1. Introduction
The COVID-19 pandemic swept across the world and has been deemed the most devastating disease since the Spanish Flu in 1918–1919 [
1]. By the end of January 2021, COVID-19 caused over one hundred million confirmed infections and two million deaths worldwide [
2]. Although the first confirmed case was identified in Wuhan in December 2019, and the disease rapidly spread to other parts of China, through strict and effective preventive regulations and fully implemented policies, China was successful in keeping the COVID-19 pandemic under control with the efforts of the entire society.
COVID-19 prevention and control posed greater challenges and more stringent requirements for higher education institutions (HEIs) than for other social organizations. In contrast to other social systems, HEIs have a high density of people, which means that once one student gets it, large-scale pandemic transmission is likely to be triggered due to the high rate of spread of COVID-19 in crowded settlements [
3]. China’s health authorities responded early and quickly regarding COVID-19 prevention in HEIs. In late January 2020, soon after the outbreak of COVID-19, China’s Ministry of Education (MOE) issued a series of notices requesting that all educational institutions take effective epidemic prevention and control measures and postpone the start of the 2020 spring semester. On 13 April 2020, the MOE and the National Health Commission (NHC) released the Scheme on COVID-19 Prevention and Control in HEIs and proposed that comprehensive preventive measures be implemented before, during and after students’ return to campus. After campuses reopened, the Guidelines on COVID-19 Prevention and Control in HEIs for the 2020 autumn semester and for the 2021 spring semester were issued successively by the MOE and NHC. HEIs in China also actively displayed their major functions (talent training, scientific research and social services) during the COVID-19 pandemic by providing professional personnel, knowledge, skills and resources to combat COVID-19 and contribute to the research and development of definitive vaccines and forms of therapy.
Although some countries and regions, including China, have introduced a wide range of vaccinations, given the long-term complexity of the global pandemic situation, the construction and promotion of the preventive literature and behavior are critical in the “new normal” period of COVID-19 in addition to treatment and vaccine development. In fact, increasing numbers of studies added to the understanding of general public preventive behavior in many countries after the outbreak of COVID-19 [
4,
5,
6,
7,
8,
9]. However, few have targeted higher education systems [
10,
11], and most have focused on the role of knowledge and attitudes in predicting students’ COVID-19 preventive behavior [
12]. Thus, although HEIs are regarded as effective settings to shape specific attitudes and behaviors of students through institutional interventions [
13], we still have limited knowledge about how the institutional factors of HEIs are affecting the preventive behaviors of university students and the psychological mechanism underlying this relationship during the outbreak of the COVID-19 pandemic.
To overcome the limitations of existing studies, our study explicitly identifies the impacts of the institutional climate, attitudes, subjective norms, perceived behavioral control and perceived risk of university students’ COVID-19 preventive behaviors based on an extended theory of planned behavior (TPB) model. The TPB model proposed by Ajzen [
14] may be one of the most influential theoretical perspectives to explain a range of health behavior intentions or actual behavior. While the TPB has been used in several recent studies of COVID-19 preventive behaviors [
15], to improve the predictive capabilities of the TPB model, it is necessary to study university students’ COVID-19 preventive behavior by including the institutional climate in the TPB model, because the critical role of HEIs in the prevention and control of COVID-19 has been widely reported in the literature [
16]. Although the existing literature recognizes the moderating role of risk perception on a range of health behaviors [
17], to the best of our knowledge, no previous study has examined the variations in the influence of institutional factors and TPB components on COVID-19 preventive behaviors in terms of different levels of risk perception.
Bearing the above considerations in mind, the key objective of the current research is to employ an extended TPB model to (1) explore the influence of the institutional climate on the COVID-19 preventive behaviors of university students, (2) test the mediating effect of three TPB elements, namely attitudes, subjective norms and perceived behavioral control toward COVID-19 prevention in the relationship between the institutional climate and university students’ preventive behaviors, and (3) investigate the moderating role of perceived risk for the impacts of the institutional climate and TPB elements on university students’ preventive behaviors. The results of our study will contribute to widening the reach of the application of the TPB model in COVID-19 prevention within a higher education context and improve its explanatory capacity by adding external institutional factors and internal perceived risk. Notably, with deeper knowledge of the drivers of university students’ preventive behaviors, the present research can shed further light on anti-epidemic practices and measures in HEIs in China and in other areas suffering the devastating effects of COVID-19.
