
A Systematic Review of Characteristics Associated with COVID-19 in Children with Typical Presentation and with Multisystem Inflammatory Syndrome

 ,
,
Abstract
:1. Introduction
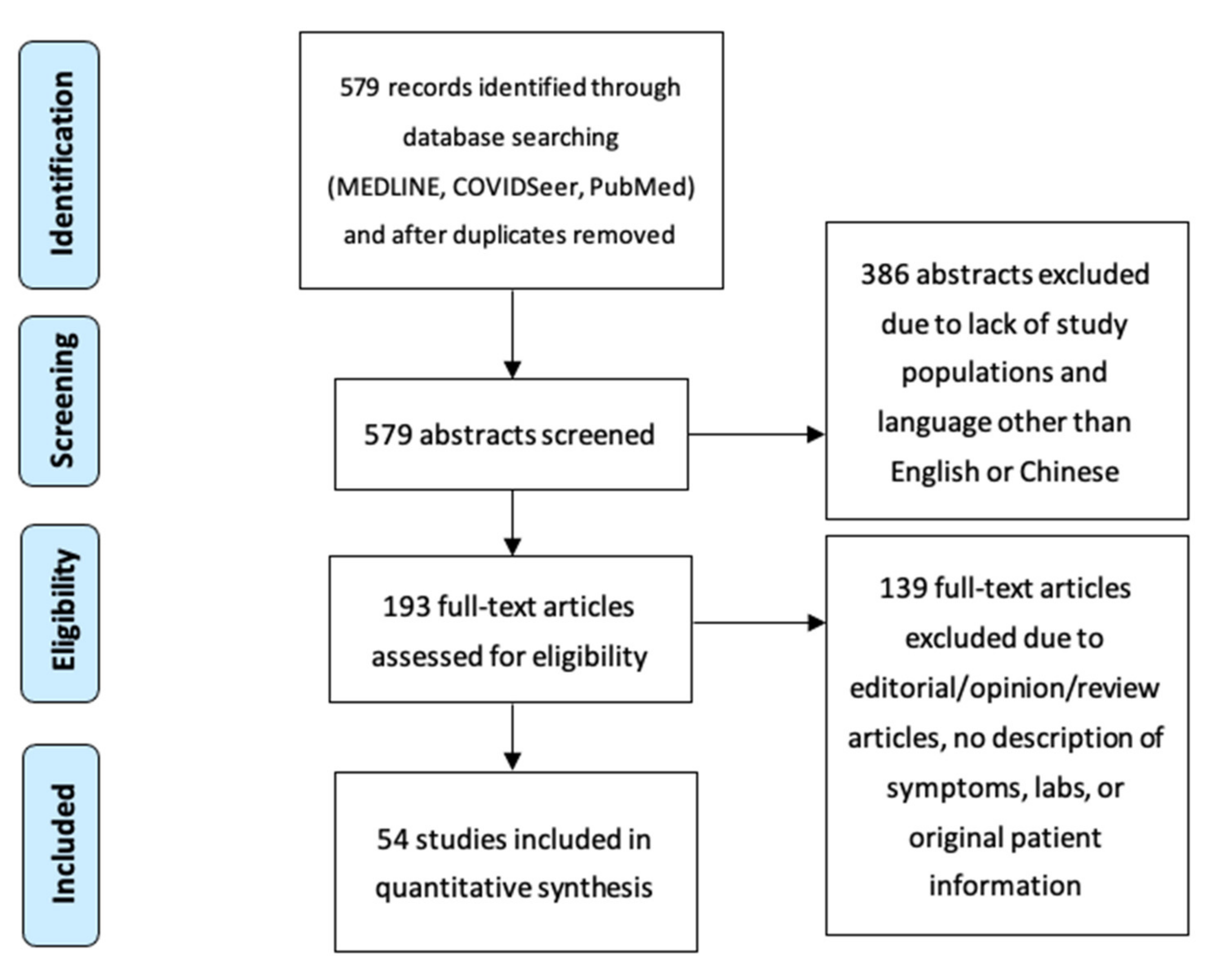
2. Materials and Methods
3. Results
3.1. All Cases
3.2. Kawasaki-like Multisystem Inflammatory (MIS-C) Cases
3.3. Children without MIS-C
3.4. Comparing Children with and without MIS-C
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dong, Y.; Mo, X.; Hu, Y.; Qi, X.; Jiang, F.; Jiang, Z.; Tong, S. Epidemiology of Covid-19 among Children in China. Pediatrics 2020, 145, e20200702. [Google Scholar] [CrossRef] [Green Version]
- WHO Coronavirus (Covid-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 14 May 2021).
