
The Impact of Different Types of Shift Work on Blood Pressure and Hypertension: A Systematic Review and Meta-Analysis

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search and Selection
2.2. Inclusion Criteria
2.3. Data Extraction
2.4. Methodologic Quality Assessment
2.5. Data Analysis
3. Results
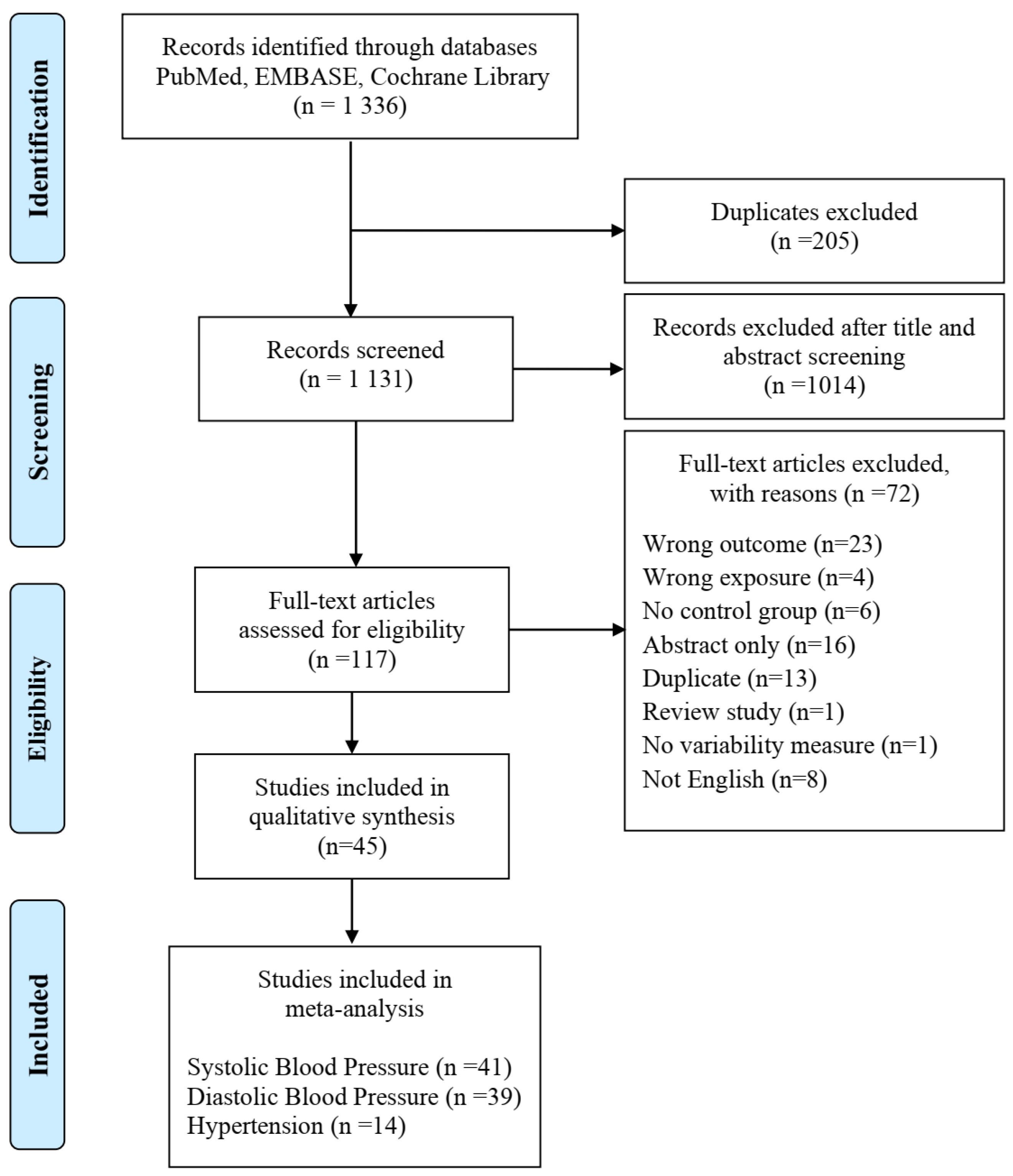
3.1. Search Results
3.2. Study Characteristics
3.3. Risk of Bias
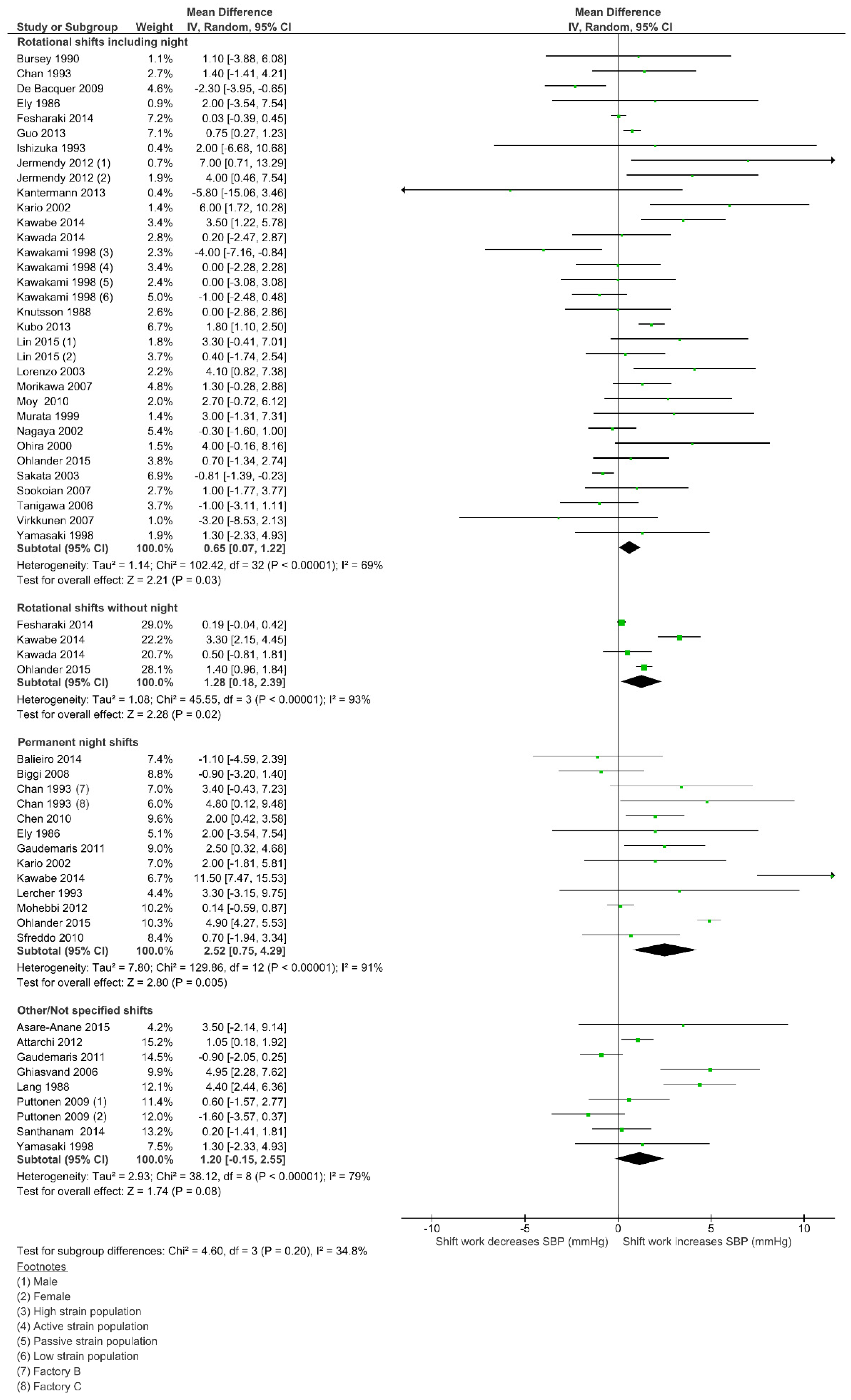
3.4. Effect of Shift Work on Systolic Blood Pressure (SBP)
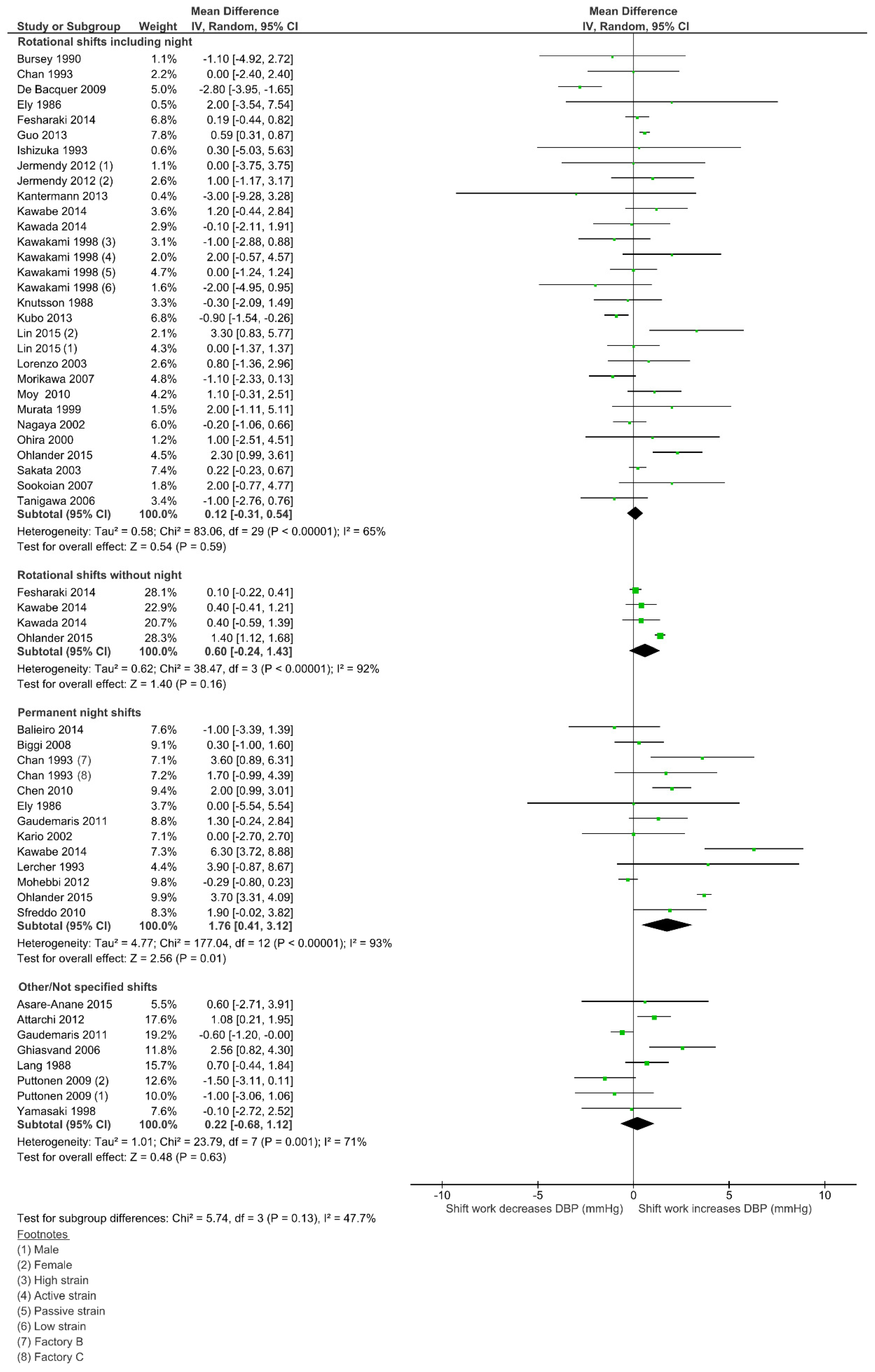
3.5. Effect of Shift Work on Diastolic Blood Pressure (DBP)
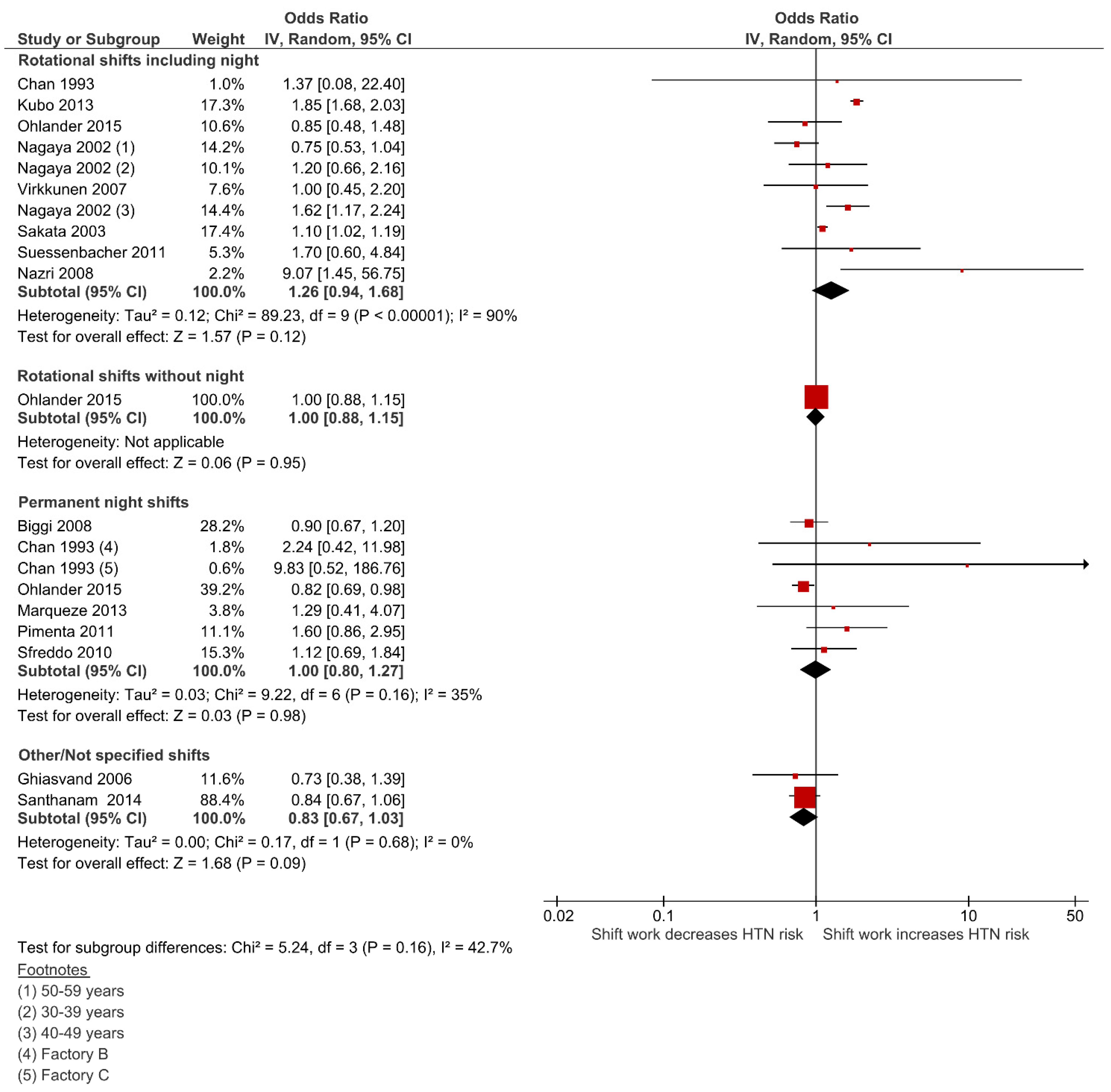
3.6. Effect of Shift Work on Hypertension (HTN)
4. Discussion
4.1. Main Findings
4.2. Overall Limitations of Included Studies
4.3. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the Management of Arterial Hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef]
- Flint, A.C.; Conell, C.; Ren, X.; Banki, N.M.; Chan, S.L.; Rao, V.A.; Melles, R.B.; Bhatt, D.L. Effect of Systolic and Diastolic Blood Pressure on Cardiovascular Outcomes. N. Engl. J. Med. 2019, 381, 243–251. [Google Scholar] [CrossRef]
- Ettehad, D.; Emdin, C.A.; Kiran, A.; Anderson, S.G.; Callender, T.; Emberson, J.; Chalmers, J.; Rodgers, A.; Rahimi, K. Blood Pressure Lowering for Prevention of Cardiovascular Disease and Death: A Systematic Review and Meta-Analysis. Lancet 2016, 387, 957–967. [Google Scholar] [CrossRef] [Green Version]
- Piepoli, M.F.; Hoes, A.W.; Agewall, S.; Albus, C.; Brotons, C.; Catapano, A.L.; Cooney, M.-T.; Corrà, U.; Cosyns, B.; Deaton, C.; et al. 2016 European Guidelines on Cardiovascular Disease Prevention in Clinical Practice. Eur. Heart J. 2016, 37, 2315–2381. [Google Scholar] [CrossRef] [PubMed]
- Messenger, J. Working Time and the Future of Work; International Labour Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Manohar, S.; Thongprayoon, C.; Cheungpasitporn, W.; Mao, M.A.; Herrmann, S.M. Associations of Rotational Shift Work and Night Shift Status with Hypertension: A Systematic Review and Meta-Analysis. J. Hypertens. 2017, 35, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Herzog, R.; Álvarez-Pasquin, M.J.; Díaz, C.; del Barrio, J.L.; Estrada, J.M.; Gil, Á. Are Healthcare Workers’ Intentions to Vaccinate Related to Their Knowledge, Beliefs and Attitudes? A Systematic Review. BMC Public Health 2013, 13, 154. [Google Scholar] [CrossRef] [Green Version]
- Luchini, C.; Stubbs, B.; Solmi, M.; Veronese, N. Assessing the Quality of Studies in Meta-Analyses: Advantages and Limitations of the Newcastle Ottawa Scale. World J. Meta Anal. 2017, 5, 80. [Google Scholar] [CrossRef]
- Torquati, L.; Mielke, G.I.; Brown, W.J.; Kolbe-Alexander, T. Shift Work and the Risk of Cardiovascular Disease. A Systematic Review and Meta-Analysis Including Dose–Response Relationship. Scand. J. Work Environ. Health 2018, 44, 229–238. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.T.; Green, S. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available online: www.handbook.cochrane.org (accessed on 5 June 2021).
