
A Study of Older Adults’ Perception of High-Density Housing Neighbourhoods in Singapore: Multi-Sensory Perspective


Abstract
:1. Introduction
1.1. Ageing Population Trends
1.2. Sensory Decline
1.3. Cognitive Decline
1.4. Sensory Approaches in Architecture and Urban Design
1.5. Research Objectives
2. Materials and Methods
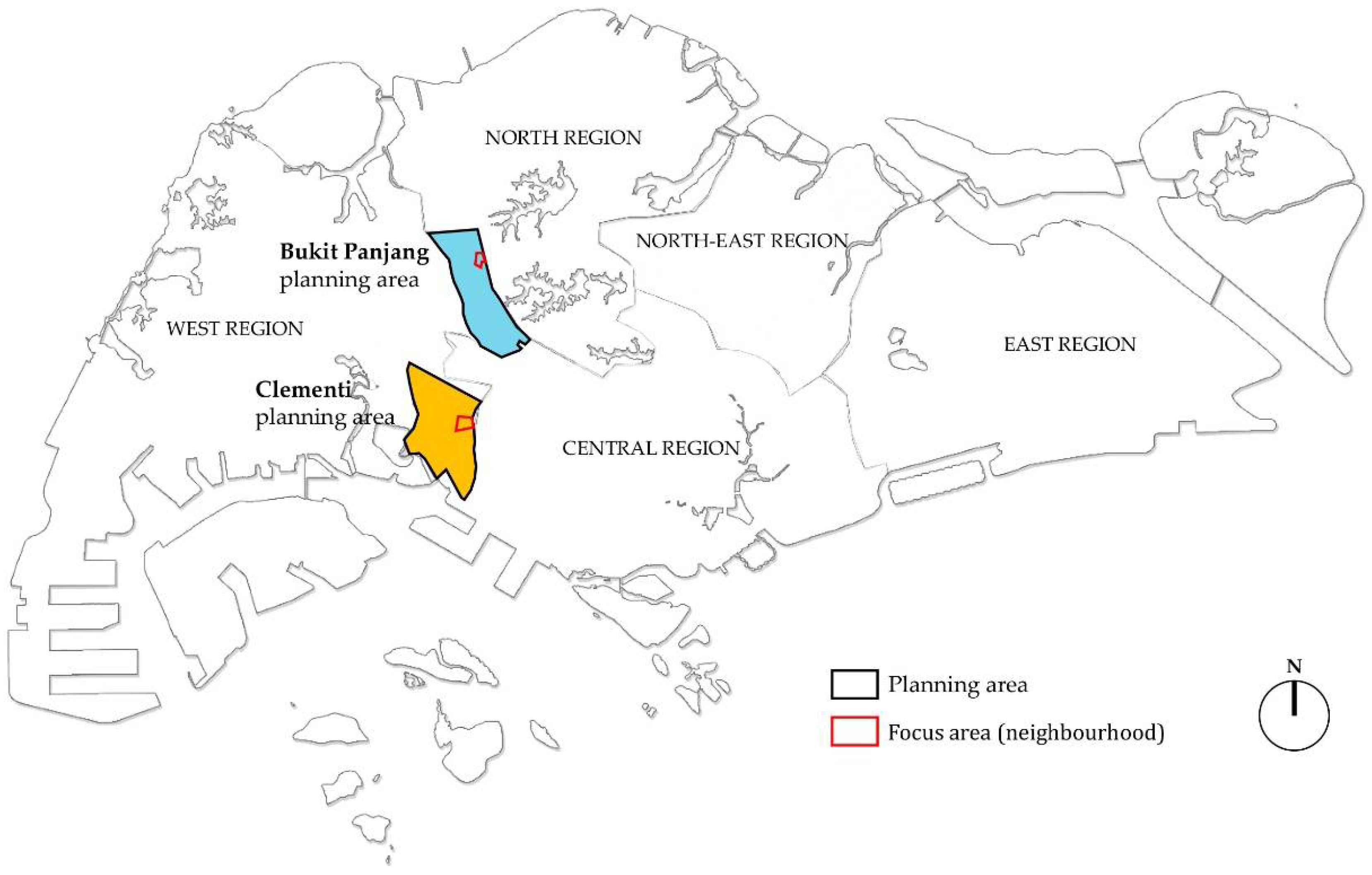
2.1. Study Areas
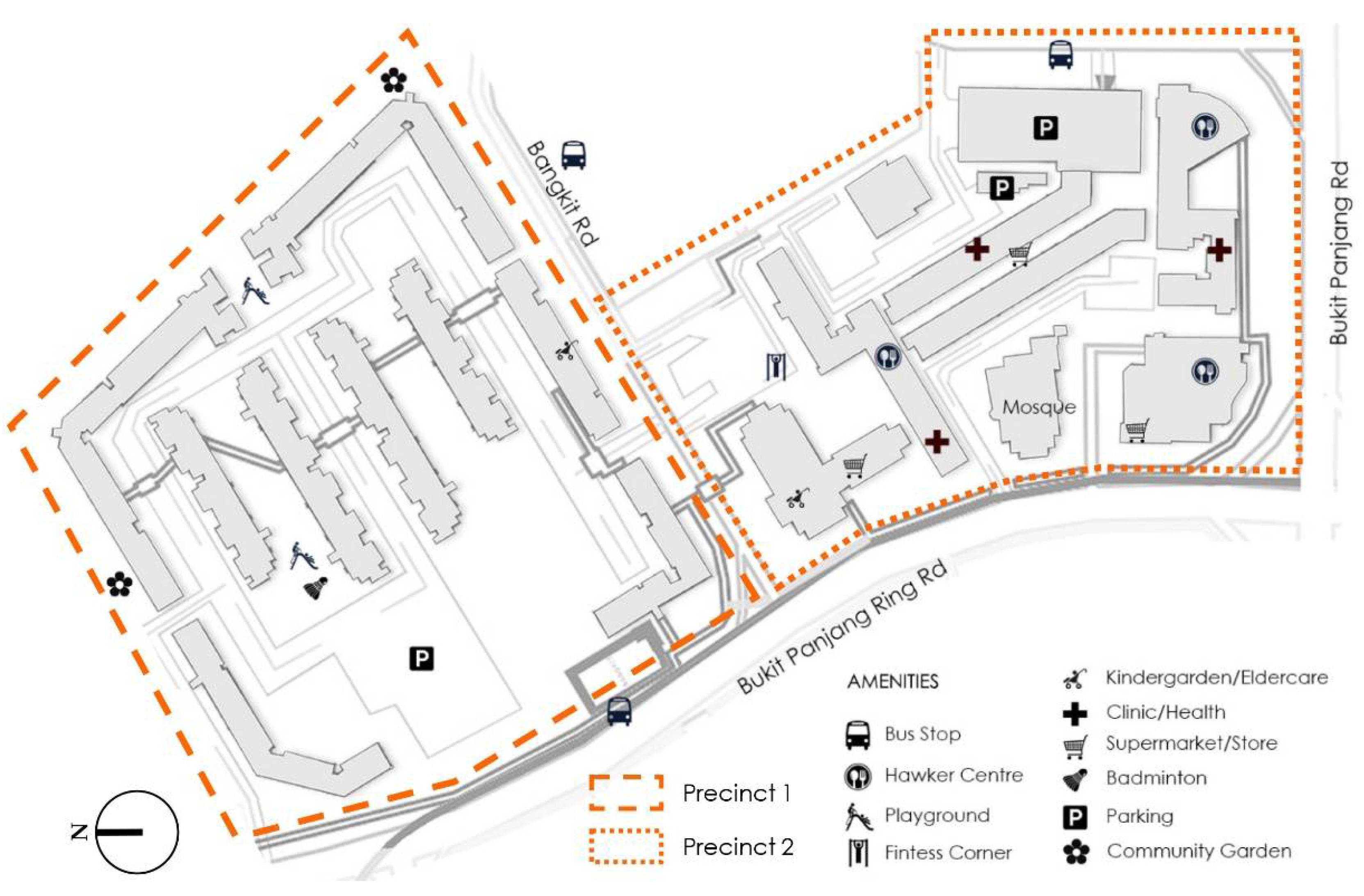
2.1.1. Neighbourhood 1: Bangkit
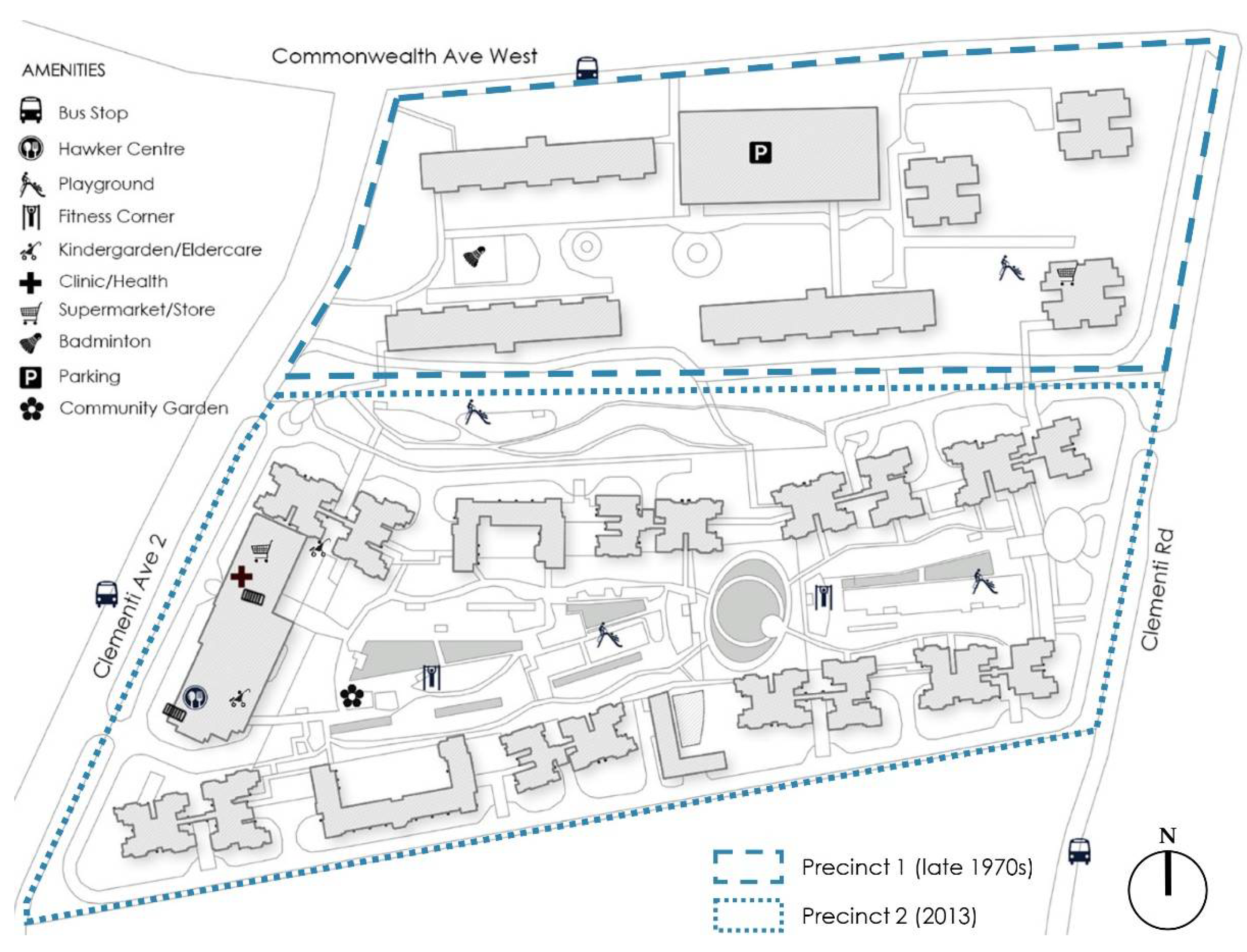
2.1.2. Neighbourhood 2: Clementi
2.2. Exploratory On-Site Studies
2.2.1. ‘Sensing the Site’ Journeys
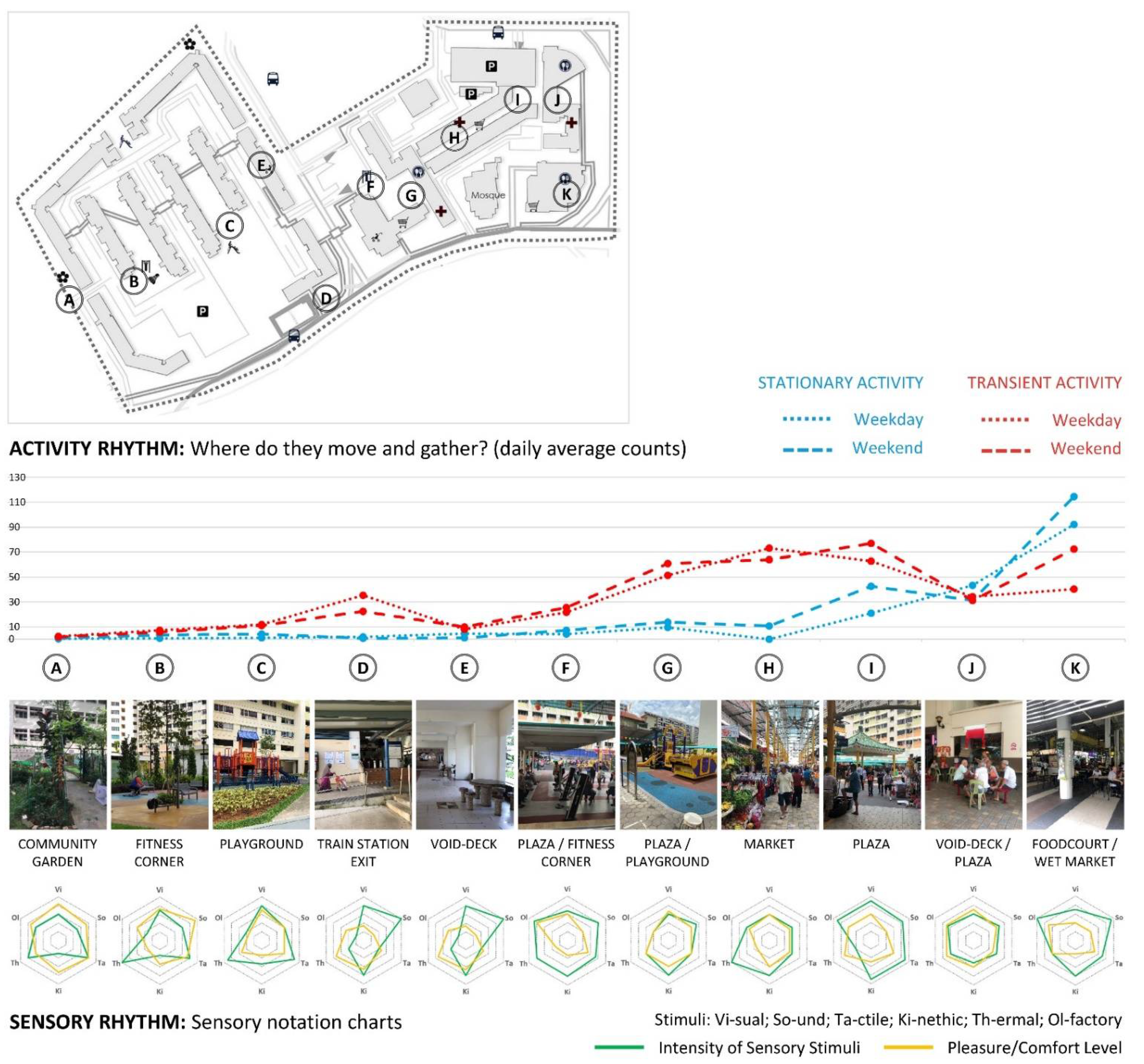
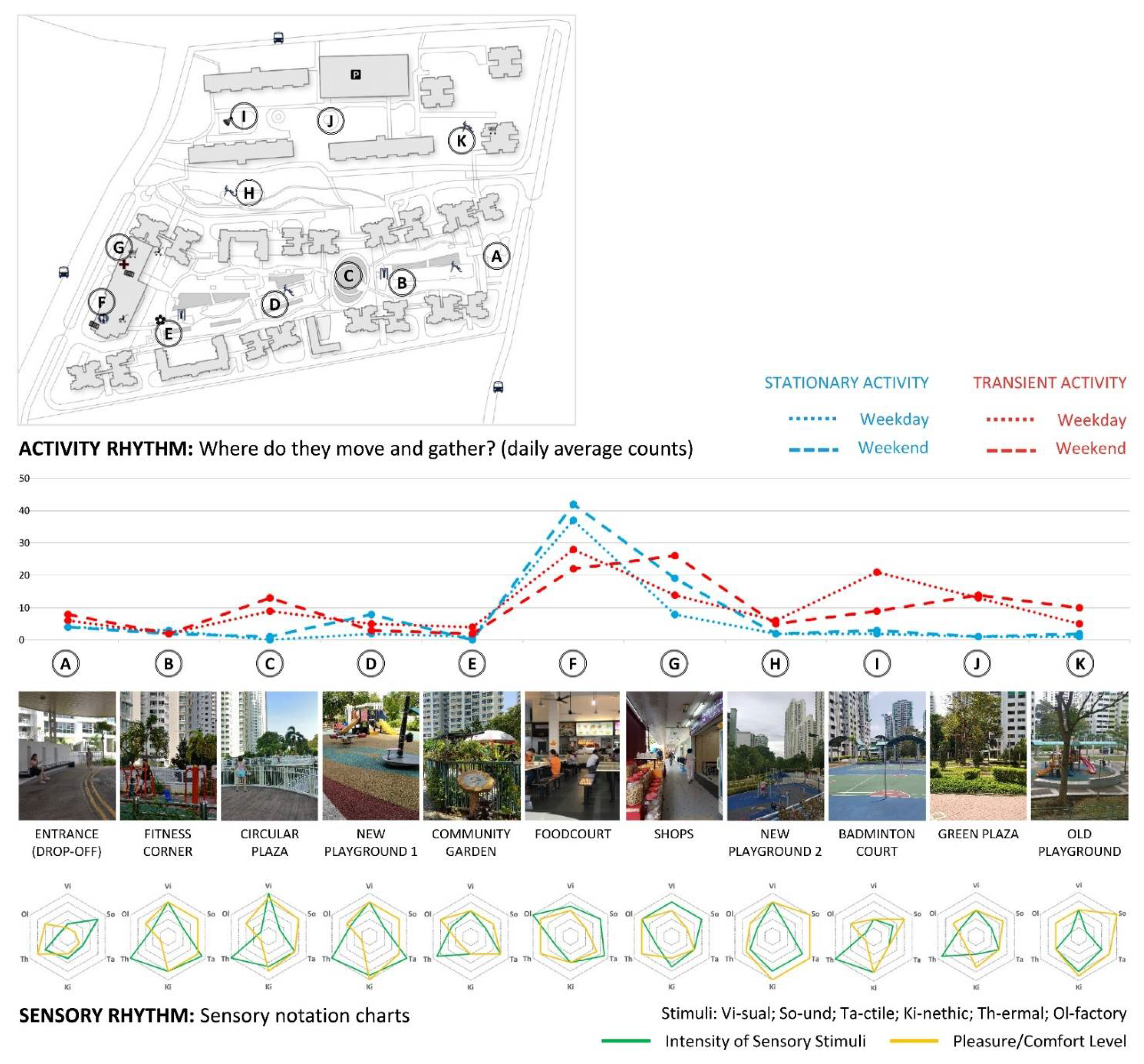
2.2.2. Documentation of Sensory Rhythms and Pedestrian Activity Patterns
2.2.3. Synthesis: Rhythm Analysis
2.3. Socio-Sensory Perception Surveys
Statistical Analysis
3. Results
3.1. Rhythm Analysis Findings
3.2. Survey Results
3.2.1. Survey Sample and General Information
3.2.2. Daily Routine
3.2.3. Overall Sensory Appreciation
3.2.4. Walking Experience
3.2.5. Overall Satisfaction with the Neighbourhood
3.2.6. Other Correlations
4. Discussion
5. Conclusions
Supplementary Materials
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| General Information |
| Age: |
| Gender: male/female |
| Ethnicity: Chinese/Malay/Indian/Others |
| How long have you lived in this neighbourhood? _________ |
| Any sensory impairment: poor vision/poor hearing/poor smell detection/walking difficulties/cognitive difficulties/other (please specify) |
| Overall health condition: poor/could be better/good/very good/excellent |
| Daily Routine |
| 1. How often do you go out of your home into your neighbourhood? (a) more than 3 times per day; (b) 2–3 times a day; (c) once a day; (d) few times every week; (e) few times every month |
| 2. What activities do you most frequently perform within your neighbourhood (as part of your daily routine)? Choose up to 3 answers. (a) Commuting (e.g., walking to MRT station, bus stop, school, work); (b) Strolling around; (c) Shopping (e.g., going to supermarket, wet market, shopping mall); (d) Eating (e.g., in nearby foodcourt, coffee shop, restaurant); (e) Playing; (f) Jogging, exercising, cycling, etc.; (g) Meeting friends; (h) Gardening (e.g., in community garden); (i) Visiting community organisations (e.g., CC clubs, childcare, elderly care, RCs); (j) Other (please specify) _________ |
| 3. Where do you most frequently visit on daily basis in this neighbourhood? Name up to 2 places. |
