol. 2020, 106, 29–47. [Google Scholar] [CrossRef]
- Zheng, X.; Zhu, W.; Zhao, H.; Zhang, C. Employee Well-Being in Organizations: Theoretical Model, Scale Development, and Cross-Cultural Validation. J. Organ. Behav. 2015, 36, 621–644. [Google Scholar] [CrossRef]
- Blau, G. The Measurement and Prediction of Career Commitment. J. Occup. Psychol. 1985, 58, 277–288. [Google Scholar] [CrossRef]
- Weiss, H.; Cropanzano, R. Affective Events Theory: A Theoretical Discussion of The Structure, Cause and Consequences of Affective Experiences at Work. Res. Organ. Behav. 1996, 18, 1–74. [Google Scholar] [CrossRef]
- Baranik, L.E.; Wang, M.; Gong, Y.; Shi, J. Customer Mistreatment, Employee Health, and Job Performance: Cognitive Rumination and Social Sharing as Mediating Mechanisms. J. Manag. 2017, 43, 1261–1282. [Google Scholar] [CrossRef]
- Karaeminogullari, A.; Erdogan, B.; Bauer, T. Biting the Hand That Heals: Mistreatment by Patients and the Well-Being of Healthcare Workers. Pers. Rev. 2018, 47, 572–591. [Google Scholar] [CrossRef]
- Singhal, H.; Rastogi, R. Psychological Capital and Career Commitment: The Mediating Effect of Subjective Well-Being. Manag. Decis. 2018, 56, 458–473. [Google Scholar] [CrossRef]
- Chang, H.-Y.; Chu, T.-L.; Liao, Y.-N.; Chang, Y.-T.; Teng, C.-I. How Do Career Barriers and Supports Impact Nurse Professional Commitment and Professional Turnover Intention? J. Nurs. Manag. 2019, 27, 347–356. [Google Scholar] [CrossRef] [PubMed]
- Wilson, V.; Donsante, J.; Pai, P.; Franklin, A.; Bowden, A.; Almeida, S. Building Workforce Wellbeing Capability the Findings of a Wellness Self-care Program. J. Nurs. Manag. 2021, 1–10. [Google Scholar] [CrossRef]
- Koopmann, J.; Wang, M.; Liu, Y.; Song, Y. Customer Mistreatment: A Review of Conceptualizations and a Multilevel Theoretical Model. Res. Occup. Stress Well Being 2015, 13, 33–79. [Google Scholar] [CrossRef] [Green Version]
- Peihang, S.; Zhang, X.; Sun, Y.; Ma, H.; Jiao, M.; Xing, K.; Kang, Z.; Ning, N.; Fu, Y.; Wu, Q.; et al. Workplace Violence against Health Care Workers in North Chinese Hospitals: A Cross-Sectional Survey. Int. J. Environ. Res. Public Health 2017, 14, 96. [Google Scholar] [CrossRef]
- Schablon, A.; Wendeler, D.; Kozak, A.; Nienhaus, A.; Steinke, S. Prevalence and Consequences of Aggression and Violence towards Nursing and Care Staff in Germany—A Survey. Int. J. Environ. Res. Public Health 2018, 15, 1274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gutiérrez-Cobo, M.J.; Megías, A.; Gómez-Leal, R.; Cabello, R.; Fernández-Berrocal, P. The Role of Emotional Intelligence and Negative Affect as Protective and Risk Factors of Aggressive Behavior: A Moderated Mediation Model. Aggress. Behav. 2018, 44, 638–646. [Google Scholar] [CrossRef]
- Sun, H.; Wang, S.; Wang, W.; Han, G.; Liu, Z.; Wu, Q.; Pang, X. Correlation between Emotional Intelligence and Negative Emotions of Front-line Nurses during the COVID-19 Epidemic: A Cross-sectional Study. J. Clin. Nurs. 2020, 30, 385–396. [Google Scholar] [CrossRef] [PubMed]
- Hatfield, E.; Cacioppo, J.; Rapson, R. Primitive emotional contagion. In Current Directions in Psychological Science; Margaret, S.C., Ed.; Sage: Thousand Oaks, CA, USA, 1992; Volume 2, pp. 151–177. [Google Scholar]
- Law, K.S.; Wong, C.-S.; Song, L.J. The Construct and Criterion Validity of Emotional Intelligence and Its Potential Utility for Management Studies. J. Appl. Psychol. 2004, 89, 483–496. [Google Scholar] [CrossRef] [PubMed]
