
Baduanjin Qigong Intervention by Telerehabilitation (TeleParkinson): A Proof-of-Concept Study in Parkinson’s Disease

 ,
, 
Abstract
:1. Introduction
2. Material and Methods
2.1. Study Design, Sample Characteristics, and Ethics
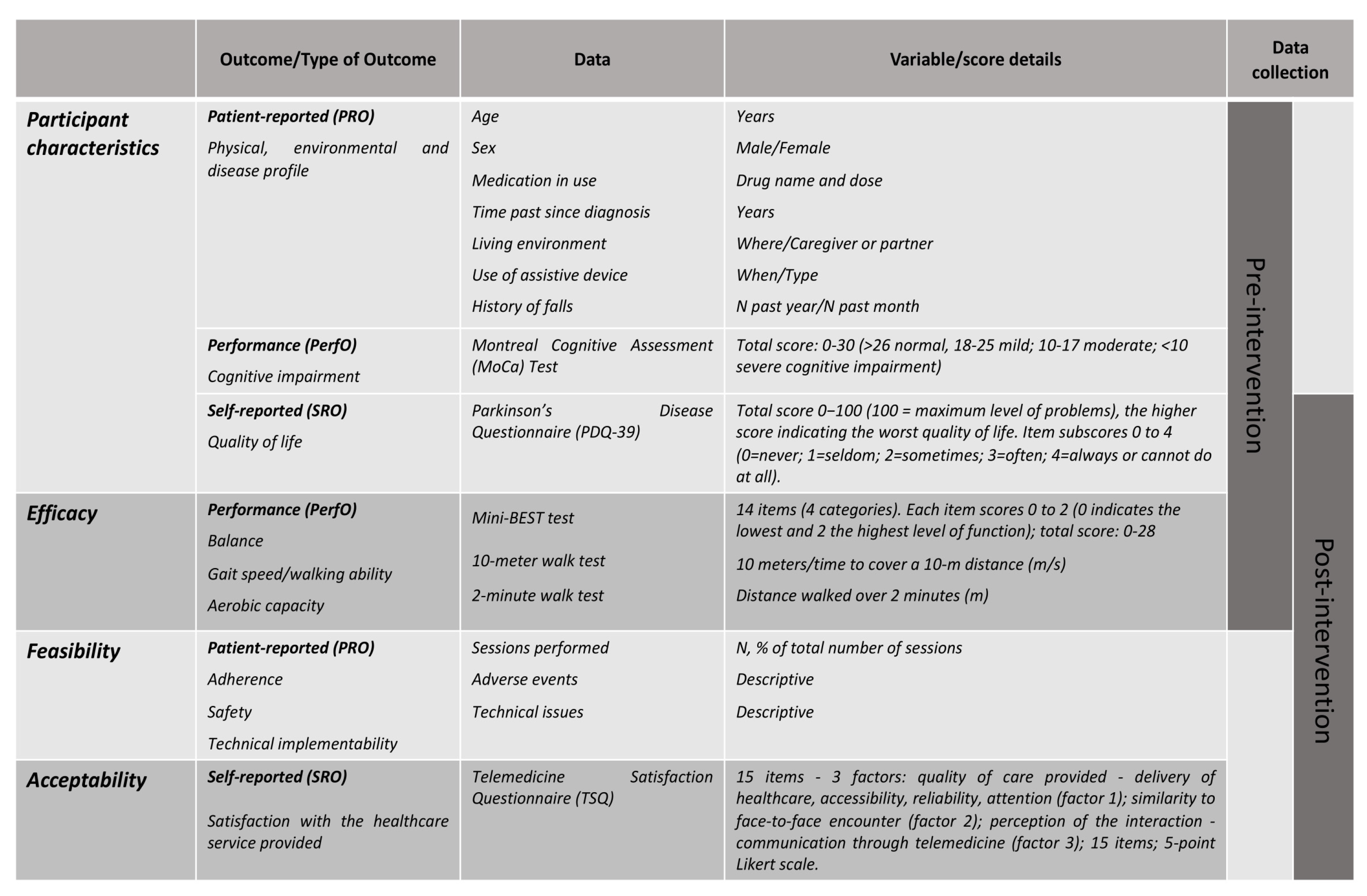
2.2. Measures
2.3. Intervention: The Baduanjin Qigong Exercise Program
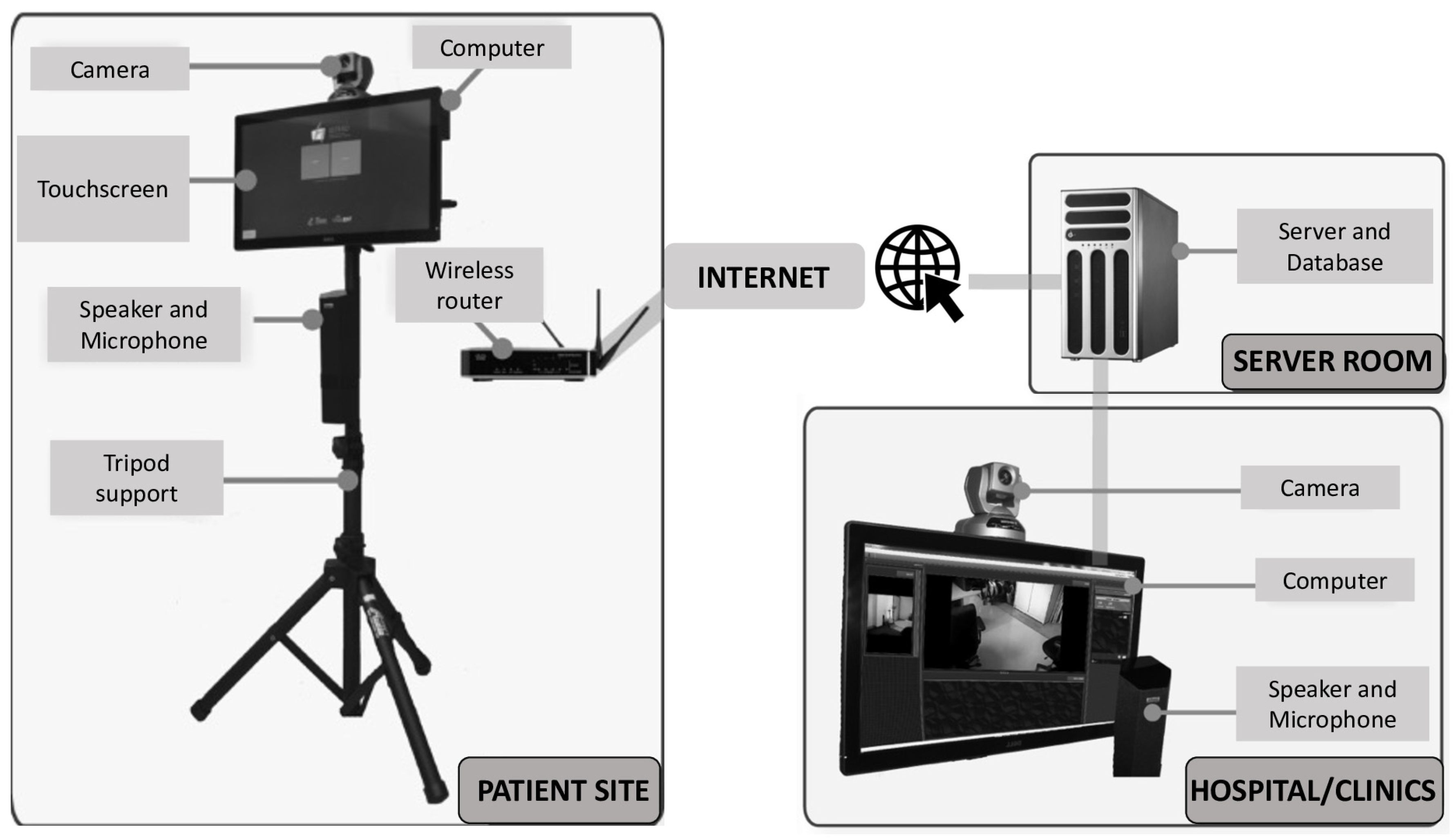
2.4. The Telerehabilitation Platform
2.5. Analysis
3. Results
3.1. Sample Characteristics
3.2. Adherence and Adverse Events
3.3. Feasibility
3.4. Acceptability
3.5. Potential Efficacy
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- DeMaagd, G.; Philip, A. Parkinson’s disease and its management part 1: Disease entity, risk factors, pathophysiology, clinical presentation, and diagnosis. Pharm. Ther. 2015, 40, 504–532. [Google Scholar]
- Alves, G.; Wentzel-Larsen, T.; Aarsland, D.; Larsen, J.P. Progression of motor impairment and disability in Parkinson disease: A population-based study. Neurology 2005, 65, 1436–1441. [Google Scholar] [CrossRef] [PubMed]
- Allen, N.E.; Schwarzel, A.K.; Canning, C.G. Recurrent Falls in Parkinson’s Disease: A Systematic Review. Park. Dis. 2013, 2013, 906274. [Google Scholar] [CrossRef] [Green Version]