| 4. With regard to Question 3, please describe in any 3 keywords or phrases that reflect your feel and mood with regard to why you visit each of these places so often. |
| 5. Where do you like the most in this neighbourhood? Name up to 2 places or features. |
| 6. With regard to Question 5, please describe in 3 keywords or phrases that reflect your feel and mood with regard to why you like each of these places. |
| 7. Where do you usually meet your fellow neighbours or friends? Name 1 place. |
| 8. Where do you dislike the most in this neighbourhood? Name up to 2 places or features. |
| 9. With regard to Question 8, please describe in any 3 keywords or phrases that reflect your feel and mood with regard to why you dislike these places. |
| Overall Sensory Appreciation |
| 10. Do you agree with the following statements related to your sensory experience? (strongly disagree—1/disagree—2/neither agree nor disagree—3/somewhat agree—4/strongly agree—5) |
| a. This neighbourhood is overall aesthetically appealing. |
| b. This neighbourhood offers good variety of areas with distinguishable ambients. |
| c. This neighbourhood shows obvious features pertinent to different cultures. |
| d. This neighbourhood is often too crowded. |
| e. Spaces around my home are generally clean and tidy. |
| f. I often find spaces around my home smelly. |
| g. I often find spaces around my home quite noisy. |
| h. I feel overwhelmed and bombarded in this neighbourhood on everyday basis. |
| Walking Experience |
| 11. Do you agree with the following statements related to your sensory experience? (strongly disagree—1/disagree—2/neither agree nor disagree—3/somewhat agree—4/strongly agree—5) |
| a. There are many obstacles (e.g., steps, dangerous curbs, gaps) to walk around this neighbourood. |
| b. Floors in this neighbourhood are slippery when it rains and I feel unsafe to walk. |
| c. I hesitate to go out if there is no one accompanying or helping me. |
| d. Sometimes, I can’t find my way in this neighbourhood. |
| e. Nature makes walking through this neighbourhood more enjoyable. |
| f. I avoid passing by rubbish chutes, messy areas and dark places. |
| g. I always prefer walking on sheltered pathways (covered walkways and void decks). |
| Overall Satisfaction with the Neighbourhood |
| 12. Do you agree with the following statements related to your sensory experience? (strongly disagree—1/disagree—2/neither agree nor disagree—3/somewhat agree—4/strongly agree—5) |
| a. Amenities in this neighbourhood provide well for my daily routine needs. |
| b. There are plenty of opportunities for different generations (e.g., children and elderly) to meet. |
