
Rural–Urban Inequalities in Poor Self-Rated Health, Self-Reported Functional Disabilities, and Depression among Chinese Older Adults: Evidence from the China Health and Retirement Longitudinal Study 2011 and 2015


Abstract
:1. Introduction
2. Materials and Methods
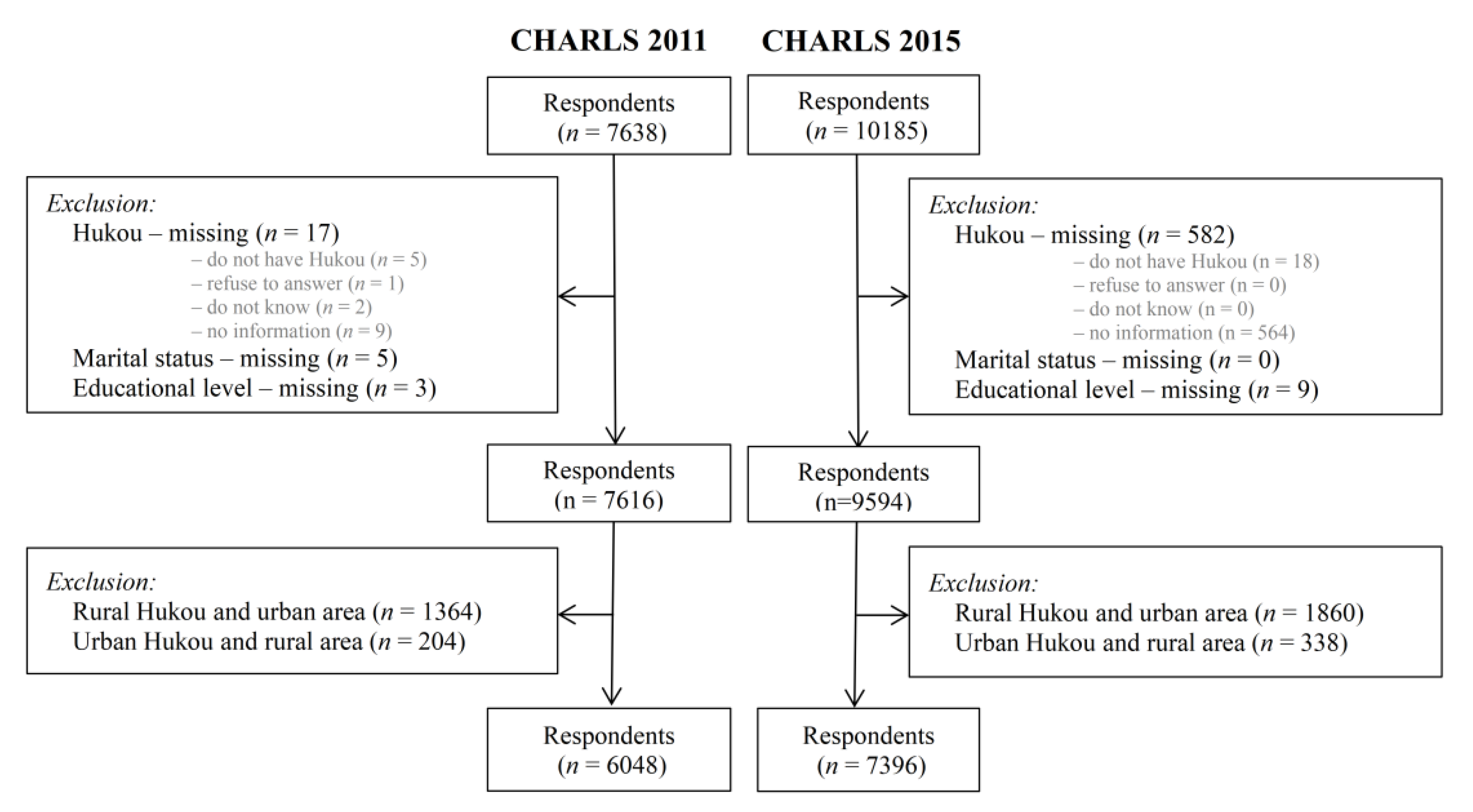
2.1. Data Sources
2.2. Demographic Indicators
2.3. Socioeconomic Indicators
2.4. Outcome Variables
2.4.1. Self-Rated Health
2.4.2. Basic Activities of Daily Living
2.4.3. Instrumental Activities of Daily Living
2.4.4. Self-Reported Depression
2.5. Statistical Analyses
3. Results
3.1. Results of Initial Analyses on Hukou Registration and Residence
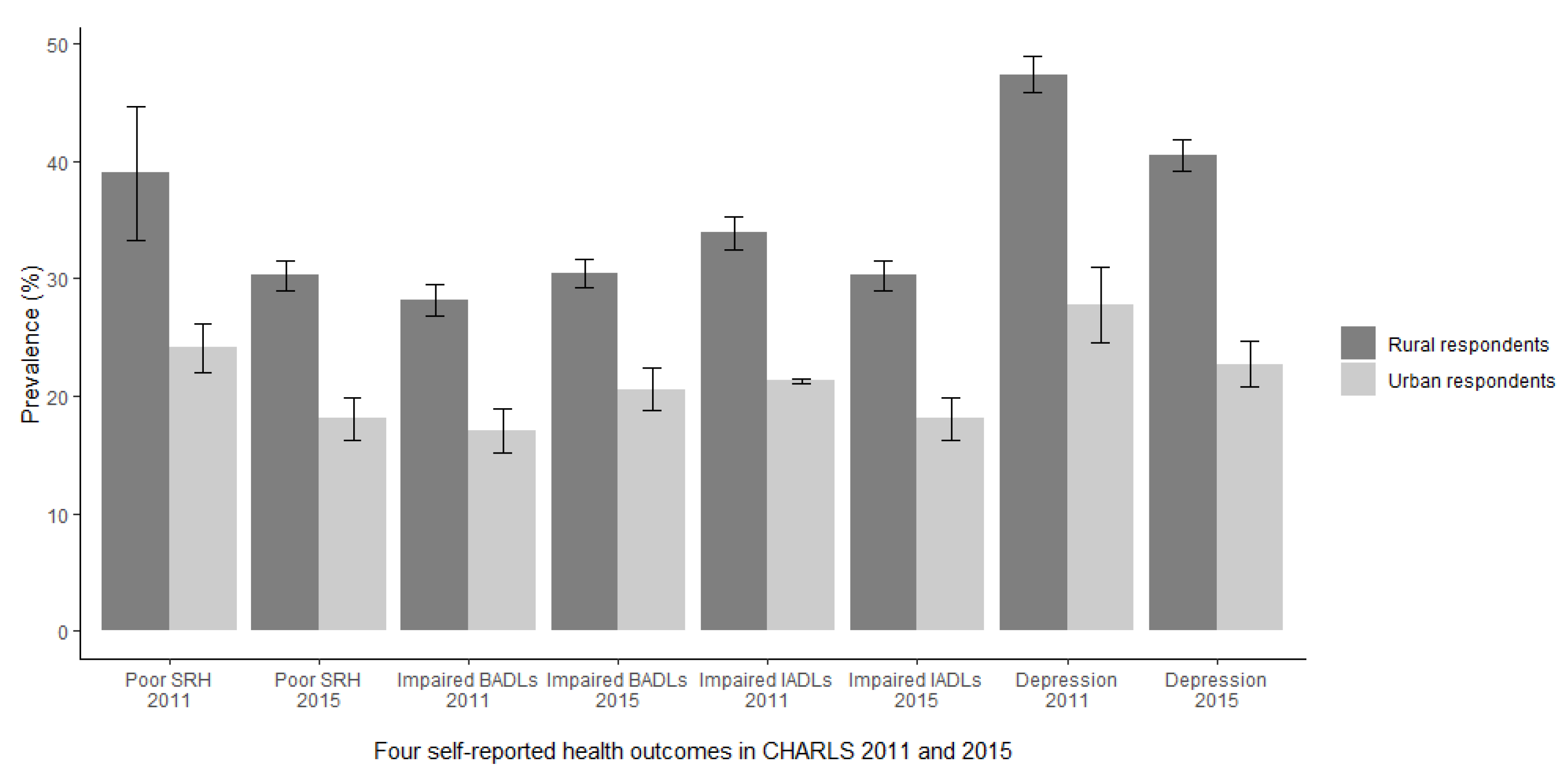
3.2. Prevalence of Health Outcomes in 2011 and 2015
3.3. Individual Characteristics
3.4. Prevalence of Poor SRH by Individual Characteristics
3.5. Prevalence of Impaired BADLs by Individual Characteristics
3.6. Prevalence of Impaired IADLs by Individual Characteristics
3.7. Prevalence of Self-Reported Depression by Individual Characteristics
3.8. Sociodemographic Determinants of Poor SRH, Self-Reported Functional Disabilities and Depression
4. Discussion
Strengths and Limitations of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CHARLS | China Health and Retirement Longitudinal Study |
| SRH | Self-Rated Health |
| BADLs | Basic Activities of Daily Living |
| IADLs | Instrumental Activities of Daily Living |
| CNY | Chinese Yuan |
| OR | Odds Ratio |
| SD | Standard Deviation |
References
- Williams, J.S.; Norström, F.; Ng, N. Disability and ageing in China and India—Decomposing the effects of gender and residence. Results from the WHO study on global ageing and adult health (SAGE). BMC Geriatr. 2017, 17, 197. [Google Scholar] [CrossRef]
- Liang, Y.; Welmer, A.-K.; Wang, R.; Song, A.; Fratiglioni, L.; Qiu, C. Trends in Incidence of Disability in Activities of Daily Living in Chinese Older Adults: 1993–2006. J. Am. Geriatr. Soc. 2017, 65, 306–312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zimmer, Z.; Kwong, J. Socioeconomic status and health among older adults in rural and urban China. J. Aging Health 2004, 16, 44–70. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Goza, F.W. Who will care for the elderly in China? A review of the problems caused by China’s one-child policy and their potential solutions. J. Aging Stud. 2006, 20, 151–164. [Google Scholar] [CrossRef]
- Sun, S.; Chen, J.; Johannesson, M.; Kind, P.; Xu, L.; Zhang, Y.; Burström, K. Regional differences in health status in China: Population health-related quality of life results from the National Health Services Survey 2008. Health Place 2011, 17, 671–680. [Google Scholar] [CrossRef] [Green Version]