- Science Brief: Transmission of Sars-Cov-2 in K-12 Schools. Available online: https://www.cdc.gov/coronavirus/2019-ncov/science/science-briefs/transmission_k_12_schools.html#ftn-4 (accessed on 14 May 2021).
- Provisional Covid-19 Deaths: Focus on Ages 0–18 Years. Available online: https://data.cdc.gov/NCHS/Provisional-COVID-19-Deaths-Focus-on-Ages-0-18-Yea/nr4s-juj3 (accessed on 12 May 2021).
- Alizargar, J. The Novel Coronavirus (Covid-19) and the Risk of Kawasaki Disease in Children. J. Formos. Med. Assoc. Taiwan Yi Zhi 2020, 119, 1713–1714. [Google Scholar] [CrossRef]
- Giray, T.; Biçer, S.; Küçük, Ö.; Çöl, D.; Yalvaç, Z.; Gürol, Y.; Yilmaz, G.; Saç, A.; Mogol, Y. Four Cases with Kawasaki Disease and Viral Infection: Aetiology or Association. Le Infezioni in Medicina 2016, 24, 340–344. [Google Scholar] [PubMed]
- Riphagen, S.; Gomez, X.; Gonzalez-Martinez, C.; Wilkinson, N.; Theocharis, P. Hyperinflammatory Shock in Children During Covid-19 Pandemic. Lancet 2020, 395, 1607–1608. [Google Scholar] [CrossRef]
- Verdoni, L.; Mazza, A.; Gervasoni, A.; Martelli, L.; Ruggeri, M.; Ciuffreda, M.; Bonanomi, E.; D’Antiga, L. An Outbreak of Severe Kawasaki-Like Disease at the Italian Epicentre of the Sars-Cov-2 Epidemic: An Observational Cohort Study. Lancet 2020, 395, 1771–1778. [Google Scholar] [CrossRef]
- Waltuch, T.; Gill, P.; Zinns, L.E.; Whitney, R.; Tokarski, J.; Tsung, J.W.; Sanders, J.E. Features of Covid-19 Post-Infectious Cytokine Release Syndrome in Children Presenting to the Emergency Department. Am. J. Emerg. Med. 2020, 38, 2246.e3–2246.e6. [Google Scholar] [CrossRef] [PubMed]
- Feldstein, L.R.; Rose, E.B.; Horwitz, S.M.; Collins, J.P.; Newhams, M.M.; Son, M.B.F.; Newburger, J.W.; Kleinman, L.C.; Heidemann, S.M.; Martin, A.A.; et al. Multisystem Inflammatory Syndrome in U.S. Children and Adolescents. N. Engl. J. Med. 2020, 383, 334–346. [Google Scholar] [CrossRef]
- Son, M.B.F.; Friedman, K. Covid-19: Multisystem Inflammatory Syndrome in Children (Mis-C) Clinical Features, Evaluation, and Diagnosis. UpToDate 2021. Available online: https://www.uptodate.com/contents/covid-19-multisystem-inflammatory-syndrome-in-children-mis-c-clinical-features-evaluation-and-diagnosis (accessed on 15 May 2021).