- Shahgholi, L.; De Jesus, S.; Wu, S.S.; Pei, Q.; Hassan, A.; Armstrong, M.J.; Martinez-Ramirez, D.; Schmidt, P.; Okun, M.S. Hospitalization and rehospitalization in Parkinson disease patients: Data from the Na-tional Parkinson Foundation Centers of Excellence. PLoS ONE 2017, 12, e0180425. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weerkamp, N.J.; Tissingh, G.; Poels, P.J.; Zuidema, S.U.; Munneke, M.; Koopmans, R.T.; Bloem, B.R. Parkinson Disease in Long Term Care Facilities: A Review of the Literature. J. Am. Med. Dir. Assoc. 2014, 15, 90–94. [Google Scholar] [CrossRef] [PubMed]
- Fan, Y.; Liang, X.; Han, L.; Shen, Y.; Shen, B.; Chen, C.; Sun, Y.; Wang, J.; Tang, Y. Determinants of Quality of Life According to Cognitive Status in Parkinson’s Disease. Front. Aging Neurosci. 2020, 12, 269. [Google Scholar] [CrossRef] [PubMed]
- Dorsey, E.R.; Elbaz, A.; Nichols, E.; Abd-Allah, F.; Abdelalim, A.; Adsuar, J.C.; Ansha, M.G.; Brayne, C.; Choi, J.-Y.J.; Collado-Mateo, D.; et al. Global, regional, and national burden of Parkinson’s disease, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2018, 17, 939–953. [Google Scholar] [CrossRef] [Green Version]
- Public Health Agency of Canada (PHAC); Neurological Health Charities Canada (NHCC). Mapping Connections: An Understanding of Neurological Conditions in Canada; PHAC: Ottawa, ON, Canada, 2014.
- Statistics Canada. Table 17-10-0005-01 Population Estimates on 1 July by Age and Sex. Available online: https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1710000501 (accessed on 18 October 2020).
- Canadian Institute for Health Information (CIHI). The Burden of Neurological Diseases, Disorders and Injuries in Canada; Canadian Institute for Health Information (CIHI): Ottawa, ON, Canada, 2007. [Google Scholar]
- Parkinson Canada. Written Submission for the Pre-Budget Consultations in Advance of the 2020 Budget. Available online: https://www.ourcommons.ca/Content/Committee/421/FINA/Brief/BR10596290/br-external/ParkinsonCanada-e.pdf (accessed on 18 October 2020).
- Dodel, R.; Tinelli, M.; Deuschl, G.; Petersen, G.; Oertel, W.; Ahmerkamp-Böhme, J. The economic benefit of timely, adequate, and adherence to Parkinson’s disease treatment: The Value of Treatment Project 2. Eur. J. Neurol. 2021, 28, 707–716. [Google Scholar] [CrossRef]
- People with Parkinson’s Face Gaps in the Availability of Health Services. Available online: https://www.ipsos.com/en-ca/news-polls/parkinson-canada-stakeholder-survey-2018 (accessed on 18 October 2020).