- Chan, K.W. The household registration system and migrant labor in China: Notes on a debate. Popul. Dev. Rev. 2010, 36, 357–364. [Google Scholar] [CrossRef]
- Lu, Y. Does hukou still matter? The household registration system and its impact on social stratification and mobility in China. Soc. Sci. China 2008, 29, 56–75. [Google Scholar] [CrossRef]
- Liu, H.; Rizzo, J.A.; Fang, H. Urban-rural disparities in child nutrition-related health outcomes in China: The role of hukou policy. BMC Public Health 2015, 15, 1159. [Google Scholar] [CrossRef] [Green Version]
- Chan, K.W.; Zhang, L. The “hukou” system and rural-urban migration in China: Processes and changes. China Q. 1996, 160, 818–855. [Google Scholar] [CrossRef] [Green Version]
- Song, Q.; Smith, J.P. Hukou system, mechanisms, and health stratification across the life course in rural and urban China. Health Place 2019, 58, 102150. [Google Scholar] [CrossRef]
- Dorélien, A.; Xu, H. Estimating rural–urban disparities in self-rated health in China: Impact of choice of urban definition. Demogr. Res. 2020, 43, 1429–1460. [Google Scholar] [CrossRef]
- The 14th Five-Year Plan (2021–2025) for National Economic and Social Development and the Long-Range Objectives through the Year 2035. Available online: http://www.gov.cn/zhengce/2020-11/03/content_5556991.htm (accessed on 3 November 2020). (In Chinese)
- Bernard, S.L.; Kincade, J.E.; Konrad, T.R.; Arcury, T.A.; Rabiner, D.J.; Woomert, A.; DeFriese, G.H.; Ory, M.G. Predicting mortality from community surveys of older adults: The importance of self-rated functional ability. J. Gerontol. B. Psychol. Sci. Soc. Sci. 1997, 52, S155–S163. [Google Scholar] [CrossRef] [Green Version]
- Bowling, A.; Iliffe, S. Psychological approach to successful ageing predicts future quality of life in older adults. Health Qual. Life Outcome 2011, 9, 13. [Google Scholar] [CrossRef] [Green Version]
- Phelan, E.A.; Anderson, L.A.; LaCroix, A.Z.; Larson, E.B. Older adults’ views of “successful aging”—How do they compare with researchers’ definitions? J. Am. Geriatr. Soc. 2004, 52, 211–216. [Google Scholar] [CrossRef]
- McPhee, J.S.; French, D.P.; Jackson, D.; Nazroo, J.; Pendleton, N.; Degens, H. Physical activity in older age: Perspectives for healthy ageing and frailty. Biogerontology 2016, 17, 567–580. [Google Scholar] [CrossRef]
- Magaziner, J.; Cadigan, D.A.; Hebel, J.R.; Parry, R.E. Health and living arrangements among older women: Does living alone increase the risk of illness? J. Gerontol. 1988, 43, M127–M133. [Google Scholar] [CrossRef]