- Oh, S.J.; Shin, O.S. SARS-CoV-2 Nucleocapsid Protein Targets RIG-I-Like Receptor Pathways to Inhibit the Induction of Interferon Response. Cells. 2021, 10, 530. [Google Scholar] [CrossRef]
- Mawson, A.R.; Croft, A.M.; Gonzalez-Fernandez, F. Liver Damage and Exposure to Toxic Concentrations of Endogenous Retinoids in the Pathogenesis of COVID-19 Disease: Hypothesis. Viral Immunol. 2021. ahead of print. [Google Scholar] [CrossRef]
- Cao, X. COVID-19: Immunopathology and its implications for therapy. Nat. Rev. Immunol. 2020, 20, 269–270. [Google Scholar] [CrossRef] [Green Version]
- Tang, Y.; Liu, J.; Zhang, D.; Xu, Z.; Ji, J.; Wen, C. Cytokine storm in COVID-19: The current evidence and treatment strategies. Front. Immunol. 2020, 11, 1708. [Google Scholar] [CrossRef] [PubMed]
- Qin, C.; Zhou, L.; Hu, Z.; Zhang, S.; Yang, S.; Tao, Y.; Xie, C.; Ma, K.; Shang, K.; Wang, W.; et al. Dysregulation of immune response in patients with coronavirus 2019 (COVID-19) in Wuhan, China. Clin. Infect. Dis. 2020, 71, 762–768. [Google Scholar] [CrossRef] [PubMed]
- Zheng, M.; Gao, Y.; Wang, G.; Song, G.; Liu, S.; Sun, D.; Xu, Y.; Tian, Z. Functional exhaustion of antiviral lymphocytes in COVID-19 patients. Cell. Mol. Immunol. 2020, 17, 533–535. [Google Scholar] [CrossRef] [Green Version]
- Hertanto, D.M.; Sutanto, H.; Wiratama, B.S.; Wungu, C. Modulating the host immune response to fight against COVID-19: Where are we in 2021? Virulence 2021, 12, 1732–1736. [Google Scholar] [CrossRef]
- Guo, C.X.; He, L.; Yin, J.Y.; Meng, X.G.; Tan, W.; Yang, G.P.; Bo, T.; Liu, J.P.; Lin, X.J.; Chen, X. Epidemiological and clinical features of pediatric COVID-19. BMC Med. 2020, 18, 1–7. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The Prisma Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cui, Y.; Tian, M.; Huang, D.; Wang, X.; Huang, Y.; Fan, L.; Wang, L.; Chen, Y.; Liu, W.; Zhang, K.; et al. A 55-Day-Old Female Infant Infected with 2019 Novel Coronavirus Disease: Presenting with Pneumonia, Liver Injury, and Heart Damage. J. Infect. Dis 2020, 221, 1775–1781. [Google Scholar] [CrossRef]
- Li, Y.; Guo, F.; Cao, Y.; Li, L.; Guo, Y. Insight into Covid-2019 for Pediatricians. Pediatr. Pulmonol. 2020, 55, E1–E4. [Google Scholar] [CrossRef]
- Su, L.; Ma, X.; Yu, H.; Zhang, Z.; Bian, P.; Han, Y.; Sun, J.; Liu, Y.; Yang, C.; Geng, J.; et al. The Different Clinical Characteristics of Corona Virus Disease Cases between Children and Their Families in China—the Character of Children with Covid-19. Emerg. Microbes Infect. 2020, 9, 707–713. [Google Scholar] [CrossRef] [Green Version]
- Ji, L.N.; Chao, S.; Wang, Y.J.; Li, X.J.; Mu, X.D.; Lin, M.G.; Jiang, R.M. Clinical Features of Pediatric Patients with Covid-19: A Report of Two Family Cluster Cases. World J. Pediatr. 2020, 16, 267–270. [Google Scholar] [CrossRef] [Green Version]