- Yue, Y.; Wang, K.; Groth, M. Feeling Bad and Doing Good: The Effect of Customer Mistreatment on Service Employee’s Daily Display of Helping Behaviors. Pers. Psychol. 2017, 70, 769–808. [Google Scholar] [CrossRef]
- Cai, D.; Li, F.; Feng, T.; Liu, B.; Qi, L.; Men, C. Mistreatment from Patients and Nurses’ Career Withdrawal Intention: Does Political Skill Matter? Asia Pac. J. Hum. Resour. 2020, 1744–7941. [Google Scholar] [CrossRef]
- Şat, S.Ö.; Akbaş, P.; Yaman, Ş. Nurses’ Exposure to Violence and Their Professional Commitment during the COVID-19 Pandemic. J. Clin. Nurs. 2021, 1–12. [Google Scholar] [CrossRef]
- Wickrama, K.; Lee, S.; Klopack, E.; Wickrama, T. Stressful Work Conditions, Positive Affect, and Physical Health of Middle-Aged Couples: A Dyadic Analysis. Stress Health 2019, 35, 382–395. [Google Scholar] [CrossRef]
- Bendersky, C.; Brockner, J. Mistreatment from Peers Can Reduce the Effects of Respectful Treatment from Bosses, and Respectful Peers Can Offset Mistreatment from Bosses. J. Organ. Behav. 2020, 41, 1–15. [Google Scholar] [CrossRef]
- Miner, K.; Cortina, L. Observed Workplace Incivility toward Women, Perceptions of Interpersonal Injustice, and Observer Occupational Well-Being: Differential Effects for Gender of the Observer. Front. Psychol. 2016, 7, 482. [Google Scholar] [CrossRef] [Green Version]
- Hershcovis, S.; Barling, J. Towards a Multi-Foci Approach to Workplace Aggression: A Meta-Analytic Review of Outcomes from Different Perpetrators. J. Organ. Behav. 2009, 31, 24–44. [Google Scholar] [CrossRef]
- Labrague, L.; McEnroe-Petitte, D. Job Stress in New Nurses during the Transition Period: An Integrative Review. Int. Nurs. Rev. 2018, 65, 491–504. [Google Scholar] [CrossRef]
- Tee, E. The Emotional Link: Leadership and the Role of Implict and Explicit Emotional Contagion Processes across Multiple Organizational Levels. Leadersh. Q. 2015, 26, 654–670. [Google Scholar] [CrossRef]
- Ni, X.; Zhou, H.; Chen, W. Addition of an Emotionally Stable Node in the SOSa-SPSa Model for Group Emotional Contagion of Panic in Public Health Emergency: Implications for Epidemic Emergency Responses. Int. J. Environ. Res. Public Health 2020, 17, 5044. [Google Scholar] [CrossRef] [PubMed]
- May, D.D.; Grubbs, L.M. The Extent, Nature, and Precipitating Factors of Nurse Assault among Three Groups of Registered Nurses in a Regional Medical Center. J. Emerg. Nurs. 2002, 28, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Du, J.; Fan, X.; Feng, T. Multiple Emotional Contagions in Service Encounters. J. Acad. Mark. Sci. 2011, 39, 449–466. [Google Scholar] [CrossRef]
- Pugh, S. Service with a Smile: Emotional Contagion in the Service Encounter. Acad. Manag. J. 2001, 44, 1018–1027. [Google Scholar] [CrossRef]
- Geßler, S.; Nezlek, J.; Schuetz, A. Training Emotional Intelligence: Does Training in Basic Emotional Abilities Help People to Improve Higher Emotional Abilities? J. Posit. Psychol. 2020. [Google Scholar] [CrossRef]
- Gross, J. Emotion Regulation: Affective, Cognitive, and Social Consequences. Psychophysiology 2002, 39, 281–291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Waugh, C.E. The Roles of Positive Emotion in the Regulation of Emotional Responses to Negative Events. Emotion 2020, 20, 54–58. [Google Scholar] [CrossRef]