- Sereny, M. Living Arrangements of Older Adults in China: The Interplay among Preferences, Realities, and Health. Res. Aging 2011, 33, 172–204. [Google Scholar] [CrossRef]
- Hawton, A.; Green, C.; Dickens, A.P.; Richards, S.H.; Taylor, R.S.; Edwards, R.; Greaves, C.J.; Campbell, J.L. The impact of social isolation on the health status and health-related quality of life of older people. Qual. Life Res. 2011, 20, 57–67. [Google Scholar] [CrossRef] [PubMed]
- Silverstein, M.; Cong, Z.; Li, S. Intergenerational transfers and living arrangements of older people in rural China: Consequences for psychological well-being. J. Gerontol. B. Psychol. Sci. Soc. Sci. 2006, 61, S256–S266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Woolf, S.H.; Braveman, P. Where health disparities begin: The role of social and economic determinants—And why current policies may make matters worse. Health Affair. 2011, 30, 1852–1859. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, K.V.; Goldman, N. Socioeconomic differences in health among older adults in Mexico. Soc. Sci. Med. 2007, 65, 1372–1385. [Google Scholar] [CrossRef] [Green Version]
- Zhao, Y.; Hu, Y.; Smith, J.P.; Strauss, J.; Yang, G. Cohort profile: The China Health and Retirement Longitudinal Study (CHARLS). Int. J. Epidemiol. 2014, 43, 61–68. [Google Scholar] [CrossRef] [Green Version]
- Sun, S.; Chen, J.; Johannesson, M.; Kind, P.; Xu, L.; Zhang, Y.; Burström, K. Population health status in China: EQ-5D results, by age, sex and socio-economic status, from the National Health Services Survey 2008. Qual. Life Res. 2011, 20, 309–320. [Google Scholar] [CrossRef] [Green Version]
- Dowd, J.B.; Zajacova, A. Does self-rated health mean the same thing across socioeconomic groups? Evidence from biomarker data. Ann. Epidemiol. 2010, 20, 743–749. [Google Scholar] [CrossRef] [Green Version]
- Jylhä, M. What is self-rated health and why does it predict mortality? Towards a unified conceptual model. Soc. Sci. Med. 2009, 69, 307–316. [Google Scholar] [CrossRef]
- Katz, S. Assessing self-maintenance: Activities of daily living, mobility, and instrumental activities of daily living. J. Am. Geriatr. Soc. 1983, 31, 721–727. [Google Scholar] [CrossRef]
- Danan, G.; Research, Z.Y.J.D. Sociodemographic Effects on the Onset and Recovery of ADL Disability among Chinese Oldest-old. Demogr. Res. 2004, 11, 1–42. [Google Scholar] [CrossRef]