- Achey, M.; Aldred, J.L.; Aljehani, N.; Bloem, B.R.; Biglan, K.M.; Chan, P.; Cubo, E.; Dorsey, E.R.; Goetz, C.G.; Guttman, M.; et al. The past, present, and future of telemedicine for Parkinson’s disease. Mov. Disord. 2014, 29, 871–883. [Google Scholar] [CrossRef]
- Isernia, S.; Di Tella, S.; Pagliari, C.; Jonsdottir, J.; Castiglioni, C.; Gindri, P.; Salza, M.; Gramigna, C.; Palumbo, G.; Molteni, F.; et al. Effects of an Innovative Telerehabilitation Intervention for People with Parkinson’s Disease on Quality of Life, Motor, and Non-motor Abilities. Front. Neurol. 2020, 11, 846. [Google Scholar] [CrossRef]
- Gandolfi, M.; Geroin, C.; Dimitrova, E.; Boldrini, P.; Waldner, A.; Bonadiman, S.; Picelli, A.; Regazzo, S.; Stirbu, E.; Primon, D.; et al. Virtual Reality Telerehabilitation for Postural Instability in Parkinson’s Disease: A Multicenter, Single-Blind, Randomized, Controlled Trial. BioMed Res. Int. 2017, 2017, 7962826. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.-Y.; Guan, B.-S.; Li, Z.-K.; Yang, Q.-H.; Xu, T.-J.; Li, H.-B.; Wu, Q.-Y. Application of telehealth intervention in Parkinson’s disease: A systematic review and meta-analysis. J. Telemed. Telecare 2018, 26, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Caughlin, S.; Mehta, S.; Corriveau, H.; Eng, J.J.; Eskes, G.; Kairy, D.; Meltzer, J.; Sakakibara, B.M.; Teasell, R. Implementing Telerehabilitation After Stroke: Lessons Learned from Canadian Trials. Telemed. e-Health 2020, 26, 710–719. [Google Scholar] [CrossRef]
- Tousignant, M.; Boissy, P.; Corriveau, H.; Moffet, H. In home telerehabilitation for older adults after discharge from an acute hospital or rehabilitation unit: A proof-of-concept study and costs estimation. Disabil. Rehabil. Assist. Technol. 2006, 1, 209–216. [Google Scholar] [CrossRef] [PubMed]
- Orlando, J.F.; Beard, M.; Kumar, S. Systematic review of patient and caregivers’ satisfaction with telehealth videoconferencing as a mode of service delivery in managing patients’ health. PLoS ONE 2019, 14, e0221848. [Google Scholar] [CrossRef] [Green Version]
- Klein, B.C.; Busis, N.A. COVID-19 is catalyzing the adoption of teleneurology. Neurology 2020, 94, 903–904. [Google Scholar] [CrossRef] [Green Version]
- Centers for Disease Control and Prevention. Using Telehealth to Expand access to Essential Health Services during the COVID-19 Pandemic. Coronavirus Disease 2019 (COVID-10). Available online: https://www.cdc.gov/coronavirus/2019-ncov/hcp/telehealth.html (accessed on 18 October 2020).
- Bhalsing, K.S.; Abbas, M.M.; Tan, L.C.S. Role of Physical Activity in Parkinson’s Disease. Ann. Indian Acad. Neurol. 2018, 21, 242–249. [Google Scholar] [CrossRef] [PubMed]
- Morris, M.E.; Martin, C.L.; Schenkman, M.L. Striding out with Parkinson disease: Evidence-based physical therapy for gait disorders. Phys. Ther. 2010, 90, 280–288. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carapellotti, A.M.; Stevenson, R.; Doumas, M. The efficacy of dance for improving motor impairments, non-motor symptoms, and quality of life in Parkinson’s disease: A systematic review and meta-analysis. PLoS ONE 2020, 15, e0236820. [Google Scholar] [CrossRef]
- Xiao, C.; Zhuang, Y.; Kang, Y. Effect of Health Qigong Baduanjin on Fall Prevention in Individuals with Parkinson’s Disease. J. Am. Geriatr. Soc. 2016, 64, e227–e228. [Google Scholar] [CrossRef] [PubMed]