| c. This neighbourhood is overall well-designed for the elderly users. |
| d. I feel happy living in this neighbourhood. |
References
- Merleau-Ponty, M. Phenomenology of Perception, 2nd ed.; Routledge: London, UK; New York, NY, USA, 2002. [Google Scholar]
- Pallasmaa, J. The Eyes of the Skin: Architecture and the Senses; Academy Editions: London, UK, 1996. [Google Scholar]
- Tuan, Y.-F. Space and Place: The Perspective of Experience; University of Minnesota Press: Minneapolis, MN, USA, 1977. [Google Scholar]
- Schweitzer, M.; Gilpin, L.; Frampton, S. Healing spaces: Elements of environmental design that make an impact on health. J. Altern. Complement. Med. 2004, 10 (Suppl. 1), S71–S83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sternberg, E.M. Healing Spaces: The Science of Place and Well-Being; Belknap Press of Harvard University Press: Cambridge, MA, USA, 2009. [Google Scholar]
- Degen, M.M. Sensing Cities: Regenerating Public Life in Barcelona and Manchester; Routledge: London, UK; New York, NY, USA, 2008. [Google Scholar]
- Zardini, M. Toward a sensorial urbanism. In Sense of the City: An Alternate Approach to Urbanism; Zardini, M., Ed.; Lars Müller Publishers: Baden, Switzerland; Canadian Centre for Architecture: Montreal, QC, Canada, 2005; pp. 17–27. [Google Scholar]
- Cacchione, P.Z. Sensory impairment: A new research imperative. J. Gerontol. Nurs. 2014, 40, 3–5. [Google Scholar] [CrossRef] [PubMed]
- United Nations, Department of Economic and Social Affairs, Population Division. World Population Prospects 2019: Highlights; United Nations: New York, NY, USA, 2019; Available online: https://population.un.org/wpp/Publications/Files/WPP2019_Highlights.pdf (accessed on 8 December 2020).
- United Nations (UN), Department of Economic and Social Affairs, Population Division. World Population Prospects 2019: Volume 1: Comprehensive Tables; United Nations: New York, NY, USA, 2019; Available online: https://population.un.org/wpp/Publications/Files/WPP2019_Volume-I_Comprehensive-Tables.pdf (accessed on 8 December 2020).
- Department of Statistics. Population Trends 2020; Department of Statistics, Ministry of Trade & Industry: Singapore, 2020. Available online: https://www.singstat.gov.sg/-/media/files/publications/population/population2020.pdf (accessed on 8 December 2020).
- Ministry of Health. I Feel Young in My Singapore! Action Plan for Successful Ageing; Ministry of Health: Singapore, 2016. Available online: https://www.moh.gov.sg/docs/librariesprovider3/action-plan/action-plan.pdf (accessed on 8 December 2020).