- Lawton, M.P.; Brody, E.M. Assessment of older people: Self-maintaining and instrumental activities of daily living. Gerontologist 1969, 9, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Graf, C. The Lawton instrumental activities of daily living scale. Am. J. Nurs. 2008, 108, 52–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andresen, E.M.; Malmgren, J.A.; Carter, W.B.; Patrick, D.L. Screening for depression in well older adults: Evaluation of a short form of the CES-D (Center for Epidemiologic Studies Depression Scale). Am. J. Prev. Med. 1994, 10, 77–84. [Google Scholar] [CrossRef]
- Chapman, D.G.; Nam, J.M. Asymptotic power of chi square tests for linear trends in proportions. Biometrics 1968, 24, 315–327. [Google Scholar] [CrossRef]
- Stutzer, A.; Frey, B.S. Does marriage make people happy, or do happy people get married? J. Socio-Econ. 2006, 35, 326–347. [Google Scholar] [CrossRef] [Green Version]
- Goodwin, J.S.; Hunt, W.C.; Key, C.R.; Samet, J.M. The effect of marital status on stage, treatment, and survival of cancer patients. JAMA 1987, 258, 3125–3130. [Google Scholar] [CrossRef]
- Gui, S.; Chen, J. Average life expectancy of the Chinese population in 1949–2019: Trends, contributors and prospects. China Popul. Dev. Stud. 2020, 3, 142–153. [Google Scholar] [CrossRef]
- Bowling, A. The concepts of successful and positive ageing. Fam. Pract. 1993, 10, 449–453. [Google Scholar] [CrossRef] [PubMed]
- Iwarsson, S.; Isacsson, Å.; Lanke, J. ADL dependence in the elderly population living in the community: The influence of functional limitations and physical environmental demand. Occup. Ther. Int. 1998, 5, 173–193. [Google Scholar] [CrossRef]
- Johnson, J.K.; Lui, L.Y.; Yaffe, K. Executive function, more than global cognition, predicts functional decline and mortality in elderly women. J. Gerontol. A. Biol. Sci. Med. Sci. 2007, 62, 1134–1141. [Google Scholar] [CrossRef] [Green Version]
- Gubhaju, B.; Østbye, T.; Chan, A. Living arrangements of community-dwelling older Singaporeans: Predictors and consequences. Ageing Soc. 2017, 38, 1174–1198. [Google Scholar] [CrossRef]
- Katz, S.; Ford, A.B.; Moskowitz, R.W.; Jackson, B.A.; Jaffe, M.W. Studies of Illness in the Aged: The Index of ADL: A Standardized Measure of Biological and Psychosocial Function. JAMA 1963, 185, 914–919. [Google Scholar] [CrossRef] [PubMed]
- Ouchi, Y.; Kato, Y.; Nakai, M.; Ishikawa, H.; Nakamura, K.; Nakatsuka, M.; Kasai, M.; Tanaka, N.; Meguro, K. Scope (quantitative) and performance (qualitative) of instrumental ADLs in older adults with mild cognitive impairment: Difference between very mild Alzheimer’s disease and very mild subcortical vascular dementia—The Kurihara Project. Alzheimer’s Dement. 2012, 8, P318. [Google Scholar] [CrossRef]
- Martin, L.G.; Feng, Q.; Schoeni, R.F.; Zeng, Y. Trends in Functional and Activity Limitations among Chinese Oldest-Old, 1998 to 2008. Popul. Dev. Rev. 2014, 40, 475–495. [Google Scholar] [CrossRef] [Green Version]