- Lau, J.; Ioannidis, J.P.A.; Schmid, C.H. Quantitative Synthesis in Systematic Reviews. Ann. Intern. Med. 1997, 127, 820–826. [Google Scholar] [CrossRef]
- Bray, E.P.; Holder, R.; Mant, J.; McManus, R.J. Does Self-Monitoring Reduce Blood Pressure? Meta-Analysis with Meta-Regression of Randomized Controlled Trials. Ann. Med. 2010, 42, 371–386. [Google Scholar] [CrossRef] [PubMed]
- Asare-Anane, H.; Abdul-Latif, A.; Ofori, E.K.; Abdul-Rahman, M.; Amanquah, S.D. Shift Work and the Risk of Cardiovascular Disease among Workers in Cocoa Processing Company, Tema. BMC Res. Notes 2015, 8, 4–9. [Google Scholar] [CrossRef] [Green Version]
- Attarchi, M.; Dehghan, F.; Safakhah, F.; Nojomi, M.; Mohammadi, S. Effect of Exposure to Occupational Noise and Shift Working on Blood Pressure in Rubber Manufacturing Company Workers. Ind. Health 2012, 50, 205–213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balieiro, L.C.; Rossato, L.T.; Waterhouse, J.; Paim, S.L.; Mota, M.C.; Crispim, C.A. Nutritional Status and Eating Habits of Bus Drivers during the Day and Night. Chronobiol. Int. 2014, 31, 1123–1129. [Google Scholar] [CrossRef] [PubMed]
- Biggi, N.; Consonni, D.; Galluzzo, V.; Sogliani, M.; Costa, G. Metabolic Syndrome in Permanent Night Workers. Chronobiol. Int. 2008, 25, 443–454. [Google Scholar] [CrossRef]
- Bursey, R.G. A Cardiovascular Study of Shift Workers with Respect to Coronary Artery Disease Risk Factor Prevalence. J. Soc. Occup. Med. 1990, 40, 65–67. [Google Scholar] [CrossRef] [PubMed]
- Chan, O.Y.; Gan, S.L.; Yeo, M.H. Study on the Health of Female Electronics Workers on 12 Hour Shifts. Occup. Med. 1993, 43, 143–148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, J.D.; Lin, Y.C.; Hsiao, S.T. Obesity and High Blood Pressure of 12-Hour Night Shift Female Clean-Room Workers. Chronobiol. Int. 2010, 27, 334–344. [Google Scholar] [CrossRef]
- De Bacquer, D.; van Risseghem, M.; Clays, E.; Kittel, F.; de Backer, G.; Braeckman, L. Rotating Shift Work and the Metabolic Syndrome: A Prospective Study. Int. J. Epidemiol. 2009, 38, 848–854. [Google Scholar] [CrossRef] [Green Version]
- De Gaudemaris, R.; Levant, A.; Ehlinger, V.; Hérin, F.; Lepage, B.; Soulat, J.M.; Sobaszek, A.; Kelly-Irving, M.; Lang, T. Blood Pressure and Working Conditions in Hospital Nurses and Nursing Assistants. The ORSOSA Study. Arch. Cardiovasc. Dis. 2011, 104, 97–103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Lorenzo, L.; de Pergola, G.; Zocchetti, C.; L’Abbate, N.; Basso, A.; Pannacciulli, N.; Cignarelli, M.; Giorgino, R.; Soleo, L. Effect of Shift Work on Body Mass Index: Results of a Study Performed in 319 Glucose-Tolerant Men Working in a Southern Italian Industry. Int. J. Obes. 2003, 27, 1353–1358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ely, D.L.; Mostardi, R.A. The Effect of Recent Life Events Stress, Life Assets, and Temperament Pattern on Cardiovascular Risk Factors for Akron City Police Officers. J. Hum. Stress 1986, 12, 77–91. [Google Scholar] [CrossRef]