- Correia, C.; Lopez, K.J.; Wroblewski, K.E.; Huisingh-Scheetz, M.; Kern, D.W.; Chen, R.C.; Schumm, L.P.; Dale, W.; McClintock, M.K.; Pinto, J.M. Global sensory impairment in older adults in the United States. J. Am. Geriatr. Soc. 2016, 64, 306–313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organisation. World Report on Vision; World Health Organisation: Geneva, Switzerland, 2019; Available online: https://apps.who.int/iris/rest/bitstreams/1257940/retrieve (accessed on 8 December 2020).
- Bourne, R.R.A.; Flaxman, S.R.; Braithwaite, T.; Cicinelli, M.V.; Das, A.; Jonas, J.B.; Keeffe, J.; Kempen, J.H.; Leasher, J.; Limburg, H.; et al. Vision Loss Expert Group. Magnitude, temporal trends, and projections of the global prevalence of blindness and distance and near vision impairment: A systematic review and meta-analysis. Lancet Glob. Health 2017, 5, e888–e897. [Google Scholar] [CrossRef] [Green Version]
- Tham, Y.C.; Lim, S.H.; Shi, Y.; Chee, M.L.; Zheng, Y.F.; Chua, J.; Saw, S.M.; Foster, P.; Aung, T.; Wong, T.Y.; et al. Trends of visual impairment and blindness in the Singapore Chinese population over a decade. Sci. Rep. 2018, 8, 12224. [Google Scholar] [CrossRef] [Green Version]
- Crews, J.E.; Campbell, V.A. Vision impairment and hearing loss among community-dwelling older Americans: Implications for health and functioning. Am. J. Public Health 2004, 94, 823–829. [Google Scholar] [CrossRef]
- Kwon, H.J.; Kim, J.S.; Kim, Y.J.; Kwon, S.J.; Yu, J.N. Sensory impairment and health-related quality of life. Iran. J. Public Health 2015, 44, 772–782, PMCID:PMC4524301. [Google Scholar] [PubMed]
- Freeman, E.E.; Egleston, B.L.; West, S.K.; Bandeen-Roche, K.; Rubin, G. Visual acuity change and mortality in older adults. Investig. Ophthalmol. Vis. Sci. 2005, 46, 4040–4045. [Google Scholar] [CrossRef] [Green Version]
- Sarant, J.; Harris, D.; Busby, P.; Maruff, P.; Schembri, A.; Lemke, U.; Launer, S. The effect of hearing aid use on cognition in older adults: Can we delay decline or even improve cognitive function? J. Clin. Med. 2020, 9, 254. [Google Scholar] [CrossRef] [Green Version]
- Lee, G.J.C.; Danker, A.N.; Wong, Y.H.; Lim, M.Y. Hearing loss amongst the elderly in a Southeast Asian population–A community-based study. Ann. Acad. Med. Singap. 2017, 46, 145–154. [Google Scholar] [PubMed]
- Lewis, T.J. Hearing impairment. In Primary Care Geriatrics: A Case-based Approach, 6th ed.; Ham, R.J., Sloane, P.D., Warshaw, G.A., Bernard, M.A., Flaherty, E., Eds.; Elsevier/Saunders: Philadelphia, PA, USA, 2014; pp. 291–300. [Google Scholar]
- Mick, P. Associations between sensory loss and social networks, participation, support, and loneliness: Analysis of the Canadian Longitudinal Study on Aging. Can. Fam. Physician 2018, 64, e33–e41. [Google Scholar]
- Kern, D.W.; Wroblewski, K.E.; Schumm, L.P.; Pinto, J.M.; McClintock, M.K. Field survey measures of olfaction: The olfactory function field exam (OFFE). Field Methods 2014, 26, 421–434. [Google Scholar] [CrossRef] [Green Version]
- Murphy, C.; Schubert, C.R.; Cruickshanks, K.J.; Klein, B.E.; Klein, R.; Nondahl, D.M. Prevalence of olfactory impairment in older adults. JAMA 2002, 288, 2307–2312. [Google Scholar] [CrossRef]
- Welge-Lüssen, A. Ageing, neurodegeneration, and olfactory and gustatory loss. B-ENT 2009, 5 (Suppl. 13), 129–132. [Google Scholar] [PubMed]
- Wickremaratchi, M.M.; Llewelyn, J.G. Effects of ageing on touch. Postgrad. Med. J. 2006, 82, 301–304. [Google Scholar] [CrossRef]
- Albers, M.W.; Gilmore, G.C.; Kaye, J.; Murphy, C.; Wingfield, A.; Bennett, D.A.; Boxer, A.L.; Buchman, A.S.; Cruickshanks, K.J.; Devanand, D.P.; et al. At the interface of sensory and motor dysfunctions and Alzheimer’s disease. Alzheimers Dement. 2015, 11, 70–98. [Google Scholar] [CrossRef] [Green Version]
- Chan, K.M.; Pang, W.S.; Ee, C.H.; Ding, Y.Y.; Choo, P. Epidemiology of falls among the elderly community dwellers in Singapore. Singap. Med. J. 1997, 38, 427–431. [Google Scholar] [PubMed]
- World Health Organisation. Risk Reduction of Cognitive Decline and Dementia: WHO Guidelines; World Health Organisation: Geneva, Switzerland, 2019; Available online: https://apps.who.int/iris/bitstream/handle/10665/312180/9789241550543-eng.pdf?ua=1 (accessed on 8 December 2020).
- Subramaniam, M.; Chong, S.A.; Vaingankar, J.A.; Abdin, E.; Chua, B.Y.; Chua, H.C.; Eng, G.K.; Heng, D.; Hia, S.B.; Huang, W.; et al. Prevalence of dementia in people aged 60 years and above: Results from the WiSE study. J. Alzheimers Dis. 2015, 45, 1127–1138. [Google Scholar] [CrossRef]
- Heywood, R.; Gao, Q.; Nyunt, M.S.Z.; Feng, L.; Chong, M.S.; Lim, W.S.; Yap, P.; Lee, T.S.; Yap, K.B.; Wee, S.L.; et al. Hearing loss and risk of mild cognitive impairment and dementia: Findings from the Singapore longitudinal ageing study. Dement. Geriatr. Cogn. Disord. 2017, 43, 259–268. [Google Scholar] [CrossRef]
- Inouye, S.K.; Westendorp, G.J.; Saczynski, J.S. Delirium in elderly people. Lancet 2014, 383, 911–922. [Google Scholar] [CrossRef] [Green Version]
- Ribeiro, M.V.; Hasten-Reiter, H.N., Jr.; Ribeiro, E.A.; Jucá, M.J.; Barbosa, F.T.; Sousa-Rodrigues, C.F. Association between visual impairment and depression in the elderly: A systematic review. Arq. Bras. Oftalmol. 2015, 78, 197–201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feng, L.; Nyunt, M.S.Z.; Gao, Q.; Feng, L.; Lee, T.S.; Tsoi, T.; Chong, M.S.; Lim, W.S.; Collinson, S.; Yap, P.; et al. Physical frailty, cognitive impairment, and the risk of neurocognitive disorder in the Singapore longitudinal ageing studies. J. Gerontol. A Biol. Sci. Med. Sci. 2016, 72, 369–375. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guthrie, D.M.; Declercq, A.; Finne-Soveri, H.; Fries, B.E.; Hirdes, J.P. The health and well-being of older adults with dual sensory impairment (DSI) in four countries. PLoS ONE 2016, 11, e0155073. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fischer, M.E.; Cruickshanks, K.J.; Klein, B.E.; Klein, R.; Schubert, C.R.; Wiley, T.L. Multiple sensory impairment and quality of life. Ophthalmic Epidemiol. 2009, 16, 346–353. [Google Scholar] [CrossRef] [Green Version]
- Lopez, D.; McCaul, K.A.; Hankey, G.J.; Norman, P.E.; Almeida, O.P.; Dobson, A.J.; Byles, J.E.; Yeap, B.B.; Flicker, L. Falls, injuries from falls, health related quality of life and mortality in older adults with vision and hearing impairment-is there a gender difference? Maturitas 2011, 69, 359–364. [Google Scholar] [CrossRef]
- Andressen, M.; Puggaard, L. Autonomy among physically frail older people in nursing home settings: A study protocol for an intervention study. BMC Geriatr. 2008, 8, 32. [Google Scholar] [CrossRef] [Green Version]
- Heine, C.; Browning, C.J. The communication and psychosocial perceptions of older adults with sensory loss: A qualitative study. Ageing Soc. 2004, 24, 113–130. [Google Scholar] [CrossRef] [Green Version]