- Hagger, M.; Koch, S.; Chatzisarantis, N.; Orbell, S. The Common Sense Model of Self-Regulation: Meta-Analysis and Test of a Process Model. Psychol. Bull. 2017, 143, 1117–1154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gabriel, A.; Diefendorff, J. Emotional Labor Dynamics: A Momentary Approach. Acad. Manag. J. 2015, 58, 1804–1825. [Google Scholar] [CrossRef]
- Li, Y.; Chen, M.; Lyu, Y.; Qiu, C. Sexual Harassment and Proactive Customer Service Performance: The Roles of Job Engagement and Sensitivity to Interpersonal Mistreatment. Int. J. Hosp. Manag. 2016, 54, 116–126. [Google Scholar] [CrossRef]
- Sultana, R.; Yousaf, A.; Khan, I.; Saeed, A. Probing the Interactive Effects of Career Commitment and Emotional Intelligence on Perceived Objective/Subjective Career Success. Pers. Rev. 2016, 45, 724–742. [Google Scholar] [CrossRef]
- Gross, J. The Emerging Field of Emotion Regulation: An Integrative Review. Rev. Gen. Psychol. 1998, 2, 271–299. [Google Scholar] [CrossRef]
- Podsakoff, P.; MacKenzie, S.; Lee, J.-Y.; Podsakoff, N. Common Method Biases in Behavioral Research: A Critical Review of the Literature and Recommended Remedies. J. Appl. Psychol. 2003, 88, 879–903. [Google Scholar] [CrossRef]
- Brislin, R.W. The wording and translation of research instruments. In Field Methods in Cross-Cultural Research; Lonner, W.J., Berry, J.W., Eds.; Sage Publications: Thousand Oaks, CA, USA, 1986; Volume 8, pp. 137–164. [Google Scholar]
- Skarlicki, D.; Van Jaarsveld, D.; Walker, D. Getting Even for Customer Mistreatment: The Role of Moral Identity in the Relationship between Customer Interpersonal Injustice and Employee Sabotage. J. Appl. Psychol. 2008, 93, 1335–1347. [Google Scholar] [CrossRef] [Green Version]
- McBane, D.A. Empathy and the Salesperson: A Multidimensional Perspective. Psychol. Mark. 1995, 12, 349–370. [Google Scholar] [CrossRef]
- Alshowkan, A. Nurses Attitude toward People with Mental Illness. Eur. Psychiatry 2015, 30, 620. [Google Scholar] [CrossRef]
- Lisa, E.; Anne, S.; Cassidy, M. Age Differences in Negative, but Not Positive, Rumination. J. Gerontol. Ser. B. 2019, 75, 80–84. [Google Scholar] [CrossRef]
- Aiken, L.; West, S. Multiple Regression: Testing and Interpreting Interactions; Sage: Thousand Oaks, CA, USA, 1991; pp. 119–120. [Google Scholar]
- Tang, N.; Thomson, L. Workplace Violence in Chinese Hospitals: The Effects of Healthcare Disturbance on the Psychological Well-Being of Chinese Healthcare Workers. Int. J. Environ. Res. Public Health 2019, 16, 3687. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheung, T.; Lee, P.; Yip, P. Workplace Violence toward Physicians and Nurses: Prevalence and Correlates in Macau. Int. J. Environ. Res. Public Health 2017, 14, 879. [Google Scholar] [CrossRef] [PubMed]
- Yıldırım, D. Bullying among Nurses and Its Effects. Int. Nurs. Rev. 2009, 56, 504–511. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.; Liao, H.; Zhan, Y.; Shi, J. Daily Customer Mistreatment and Employee Sabotage Against Customers:Examining Emotion and Resource Perspectives. Acad. Manag. J. 2011, 54, 312–334. [Google Scholar] [CrossRef]
- Isbell, L.M.; Boudreaux, E.D.; Chimowitz, H.; Liu, G.; Cyr, E.; Kimball, E. What Do Emergency Department Physicians and Nurses Feel? A Qualitative Study of Emotions, Triggers, Regulation Strategies, and Effects on Patient Care. BMJ Qual. Saf. 2020, 29, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Totterdell, P. Catching Moods and Hitting Runs: Mood Linkage and Subjective Performance in Professional Sport Teams. J. Appl. Psychol. 2000, 85, 848–859. [Google Scholar] [CrossRef] [PubMed]