- Xiao, C.M.; Zhuang, Y.C. Effect of Health Baduanjin Qigong for mild to moderate Parkinson’s Disease. Geriatr. Gerontol. Int. 2016, 16, 911–919. [Google Scholar] [CrossRef]
- Moreira, A.; Matos, L.C.; Conceição, A.M. Does Qigong Practice Have Benefits on the Management of Parkinson’s Disease? J—Multidiscip. Sci. J. 2019, 2, 352–363. [Google Scholar] [CrossRef] [Green Version]
- Chen, S.; Zhang, Y.; Wang, Y.T.; Liu, X.; Song, W.; Du, X. The effect of Qigong-based therapy on patients with Parkinson’s disease: A systematic review and meta-analysis. Clin. Rehabil. 2020, 34, 1436–1448. [Google Scholar] [CrossRef]
- Choi, H.-J.; Garber, C.E.; Jun, T.-W.; Jin, Y.-S.; Chung, S.-J.; Kang, H.-J. Therapeutic Effects of Tai Chi in Patients with Parkinson’s Disease. ISRN Neurol. 2013, 2013, 1–7. [Google Scholar] [CrossRef]
- Hackney, M.E.; Earhart, G.M. Tai Chi improves balance and mobility in people with Parkinson disease. Gait Posture 2008, 28, 456–460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amano, S.; Nocera, J.R.; Vallabhajosula, S.; Juncos, J.L.; Gregor, R.J.; Waddell, D.E.; Wolf, S.L.; Hass, C.J. The effect of Tai Chi exercise on gait initiation and gait performance inpersons with Parkinson’s disease. Parkinsonism Relat. Disord. 2013, 19, 955–960. [Google Scholar] [CrossRef] [Green Version]
- Li, F.; Harmer, P.; Fitzgerald, K.; Eckstrom, E.; Stock, R.; Galver, J.; Maddalozzo, G.; Batya, S.S. Tai Chi and Postural Stability in Patients with Parkinson’s Disease. N. Engl. J. Med. 2012, 366, 511–519. [Google Scholar] [CrossRef] [Green Version]
- Ni, X.; Liu, S.; Lu, F.; Shi, X.; Guo, X. Efficacy and Safety of Tai Chi for Parkinson’s Disease: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. PLoS ONE 2014, 9, e99377. [Google Scholar] [CrossRef]
- Liu, H.H.; Yeh, N.C.; Wu, Y.F.; Yang, Y.R.; Wang, R.Y.; Cheng, F.Y. Effects of Tai Chi Exercise on Reducing Falls and Improving Balance Performance in Parkinson’s Disease: A Meta-Analysis. Parkinson’s Dis. 2019, 2019. [Google Scholar] [CrossRef]
- Kamieniarz, A.; Milert, A.; Grzybowska-Ganszczyk, D.; Opara, J.; Juras, G. Tai Chi and Qi Gong therapies as a complementary treatment in Parkinson’s disease—A systematic review. Complement. Ther. Med. 2021, 56, 102589. [Google Scholar] [CrossRef]
- Yu, X.; Wu, X.; Hou, G.; Han, P.; Jiang, L.; Guo, Q. The Impact of Tai Chi on Motor Function, Balance, and Quality of Life in Parkinson’s Disease: A Systematic Review and Meta-Analysis. Evid. Based Complement. Altern. Med. 2021, 2021, 6637612. [Google Scholar] [CrossRef]
- Garcia-Agundez, A.; Folkerts, A.K.; Konrad, R.; Caserman, P.; Tregel, T.; Goosses, M.; Göbel, S.; Kalbe, E. Recent advances in rehabilitation for Parkinson’s Disease with Exergames: A Systematic Review. J. Neuroeng. Rehabil. 2019, 16, 17. [Google Scholar] [CrossRef]
- Lei, C.; Sunzi, K.; Dai, F.; Liu, X.; Wang, Y.; Zhang, B.; He, L.; Ju, M. Effects of virtual reality rehabilitation training on gait and balance in patients with Parkinson’s disease: A systematic review. PLoS ONE 2019, 14, e0224819. [Google Scholar] [CrossRef] [Green Version]
- Tousignant, M.; Corriveau, H.; Kairy, D.; Berg, K.; Dubois, M.-F.; Gosselin, S.; Swartz, R.H.; Boulanger, J.-M.; Danells, C. Tai Chi-based exercise program provided via telerehabilitation compared to home visits in a post-stroke population who have returned home without intensive rehabilitation: Study protocol for a randomized, non-inferiority clinical trial. Trials 2014, 15, 42. [Google Scholar] [CrossRef] [Green Version]