- Ohlander, J.; Keskin, M.C.; Stork, J.; Radon, K. Shift Work and Hypertension: Prevalence and Analysis of Disease Pathways in a German Car Manufacturing Company. Am. J. Ind. Med. 2015, 58, 549–560. [Google Scholar] [CrossRef]
- Gholami-Fesharaki, M.; Kazemnejad, A.; Zayeri, F.; Rowzati, M.; Sanati, J.; Akbari, H. Multicenter Historical Cohort Study of the Relationship between Shift Work and Blood Pressure. ARYA Atheroscler. 2014, 10, 287–291. [Google Scholar]
- Guo, Y.; Liu, Y.; Huang, X.; Rong, Y.; He, M.; Wang, Y.; Yuan, J.; Wu, T.; Chen, W. The Effects of Shift Work on Sleeping Quality, Hypertension and Diabetes in Retired Workers. PLoS ONE 2013, 8, e71107. [Google Scholar] [CrossRef] [Green Version]
- Ghiasvand, M.; Heshmat, R.; Golpira, R.; Haghpanah, V.; Soleimani, A.; Shoushtarizadeh, P.; Tavangar, S.M.; Larijani, B. Shift Working and Risk of Lipid Disorders: A Cross-Sectional Study. Lipids Health Dis. 2006, 5, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ishizuka, T.; Furuya, Y. Influence of Meals and Night Shifts on Health. J. Med. Syst. 1993, 17, 201–206. [Google Scholar] [CrossRef]
- Jermendy, G.; Nadas, J.; Hegyi, I.; Vasas, I.; Hidvegi, T. Assessment of Cardiometabolic Risk among Shift Workers in Hungary. Health Qual. Life Outcomes 2012, 10, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kantermann, T.; Duboutay, F.; Haubruge, D.; Kerkhofs, M.; Schmidt-Trucksäss, A.; Skene, D.J. Atherosclerotic Risk and Social Jetlag in Rotating Shift-Workers: First Evidence from a Pilot Study. Work 2013, 46, 273–282. [Google Scholar] [CrossRef] [Green Version]
- Kawabe, Y.; Nakamura, Y.; Kikuchi, S.; Murakami, Y.; Tanaka, T.; Takebayashi, T.; Okayama, A.; Miura, K.; Okamura, T.; Ueshima, H. Relationship between Shift Work and Clustering of the Metabolic Syndrome Diagnostic Components. J. Atheroscler. Thromb. 2014, 21, 703–711. [Google Scholar] [CrossRef] [Green Version]
- Kawada, T.; Otsuka, T. Effect of Shift Work on the Development of Metabolic Syndrome After 3 Years in Japanese Male Workers. Arch. Environ. Occup. Health 2014, 69, 55–61. [Google Scholar] [CrossRef]
- Kawakami, N.; Haratani, T.; Araki, S. Job Strain and Arterial Blood Pressure, Serum Cholesterol, and Smoking as Risk Factors for Coronary Heart Disease in Japan. Int. Arch. Occup. Environ. Health 1998, 71, 429–432. [Google Scholar] [CrossRef] [PubMed]
- Knutsson, A.; Akerstedt, T.; Jonsson, B.G. Prevalence of Risk-Factors for Coronary-Artery Disease among Day and Shift Workers. Scand. J. Work Environ. Health 1988, 14, 317–321. [Google Scholar] [CrossRef]