- Fitz, A.G.; Teri, L. Depression, cognition, and functional ability in patients with Alzheimer’s disease. J. Am. Geriatr. Soc. 1994, 42, 186–191. [Google Scholar] [CrossRef]
- Purtle, J.; Nelson, K.L.; Yang, Y.; Langellier, B.; Stankov, I.; Roux, A.V.D. Urban-Rural Differences in Older Adult Depression: A Systematic Review and Meta-analysis of Comparative Studies. Am. J. Prev. Med. 2019, 56, 603–613. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fulbright, S.A. Rates of depression and participation in senior centre activities in community-dwelling older persons. J. Psychiatr. Ment. Health Nurs. 2010, 17, 385–391. [Google Scholar] [CrossRef] [PubMed]
- World Bank. World Bank in China. Available online: https://www.worldbank.org/en/country/china/overview (accessed on 4 May 2021).
- Marmot, M. The Influence of Income on Health: Views of an Epidemiologist. Health Aff. 2002, 21, 31–46. [Google Scholar] [CrossRef] [PubMed]
- Babones, S. Income, education, and class gradients in health in global perspective. Health Sociol. Rev. 2010, 19, 130–143. [Google Scholar] [CrossRef]
- Bartram, J.; Lewis, K.; Lenton, R.; Wright, A. Focusing on improved water and sanitation for health. Lancet 2005, 365, 810–812. [Google Scholar] [CrossRef]
- Zhao, L.; Guo, Y.; Shao, T. Can the minimum living standard guarantee scheme enable the poor to escape the poverty trap in rural China? Int. J. Soc. Welf. 2017, 26, 314–328. [Google Scholar] [CrossRef]
- Benjamin, D.; Brandt, L.; Giles, J. The evolution of income inequality in rural China. Econ. Dev. Cult. Chang. 2005, 53, 769–824. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Hukou Registration | Living Area | CHARLS 2011 (n = 7616) | CHARLS 2015 (n = 9594) | ||
|---|---|---|---|---|---|
| n | % | n | % | ||
| Rural Hukou | Rural area | 4391 | 76.3 | 5385 | 74.3 |
| Urban area | 1364 | 23.7 | 1860 | 25.7 | |
| Urban Hukou | Rural area | 204 | 11.0 | 338 | 14.4 |
| Urban area | 1657 | 89.0 | 2011 | 85.6 | |
| Living Area | Hukou Registration | Poor SRH a | Impaired BADLs b | Impaired IADLs c | Depression | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| % | p * | % | p * | % | p * | % | p * | |||
| CHARLS 2011 | Total | 34.0 | 25.1 | 30.1 | 41.5 | |||||
| Rural area | Rural Hukou | 39.0 | <0.001 | 28.2 | 0.936 | 33.9 | <0.001 | 47.4 | <0.001 | |
| Urban Hukou | 26.1 | 27.7 | 18.8 | 27.0 | ||||||
| Urban area | Rural Hukou | 30.7 | <0.001 | 24.4 | <0.001 | 29.9 | <0.001 | 41.3 | <0.001 | |
| Urban Hukou | 24.1 | 17.1 | 21.3 | 27.8 | ||||||
| CHARLS 2015 | Total | 26.3 | 27.3 | 29.7 | 35.2 | |||||