- Kim, J. Emotional Labor Strategies, Stress, and Burnout Among Hospital Nurses: A Path Analysis. J. Nurs. Sch. 2019, 52, 105–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guenter, H.; van Emmerik, I.J.H.; Schreurs, B. The Negative Effects of Delays in Information Exchange: Looking at Workplace Relationships from an Affective Events Perspective. Hum. Resour. Manag. Rev. 2014, 24, 283–298. [Google Scholar] [CrossRef]
- Judge, T.; Scott, B.; Ilies, R. Hostility, Job Attitudes, and Workplace Deviance: Test of a Multilevel Model. J. Appl. Psychol. 2006, 91, 126–138. [Google Scholar] [CrossRef] [Green Version]
- Matta, F.; Erol, T.; Johnson, R.; Bıçaksız, P. Significant Work Events and Counterproductive Work Behavior: The Role of Fairness, Emotions, and Emotion Regulation. J. Organ. Behav. 2014, 35, 920–944. [Google Scholar] [CrossRef]
- Botsford Morgan, W.; Perry, S.J.; Wang, Y. The Angry Implications of Work-to-Family Conflict: Examining Effects of Leadership on an Emotion-Based Model of Deviance. J. Vocat. Behav. 2018, 108, 13–27. [Google Scholar] [CrossRef]
- Leiba, P. Learning from Incidents of Violence in Health Care. An Investigation of ‘Case Reports’ as a Basis for Staff Development and Organisational Change. Nurse Educ. Today 1992, 12, 116–121. [Google Scholar] [CrossRef]
- Lin, Y.-H.; Liu, H.-E. The Impact of Workplace Violence on Nurses in South Taiwan. Int. J. Nurs. Stud. 2005, 42, 773–778. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Jensen, J. The Effects of Active Constructive and Passive Corrective Leadership on Workplace Incivility and the Mediating Role of Fairness Perceptions. Group Organ. Manag. 2014, 39, 416–443. [Google Scholar] [CrossRef]
- Hsu, C.-P.; Chiang, C.-Y.; Chang, C.-W.; Huang, H.-C.; Chen, C.-C. Enhancing the Commitment of Nurses to the Organisation by Means of Trust and Monetary Reward. J. Nurs. Manag. 2015, 23, 567–576. [Google Scholar] [CrossRef]
- Huyghebaert, T.; Gillet, N.; Audusseau, O.; Fouquereau, E. Perceived Career Opportunities, Commitment to the Supervisor, Social Isolation: Their Effects on Nurses’ Well-Being and Turnover. J. Nurs. Manag. 2019, 27, 207–214. [Google Scholar] [CrossRef] [Green Version]
- Karatuna, I.; Jönsson, S.; Muhonen, T. Workplace Bullying in the Nursing Profession: A Cross-Cultural Scoping Review. Int. J. Nurs. Stud. 2020, 111, 103628. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
|---|---|---|---|---|---|---|---|---|---|
| 1. Gender | |||||||||
| 2. Age | 0.112 | ||||||||
| 3. Education | 0.053 | 0.115 | |||||||
| 4. Tenure | 0.143 * | 0.919 *** | 0.076 | ||||||
| 5. Mistreatment by patients | −0.037 | −0.086 | −0.207 *** | −0.085 | (0.878) | ||||
| 6. Workplace well-being | −0.072 | 0.119 * | 0.143 * | 0.082 | −0.210 *** | (0.902) | |||
| 7. Career commitment | −0.058 | 0.039 | 0.127 * | −0.017 | −0.161 ** | 0.598 *** | (0.898) | ||
| 8. Emotional contagion susceptibility | 0.063 | 0.023 | 0.115 * | 0.020 | −0.103 | −0.082 | 0.045 | (0.659) | |
| 9. Emotional regulation ability | −0.027 | −0.043 | 0.013 | −0.064 | −0.083 | 0.355 *** | 0.314 *** | −0.158 ** | (0.879) |
| Mean | 0.98 | 31.310 | 2.700 | 9.180 | 1.620 | 3.179 | 2.884 | 3.269 | 3.108 |
| S. D. | 0.143 | 5.826 | 0.537 | 6.319 | 0.598 | 0.703 | 0.858 | 0.746 | 0.777 |
| Workplace Well-Being | Career Commitment | |||||
|---|---|---|---|---|---|---|
| Predictor | Model 1 | Model 2 | Model 3 | Model 4 | Model 5 | Model 6 |