- Kubo, T.; Fujino, Y.; Nakamura, T.; Kunimoto, M.; Tabata, H.; Tsuchiya, T.; Kadowaki, K.; Odoi, H.; Oyama, I.; Matsuda, S. An Industry-Based Cohort Study of the Association Between Weight Gain and Hypertension Risk Among Rotating Shift Workers. J. Occup. Environ. Med. 2013, 55, 1041–1045. [Google Scholar] [CrossRef]
- Lang, T.; Pariente, P.; Salem, G.; Tap, D. Social, Professional Conditions and Arterial Hypertension: An Epidemiological Study in Dakar, Senegal. J. Hypertens. 1988, 6, 271–276. [Google Scholar] [CrossRef]
- Lercher, P.; Hortnagl, J.; Kofler, W.W. Work Noise Annoyance and Blood Pressure: Combined Effects with Stressful Working Conditions. Int. Arch. Occup. Environ. Health 1993, 65, 23–28. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.C.; Hsieh, I.C.; Chen, P.C. Utilizing the Metabolic Syndrome Component Count in Workers’ Health Surveillance: An Example of Day-Time vs. Day-Night Rotating Shift Workers. Int. J. Occup. Med. Environ. Health 2015, 28, 675–688. [Google Scholar] [CrossRef]
- Marqueze, E.C.; Ulhoa, M.A.; Moreno, C.R.C. Effects of Irregular-Shift Work and Physical Activit on Cardiovascular Risk Factors in Truck Drivers. Rev. Saude Publica 2013, 47, 497–505. [Google Scholar] [CrossRef]
- Nazri, S.M.; Tengku, M.A.; Winn, T. The Association of Shift Work and Hypertension among Male Factory Workers in Kota Bharu, Kelantan, Malaysia. Southeast Asian J. Trop. Med. Public Health 2008, 39, 176–183. [Google Scholar] [PubMed]
- Mohebbi, I.; Shateri, K.; Seyedmohammadzad, M. The Relationship between Working Schedule Patterns and the Markers of the Metabolic Syndrome: Comparison of Shift Workers with Day Workers. Int. J. Occup. Med. Environ. Health 2012, 25, 383–391. [Google Scholar] [CrossRef]
- Morikawa, Y.; Nakagawa, H.; Miura, K.; Soyama, Y.; Ishizaki, M.; Kido, T.; Naruse, Y.; Suwazono, Y.; Nogawa, K. Effect of Shift Work on Body Mass Index and Metabolic Parameters. Scand. J. Work Environ. Health 2007, 33, 45–50. [Google Scholar] [CrossRef] [PubMed]
- Moy, F.M.; Hoe, V.C.W.; Tan, C.P.L.; Rosmawati, M. Cardiovascular Risks among Shift and Non-Shift Workers in a Public Medical Centre in Kuala Lumpur. J. Health Transl. Med. 2010, 13, 45–49. [Google Scholar]
- Murata, K.; Yano, E.; Shinozaki, T. Impact of Shift Work on Cardiovascular Functions in a 10-Year Follow-up Study. Scand. J. Work Environ. Health 1999, 25, 272–277. [Google Scholar] [CrossRef]
- Nagaya, T.; Yoshida, H.; Takahashi, H.; Kawai, M. Markers of Insulin Resistance in Day and Shift Workers Aged 30-59 Years. Int. Arch. Occup. Environ. Health 2002, 75, 562–568. [Google Scholar] [CrossRef] [PubMed]
- Pimenta, A.M.; Kac, G.; e Souza, R.R.C.; de Barros Almeida Ferreira, L.M.; de Fátima Silqueira, S.M. Night-Shift Work and Cardiovascular Risk among Employees of a Public University. Rev. Assoc. Med. Bras. 2012, 58, 168–177. [Google Scholar] [CrossRef]