| Rural area | Rural Hukou | 30.3 | <0.001 | 30.5 | 0.012 | 33.6 | <0.001 | 40.5 | 0.005 | |
| Urban Hukou | 24.2 | 24.0 | 24.0 | 32.6 | ||||||
| Urban area | Rural Hukou | 23.6 | <0.001 | 25.9 | <0.001 | 28.9 | <0.001 | 33.4 | <0.001 | |
| Urban Hukou | 18.1 | 20.6 | 20.8 | 22.7 | ||||||
| CHARLS 2011 (n = 6048) | CHARLS 2015 (n = 7396) | |||||
|---|---|---|---|---|---|---|
| Rural (n = 4391) | Urban (n = 1657) | p | Rural (n = 5385) | Urban (n = 2011) | p | |
| % | % | % | % | |||
| Age (mean ± SD a, years) | 68.3 ± 7.0 | 69.0 ± 7.0 | 0.001 * | 68.6 ± 7.2 | 69.2 ± 7.2 | 0.001 * |
| Age group (years) | 0.009 ** | 0.001 ** | ||||
| 60–64 | 38.3 | 34.3 | 35.8 | 32.7 | ||
| 65–69 | 24.6 | 23.2 | 26.9 | 26.3 | ||
| 70–74 | 17.3 | 20.0 | 17.7 | 17.3 | ||
| 75–79 | 11.4 | 13.7 | 10.5 | 14.2 | ||
| 80–84 | 5.7 | 6.3 | 5.9 | 6.3 | ||
| 85–89 | 2.0 | 2.1 | 2.5 | 2.5 | ||
| 90+ | 0.6 | 0.5 | 0.8 | 0.7 | ||
| Sex | 0.111 *** | 0.006 *** | ||||
| Male | 49.6 | 51.9 | 48.3 | 51.9 | ||
| Female | 50.4 | 48.1 | 51.7 | 48.1 | ||
| Marital status | <0.001 *** | <0.001 *** | ||||
| Married | 76.7 | 81.1 | 77.3 | 81.6 | ||
| Unmarried | 23.3 | 18.9 | 22.7 | 18.4 | ||
| Living arrangement | <0.001 *** | 0.234 *** | ||||
| Not living alone | 90.5 | 86.3 | 91.1 | 91.9 | ||
| Living alone | 9.5 | 13.7 | 8.9 | 8.1 | ||
| Living near children | <0.001 ** | 0.818 *** | ||||
| Living near children | 90.9 | 91.9 | 87.4 | 87.9 | ||
| Not living near children | 6.9 | 4.7 | 10.5 | 10.2 | ||
| No child | 2.2 | 3.4 | 2.0 | 1.8 | ||
| Educational level | <0.001 ** | <0.001 ** | ||||
| Below primary school | 67.2 | 26.6 | 64.9 | 22.0 | ||
| Primary school | 23.5 | 23.9 | 22.8 | 27.5 | ||
| Middle school | 7.8 | 24.6 | 9.8 | 26.0 | ||
| High school | 1.5 | 16.5 | 2.4 | 17.3 | ||
| College and above | 0.1 | 8.3 | 0.1 | 7.2 | ||
| Income (mean, CNY b) | 4126 | 18,846 | <0.001 * | 5294 | 20,979 | <0.001 * |
| Income group | <0.001 ** | <0.001 ** | ||||
| First group (low) | 21.0 | 4.0 | 10.4 | 5.3 | ||
| Second group | 22.8 | 2.2 | 11.8 | 1.3 | ||
| Third group | 20.2 | 6.1 | 11.9 | 1.9 | ||
| Fourth group | 13.9 | 18.9 | 10.0 | 7.0 | ||
| Fifth group (high) | 6.2 | 50.2 | 4.1 | 24.4 | ||
| Missing | 15.9 | 18.7 | 51.8 | 60.1 | ||
| CHARLS 2011 (n = 6003) | CHARLS 2015 (n = 6844) | |||||
|---|---|---|---|---|---|---|
| Rural (n = 4370) | Urban (n = 1633) | p * | Rural (n = 5018) | Urban (n = 1826) | p * | |
| Total | 39.0 | 24.1 | <0.001 | 30.3 | 18.1 | <0.001 |
| Age group (years) | ||||||
| 60–64 | 35.5 | 20.0 | <0.001 | 27.1 | 16.8 | <0.001 |
| 65–69 | 35.9 | 26.6 | 0.001 | 30.7 | 14.8 | <0.001 |
| 70–74 | 42.0 | 26.1 | <0.001 | 32.2 | 22.4 | 0.001 |
