
A Randomized Controlled Trial Protocol to Test the Efficacy of a Dual-Task Multicomponent Exercise Program vs. a Simple Program on Cognitive and Fitness Performance in Elderly People

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
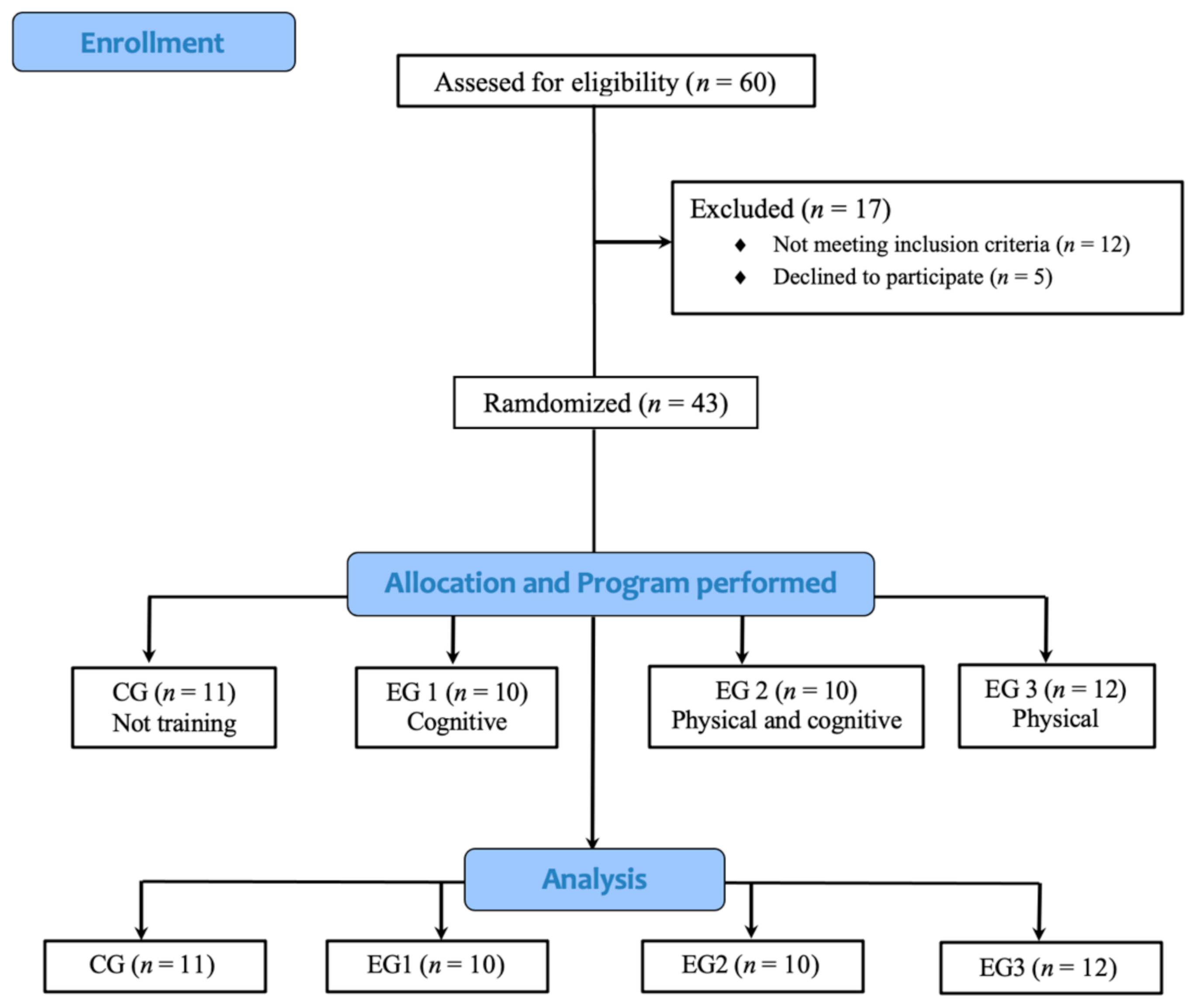
2.1. Participants
2.2. Materials and Testing
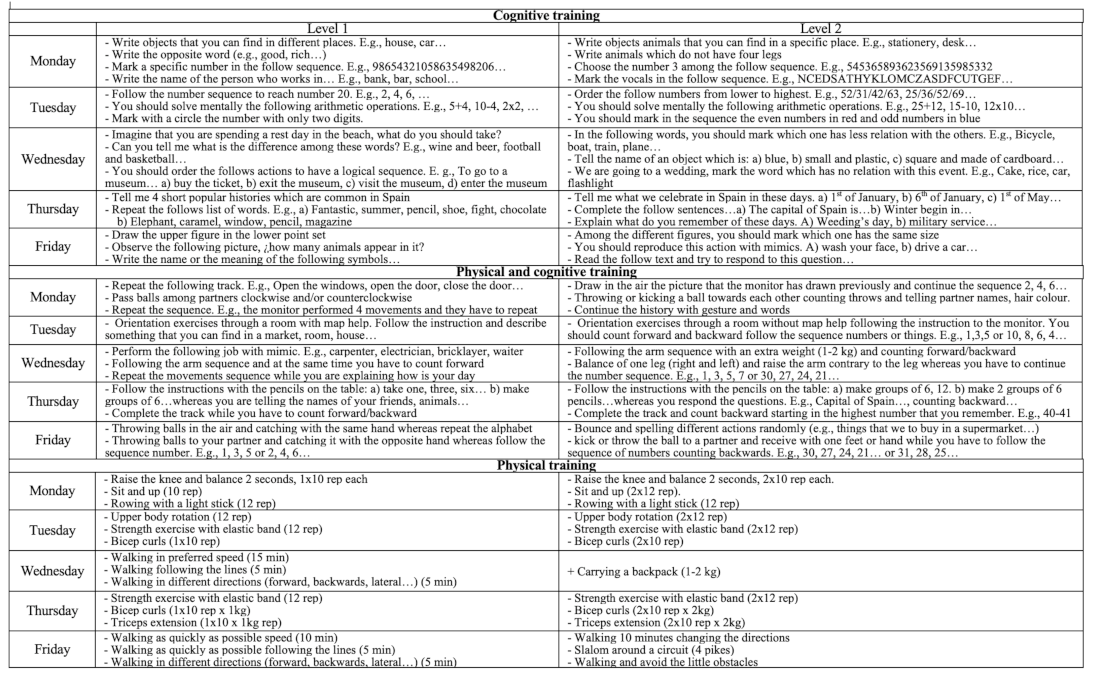
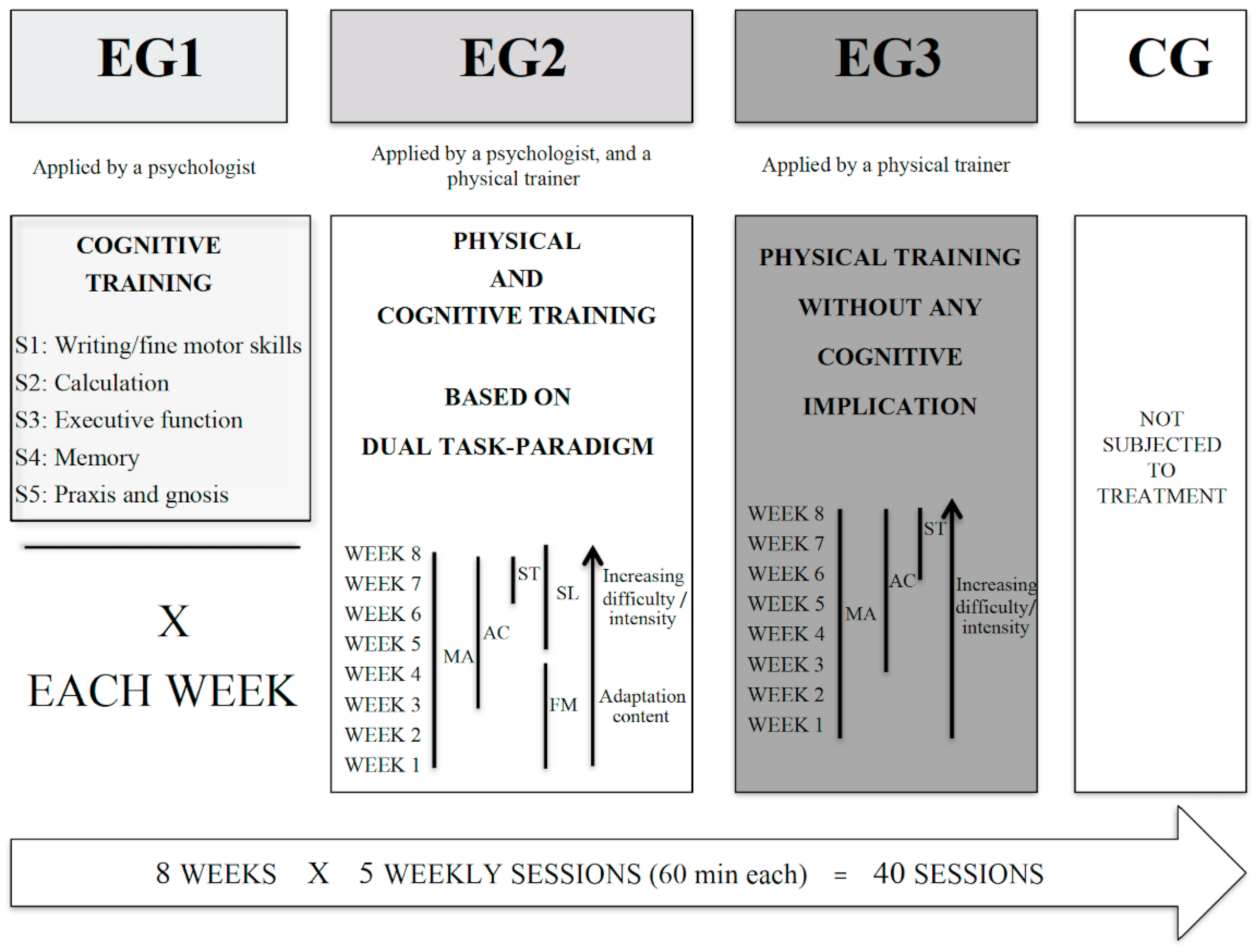
2.3. Procedures
2.4. Data Analysis
3. Results
4. Discussion
4.1. Cognitive Variables
4.2. Fitness Variables
4.3. Practical Application
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BMI | Body Mass Index |
| HS | Handgrip Strength |
| CG | Control Group |
| EG1 | Experimental Group 1 |
| EG2 | Experimental Group 2 |
| EG3 | Experimental Group 3 |
| V-ART | Visual Art Reaction Time |
| TMT | Trail Making Test |
| 2MST | 2 Minutes Step Test |
References
- Sternäng, O.; Reynolds, C.A.; Finkel, D.; Ernsth-Bravell, M.; Pedersen, N.L.; Dahl Aslan, A.K. Grip strength and cognitive abilities: Associations in old age. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2016, 71, 841–848. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rönnlund, M.; Nyberg, L.; Bäckman, L.; Nilsson, L.G. Stability, growth, and decline in adult life span development of declarative memory: Cross-sectional and longitudinal data from a population-based study. Psychol. Aging 2005, 20, 3–18. [Google Scholar] [CrossRef] [PubMed]
- Auyeung, T.W.; Lee, J.S.W.; Kwok, T.; Woo, J. Physical frailty predicts future cognitive decline - A four-year prospective study in 2737 cognitively normal older adults. J. Nutr. Heal. Aging 2011, 15, 690–694. [Google Scholar] [CrossRef] [PubMed]
- López, M.D.; Zamarrón, M.D.; Fernández-Ballesteros, R. Asociación entre la realización de ejercicio e indicadores de funcionamiento físico y cognitivo. Comparativa de resultados en función de la edad. Rev. Esp. Geriatr. Gerontol. 2011, 46, 15–20. [Google Scholar] [CrossRef]
- Rezola-Pardo, C.; Arrieta, H.; Gil, S.M.; Yanguas, J.J.; Iturburu, M.; Irazusta, J.; Sanz, B.; Rodriguez-Larrad, A. A randomized controlled trial protocol to test the efficacy of a dual-task multicomponent exercise program in the attenuation of frailty in long-term nursing home residents: Aging-ONDUAL-TASK study. BMC Geriatr. 2019, 19, 6. [Google Scholar] [CrossRef]