- Malnar, J.M.; Vodvarka, F. Sensory Design; University of Minnesota Press: Minneapolis, MN, USA, 2004. [Google Scholar]
- Perdue, W.C.; Gostin, L.O.; Stone, L.A. Public health and the built environment: Historical, empirical and theoretical foundations for an expanded role. J. Law Med. Ethics 2003, 31, 557–566. [Google Scholar] [CrossRef]
- Kaplan, R.; Kaplan, S. The Experience of Nature: A Psychological Perspective; Cambridge University Press: Cambridge, UK; New York, NY, USA, 1989. [Google Scholar]
- Ulrich, R.S. Effects of interior design on wellness: Theory and recent scientific research. J. Health Care Inter. Des. 1991, 3, 97–109. [Google Scholar] [PubMed]
- Linton, P.E. Creating a total healing environment. In Innovations in Healthcare Design: Selected Presentations from the First Five Symposia on Healthcare Design; Marberry, S.O., Ed.; Van Nostrand Reinhold: New York, NY, USA, 1995; pp. 121–131. [Google Scholar]
- Antonovski, A. The salutogenic model as a theory to guide health promotion. Health Promot. Int. 1996, 11, 11–18. [Google Scholar] [CrossRef]
- Riley-Doucet, C.K. Use of multisensory environments in the home for people with dementia. J. Gerontol. Nurs. 2009, 35, 42–52. [Google Scholar] [CrossRef]
- Vozzella, S. Sensory stimulation in dementia care: Why it is important and how to implement it. Top. Geriatr. Rehabil. 2007, 23, 102–113. [Google Scholar] [CrossRef] [Green Version]
- Lawton, M.P.; Nahemow, L. Ecology and the aging process. In Psychology of Adult Development and Aging; Eisdorfer, C., Lawton, M.P., Eds.; American Psychological Association: Washington, DC, USA, 1973; pp. 619–674. [Google Scholar]
- Kahana, E.; Lovegreen, L.; Kahana, B.; Kahana, M. Person, environment, and person-environment fit as influences on residential satisfaction of elders. Environ. Behav. 2003, 35, 434–453. [Google Scholar] [CrossRef]
- Chalfont, G.E. Creating enabling outdoor environments for residents. Nurs. Resid. Care 2005, 7, 454–457. [Google Scholar]
- Bengtsson, A.; Grahn, P. Outdoor environments in healthcare settings: A quality evaluation tool for use in designing healthcare gardens. Urban. For. Urban. Gree. 2014, 13, 878–891. [Google Scholar] [CrossRef] [Green Version]
- Cox, H.; Burns, I.; Savage, S. Multisensory environments for leisure: Promoting well-being in nursing home residents with dementia. J. Gerontol. Nurs. 2004, 30, 37–45. [Google Scholar] [CrossRef]
- van den Berg, M.E.L.; Winsall, M.; Dyer, S.M.; Breen, F.; Gresham, M.; Crotty, M. Understanding the barriers and enablers to using outdoor spaces in nursing homes: A systematic review. Gerontologist 2020, 60, e254–e269. [Google Scholar] [CrossRef] [Green Version]
- Bengtsson, A.; Carlsson, G. Outdoor environments at three nursing homes: Focus group interviews with staff. J. Hous. Elder. 2008, 19, 49–69. [Google Scholar] [CrossRef]
- Chung, J.C.C.; Chan, T.Y.P.; Lee, I.W.S. Sensory-based intervention for management of maladaptive behaviors in people with dementia. Asian J. Gerontol. Geriatr. 2007, 2, 107–110. [Google Scholar]
- Low, E.Y.K.; Kalekin-Fishman, D. (Eds.) Senses in Cities: Experiences of Urban. Settings; Routledge: London, UK; New York, NY, USA, 2017. [Google Scholar]
- Thibaud, J.P. The sensory fabric of urban ambiances. Senses Soc. 2011, 6, 203–215. [Google Scholar] [CrossRef] [Green Version]
- Howes, D. Charting the sensorial revolution. Senses Soc. 2006, 1, 113–128. [Google Scholar] [CrossRef]
- Howes, D. Sensual Relations: Engaging the Senses in Culture and Social Theory; The University of Michigan Press: Ann Arbor, MI, USA, 2003. [Google Scholar]
- Edwards, E.; Gosden, C.; Phillips, R.B. (Eds.) Introduction. In Sensible Objects: Colonialism, Museums and Material Culture; Berg: Oxford, UK; New York, NY, USA, 2006; pp. 1–32. [Google Scholar]
- Mallgrave, H.F. Architecture and Embodiment: The Implications of the New Sciences and Humanities for Design; Routledge: New York, NY, USA, 2013. [Google Scholar]
- Spence, C. Senses of place: Architectural design for the multisensory mind. Cogn. Res. Princ. Implic. 2020, 5, 46. [Google Scholar] [CrossRef]
- Sternberg, E.M.; Wilson, M.A. Neuroscience and architecture: Seeking common ground. Cell 2006, 127, 239–242. [Google Scholar] [CrossRef] [Green Version]
- Jelic, A.; Tieri, G.; De Matteis, F.; Babiloni, F.; Vecchiato, G. The enactive approach to architectural experience: A neurophysiological perspective on embodiment, motivation, and affordances. Front. Psychol. 2016, 7, 481. [Google Scholar] [CrossRef] [Green Version]
- Husserl, E. Ideas: General Introduction to a Pure Phenomenology; Gibson, W.R.B., Translator; Routledge: London, UK; New York, NY, USA, 2012. [Google Scholar]
- Heidegger, M. Poetry, Language, Thought; Hofstadter, A., Translator; Harper & Row: New York, NY, USA, 1971. [Google Scholar]
- Norberg-Schulz, C. The phenomenon of place. In The Urban Design Reader; Larice, M., Macdonald, E., Eds.; Routledge: London, UK; New York, NY, USA, 2013; pp. 272–284. [Google Scholar]
- Norberg-Schulz, C. Genius Loci: Towards a Phenomenology of Architecture; Rizzoli: New York, NY, USA, 1980. [Google Scholar]
- Bachelard, G. The Poetics of Space; Jolas, M., Translator; Beacon Press: Boston, MA, USA, 1994. [Google Scholar]
- Perec, G. Species of Spaces and Other Pieces; Sturrock, J., Translator; Penguin Books: London, UK; New York, NY, USA, 1974. [Google Scholar]
- Dovey, K. The aesthetics of place. In Aesthetics, Well-Being, and Health: Essays within Architecture and Environmental Aesthetics; Cold, B., Ed.; Ashgate: Aldershot, UK; Burlington, VT, USA, 2001; pp. 93–101. [Google Scholar]
- Pink, S. Home Truths: Gender, Domestic Objects and Everyday Lift; Oxford: Berg, UK, 2004. [Google Scholar]
- Pink, S. Situating Everyday Life: Practices and Places; SAGE: Los Angeles, CA, USA; London, UK, 2012. [Google Scholar]
- Buttimer, A. Grasping the dynamism of lifeworld. Ann. Am. Assoc. Geogr. 1976, 66, 277–292. Available online: http://0-www-jstor-org.brum.beds.ac.uk/stable/2562470 (accessed on 10 June 2021). [CrossRef] [Green Version]
- Buttimer, A.; Seamon, D. The Human Experience of Space and Place; St. Martin’s Press: New York, NY, USA, 1980. [Google Scholar]
- Replh, E.C. Place and Placelessness; Pion: London, UK, 1976. [Google Scholar]
- Tuan, Y.-F. Topophilia: A Study of Environmental Perception, Attitudes, and Values; Prentice-Hall: Englewood Cliffs, NJ, USA, 1974. [Google Scholar]
- Massey, D. Space, Place and Gender; Polity: Cambridge, UK, 1994. [Google Scholar]
- Deleuze, G.; Guattari, F. A Thousand Plateaus: Capitalism and Schizophrenia; Massumi, B., Translator; Continuum: London, UK; New York, NY, USA, 2004. [Google Scholar]