- Puttonen, S.; Kivimäki, M.; Elovainio, M.; Pulkki-Råback, L.; Hintsanen, M.; Vahtera, J.; Telama, R.; Juonala, M.; Viikari, J.S.A.; Raitakari, O.T.; et al. Shift Work in Young Adults and Carotid Artery Intima–Media Thickness: The Cardiovascular Risk in Young Finns Study. Atherosclerosis 2009, 205, 608–613. [Google Scholar] [CrossRef]
- Sakata, K.; Suwazono, Y.; Harada, H.; Okubo, Y.; Kobayashi, E.; Nogawa, K. The Relationship Between Shift Work and the Onset of Hypertension in Male Japanese Workers. J. Occup. Environ. Med. 2003, 45, 1002–1006. [Google Scholar] [CrossRef]
- Santhanam, P.; Driscoll, H.K.; Gress, T.W.; Khthir, R. Metabolic Disease and Shift Work: Is There an Association? An Analysis of NHANES Data for 2007–2008. Occup. Environ. Med. 2014, 71, 661–662. [Google Scholar] [CrossRef]
- Sfreddo, C.; Fuchs, S.C.; Merlo, A.R.; Fuchs, F.D. Shift Work Is Not Associated with High Blood Pressure or Prevalence of Hypertension. PLoS ONE 2010, 5, e15250. [Google Scholar] [CrossRef]
- Sookoian, S.; Gemma, C.; Fernández Gianotti, T.; Burgueño, A.; Alvarez, A.; González, C.D.; Pirola, C.J. Effects of Rotating Shift Work on Biomarkers of Metabolic Syndrome and Inflammation. J. Intern. Med. 2007, 261, 285–292. [Google Scholar] [CrossRef]
- Suessenbacher, A.; Potocnik, M.; Dörler, J.; Fluckinger, G.; Wanitschek, M.; Pachinger, O.; Frick, M.; Alber, H.F. Comparison of Peripheral Endothelial Function in Shift Versus Nonshift Workers. Am. J. Cardiol. 2011, 107, 945–948. [Google Scholar] [CrossRef]
- Tanigawa, T.; Muraki, I.; Umesawa, M.; Tachibana, N.; Noda, H.; Takahashi, M.; Mutou, K.; Kage, Y.; Smith, L.; Iso, H. Sleep-Disordered Breathing and Blood Pressure Levels Among Shift and Day Workers. Am. J. Hypertens. 2006, 19, 346–351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Virkkunen, H.; Härmä, M.; Kauppinen, T.; Tenkanen, L. Shift Work, Occupational Noise and Physical Workload with Ensuing Development of Blood Pressure and Their Joint Effect on the Risk of Coronary Heart Disease. Scand. J. Work Environ. Health 2007, 33, 425–434. [Google Scholar] [CrossRef] [Green Version]
- Yamasaki, F.; Schwartz, J.E.; Gerber, L.M.; Warren, K.; Pickering, T.G. Impact of Shift Work and Race/Ethnicity on the Diurnal Rhythm of Blood Pressure and Catecholamines. Hypertension 1998, 32, 417–423. [Google Scholar] [CrossRef] [Green Version]
- Ohira, T.; Tanigawa, T.; Iso, H.; Odagiri, Y.; Takamiya, T.; Shimomitsu, T.; Hayano, J.; Shimamoto, T. Effects of Shift Work on 24-Hour Ambulatory Blood Pressure and Its Variability among Japanese Workers. Scand. J. Work Environ. Health 2000, 26, 421–426. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kario, K.; Schwartz, J.E.; Gerin, W.; Robayo, N.; Maceo, E.; Pickering, T.G. Psychological and Physical Stress-Induced Cardiovascular Reactivity and Diurnal Blood Pressure Variation in Women with Different Work Shifts. Hypertens Res. 2002, 25, 543–551. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moreno, C.R.C.; Marqueze, E.C.; Sargent, C.; Wright, K.P., Jr.; Ferguson, S.A.; Tucker, P. Working Time Society Consensus Statements: Evidence-Based Effects of Shift Work on Physical and Mental Health. Ind. Health 2019, 57, 139–157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Makarem, N.; Shechter, A.; Carnethon, M.R.; Mullington, J.M.; Hall, M.H.; Abdalla, M. Sleep Duration and Blood Pressure: Recent Advances and Future Directions. Curr. Hypertens. Rep. 2019, 21. [Google Scholar] [CrossRef] [PubMed]
- Juda, M.; Vetter, C.; Roenneberg, T. Chronotype Modulates Sleep Duration, Sleep Quality, and Social Jet Lag in Shift-Workers. J. Biol. Rhythm. 2013, 28, 141–151. [Google Scholar] [CrossRef] [Green Version]
- Chellappa, S.L.; Vujovic, N.; Williams, J.S.; Scheer, F.A.J.L. Impact of Circadian Disruption on Cardiovascular Function and Disease. Trends Endocrinol. Metab. 2019, 30, 767–779. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author Year | Design | Country | Population | Sex | Shift Work | Sample Size (SWs/DWs) | Mean Age i (SWs/DWs) | Outcome | Outcome Adjustments | NOS |
|---|---|---|---|---|---|---|---|---|---|---|
| Asare-Anane 2015 [14] | CS | Ghana | cocoa industry | F&M | NS | 113/87 | 42.0/40.3 | SBP DBP | No | 4 |
| Attarchi 2012 [15] | CS | Iran | tire manufacturing factory | M | NS | 88/76 | 38.5/40.2 | * SBP * DBP | * age, BMI, smoking, salt, exercise, family HTN, job duration | 8 |
| Balieiro 2014 [16] | CS | Brazil | bus drivers | M | PN | 81/69 | 44.0/46.7 | SBP DBP | No | 4 |
| Biggi 2008 [17] | CH (76-07) | Italy | street cleaning and waste collection | M | PN | 331/157 | 47.0/42.3 | * HTN ** SBP ** DBP | * age, job company and branch, study period ** plus smoking and alcohol | 8 |
| Bursey 1990 [18] | CS | UK | nuclear fuel factory | M | R + N | 57/57 | 50/50 | SBP DBP | No | 5 |
| Chan 1993 [19] | CS | Singapore | electronics industry | F | R + N PN | R + N 55/75 PN B 73/63 PN C 58/59 | R + N 28/30 PN B,C NotR | SBP DBP HTN | No | 4 |
| Chen 2010 [20] | CS | Taiwan | semiconductor manufacturing | F | PN | 561/656 | 32.7/34.9 | SBP DBP | No | 4 |
| De Bacquer 2009 [21] | CS | Belgium | nine companies and public administration | M | R + N | 309/1220 | 44.7/43.1 | SBP DBP | No | 6 |
| Gaudemaris 2011 [22] | CS | France | nursing staff | F | PN NS | PN 149 NS 1802/1863 | NotR | SBP DBP | No | 6 |
| Di Lorenzo 2003 [23] | CS | Italy | chemical industry | M | R + N | 185/134 | 48.7/48.9 | SBP DBP | No | 6 |
| Ely 1986 [24] | CS | US | police officers | M | R + N PN | R + N 41 PN 80/156 | R + N 37.4 PN 38.1/40.0 | SBP DBP | No | 6 |
| Ohlander 2015 [25] | CS | Germany | car manufacturing | F&M | R + N R-N PN | R + N 198 R-N 9572 PN 3568/12,005 | R + N 40.0 R-N 38.3 PN 41.4/37.8 | SBP DBP * HTN | * age, sex, BMI, lipids, smoking, alcohol, exercise, sleep disorders, job status, noise, heat, social disruption | 8 |