- Woollacott, M.; Shumway-Cook, A. Attention and the control of posture and gait: A review of an emerging area of research. Gait Posture 2002, 16, 1–14. [Google Scholar] [CrossRef]
- Montero-Odasso, M.; Bergman, H.; Phillips, N.A.; Wong, C.H.; Sourial, N.; Chertkow, H. Dual-tasking and gait in people with mild cognitive impairment. The effect of working memory. BMC Geriatr. 2009, 9, 41. [Google Scholar] [CrossRef] [Green Version]
- Bridenbaugh, S.A.; Kressig, R.W. Laboratory review: The role of gfait analysis in seniors’ mobility and fall prevention. Gerontology 2011, 57, 256–264. [Google Scholar] [CrossRef] [Green Version]
- Weuve, J.; Kang, J.H.; Manson, J.A.E.; Breteler, M.M.B.; Ware, J.H.; Grodstein, F. Physical activity, including walking, and cognitive function in older women. J. Am. Med. Assoc. 2004, 292, 1454–1461. [Google Scholar] [CrossRef] [Green Version]
- Alves, C.R.R.; Gualano, B.; Takao, P.P.; Avakian, P.; Fernandes, R.M.; Morine, D.; Takito, M.Y. Effects of acute physical exercise on executive functions: A comparison between aerobic and strength exercise. J. Sport Exerc. Psychol. 2012, 34, 539–549. [Google Scholar] [CrossRef] [Green Version]
- Mavros, Y.; Gates, N.; Wilson, G.C.; Jain, N.; Meiklejohn, J.; Brodaty, H.; Wen, W.; Singh, N.; Baune, B.T.; Suo, C.; et al. Mediation of Cognitive Function Improvements by Strength Gains After Resistance Training in Older Adults with Mild Cognitive Impairment: Outcomes of the Study of Mental and Resistance Training. J. Am. Geriatr. Soc. 2017, 65, 550–559. [Google Scholar] [CrossRef]
- Kramer, A.F.; Colcombe, S. Fitness Effects on the Cognitive Function of Older Adults: A Meta-Analytic Study—Revisited. Perspect. Psychol. Sci. 2018, 13, 213–217. [Google Scholar] [CrossRef] [Green Version]
- Farina, N.; Rusted, J.; Tabet, N. The effect of exercise interventions on cognitive outcome in Alzheimer’s disease: A systematic review. Int. Psychogeriatrics 2014, 26, 9–18. [Google Scholar] [CrossRef] [Green Version]