- Tousignant, M.; Moffet, H.; Boissy, P.; Corriveau, H.; Cabana, F.; Marquis, F. A randomized controlled trial of home telerehabilitation for post-knee arthroplasty. J. Telemed. Telecare 2011, 17, 195–198. [Google Scholar] [CrossRef]
- Goetz, C.G.; Tilley, B.C.; Shaftman, S.R.; Stebbins, G.T.; Fahn, S.; Martinez-Martin, P.; Poewe, W.; Sampaio, C.; Stern, M.B.; Dodel, R.; et al. Movement Disorder Society-Sponsored Revision of the Unified Parkinson’s Disease Rating Scale (MDS-UPDRS): Scale presentation and clinimetric testing results. Mov. Disord. 2008, 23, 2129–2170. [Google Scholar] [CrossRef]
- Cummings, J.L. Mini-Mental State Examination. Norms, normals, and numbers. JAMA 1993, 269, 2420–2421. [Google Scholar] [CrossRef]
- Yip, M.P.; Chang, A.M.; Chan, J.; Mackenzie, A.E. Development of the Telemedicine Satisfaction Questionnaire to evaluate patient satisfaction with telemedicine: A preliminary study. J. Telemed. Telecare 2003, 9, 46–50. [Google Scholar] [CrossRef]
- Mayo, N.E.; Figueiredo, S.; Ahmed, S.; Bartlett, S.J. Montreal Accord on Patient-Reported Outcomes (PROs) use series—Paper 2: Terminology proposed to measure what matters in health. J. Clin. Epidemiol. 2017, 89, 119–124. [Google Scholar] [CrossRef]
- Auquier, P.; Sapin, C.; Ziegler, M.; Tison, F.; Destée, A.; Dubois, B.; Allicar, M.P.; Thibault, J.L.; Jenkinson, C.; Peto, V. Validation of the French language version of the Parkinson’s Disease Questionnaire-PDQ-39. Rev. Neurol. 2002, 158, 41–50. [Google Scholar] [PubMed]
- Nasreddine, Z.S.; Phillips, N.A.; Bedirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A Brief Screening Tool for Mild Cognitive Impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef]
- Franchignoni, F.; Horak, F.; Godi, M.; Nardone, A.; Giordano, A. Using psychometric techniques to improve the Balance Evaluation Systems Test: The mini-BESTest. J. Rehabil. Med. 2010, 42, 323–331. [Google Scholar] [CrossRef] [Green Version]
- Lindholm, B.; Nilsson, M.H.; Hansson, O.; Hagell, P. The clinical significance of 10-m walk test standardizations in Parkinson’s disease. J. Neurol. 2018, 265, 1829–1835. [Google Scholar] [CrossRef] [Green Version]
- White, D.K.; Wagenaar, R.C.; Ellis, T.D.; Tickle-Degnen, L. Changes in Walking Activity and Endurance Following Rehabilitation for People with Parkinson Disease. Arch. Phys. Med. Rehabil. 2009, 90, 43–50. [Google Scholar] [CrossRef]
- Tousignant, M.; Corriveau, H.; Roy, P.M.; Desrosiers, J.; Dubuc, N.; Hebert, R. Efficacy of supervised Tai Chi exercises versus conventional physical therapy exercises in fall prevention for frail older adults: A randomized controlled trial. Disabil. Rehabil. 2013, 35, 1429–1435. [Google Scholar] [CrossRef] [PubMed]
- Steffen, T.; Seney, M. Test-Retest Reliability and Minimal Detectable Change on Balance and Ambulation Tests, the 36-Item Short-Form Health Survey, and the Unified Parkinson Disease Rating Scale in People with Parkinsonism. Phys. Ther. 2008, 88, 733–746. [Google Scholar] [CrossRef] [PubMed]
- Anson, E.; Thompson, E.; Ma, L.; Jeka, J. Reliability and Fall Risk Detection for the BESTest and Mini-BESTest in Older Adults. J. Geriatr. Phys. Ther. 2019, 42, 81–85. [Google Scholar] [CrossRef]
- Godi, M.; Franchignoni, F.; Caligari, M.; Giordano, A.; Turcato, A.M.; Nardone, A. Comparison of reliability, validity, and responsiveness of the Mini-BESTest and berg balance scale in patients with balance disorders. Phys. Ther. 2013, 93, 158–167. [Google Scholar] [CrossRef] [Green Version]