| 75–79 | 45.3 | 24.4 | <0.001 | 36.9 | 21.2 | <0.001 |
| 80–84 | 48.0 | 27.5 | 0.001 | 29.7 | 17.3 | 0.016 |
| 85–89 | 57.5 | 30.3 | 0.013 | 38.8 | 28.1 | 0.282 |
| 90+ | 40.7 | 37.5 | 1.000 | 26.7 | 16.7 | 1.000 |
| Sex | ||||||
| Male | 35.5 | 21.4 | <0.001 | 27.9 | 15.9 | <0.001 |
| Female | 42.4 | 27.1 | <0.001 | 32.6 | 20.5 | <0.001 |
| Marital status | ||||||
| Married | 38.1 | 24.3 | <0.001 | 28.7 | 17.5 | <0.001 |
| Unmarried | 42.0 | 23.3 | <0.001 | 36.4 | 21.2 | <0.001 |
| Living arrangement | ||||||
| Not living alone | 39.1 | 24.3 | <0.001 | 30.3 | 18.0 | <0.001 |
| Living alone | 38.2 | 22.7 | <0.001 | 30.2 | 20.3 | 0.024 |
| Living near children | ||||||
| Living near children | 39.0 | 24.0 | <0.001 | 30.6 | 18.2 | <0.001 |
| Not living near children | 39.2 | 23.1 | 0.008 | 26.8 | 16.9 | 0.007 |
| No child | 38.7 | 29.4 | 0.265 | 38.3 | 25.0 | 0.225 |
| Educational level | ||||||
| Below primary school | 41.9 | 31.4 | <0.001 | 32.2 | 23.8 | 0.001 |
| Primary school | 35.0 | 26.9 | 0.004 | 28.0 | 18.1 | <0.001 |
| Middle school | 29.1 | 20.3 | 0.006 | 26.5 | 16.0 | <0.001 |
| High school | 29.2 | 18.1 | 0.045 | 19.8 | 16.6 | 0.419 |
| College and above | 0.0 | 16.2 | 1.000 | 0.0 | 13.1 | 0.344 |
| Income group | ||||||
| First group (low) | 45.4 | 39.4 | 0.344 | 33.2 | 21.7 | 0.020 |
| Second group | 41.6 | 36.1 | 0.524 | 31.3 | 26.9 | 0.638 |
| Third group | 35.9 | 33.7 | 0.652 | 32.2 | 34.2 | 0.801 |
| Fourth group | 32.8 | 25.9 | 0.029 | 28.0 | 25.5 | 0.561 |
| Fifth group (high) | 27.7 | 20.9 | 0.020 | 14.8 | 12.8 | 0.475 |
| Missing | 40.7 | 23.3 | <0.001 | 30.8 | 18.5 | <0.001 |
| Model 1 | Model 2 | Model 3 | Model 4 | Model 5 | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | OR | 95% CI | OR | 95% CI | OR | 95% CI | OR | 95% CI | |
| Rural respondents a | 2.05 | 1.80–2.33 | 2.04 | 1.79–2.32 | 1.66 | 1.43–1.92 | 1.55 | 1.32–1.81 | 1.34 | 1.13–1.58 |
| Marital status b | ||||||||||
| Unmarried | — | — | 0.99 | 0.84–1.16 | 0.97 | 0.83–1.14 | 0.99 | 0.84–1.17 | 0.98 | 0.83–1.15 |
| Living arrangement c | ||||||||||
| Living alone | — | — | 0.81 | 0.65–1.00 | 0.80 | 0.65–0.99 | 0.74 | 0.59–0.92 | 0.74 | 0.59–0.92 |
| Living near children d | ||||||||||
| Not living near children | — | — | 1.10 | 0.88–1.37 | 1.10 | 0.89–1.38 | 1.07 | 0.85–1.33 | 1.07 | 0.86–1.34 |
| No child | — | — | 1.25 | 0.87–1.79 | 1.23 | 0.86–1.76 | 1.26 | 0.88–1.81 | 1.29 | 0.87–1.79 |
| Educational level e | ||||||||||
| Primary school | — | — | — | — | 0.85 | 0.74–0.98 | — | — | 0.86 | 0.75–0.99 |
| Middle school | — | — | — | — | 0.66 | 0.54–0.80 | — | — | 0.69 | 0.56–0.84 |