- Hsu, C.L.; Best, J.R.; Davis, J.C.; Nagamatsu, L.S.; Wang, S.; Boyd, L.A.; Hsiung, G.R.; Voss, M.W.; Eng, J.J.; Liu-Ambrose, T. Aerobic exercise promotes executive functions and impacts functional neural activity among older adults with vascular cognitive impairment. Br. J. Sports Med. 2018, 52, 184–191. [Google Scholar] [CrossRef]
- Bliss, E.S.; Wong, R.H.X.; Howe, P.R.C.; Mills, D.E. Benefits of exercise training on cerebrovascular and cognitive function in ageing. J. Cereb. Blood Flow Metab. 2021, 41, 447–470. [Google Scholar] [CrossRef]
- Nagamatsu, L.S.; Chan, A.; Davis, J.C.; Beattie, B.L.; Graf, P.; Voss, M.W.; Sharma, D.; Liu-Ambrose, T. Physical activity improves verbal and spatial memory in older adults with probable mild cognitive impairment: A 6-month randomized controlled trial. J. Aging Res. 2013, 2013. [Google Scholar] [CrossRef] [Green Version]
- Liu-Ambrose, T.; Nagamatsu, L.S.; Voss, M.W.; Khan, K.M.; Handy, T.C. Resistance training and functional plasticity of the aging brain: A 12-month randomized controlled trial. Neurobiol. Aging 2012, 33, 1690–1698. [Google Scholar] [CrossRef]
- Vaughan, S.; Wallis, M.; Polit, D.; Steele, M.; Shum, D.; Morris, N. The effects of multimodal exercise on cognitive and physical functioning and brain-derived neurotrophic factor in older women: A randomised controlled trial. Age Ageing 2014, 43, 623–629. [Google Scholar] [CrossRef] [Green Version]
- Fragala, M.S.; Beyer, K.S.; Jajtner, A.R.; Jeremy, R.; Pruna, G.J.; Boone, C.H.; Bohner, J.D.; Fukuda, D.H.; Stout, J.R.; Hoffman, J.R. Resistance exercise may improve spatial awareness and visual reaction in older adults. J. Strength Cond. Res. 2014, 28, 2079–2087. [Google Scholar] [CrossRef] [Green Version]
- Keating, C.J.; Cabrera-Linares, J.C.; Párraga-Montilla, J.A.; Latorre-Román, P.A.; del Castillo, R.M.; García-Pinillos, F. Influence of Resistance Training on Gait & Balance Parameters in Older Adults: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 1759. [Google Scholar] [CrossRef]
- Bouaziz, W.; Vogel, T.; Schmitt, E.; Kaltenbach, G.; Geny, B.; Lang, P.O. Health benefits of aerobic training programs in adults aged 70 and over: A systematic review. Arch. Gerontol. Geriatr. 2017, 69, 110–127. [Google Scholar] [CrossRef] [PubMed]