- Dovey, K. Becoming Places; Routledge: London, UK; New York, NY, USA, 2010. [Google Scholar]
- Degen, M.M.; Rose, G. The sensory experience of urban design: The role of walking and perceptual memory. Urban Studies 2012, 49, 3271–3287. [Google Scholar] [CrossRef] [Green Version]
- Piga, B.E.A.; Salerno, R. (Eds.) Urban. Design and Representation: A Multidisciplinary and Multisensory Approach; Springer: Cham, Switzerland, 2017. [Google Scholar]
- Pink, S. Doing Sensory Ethnography: Images, Media and Representation in Research; SAGE: London, UK; Thousand Oaks, CA, USA; New Delhi, India, 2017. [Google Scholar]
- Lucas, R.; Romice, O. Assessing the multi-sensory qualities of urban space: A methodological approach and notational system for recording and designing the multi-sensory experience of urban space. Psyecology 2010, 1, 263–276. [Google Scholar] [CrossRef] [Green Version]
- Gibson, J.J. The Senses Considered as Perceptual Systems; Greenwood Press: Westport, CT, USA, 1983. [Google Scholar]
- Ingold, T. The Perception of the Environment: Essays on Livelihood, Dwelling and Skill; Routledge: London, UK; New York, NY, USA, 2000. [Google Scholar]
- Palipane, K. Interrogating place: A socio-sensory approach. Cities People Places 2017, 2, 55–69. [Google Scholar] [CrossRef] [Green Version]
- Palipane, K. Multimodal mapping–a methodological framework. J. Archit. 2019, 24, 91–113. [Google Scholar] [CrossRef]
- Pink, S. An urban tour: The sensory sociality of ethnographic place-making. Ethnography 2008, 9, 175–196. [Google Scholar] [CrossRef] [Green Version]
- Rogerson, R.; Rice, G. Making sense of places: “moral geographies” of sensory urbanism. Archit. Theory Rev. 2009, 14, 142–155. [Google Scholar] [CrossRef]
- La Malva, F.; Lo Verso, V.R.M.; Astolfi, A. Livingscape: A multi-sensory approach to improve the quality of urban spaces. Energy Procedia 2015, 78, 37–42. [Google Scholar] [CrossRef] [Green Version]
- Gomes, A. A framework of analysis for urban sensory aesthetics: Looking at sensescapes as ‘brush strokes’ of an urban canvas. In Senses in Cities: Experiences of Urban Settings; Low, E.Y.K., Kalekin-Fishman, D., Eds.; Routledge: London, UK, 2017; pp. 137–153. [Google Scholar]
- Law, L. Urban senses. In Introducing Human Geographies, 3rd ed.; Cloke, P., Crang, P., Goodwin, M., Eds.; Routledge: London, UK; New York, NY, USA, 2014; pp. 706–719. [Google Scholar]
- Pow, C.P. Public intervention, private aspiration: Gated communities and the condominization of housing landscapes in Singapore. Asia Pac. Viewp. 2009, 50, 215–227. [Google Scholar] [CrossRef]
- Chua, B.H. Public housing residents as clients of the state. Hous. Stud. 2000, 15, 45–60. [Google Scholar] [CrossRef]
- Lai, A.E. A neighbourhood in Singapore: Ordinary people’s lives “downstairs”. In Future Asian Space: Projecting the Urban Space of New East Asia; Hee, L., Boontharm, D., Viray, E., Eds.; NUS Press: Singapore, 2012; pp. 115–137. [Google Scholar]
- Pow, C.P. Urban dystopia and epistemologies of hope. Prog Hum. Geogr 2015, 39, 464–485. [Google Scholar] [CrossRef]
- Debord, G. Theory of the Dérive. In Situationist International Anthology; Knabb, K., Ed.; Bureau of Public Secrets: Berkeley, CA, USA, 2006; pp. 62–66. [Google Scholar]
- Gehl, J.; Svarre, B. How to Study Public Life; Island Press: Washington, DC, USA, 2013. [Google Scholar]
- Whyte, W.H. The Social Life of Small Urban. Spaces; Conservation Foundation: Washington, DC, USA, 1980. [Google Scholar]
- Trivic, Z.; Tan, B.K.; Mascarenhas, N.; Duong, Q. Capacities and impacts of community arts and culture initiatives in Singapore. J. Arts Manag. Law Soc. 2020, 50, 85–114. [Google Scholar] [CrossRef]
- Yuen, B.; Nair, P. Investigating Space, Activities and Social Dynamics. In Ageing and the Built Environment in Singapore; Yuen, B., Ed.; Springer: Cham, Switzerland, 2019; pp. 175–219. [Google Scholar]
- Lefebvre, H. Rhythmanalysis: Space, Time and Everyday Life; Continuum: New York, NY, USA, 2004. [Google Scholar]
- Chan, Y.H. Biostatistics 104: Correlational analysis. Singap. Med. J. 2003, 44, 614–619. [Google Scholar] [PubMed]
- Hinkle, D.E.; Wiersma, W.; Jurs, S.G. Applied Statistics for the Behavioral Sciences, 5th ed.; Houghton Mifflin: Boston, MA, USA, 2003. [Google Scholar]
- Mukaka, M.M. Statistics corner: A guide to appropriate use of correlation coefficient in medical research. Malawi Med. J. 2012, 24, 69–71, PMCID:PMC3576830. [Google Scholar] [PubMed]
- Evans, J.D. Straightforward Statistics for the Behavioral Sciences; Brooks/Cole Publishing: Pacific Grove, CA, USA, 1996. [Google Scholar]
- Alterovitz, S.S.; Mendelsohn, G.A. Relationship goals of middle-aged, young-old, and old-old Internet daters: An analysis of online personal ads. J. Aging Stud. 2013, 27, 159–165. [Google Scholar] [CrossRef]
- Cohen-Mansfield, J.; Shmotkin, D.; Blumstein, Z.; Shorek, A.; Eyal, N.; Hazan, H. The old, old-old, and the oldest old: Continuation or distinct categories? An examination of the relationship between age and changes in health, function, and wellbeing. Int. J. Aging Hum. Dev. 2013, 77, 37–57. [Google Scholar] [CrossRef]
- Bozovic-Stamenovic, R. Old, Older, Oldish–NEW elderly and impact on healing design in Singapore. In Get Better! UIA/PHG Healthcare Forum; Del Nord, R., Ed.; TESIS Inter-University Research Center, Systems and Technologies for Healthcare Facilities, University of Florence: Florence, Italy, 2014; pp. 317–330. [Google Scholar]
- Yuen, B.; Močnik, Š.; Yu, F.C.H.; Yap, W. Ageing-Friendly Neighbourhoods in Singapore, Asia-Pacific, Europe and North. America: An. Annotated Bibliography; Springer Nature: Cham, Switzerland, 2020. [Google Scholar]
- Bhuyan, M.R.; Lane, A.P.; Moogoor, A.; Močnik, Š.; Yuen, B. Meaning of age-friendly neighbourhood: An exploratory study with older adults and key informants in Singapore. Cities 2021, 107, 102940. [Google Scholar] [CrossRef]
- Cao, Y.; Heng, C.K.; Fung, J.C. Using walk-along interviews to identify environmental factors influencing older adults’ out-of-home behaviors in a high-rise, high-density neighborhood. Int. J. Environ. Res. Public Health 2019, 16, 4251. [Google Scholar] [CrossRef] [Green Version]
- Gan, D.R.Y.; Fung, J.C.; Cho, I.S. Neighborhood experiences of people over age 50: Factor structure and validity of a scale. Gerontologist 2020, 60, 559–571. [Google Scholar] [CrossRef]
- Hou, Y.; Yap, W.; Chua, R.; Song, S.; Yuen, B. The associations between older adults’ daily travel pattern and objective and perceived built environment: A study of three neighbourhoods in Singapore. Transp. Policy 2020, 99, 314–328. [Google Scholar] [CrossRef]
- Song, S.; Yap, W.; Hou, Y.; Yuen, B. Neighbourhood built environment, physical activity, and physical health among older adults in Singapore: A simultaneous equations approach. J. Transp. Health 2020, 18, 100881. [Google Scholar] [CrossRef]