- Chan, W.L.; Pin, T.W. Reliability, validity and minimal detectable change of 2-minute walk test, 6-minute walk test and 10-meter walk test in frail older adults with dementia. Exp. Gerontol. 2019, 115, 9–18. [Google Scholar] [CrossRef]
- Gijbels, D.; Eijnde, B.; Feys, P. Comparison of the 2- and 6-minute walk test in multiple sclerosis. Mult. Scler. J. 2011, 17, 1269–1272. [Google Scholar] [CrossRef]
- Peto, V.; Jenkinson, C.; Fitzpatrick, R. Determining minimally important differences for the PDQ-39 Parkinson’s disease questionnaire. Age Ageing 2001, 30, 299–302. [Google Scholar] [CrossRef] [Green Version]
- Miele, G.; Straccia, G.; Moccia, M.; Leocani, L.; Tedeschi, G.; Bonavita, S.; Lavorgna, L.; Padovani, A.; Clerico, M.; Brigo, F.; et al. Telemedicine in Parkinson’s Disease: How to Ensure Patient Needs and Continuity of Care at the Time of COVID-19 Pandemic. Telemed. e-Health 2020, 26, 1533–1536. [Google Scholar] [CrossRef]
- Liu, X.-Y.; Gao, J.; Yin, B.-X.; Yang, X.-Y.; Bai, D.-X. Efficacy of Ba Duan Jin in Improving Balance: A Study in Chinese Community-Dwelling Older Adults. J. Gerontol. Nurs. 2016, 42, 38–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zou, L.; Yeung, A.; Quan, X.; Hui, S.S.-C.; Hu, X.; Chan, J.S.M.; Wang, C.; Boyden, S.D.; Sun, L.; Wang, H. Mindfulness-Based Baduanjin Exercise for Depression and Anxiety in People with Physical or Mental Illnesses: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2018, 15, 321. [Google Scholar] [CrossRef] [Green Version]
- Sharma, N.K.; Robbins, K.; Wagner, K.; Colgrove, Y.M. A randomized controlled pilot study of the therapeutic effects of yoga in people with Parkinson’s disease. Int. J. Yoga 2015, 8, 74–79. [Google Scholar]
- Li, Q.; Liu, J.; Dai, F.; Dai, F. Tai chi versus routine exercise in patients with early-or mild-stage parkin-son’s disease: A retrospective cohort analysis. Braz. J. Med. Biol. Res. 2020, 53, e9171. [Google Scholar] [CrossRef] [Green Version]
- Yingyongyudha, A.; Saengsirisuwan, V.; Panichaporn, W.; Boonsinsukh, R. The Mini-Balance Evaluation Systems Test (Mini-BESTest) Demonstrates Higher Accuracy in Identifying Older Adult Participants with History of Falls Than Do the BESTest, Berg Balance Scale, or Timed up and Go Test. J. Geriatr. Phys. Ther. 2016, 39, 64–70. [Google Scholar] [CrossRef]
- Leddy, A.L.; Crowner, B.E.; Earhart, G.M. Utility of the Mini-BESTest, BESTest, and BESTest Sections for Balance Assessments in Individuals with Parkinson Disease. J. Neurol. Phys. Ther. 2011, 35, 90–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nemanich, S.; Duncan, R.P.; Dibble, L.E.; Cavanaugh, J.T.; Ellis, T.D.; Ford, M.P.; Foreman, K.B.; Earhart, G.M. Predictors of Gait Speeds and the Relationship of Gait Speeds to Falls in Men and Women with Parkinson Disease. Parkinson Dis. 2013, 2013, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.S.; Lee, E.-N.; Ernst, E. Is tai chi beneficial for improving aerobic capacity? A systematic review. Br. J. Sports Med. 2008, 43, 569–573. [Google Scholar] [CrossRef]
- Mate, K.; Abou-Sharkh, A.; Morais, J.; Mayo, N. Putting the best foot forward: Relationships between indicators of step quality and cadence in three gait vulnerable populations. NeuroRehabilitation 2019, 44, 295–301. [Google Scholar] [CrossRef] [PubMed]