- Taekema, D.G.; Gussekloo, J.; Maier, A.B.; Westendorp, R.G.J.; de Craen, A.J.M. Handgrip strength as a predictor of functional, psychological and social health. A prospective population-based study among the oldest old. Age Ageing 2010, 39, 331–337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taekema, D.G.; Ling, C.H.Y.; Kurrle, S.E.; Cameron, I.D.; Meskers, C.G.M.; Blauw, G.J.; Westendorp, R.G.J.; De craen, A.J.M.; Maier, A.B. Temporal relationship between handgrip strength and cognitive performance in oldest old people. Age Ageing 2012, 41, 506–512. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burns, J.M.; Johnson, D.K.; Watts, A.; Swerdlow, R.H.; Brooks, W.M. Reduced lean mass in early Alzheimer disease and its association with brain atrophy. Arch. Neurol. 2010, 67, 428–433. [Google Scholar] [CrossRef]
- Ling, C.H.Y.; Taekema, D.; De Craen, A.J.M.; Gussekloo, J.; Westendorp, R.G.J.; Maier, A.B. Handgrip strength and mortality in the oldest old population: The Leiden 85-plus study. Cmaj 2010, 182, 429–435. [Google Scholar] [CrossRef] [Green Version]
- Cooper, R.; Kuh, D.; Hardy, R. Objectively measured physical capability levels and mortality: Systematic review and meta-analysis. BMJ 2010, 341, 639. [Google Scholar] [CrossRef] [Green Version]
- Hertzog, C.; Kramer, A.F.; Wilson, R.S.; Lindenberger, U. Enrichment Effects on Adult Cognitive Development. Psychol. Sci. Public Interes. 2008, 9, 1–65. [Google Scholar] [CrossRef] [Green Version]
- Bherer, L.; Erickson, K.I.; Liu-Ambrose, T. A review of the effects of physical activity and exercise on cognitive and brain functions in older adults. J. Aging Res. 2013, 2013. [Google Scholar] [CrossRef] [Green Version]
- Aley, L.; Miller, E.W.; Bode, S.; Hall, L.; Markusic, J.; Nicholson, M.; Winegardner, M. Effects of age, task complexity, and exercise on reaction time of women during ambulation tasks. J. Geriatr. Phys. Ther. 2007, 30, 3–7. [Google Scholar] [CrossRef]
- Pijnappels, M.; Delbaere, K.; Sturnieks, D.L.; Lord, S.R. The association between choice stepping reaction time and falls in older adults-a path analysis model. Age Ageing 2010, 39, 99–104. [Google Scholar] [CrossRef] [Green Version]
- Senior fitness test manual. Choice Rev. Online 2002, 39, 39-3447. [CrossRef] [Green Version]