5. Discussion and Implications
The aim of the current study was to investigate the influencing factors of preventive behaviors for COVID-19 among university students in Beijing, China. With an extended TPB framework, we tested the hypothesized relationships among the institutional climate, three components of the original TPB model and preventive behaviors, as well as the moderating role of perceived risk in the structural relationships. The major research findings are summarized and discussed as follows.
Based on the extended TPB model, we found that the institutional climate was significantly associated with university students’ preventive behaviors against COVID-19. Consistent with previous studies [
35], the results imply that a positive institutional setting with formal policies, procedures and practices concerning COVID-19 prevention and control could enable university students to adaptively face epidemic challenges and facilitate their preventive actions against COVID-19. In addition, countries with different strengths of social norms (or cultural tightness–looseness) were varied in their effectiveness to combat COVID-19 [
64]. Thus, a possible explanation for this relationship may be that an institutional climate creates social norms, duties, obligations and expectations within a specific institution that reinforce the preventive behaviors of students, especially those from tight cultures and collectivist societies such as China [
48,
64]. Moreover, according to the focus theory of normative conduct [
65], the extent to which university students’ preventive behaviors are practiced is highly dependent on the saliency and level of HEIs’ COVID-19 prevention and control measures.
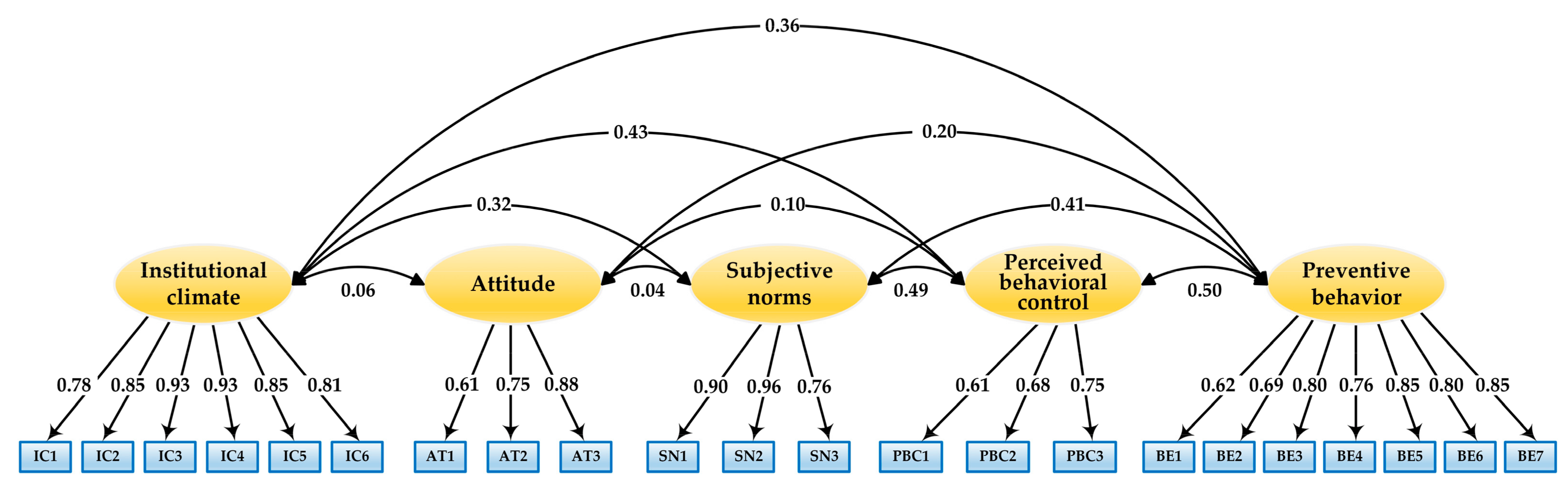
As expected, the results indicate that the institutional climate was significantly related to the three original TPB components, which in turn yielded a significant effect on preventive behaviors. The mediating effects of university students’ attitudes, subjective norms and perceived behavioral control on the relationship between the institutional climate and preventive behaviors were supported via a bootstrapping procedure. Specifically, all three TPB components partially mediated the relationship between the institutional climate and preventive behaviors. These results indicate that attitudes, subjective norms and perceived behavioral control are critical sociopsychological factors that link institutional intervention and students’ actual preventive behaviors toward COVID-19. The results suggest that with increasing emphasis on formal policies, procedures and practices concerning the prevention and control of COVID-19 on campus, university students may be expected to adopt more preventive behaviors, which requires them to possess an understanding of not only COVID-19 prevention knowledge, requirements and recommendations but also a positive emotional disposition, strong perception, substantial normative stimuli and the motivation to perform preventive behaviors; that is, the accessibility of external support, resources and information for COVID-19 prevention might lead to the enhancement of preventive behaviors by shaping the positive environment needed for university students’ active precautionary beliefs to flourish.