| High school | — | — | — | — | 0.57 | 0.43–0.77 | — | — | 0.63 | 0.46–0.85 |
| College and above | — | — | — | — | 0.45 | 0.28–0.72 | — | — | 0.49 | 0.30–0.80 |
| Income group f | ||||||||||
| Second group | — | — | — | — | — | — | 0.87 | 0.73–1.04 | 0.87 | 0.73–1.04 |
| Third group | — | — | — | — | — | — | 0.71 | 0.59–0.85 | 0.71 | 0.59–0.85 |
| Fourth group | — | — | — | — | — | — | 0.62 | 0.52–0.76 | 0.63 | 0.52–0.76 |
| Fifth group (high) | — | — | — | — | — | — | 0.48 | 0.39–0.60 | 0.52 | 0.42–0.65 |
| Missing | — | — | — | — | — | — | 0.76 | 0.63–0.92 | 0.78 | 0.64–0.94 |
| Model 1 | Model 2 | Model 3 | ||||
|---|---|---|---|---|---|---|
| OR | 95% CI | OR | 95% CI | OR | 95% CI | |
| Rural respondents a | 2.00 | 1.75–2.28 | 1.98 | 1.73–2.26 | 1.74 | 1.49–2.02 |
| Marital status b | ||||||
| Unmarried | — | — | 1.42 | 1.21–1.67 | 1.40 | 1.19–1.65 |
| Living arrangement c | ||||||
| Living alone | — | — | 0.68 | 0.54–0.85 | 0.68 | 0.53–0.85 |
| Living near children d | ||||||
| Not living near children | — | — | 0.94 | 0.79–1.13 | 0.95 | 0.79–1.14 |
| No child | — | — | 1.56 | 1.05–2.31 | 1.52 | 1.02–2.26 |
| Educational level e | ||||||
| Primary school | — | — | — | — | 0.85 | 0.74–0.98 |
| Middle school | — | — | — | — | 0.81 | 0.67–0.97 |
| High school | — | — | — | — | 0.71 | 0.54–0.94 |
| College and above | — | — | — | — | 0.53 | 0.31–0.91 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jiang, H.; Burström, B.; Chen, J.; Burström, K. Rural–Urban Inequalities in Poor Self-Rated Health, Self-Reported Functional Disabilities, and Depression among Chinese Older Adults: Evidence from the China Health and Retirement Longitudinal Study 2011 and 2015. Int. J. Environ. Res. Public Health 2021, 18, 6557. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18126557
Jiang H, Burström B, Chen J, Burström K. Rural–Urban Inequalities in Poor Self-Rated Health, Self-Reported Functional Disabilities, and Depression among Chinese Older Adults: Evidence from the China Health and Retirement Longitudinal Study 2011 and 2015. International Journal of Environmental Research and Public Health. 2021; 18(12):6557. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18126557
Chicago/Turabian StyleJiang, Haiting, Bo Burström, Jiaying Chen, and Kristina Burström. 2021. "Rural–Urban Inequalities in Poor Self-Rated Health, Self-Reported Functional Disabilities, and Depression among Chinese Older Adults: Evidence from the China Health and Retirement Longitudinal Study 2011 and 2015" International Journal of Environmental Research and Public Health 18, no. 12: 6557. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18126557