- Tao, Y.; Zhang, W.; Gou, Z.; Jiang, B.; Qi, Y. Planning walkable neighborhoods for “aging in place”: Lessons from five aging friendly districts in Singapore. Sustainability 2021, 13, 1742. [Google Scholar] [CrossRef]
- Loo, B.P.Y.; Lam, W.W.Y.; Mahendran, R.; Katagiri, K. How is the neighborhood environment related to the health of seniors living in Hong Kong, Singapore, and Tokyo? Some insights for promoting aging in place. Ann. Am. Assoc. Geogr. 2017, 4, 812–828. [Google Scholar] [CrossRef]
- Bhuyan, M.R.; Yuen, B. Older adults’ views of the connections between neighbourhood built environment and health in Singapore. J. Popul. Ageing 2021, 1–21. [Google Scholar] [CrossRef]
- Hee, L. Singapore’s public housing spaces: Alter–‘native’ spaces in transition. In Dissent and Cultural Resistance in Asia’s Cities; Butcher, M., Velayutham, S., Eds.; Routledge: Oxon, UK, 2009; pp. 72–91. [Google Scholar]
- Wu, T.; Chan, A. Families, friends, and the neighborhood of older adults: Evidence from public housing in Singapore. J. Aging Res. 2011, 2012. [Google Scholar] [CrossRef] [Green Version]
- Niti, M.; Yap, K.B.; Kua, E.H.; Tan, C.H.; Ng, T.P. Physical, social and productive leisure activities, cognitive decline and interaction with APOE-epsilon 4 genotype in Chinese older adults. Int. Psychogeriatr. 2008, 20, 237–251. [Google Scholar] [CrossRef]
- Chong, K.H.; Yow, W.Q.; Loo, D.; Patrycia, F. Psychosocial well-being of the elderly and their perception of matured estate in Singapore. J. Hous. Elder. 2015, 3, 259–297. [Google Scholar] [CrossRef]
- Yuen, B.; Withanage, C.; Nair, P. Surveying Older Adults’ Perceptions and Aspirations. In Ageing and the Built Environment in Singapore; Yuen, B., Ed.; Springer: Cham, Switzerland, 2019; pp. 1–44. [Google Scholar]
- Bozovic-Stamenovic, R. A supportive healthful housing environment for ageing: Singapore experiences and potentials for improvements. Asia Pac. J. Soc. Work 2015, 25, 198–212. [Google Scholar] [CrossRef]
- Trivic, Z.; Low, K.E.Y. Studying multi-sensory neighbourhoods and ageing-friendly design: Methodological propositions. In Nouveaux Territoires De L’expérience Olfactive; Bonnaud, X., Fraigneau, V., Eds.; Infolio: Gollion, Switzerland, 2021; pp. 179–196. [Google Scholar]







| Bangkit | Clementi | |||
|---|---|---|---|---|
| Gender | n | % | n | % |
| Male | 94 | 40.2 | 36 | 54.5 |
| Female | 140 | 59.8 | 30 | 45.5 |
| Total Valid | 234 | 100.0 | 66 | 100.0 |
| Missing | 1 | 0 | ||
| Total | 235 | 66 | ||
| Age | n | % | n | % |
| Adult (18–49) | 65 | 29.0 | 12 | 18.2 |
| Oldish (50–64) | 73 | 32.6 | 13 | 19.7 |
| Young-Old (65–74) | 56 | 25.0 | 24 | 36.4 |
| Old (75+) | 30 | 13.4 | 17 | 25.8 |
| Total Valid | 224 | 100.0 | 66 | 100.0 |
| Missing | 11 | 0 | ||
| Total | 235 | 66 | ||
| Ethnicity | n | % | n | % |
| Chinese | 211 | 90.2 | 58 | 87.9 |
| Malay | 10 | 4.3 | 4 | 6.1 |
| Indian | 12 | 5.1 | 2 | 3.0 |
| Other | 1 | 0.4 | 2 | 3.0 |
| Total Valid | 234 | 100.0 | 66 | 100.0 |
| Missing | 1 | 0 | ||
| Total | 235 | 66 | ||
| Bangkit | Clementi | |||
|---|---|---|---|---|
| n | % | n | % | |
| One sensory impairment | 47 | 20.0 | 18 | 27.2 |
| Two or more sensory impairments | 12 | 5.1 | 4 | 6.1 |
| Any sensory impairment | 59 | 25.1 | 22 | 33.3 |
| No sensory impairment | 176 | 74.9 | 44 | 66.7 |
| Total | 235 | 100.0 | 66 | 100.0 |
| Bangkit | Clementi | |||||||
|---|---|---|---|---|---|---|---|---|
| n (S.Im) | % of Total S.Im | n (A.Gr) | % of A.Gr | n (S.Im) | % of Total S.Im | n (A.Gr) | % of A.Gr | |
| Adult (18–49) | 3 | 5.5 | 65 | 4.6 | 4 | 9.1 | 12 | 16.7 |
| Oldish (50–64) | 19 | 34.5 | 73 | 26.0 | 5 | 22.7 | 13 | 38.5 |
| Young-Old (65–74) | 18 | 32.7 | 56 | 32.1 | 9 | 40.9 | 24 | 37.5 |
| Old (75+) | 15 | 27.3 | 30 | 50.0 | 6 | 27.3 | 17 | 35.3 |
| Total (S.Im.) | 55 | 100.0 | 224 | 24.5 | 22 | 100.0 | 66 | 33.3 |
| Missing | 11 | 0 | ||||||
| Bangkit | Clementi | |||||
|---|---|---|---|---|---|---|
| n | % | % of Cases 1 | n | % | % of Cases 1 | |
| Poor Vision | 34 | 43.4 | 54.1 | 13 | 46.4 | 56.5 |
| Poor Hearing | 19 | 25.0 | 31.1 | 4 | 14.3 | 17.4 |
| Poor Smell Detection | 3 | 3.9 | 4.9 | 0 | 0.0 | 0.0 |
| Walking Difficulties | 19 | 25.0 | 31.1 | 10 | 35.7 | 43.5 |
| Cognitive Difficulties | 0 | 0% | 0.0 | 1 | 3.6 | 4.3 |
| Other | 2 | 2.6 | 3.3 | 0 | 0.0 | 0.0 |
| Total Answers | 76 | 100.0 | 124.6 | 28 | 100.0 | 121.7 |
| Total Cases | 61 | 23 | ||||
| Bangkit | Clementi | |||
|---|---|---|---|---|
| n | % | N | % | |
| Poor (1) | 5 | 2.2 | 1 | 1.5 |
| Could be better (2) | 32 | 14.2 | 20 | 30.8 |
| Good (3) | 108 | 48.0 | 24 | 36.9 |
| Very good (4) | 45 | 20.0 | 15 | 23.1 |
| Excellent (5) | 35 | 15.6 | 5 | 7.7 |
| Total Valid | 225 | 100.0 | 65 | 100.0 |
| Missing | 10 | 1 | ||
| Total | 235 | 66 | ||
| Bangkit | Clementi | |||||
|---|---|---|---|---|---|---|
| Mean | n | Std. Dev. | Mean | n | Std. Dev. | |
| Adult (18–49) | 3.78 | 64 | 0.983 | 3.50 | 12 | 1.087 |
| Oldish (50–64) | 3.23 | 69 | 0.942 | 2.92 | 13 | 0.760 |
| Young-Old (65–74) | 3.04 | 54 | 0.846 | 3.00 | 23 | 0.953 |
| Old (75 and over) | 2.96 | 27 | 0.980 | 2.88 | 17 | 0.993 |
| Total Valid | 3.31 | 214 | 0.983 | 3.05 | 65 | 0.959 |
| Missing | 10 | 1 | ||||
| Total | 234 | 66 | ||||
| Bangkit | Clementi | |||
|---|---|---|---|---|
| n | % | n | % | |
| >3 times per day (1) | 42 | 18.1 | 15 | 22.7 |
| 2–3 times a day (2) | 85 | 36.6 | 25 | 37.9 |
| Once a day (3) | 64 | 27.6 | 16 | 24.2 |
| Few times every week (4) | 34 | 14.7 | 9 | 13.6 |
| Few times every month (5) | 7 | 3.0 | 1 | 1.5 |
| Total Valid | 232 | 100.0 | 66 | 100.0 |
| Missing | 3 | 0 | ||
| Total | 235 | 66 | ||
| Bangkit | Clementi | |||||
|---|---|---|---|---|---|---|
| n | % | % of Cases 1 | n | % | % of Cases 1 | |
| Commuting | 111 | 14.4 | 47.4 | 22 | 10.8 | 33.3 |
| Strolling | 79 | 10.2 | 33.8 | 28 | 13.8 | 42.4 |
| Shopping | 149 | 19.3 | 63.7 | 28 | 13.8 | 42.4 |
| Eating | 145 | 18.8 | 62.0 | 45 | 22.2 | 68.2 |
| Playing | 13 | 1.7 | 5.6 | 0 | 0.0 | 0.0 |
| Exercising | 85 | 11.0 | 36.3 | 26 | 12.8 | 39.4 |
| Meeting Friends | 100 | 12.9 | 42.7 | 31 | 15.3 | 47.0 |
| Gardening | 40 | 5.2 | 17.1 | 1 | 0.5 | 1.5 |
| Visiting Community Organisations | 48 | 6.2 | 20.5 | 21 | 10.3 | 31.8 |
| Other | 6 | 0.8 | 2.6 | 1 | 0.5 | 1.5 |
| Total Answers | 772 | 100.0 | 331.7 | 203 | 100.0 | 307.6 |
| Total Cases | 234 | 66 | ||||
| Bangkit | Clementi | |||||
|---|---|---|---|---|---|---|
| Mean | n | Std. Dev. | Mean | n | Std. Dev. | |
| Q10a Aesthetically appealing (H = better) | 3.87 | 216 | 0.703 | 3.88 | 66 | 0.734 |
| Q10b Distinguishable ambiences (H = better) | 3.76 | 217 | 0.706 | 3.52 | 65 | 0.986 |
| Q10c Different cultures (H = better) | 3.63 | 209 | 0.852 | 3.52 | 66 | 0.965 |
| Q10d Too crowded (L = better) | 3.15 | 216 | 0.953 | 2.76 | 66 | 1.096 |