- Innes, E. Handgrip strength testing: A review of the literature. Aust. Occup. Ther. J. 1999, 46, 120–140. [Google Scholar] [CrossRef]
- Pedrero-Chamizo, R.; Albers, U.; Tobaruela, J.L.; Meléndez, A.; Castillo, M.J.; González-Gross, M. Physical strength is associated with Mini-Mental State Examination scores in Spanish institutionalized elderly. Geriatr. Gerontol. Int. 2013, 13, 1026–1034. [Google Scholar] [CrossRef]
- Lienhard, K.; Schneider, D.; Maffiuletti, N.A. Validity of the Optogait photoelectric system for the assessment of spatiotemporal gait parameters. Med. Eng. Phys. 2013, 35, 500–504. [Google Scholar] [CrossRef]
- Stroop, J.R. Studies of interference in serial verbal reactions. J. Exp. Psychol. 1935, 18, 643–662. [Google Scholar] [CrossRef]
- Golden, C.J. Test de Colores y Palabras (Stroop), 6th ed.; Ruiz-Fernández, B., Luque, T., Sánchez-Sánchez, F., Eds.; TEA Ediciones, S.A.U.: Madrid, Spain, 2020; ISBN 9788416231782. [Google Scholar]
- Brickenkamp, R. d2, Test de Atención (adapt. Nicolás Seisdedos Cubero), 4th ed.; Cubero, N.S., Ed.; TEA Ediciones, S.A.U.: Madrid, Spain, 2012; ISBN 978-84-15262-68-8. [Google Scholar]
- Reitan, R.M. Validity of the trail making test as an indicator of organic brain damage. Percept. Mot. Ski. 1958, 8, 271–276. [Google Scholar] [CrossRef]
- Valencia Marín, C.M.; López Alzate, E.; Tirado Pérez, V.; Zea Herrera, M.; Lopera Restrepo, F.; Rupprecht, R.; Oswald, W.D. Efectos cognitivos de un entrenamiento combinado de memoria y psicomotricidad en adultos mayores. Rev. Neurol. 2008, 46, 465. [Google Scholar] [CrossRef] [Green Version]
- Fabre, C.; Chamari, K.; Mucci, P.; Massé-Biron, J.; Préfaut, C. Improvement of Cognitive Function by Mental and/or Individualized Aerobic Training in Healthy Elderly Subjects. Int. J. Sports Med. 2002, 23, 415–421. [Google Scholar] [CrossRef]
- Bijlsma, A.Y.; Meskers, C.G.M.; Ling, C.H.Y.; Narici, M.; Kurrle, S.E.; Cameron, I.D.; Westendorp, R.G.J.; Maier, A.B. Defining sarcopenia: The impact of different diagnostic criteria on the prevalence of sarcopenia in a large middle aged cohort. Age 2013, 35, 871–881. [Google Scholar] [CrossRef] [Green Version]