| Fesharaki 2014 [26] | CS | Iran | steel and polyacryl companies | M | R + N R-N | R + N 4050 R-N 597/3966 | R + N 41.62 R-N 43.31/41.33 | * SBP * DBP | * age, BMI, education, work experience, marital status | 8 |
| Guo 2013 [27] | CS | China | motor corporation | F&M | R + N | 9118/17,345 | 62.4/64.22 | SBP DBP | No | 6 |
| Ghiasvand 2006 [28] | CS | Iran | railroad company | M | NS | 158/266 | 46.4/38.69 | SBP DBP *HTN | * age, BMI, eating habits | 6 |
| Ishizuka 1993 [29] | CS | Japan | machine plant | M | R + N | 38/21 | 31.6/36.9 | SBP DBP | No | 5 |
| Jermendy 2012 [30] | CS | Hungary | multiple occupations | F&M | R + N | M 54/67 F 180/180 | M 42.2/42.5 F 44.5/42.9 | SBP DBP | No | 4 |
| Kantermann 2013 [31] | CS | Belgium | steel factory | M | R + N | 32/15 | 39.5/45.0 | SBP DBP | No | 4 |
| Kawabe 2014 [32] | CS | Japan | 12 large companies | F&M | R + N R-N PN | R +N 243 R-N 1017 PN 73/3094 | R + N 40.1 R-N 37.9 PN 50.8/42.6 | SBP DBP | No | 5 |
| Kawada 2014 [33] | CS | Japan | car manufacturing | M | R + N R-N | R + N 99 R-N 686/868 | R + N 44.5 R-N 44.3/44.4 | SBP DBP | No | 5 |
| Kawakami 1998 [34] | CS | Japan | electrical company | M | R + N | H 161/123 A 280/355 P 186/178 L 546/1053 | NotR | * SBP * DBP | * age, obesity, exercise, alcohol, education | 8 |
| Knutsson 1988 [35] | CS | Sweden | paper and cellulose plants | M | R +N | 361/240 | 43.2/44.8 | SBP DBP | No | 4 |
| Kubo 2013 [36] | CH (12.7 y) | Japan | industry manufacturing | M | R + N | 964/9209 | 22.3/23.8 | SBP DBP * HTN | * age, smoking, alcohol, exercise, BP and BMI at baseline and follow-up | 8 |
| Lang 1988 [37] | CS | Senegal | hotel, canning, cotton printing, tobacco, oil, companies | F&M | NS | 396/900 | M 39.3 ± 9.7 F 35.4 ± 8.8 | * SBP * DBP | * age | 5 |
| Lercher 1993 [38] | CS | Austria | rural community | F&M | PN | 22/147 | [25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62] | * SBP * DBP | * age, sex, education, smoking, BMI, other occupational risk factors | 8 |
| Lin 2015 [39] | CS | Taiwan | electronics company | F&M | RN | M 447/375 F 118/137 | M 31.5/33.8 F 32.5/31.7 | SBP DBP | No | 4 |
| Marqueze 2013 [40] | CS | Brazil | truck drivers | M | PN | 31/26 | 39.8 ± 6.6 | HTN | No | 5 |
| Nazri 2008 [41] | CS | Malaysia | semiconductors factory | M | R + N | 76/72 | 31.60/32.32 | * HTN | * age, BMI, smoking, exercise, education, marital status, job, working hours and duration | 7 |
| Mohebbi 2012 [42] | CS | Iran | long distance drivers | M | PN | 3039/3039 | [20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60] | SBP DBP | No | 4 |
| Morikawa 2007 [43] | CS | Japan | zipper and sash factory | M | R + N | 434/712 | 33.5/36.4 | SBP DBP | No+ | 5 |
| Moy 2010 [44] | CS | Malaysia | medical university | F | R + N | 112/268 | 49.8/49.2 | SBP DBP | No | 6 |