- Tudor-Locke, C.; Han, H.; Aguiar, E.J.; Barreira, T.V.; Schuna, J.M., Jr.; Kang, M.; Rowe, D.A. How fast is fast enough? Walking cadence (steps/min) as a practical estimate of intensity in adults: A narrative review. Br. J. Sports Med. 2018, 52, 776–788. [Google Scholar] [CrossRef] [PubMed]
- Tessier, A.J.; Wing, S.S.; Rahme, E.; Morais, J.A.; Chevalier, S. Physical function-derived cut-points for the diagnosis of sarcopenia and dynapenia from the Canadian longitudinal study on aging. J. Cachexia Sarcopenia Muscle 2019, 10, 985–999. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Participant | ||
|---|---|---|
| ID (W = Woman/M = Man) | A (W) | B (M) |
| Age (years) | 75 | 74 |
| Years since PD diagnosis | 12 | 17 |
| Hoehn and Yahr Stage | 3 | 3 |
| Use of medications # | 3 | 8 |
| Living environment and use of assistive device | Home, with partner, with assistive device for outdoor walking only | Home, with partner, without walking aid |
| History of falls (n past year) | 14 | 3 |
| History of falls (n past month) | 1 | 0 |
| Balance (Mini-Best Test, n/28) * | 11 | 17 |
| Anticipatory (n/6) | 1 | 4 |
| Reactive postural control (n/6) | 0 | 2 |
| Sensory orientation (n/6) | 4 | 2 |
| Dynamic gait (n/10) | 6 | 9 |
| Global cognition (MoCA, n/30) ** | 20 | 26 |
| Quality of life (PDQ-39, n/100) *** | 78 | 68 |
| Participant | A | B | ||
|---|---|---|---|---|
| Timepoints | Pre-Intervention | Post-Intervention | Pre-Intervention | Post-Intervention |
| Self-selected gait speed (m/s) | 0.77 | 1.48 | 1.49 | 1.67 |
| Fast-paced gait speed (m/s) | 0.99 | 1.72 | 1.64 | 2.00 |
| Aerobic capacity (two min walk distance, m) | 112 | 151 | 112 | 146 |
| Balance (Mini-Best total score, n/28) * | 11 | 17 | 18 | 20 |
| Anticipatory (n/6) | 1 | 4 | 3 | 5 |
| Reactive postural control (n/6) | 0 | 2 | 4 | 2 |
| Sensory orientation (n/6) | 4 | 2 | 4 | 3 |
| Dynamic gait (n/10) | 6 | 9 | 7 | 10 |
| Quality of life (PDQ-39 total score, n/100) # | 78 | 68 | 70 | 54 |
| Mobility | 25 | 16 | 30 | 10 |
| Activities of Daily Living | 10 | 15 | 2 | 15 |
| Emotional Wellbeing | 14 | 11 | 11 | 7 |
| Stigma | 9 | 9 | 9 | 9 |
| Social Support | 3 | 1 | 0 | 0 |
| Cognition | 8 | 7 | 8 | 6 |
| Communication | 5 | 5 | 5 | 3 |
| Bodily Discomfort | 4 | 4 | 5 | 4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carvalho, L.P.; Décary, S.; Beaulieu-Boire, I.; Dostie, R.; Lalonde, I.; Texier, É.; Laprise, L.; Pepin, E.; Gilbert, M.; Corriveau, H.; et al. Baduanjin Qigong Intervention by Telerehabilitation (TeleParkinson): A Proof-of-Concept Study in Parkinson’s Disease. Int. J. Environ. Res. Public Health 2021, 18, 6990. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18136990
Carvalho LP, Décary S, Beaulieu-Boire I, Dostie R, Lalonde I, Texier É, Laprise L, Pepin E, Gilbert M, Corriveau H, et al. Baduanjin Qigong Intervention by Telerehabilitation (TeleParkinson): A Proof-of-Concept Study in Parkinson’s Disease. International Journal of Environmental Research and Public Health. 2021; 18(13):6990. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18136990
Chicago/Turabian StyleCarvalho, Livia P., Simon Décary, Isabelle Beaulieu-Boire, Rosalie Dostie, Isabelle Lalonde, Émilie Texier, Laurence Laprise, Elizabeth Pepin, Mélodie Gilbert, Hélène Corriveau, and et al. 2021. "Baduanjin Qigong Intervention by Telerehabilitation (TeleParkinson): A Proof-of-Concept Study in Parkinson’s Disease" International Journal of Environmental Research and Public Health 18, no. 13: 6990. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18136990