- Falbo, S.; Condello, G.; Capranica, L.; Forte, R.; Pesce, C. Effects of Physical-Cognitive Dual Task Training on Executive Function and Gait Performance in Older Adults: A Randomized Controlled Trial. Biomed Res. Int. 2016, 2016. [Google Scholar] [CrossRef]
- Plummer, P.; Zukowski, L.A.; Giuliani, C.; Hall, A.M.; Zurakowski, D. Effects of Physical Exercise Interventions on Gait-Related Dual-Task Interference in Older Adults: A Systematic Review and Meta-Analysis. Gerontology 2015, 62, 94–117. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| TOTAL n = 43 Mean (SD) | CG n = 11 Mean (SD) | EG1 n = 10 Mean (SD) | EG2 n = 10 Mean (SD) | EG3 n = 12 Mean (SD) | p Value | |
|---|---|---|---|---|---|---|
| Age (years) | 80.86 (5.03) | 78.54 (3.83) | 82.00 (7.25) | 82.70 (5.05) | 80.50 (3.08) | 0.240 |
| BMI (kg/m2) | 24.39 (2.44) | 24.33 (2.09) | 25.97 (3.16) | 23.37 (2.24) | 23.97 (1.78) | 0.094 |
| Weight (kg) | 61.62 (6,51) | 61.40 (5.57) | 64.36 (9.25) | 59.57 (5.27) | 61.25 (5.49) | 0.435 |
| Height (cm) | 159.00 (5.38) | 158.90 (5.06) | 157.40 (8.16) | 159.70 (3.16) | 159.83 (4.56) | 0.733 |
| Variables | Groups | n | Pre-Test Median (95% CI) | Post-Test Median (95% CI) | Increase Median (95% CI) |
|---|---|---|---|---|---|
| Stroop (total points) | CG | 11 | 13.17 (9.78/27.34) | 7.57 (3.05/14.81) | −5.82 (−8.25/−4.19) a |
| EG1 | 10 | 13.95 (9.65/24.87) | 11.96 (8.70/19.63) | −3.23 (−4.47/−1.00) b | |
| EG2 | 10 | 12.90 (1.02/23.91) | 9.55 (5.54/21.02) | 0.14 (2.22/2.78) b | |
| EG3 | 12 | 17.32 (8.83/36.16) | 14.71 (5.34/35.20) | −2.16 (−2.80/−0.90) b | |
| p-value (group time) | 0.709 | 0.426 | 0.002 | ||
| D2 (total points) | CG | 11 | 145.00 (59.00/252.00) | 84.00 (69.00/136.00) | −17.00 (−94.00/2.00) a |
| EG1 | 10 | 82.50 (37.01/128.00) | 134.00 (68.00/166.50) | 20.00 (5.00/76.50) b | |
| EG2 | 10 | 147.50 (96.00/229.00) | 186.50 (137.00/247.00) | 22.00 (9.00/42.00) b | |
| EG3 | 12 | 94.00 (50.00/236.00) | 130.00 (48.234/122.33) | 7.50 (−2.00/25.85) b | |
| p-value (group time) | 0.325 | 0.091 | 0.001 | ||
| D2 (concentration) | CG | 11 | 42.00 (5.00/79.00) | 10.00 (7.00/15.00) | −30.00 (−68.00/5.00) a |
| EG1 | 10 | 3.00 (−2.41/15.50) | 20.50 (3.00/35.98) | 16.00 (4.00/34.00) b | |
| EG2 | 10 | 32.00 (23.00/94.00) | 66.00 (22.50/140.50) | 10.00 (3.50/35.00) b | |