| Intercept | 2.080 ** (0.679) | −1.575 * (0.625) | −0.446 (0.579) | 0.791 (0.790) | −1.975 ** (0.726) | −1.257 (0.671) |
| Gender | −0.399 (0.245) | −0.398 (0.245) | −0.381 (0.243) | −0.337 (0.362) | −0.350 (0.361) | −0.316 (0.359) |
| Age | 0.025 (0.022) | 0.025 (0.022) | 0.025 (0.020) | 0.042 (0.023) | 0.038 (0.023) | 0.042 * (0.020) |
| Education | 0.131 (0.072) | 0.131 (0.072) | 0.129 (0.071) | 0.132 (0.084) | 0.136 (0.085) | 0.130 (0.083) |
| Tenure | −0.010 (0.020) | −0.010 (0.020) | −0.011 (0.018) | −0.036 (0.021) | −0.036 (0.021) | −0.037 * (0.019) |
| Mistreatment by patients (MP) | −0.189 * (0.074) | −0.188 * (0.076) | −0.173 * (0.070) | −0.158 * (0.076) | −0.208 * (0.084) | −0.138 (0.076) |
| Emotional contagion susceptibility (ECS) | −0.052 (0.056) | −0.051 (0.056) | −0.057 (0.056) | 0.087 (0.077) | 0.062 (0.073) | 0.080 (0.075) |
| MP×ECS | 0.003 (0.100) | −0.293 * (0.134) | ||||
| Emotional regulation ability (ERA) | 0.301 *** (0.055) | 0.301 *** (0.055) | 0.314 *** (0.057) | 0.341 *** (0.066) | 0.344 *** (0.066) | 0.357 *** (0.067) |
| MP×ERA | 0.239 * (0.118) | 0.294 * (0.125) | ||||
| R2 | 0.193 *** | 0.193 *** | 0.211 *** | 0.148 ** | 0.168 *** | 0.166 *** |
| Emotional Contagion Susceptibility | Emotional Regulation Ability | |||||||
|---|---|---|---|---|---|---|---|---|
| Moderation effect | Estimate | SE | 95% CI | Moderation effect | Estimate | SE | 95% CI | |
| Workplace well-being | High emotional contagion susceptibility (mean +1 SD) | −0.186 | 0.114 | [−0.410, 0.040] | High emotional regulation ability (mean +1 SD) | 0.012 | 0.128 | [−0.234, 0.266] |
| Low emotional contagion susceptibility (mean −1 SD) | −0.191 | 0.098 | [−0.370, 0.014] | Low emotional regulation ability (mean −1 SD) | −0.359 *** | 0.101 | [−0.546, −0.153] | |
| The difference | 0.005 | 0.149 | [−0.293, 0.294] | The difference | 0.371 * | 0.183 | [0.027, 0.754] | |
| Career commitment | High emotional contagion susceptibility (mean +1 SD) | −0.426 ** | 0.129 | [−0.679, −0.167] | High emotional regulation ability (mean +1 SD) | 0.090 | 0.143 | [−0.163, 0.393] |
| Low emotional contagion susceptibility (mean −1 SD) | 0.010 | 0.132 | [−0.204, 0.308] | Low emotional regulation ability (mean −1 SD) | −0.367 *** | 0.100 | [−0.552, −0.156] | |
| The difference | −0.437 * | 0.200 | [−0.848, −0.076] | The difference | 0.458 * | 0.194 | [0.108, 0.878] | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, B.; Zhu, N.; Wang, H.; Li, F.; Men, C. Protecting Nurses from Mistreatment by Patients: A Cross-Sectional Study on the Roles of Emotional Contagion Susceptibility and Emotional Regulation Ability. Int. J. Environ. Res. Public Health 2021, 18, 6331. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18126331
Liu B, Zhu N, Wang H, Li F, Men C. Protecting Nurses from Mistreatment by Patients: A Cross-Sectional Study on the Roles of Emotional Contagion Susceptibility and Emotional Regulation Ability. International Journal of Environmental Research and Public Health. 2021; 18(12):6331. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18126331
Chicago/Turabian StyleLiu, Bing, Naixin Zhu, Huijuan Wang, Fengyu Li, and Chenghao Men. 2021. "Protecting Nurses from Mistreatment by Patients: A Cross-Sectional Study on the Roles of Emotional Contagion Susceptibility and Emotional Regulation Ability" International Journal of Environmental Research and Public Health 18, no. 12: 6331. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18126331