Multigroup SEM analyses indicated that perceived risk significantly moderated several paths in the research model. We found that the impacts of the institutional climate on both subjective norms and perceived behavioral control were significantly stronger among university students with a higher level of risk perception than among those with a low level of risk perception. Our study also demonstrated that the influences of the institutional climate and subjective norms on university students’ preventive behaviors were moderated by the perceived risk of COVID-19. Specifically, compared with students with a low level of perceived risk, those with a high level of perceived risk derived more benefits from the institutional climate in terms of the promotion or maintenance of preventive behaviors. These findings are highly similar to those of a recent study that found a moderating role of risk perception on the relationships among institutional factors, self-efficacy and compliance with prevention measures in Italian residents during the COVID-19 outbreak [
46]. This may be explained by the fact that high risk perception students attempted to reduce their uncertainty and anxiety by resolving to accept preventive support, opinions or information from affiliated institutions and important figures and to enact preventive behaviors more strictly, while low risk perception students may have depended more on their own ability and judgment [
66]. Moreover, our study revealed that the effect of the institutional climate on attitudes, as well as the influence of attitudes on preventive behaviors, remained invariant across the high and low risk perception groups. It can be concluded that, regardless of the level of university students’ perception of the risk related to COVID-19, a higher level of perception of the supportive institutional climate toward COVID-19 prevention stably fostered the formation of a positive attitude toward adopting preventive behavior and, in turn, resulted in increased performance of actual behaviors.
Our study has the following theoretical implications. First, it broadens the research on individuals’ preventive behaviors against COVID-19 from an institutional impact perspective with an expanded TPB model within the context of higher education. Although the institutional climate is known to be a key contextual factor for promoting individuals’ disease prevention actions, empirical evidence on the association between the institutional climate and preventive behaviors for COVID-19 is limited. We examined the direct influence of the institutional climate on the preventive behaviors of university students in Beijing, China to fill this gap in the literature. Second, to the best of our knowledge, this is the first attempt to explore quantitative evidence in the potential role of TPB core constructs for bridging the relationship between institutional factors and university students’ preventive behaviors toward COVID-19. Third, our study incorporates perceived risk as a moderator into the TPB model, thus providing more comprehensive insights into the influence mechanism of the institutional climate and TPB components on preventive behaviors. Moreover, our study verifies the scalability and versatility of the extended TPB model as a powerful theoretical basis for future studies of the COVID-19 preventive behaviors of other groups of people from diversified organizations around the world.
Regarding the practical implications, the findings of our study contribute to supporting HEIs’ vital functions in the “new normal” period of COVID-19 in China and offer meaningful information for authorities and HEIs to encourage the adoption of preventive actions among the general public and to prevent the spread of COVID-19. First, by making COVID-19 an urgent and vital political issue, institutional actors can play a powerful and effective role in shaping the social norms of epidemic prevention [
67], because political engagement and social norms represent crucial factors in facilitating prosocial behavior [
68]. Accordingly, HEIs could prompt the creation of an institutional climate for COVID-19 prevention via a series of institutional interventions, including establishing effective prevention and control measures and demonstrating commitment and concrete efforts to ensure the physical and mental health and safety of students and staff on campus and to maintain the normal functions of the institutions. Second, HEIs should contribute to the management and intervention of students’ positive psychological states, which will guide students in deciding which behaviors and protocols to pursue. Thus, we suggest that HEIs configure platforms to provide positive psychological interventions to students to stimulate them to enhance their knowledge, attitudes, norms and behavioral control toward COVID-19 prevention. Moreover, specific institutional interventions might be more efficient for individuals with a high level of risk perception. We propose that HEIs emphasize that more risk and crisis education is especially helpful for enhancing students’ beliefs regarding the obligations of the country, institutions and themselves to make successful efforts to defeat COVID-19.


 ,
, 



{kind=link}
{kind=link}
{kind=link}