| Q10e Clean and tidy (H = better) | 3.86 | 217 | 0.851 | 3.42 | 65 | 1.059 |
| Q10f Smelly (L = better) | 2.44 | 216 | 0.948 | 2.6 | 65 | 1.101 |
| Q10g Noisy (L = better) | 2.64 | 217 | 1.076 | 2.5 | 66 | 1.085 |
| Q10h Overwhelming (L = better) | 2.55 | 211 | 0.972 | 2.63 | 65 | 1.069 |
| Bangkit | Clementi | ||||
|---|---|---|---|---|---|
| Age | Health | Age | Health | ||
| Q10a Aesthetically appealing | Corr. Coef. (r) | −0.005 | 0.108 | 0.071 | 0.162 |
| Sig. (2-tailed) (p) | 0.948 | 0.120 | 0.570 | 0.196 | |
| N | 207 | 209 | 66 | 65 | |
| Q10b Distinguishable ambiences | Corr. Coef. (r) | −0.067 | 0.108 | −0.083 | 0.305 ** |
| Sig. (2-tailed) (p) | 0.339 | 0.118 | 0.512 | 0.014 | |
| N | 207 | 210 | 65 | 64 | |
| Q10c Different cultures | Corr. Coef. (r) | 0.030 | 0.052 | −0.086 | 0.210 |
| Sig. (2-tailed) (p) | 0.675 | 0.465 | 0.490 | 0.094 | |
| N | 199 | 202 | 66 | 65 | |
| Q10d Too crowded | Corr. Coef. (r) | −0.138 ** | −0.055 | −0.011 | 0.176 |
| Sig. (2-tailed) (p) | 0.048 | 0.431 | 0.928 | 0.162 | |
| N | 206 | 209 | 66 | 65 | |
| Q10e Clean and tidy | Corr. Coef. (r) | 0.070 | 0.139 ** | 0.157 | 0.065 |
| Sig. (2-tailed) (p) | 0.319 | 0.044 | 0.210 | 0.612 | |
| N | 207 | 210 | 65 | 64 | |
| Q10f Smelly | Corr. Coef. (r) | 0.018 | −0.180 * | −0.027 | 0.056 |
| Sig. (2-tailed) (p) | 0.792 | 0.009 | 0.832 | 0.661 | |
| N | 207 | 209 | 65 | 64 | |
| Q10g Noisy | Corr. Coef. (r) | −0.107 | −0.178 * | −0.108 | 0.127 |
| Sig. (2-tailed) (p) | 0.125 | 0.010 | 0.389 | 0.315 | |
| N | 207 | 210 | 66 | 65 | |
| Q10h Overwhelming | Corr. Coef. (r) | −0.009 | −0.198 * | 0.171 | −0.051 |
| Sig. (2-tailed) (p) | 0.898 | 0.004 | 0.174 | 0.692 | |
| N | 201 | 204 | 65 | 64 | |
| Bangkit | Clementi | |||||
|---|---|---|---|---|---|---|
| Mean | n | Std. Dev. | Mean | n | Std. Dev. | |
| Q11a Obstacles to walk (L = better) | 2.81 | 203 | 1.009 | 2.54 | 66 | 1.236 |
| Q11b Slippery floors (L = better) | 2.86 | 207 | 1.059 | 3.21 | 66 | 1.157 |
| Q11c Hesitate to go out (L = better) | 2.19 | 203 | 0.984 | 2.29 | 65 | 1.1 |
| Q11d Cannot find my way (L = better) | 2.08 | 206 | 0.965 | 2.33 | 66 | 1.114 |
| Q11e Nature (H = better) | 4.06 | 207 | 0.725 | 3.94 | 66 | 1.006 |
| Q11f Avoid messy and dark places (H = better) | 3.3 | 206 | 1.159 | 3.29 | 65 | 1.086 |
| Q11g Prefer sheltered pathways (H = better) | 4.15 | 204 | 0.805 | 3.73 | 66 | 0.887 |
| Bangkit | Clementi | ||||
|---|---|---|---|---|---|
| Age | Health | Age | Health | ||
| Q11a Obstacles to walk | Corr. Coef. (r) | 0.037 | −0.254 ** | 0.044 | 0.079 |
| Sig. (2-tailed) (p) | 0.606 | 0.000 | 0.725 | 0.529 | |
| N | 193 | 196 | 66 | 65 | |
| Q11b Slippery floors | Corr. Coef. (r) | −0.087 | −0.162 * | 0.016 | −0.024 |
| Sig. (2-tailed) (p) | 0.223 | 0.022 | 0.900 | 0.850 | |
| N | 197 | 200 | 66 | 65 | |
| Q11c Hesitate to go out | Corr. Coef. (r) | 0.255 ** | −0.236 ** | 0.169 | 0.120 |
| Sig. (2-tailed) (p) | 0.000 | 0.001 | 0.179 | 0.344 | |
| N | 193 | 196 | 65 | 64 | |
| Q11d Cannot find my way | Corr. Coef. (r) | 0.147 * | −0.179 * | 0.140 | −0.029 |
| Sig. (2-tailed) (p) | 0.040 | 0.011 | 0.262 | 0.817 | |
| N | 196 | 199 | 66 | 65 | |
| Q11e Nature | Corr. Coef. (r) | −0.191 ** | 0.158 * | 0.055 | 0.115 |
| Sig. (2-tailed) (p) | 0.007 | 0.026 | 0.661 | 0.360 | |
| N | 197 | 200 | 66 | 65 | |
| Q11f Avoid messy and dark places | Corr. Coef. (r) | −0.089 | −0.162 * | 0.025 | −0.086 |
| Sig. (2-tailed) (p) | 0.212 | 0.022 | 0.843 | 0.499 | |
| N | 197 | 199 | 65 | 64 | |
| Q11g Prefer sheltered pathways | Corr. Coef. (r) | −0.076 | −0.038 | −0.007 | 0.069 |
| Sig. (2-tailed) (p) | 0.291 | 0.595 | 0.952 | 0.583 | |
| N | 195 | 197 | 66 | 65 | |
| Bangkit | Clementi | |||||
|---|---|---|---|---|---|---|
| Mean | n | Std. Dev. | Mean | n | Std. Dev. | |
| Q12a Amenities (H = better) | 4.03 | 203 | 0.652 | 4.06 | 64 | 0.588 |
| Q12b Different generations (H = better) | 3.77 | 200 | 0.845 | 3.81 | 64 | 0.794 |
| Q12c Elderly-friendly (H = better) | 3.84 | 200 | 0.779 | 3.79 | 66 | 1.015 |
| Q12d Happy (H = better) | 4.27 | 203 | 0.702 | 4.24 | 66 | 0.703 |
| Bangkit | Clementi | ||||
|---|---|---|---|---|---|
| Age | Health | Age | Health | ||
| Q12a Amenities | Corr. Coef. (r) | −0.009 | 0.151 * | −0.021 | 0.048 |
| Sig. (2-tailed) (p) | 0.902 | 0.034 | 0.871 | 0.709 | |
| N | 194 | 197 | 64 | 63 | |
| Q12b Different generations | Corr. Coef. (r) | −0.108 | 0.002 | 0.154 | 0.120 |
| Sig. (2-tailed) (p) | 0.138 | 0.982 | 0.223 | 0.348 | |
| N | 191 | 194 | 64 | 63 | |
| Q12c Elderly-friendly | Corr. Coef. (r) | 0.040 | 0.262 ** | 0.112 | 0.106 |
| Sig. (2-tailed) (p) | 0.579 | 0.000 | 0.372 | 0.401 | |
| N | 191 | 194 | 66 | 65 | |
| Q12d Happy | Corr. Coef. (r) | −0.021 | 0.213 ** | −0.024 | 0.397 ** |
| Sig. (2-tailed) (p) | 0.770 | 0.003 | 0.849 | 0.001 | |
| N | 194 | 197 | 66 | 65 | |
| Q10a Aesthetically Appealing | Q10g Noisy | Q10h Overwhelming | Q11a Too ManyObstacles | Q11c Hesitate to Go Out | Q12a Amenities | Q12d Happy | ||
|---|---|---|---|---|---|---|---|---|
| Q10b Distinguishable Ambiences | Corr. Coef. (r) | 0.422 ** | ||||||
| Sig. (2-tailed) (p) | 0.000 | |||||||
| N | 215 | |||||||
| Q10f Smelly | Corr. Coef. (r) | 0.447 ** | 0.437 ** | |||||
| Sig. (2-tailed) (p) | 0.000 | 0.000 | ||||||
| N | 215 | 209 | ||||||
| Q11b Slippery Floors | Corr. Coef. (r) | 0.595 ** | ||||||
| Sig. (2-tailed) (p) | 0.000 | |||||||
| N | 203 | |||||||
| Q11d Cannot Find My Way | Corr. Coef. (r) | 0.505 ** | ||||||
| Sig. (2-tailed) (p) | 0.000 | |||||||
| N | 202 | |||||||
| Q12b Different Generations | Corr. Coef. (r) | 0.483 ** | ||||||
| Sig. (2-tailed) (p) | 0.000 | |||||||
| N | 199 | |||||||
| Q12c Elderly-Friendly Design | Corr. Coef. (r) | 0.438 ** | 0.427 ** | |||||
| Sig. (2-tailed) (p) | 0.000 | 0.000 | ||||||
| N | 199 | 200 | ||||||
| Q12d Happy | Corr. Coef. (r) | 0.498 ** | ||||||
| Sig. (2-tailed) (p) | 0.000 | |||||||
| N | 202 | |||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Trivic, Z. A Study of Older Adults’ Perception of High-Density Housing Neighbourhoods in Singapore: Multi-Sensory Perspective. Int. J. Environ. Res. Public Health 2021, 18, 6880. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18136880
Trivic Z. A Study of Older Adults’ Perception of High-Density Housing Neighbourhoods in Singapore: Multi-Sensory Perspective. International Journal of Environmental Research and Public Health. 2021; 18(13):6880. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18136880
Chicago/Turabian StyleTrivic, Zdravko. 2021. "A Study of Older Adults’ Perception of High-Density Housing Neighbourhoods in Singapore: Multi-Sensory Perspective" International Journal of Environmental Research and Public Health 18, no. 13: 6880. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18136880