| EG3 | 12 | 21.00 (6.00/99.00) | 22.50 (10.50/108.00) | 4.50 (3.00/7.00) b | |
| p-value (group time) | 0.021 | 0.096 | 0.002 | ||
| TMT (task A) (s) | CG | 11 | 229.00 (122.00/349.00) | 254.00 (72.89/143.39) | 19.00 (−14.00/45.00) a |
| EG1 | 10 | 303.50 (252.00/347.47) | 211.00 (179.50/252.00) | −76.50 (−95.00/−52.00) b | |
| EG2 | 10 | 222.50 (146.50/291.00) | 138.00 (83.00/206.00) | −66.50 (−81.00/−50.00) b | |
| EG3 | 12 | 205.80 (115.50/261.60) | 133.20 (34.80/180.31) | −57.90 (−68.40/−48.60) b | |
| p-value (group time) | 0.092 | 0.021 | <0.001 | ||
| TMT (task B) (s) | CG | 11 | 362.00 (316.00/454.00) | 430.00 (361.00/470.00) a | 41.00 (29.00/51.00) a |
| EG1 | 10 | 415.50 (298.00/468.97) | 294.50 (275.05/372.00) b | −77.00 (−116.00/−28.00) b | |
| EG2 | 10 | 305.00 (246.00/409.50) | 275.50 (230.00/312.50) b | −59.50 (−90.00/−14.00) b | |
| EG3 | 12 | 324.29 (274.20/450.00) | 264.00 (227.10/421.20) b | −59.39 (−69.59/−32.99) b | |
| p-value (group time) | 0.352 | 0.001 | <0.001 | ||
| Variables | Groups | n | Pre-Test Median (95% CI) | Post-Test Median (95% CI) | Increase Median (95% CI) |
|---|---|---|---|---|---|
| HS (Kg) | CG | 11 | 17.70 (14.40/19.20) | 17.00 (12.60/18.50) | −0.69 (−1.80/0.00) a |
| EG1 | 10 | 12.85 (9.80/16–50) | 13.25 (10.85/18.50) | 1.35 (0.30/1.69) b | |
| EG2 | 10 | 15.95 (10.10/19.15) | 17.45 (11.80/21.00) | 1.65 (1.30/2.00) b | |
| EG3 | 12 | 15.05 (10.10/18.30) | 15.95 (11.40/19.20) | 1.35 (0.59/1.75) b | |
| p-value (group time) | 0.108 | 0.551 | <0.001 | ||
| 2MST (step number) | CG | 11 | 84.00 (77.00/86.00) | 81.00 (77.00/86.00) | 0.00 (−4.00/0.00) a |
| EG1 | 10 | 71.50 (57.00/82.48) | 78.00 (63.00/88.00) | 5.50 (2.00/7.00) b | |
| EG2 | 10 | 83.00 (79.00/90.00) | 94.50 (87.00/97.00) | 11.00 (4.00/14.00) b,c | |
| EG3 | 12 | 82.50 (56.00/97.00) | 85.50 (67.00/104.00) | 9.00 (7.00/12.50) c | |
| p-value (group time) | 0.171 | 0.015 | <0.001 | ||
| V-ART (s) | CG | 11 | 0.79 (0.67/1.03) a | 1.03 (0.82/1.31) | 0.23 (0.11/0.34) a |
| EG1 | 10 | 1.26 (1.05/1.34) b | 0.92 (0.85/1.05) | −0.32 (−0.37/−0.12) b,c | |
| EG2 | 10 | 1.18 (0.90/1.45) b,c | 0.89 (0.77/1.41) | −0.33 (−0.42/−0.03) b | |
| EG3 | 12 | 0.89 (0.85/1.07) a,c | 0.81 (0.63/0.92) | −0.20 (-0.21/-0.09)c | |