| Murata 1999 [45] | CS | Japan | copper-smelting plant | M | R + N | 158/75 | 36/36 | SBP DBP | No | 5 |
| Nagaya 2002 [46] | CS | Japan | manual production, security, transportation | M | R + N | 826/2824 | 45.6/47.1 | SBP DBP * HTN | * age, BMI, job, alcohol, smoking, exercise | 7 |
| Pimenta 2012 [47] | CS | Brazil | public university | F&M | PN | 81/130 | [30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62] | HTN | No | 4 |
| Puttonen 2009 [48] | CS | Finland | population-based | F&M | NS | M 157/555 F 208/623 | [24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39] | SBP DBP | No | 5 |
| Sakata 2003 [49] | CH (91-01) | Japan | steel company | M | R + N | 2316/3022 | NotR | SBP DBP * HTN | * age, BMI, alcohol, smoking, exercise, TC, creatinine, UA GTP, HbA1c | 9 |
| Santhanam 2014 [50] | CS | USA | NHANES | F | NS | 681/2481 | 32.9/32.4 | SBP HTN | No | 4 |
| Sfreddo 2010 [51] | CS | Brazil | nursing staff | F | PN | 182/311 | 36.4/33.1 | SBP DBP HTN | No | 7 |
| Sookoian 2007 [52] | CS | Argentina | 1 factory | F | R + N | 474/877 | 36/34 | SBP DBP | No | 5 |
| Suessenbacher 2011 [53] | CS | Austria | glass factory | M | R + N | 48/47 | 48/47 | HTN | No | 5 |
| Tanigawa 2006 [54] | CS | Japan | 3 nuclear power plants | M | R + N | 253/206 | 40.4/41.5 | SBP DBP | No | 6 |
| Virkkunen 2007 [55] | CS | Finland | paper and pulp or oil industries | M | R + N | 27/285 | [40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55] | SBP HTN | No | 5 |
| Yamasaki 1998 [56] | CS | USA | nursing staff | F | NS | 35/58 | 40.7 [30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59] | SBPAMBP DBPAMBP | No | 6 |
| Ohira 2000 [57] | CS | Japan | nuclear power plant | M | R + N | 27/26 | 30.5/31.8 | * SBPAMBP DBPAMBP | * age, BMI, alcohol, exercise, anger score | 6 |
| Kario 2002 [58] | CS | USA | nursing staff | F | PN | 33/54 | 40/41 | SBPAMBP DBPAMBP | No | 5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gamboa Madeira, S.; Fernandes, C.; Paiva, T.; Santos Moreira, C.; Caldeira, D. The Impact of Different Types of Shift Work on Blood Pressure and Hypertension: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 6738. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18136738
Gamboa Madeira S, Fernandes C, Paiva T, Santos Moreira C, Caldeira D. The Impact of Different Types of Shift Work on Blood Pressure and Hypertension: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2021; 18(13):6738. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18136738
Chicago/Turabian StyleGamboa Madeira, Sara, Carina Fernandes, Teresa Paiva, Carlos Santos Moreira, and Daniel Caldeira. 2021. "The Impact of Different Types of Shift Work on Blood Pressure and Hypertension: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 18, no. 13: 6738. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18136738