| p-value (group time) | 0.001 | 0.067 | <0.001 | ||
| ∆ Stroop | ∆ D2 (Total Points) | ∆ D2 (Concentration) | ∆ TMT Task-A | ∆ TMT Task-B | ∆2MST | ∆V-ART | ∆HS | |
|---|---|---|---|---|---|---|---|---|
| ∆ Stroop | 1 | 0.104 | 0.172 | −0.352 * | −0.224 | 0.336 * | −0.311 * | 0.219 |
| D2 (total points) | 1 | 0.380 | −0.397 ** | −0.530 ** | 0.511 ** | −0.470 ** | 0.545 ** | |
| ∆ D2 (concentration) | 1 | −0.347 * | −0.307 * | 0.348 * | −0.209 | 0.409 ** | ||
| ∆ TMT Task-A | 1 | 0.495 ** | −0.350 * | 0.417 ** | −0.513 ** | |||
| ∆ TMT Task-B | 1 | −0.458 ** | 0.577 ** | −0.546 ** | ||||
| ∆ 2MST | 1 | −0.366 * | 0.560 ** | |||||
| ∆ V-ART | 1 | −0.484 ** | ||||||
| ∆ HS | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Párraga-Montilla, J.A.; Aibar-Almazán, A.; Cabrera-Linares, J.C.; Lozano-Aguilera, E.; Serrano Huete, V.; Escarabajal Arrieta, M.D.; Latorre-Román, P.Á. A Randomized Controlled Trial Protocol to Test the Efficacy of a Dual-Task Multicomponent Exercise Program vs. a Simple Program on Cognitive and Fitness Performance in Elderly People. Int. J. Environ. Res. Public Health 2021, 18, 6507. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18126507
Párraga-Montilla JA, Aibar-Almazán A, Cabrera-Linares JC, Lozano-Aguilera E, Serrano Huete V, Escarabajal Arrieta MD, Latorre-Román PÁ. A Randomized Controlled Trial Protocol to Test the Efficacy of a Dual-Task Multicomponent Exercise Program vs. a Simple Program on Cognitive and Fitness Performance in Elderly People. International Journal of Environmental Research and Public Health. 2021; 18(12):6507. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18126507
Chicago/Turabian StylePárraga-Montilla, Juan Antonio, Agustín Aibar-Almazán, José Carlos Cabrera-Linares, Emilio Lozano-Aguilera, Víctor Serrano Huete, María Dolores Escarabajal Arrieta, and Pedro Ángel Latorre-Román. 2021. "A Randomized Controlled Trial Protocol to Test the Efficacy of a Dual-Task Multicomponent Exercise Program vs. a Simple Program on Cognitive and Fitness Performance in Elderly People" International Journal of Environmental Research and Public Health 18, no. 12: 6507. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18126507