- Sun, D.; Li, H.; Lu, X.-X.; Xiao, H.; Ren, J.; Zhang, F.-R.; Liu, Z.-S. Clinical Features of Severe Pediatric Patients with Coronavirus Disease 2019 in Wuhan: A Single Center’s Observational Study. World J. Pediatrics 2020, 16, 251–259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dugue, R.; Cay-Martínez, K.C.; Thakur, K.T.; Garcia, J.A.; Chauhan, L.V.; Williams, S.H.; Briese, T.; Jain, K.; Foca, M.; McBrian, D.K.; et al. Neurologic Manifestations in an Infant with Covid-19. Neurology 2020, 94, 1100–1102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, X.; Zhang, L.; Du, H.; Zhang, J.; Li, Y.Y.; Qu, J.; Zhang, W.; Wang, Y.; Bao, S.; Li, Y.; et al. Sars-Cov-2 Infection in Children. N. Engl. J. Med. 2020, 382, 1663–1665. [Google Scholar] [CrossRef] [Green Version]
- Cai, J.H.; Wang, X.S.; Ge, Y.L.; Xia, A.M.; Chang, H.L.; Tian, H.; Zhu, Y.X.; Wang, Q.R.; Zeng, J.S. First Case of 2019 Novel Coronavirus Infection in Children in Shanghai. Zhonghua Er Ke Za Zhi 2020, 58, E002. [Google Scholar] [CrossRef]
- Kam, K.Q.; Yung, C.F.; Cui, L.; Tzer Pin Lin, R.; Mak, T.M.; Maiwald, M.; Li, J.; Chong, C.Y.; Nadua, K.; Tan, N.W.H.; et al. A Well Infant with Coronavirus Disease 2019 with High Viral Load. Clin. Infect. Dis. 2020, 71, 847–849. [Google Scholar] [CrossRef]
- Chen, J.; Zhang, Z.Z.; Chen, Y.K.; Long, Q.X.; Tian, W.G.; Deng, H.J.; Hu, J.L.; Zhang, X.X.; Pu, L.; Xiang, J.L.; et al. The Clinical and Immunological Features of Pediatric Covid-19 Patients in China. Genes Dis. 2020, 7, 535–541. [Google Scholar] [CrossRef]
- Zhang, G.X.; Zhang, A.M.; Huang, L.; Cheng, L.Y.; Liu, Z.X.; Peng, X.L.; Wang, H.W. Twin Girls Infected with Sars-Cov-2. Zhongguo Dang Dai Er Ke Za Zhi 2020, 22, 221–225. [Google Scholar] [CrossRef]
- Zhang, Y.H.; Lin, D.J.; Xiao, M.F.; Wang, J.C.; Wei, Y.; Lei, Z.X.; Zeng, Z.Q.; Li, L.; Li, H.A.; Xiang, W. 2019-Novel Coronavirus Infection in a Three-Month-Old Baby. Zhonghua Er Ke Za Zhi 2020, 58, E006. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Ju, X.L.; Xie, F.; Lu, Y.; Li, F.Y.; Huang, H.H.; Fang, X.L.; Li, Y.J.; Wang, J.Y.; Yi, B.; et al. Clinical Analysis of 31 Cases of 2019 Novel Coronavirus Infection in Children from Six Provinces (Autonomous Region) of Northern China. Zhonghua Er Ke Za Zhi 2020, 58, 269–274. [Google Scholar] [CrossRef] [PubMed]
- Feng, K.; Yun, Y.X.; Wang, X.F.; Yang, G.D.; Zheng, Y.J.; Lin, C.M.; Wang, L.F. Analysis of Ct Features of 15 Children with 2019 Novel Coronavirus Infection. Zhonghua Er Ke Za Zhi 2020, 58, E007. [Google Scholar] [CrossRef]
- Chen, F.; Liu, Z.S.; Zhang, F.R.; Xiong, R.H.; Chen, Y.; Cheng, X.F.; Wang, W.Y.; Ren, J. First Case of Severe Childhood Novel Coronavirus Pneumonia in China. Zhonghua Er Ke Za Zhi 2020, 58, E005. [Google Scholar] [CrossRef]
- Jiehao, C.; Jin, X.; Daojiong, L.; Zhi, Y.; Lei, X.; Zhenghai, Q.; Yuehua, Z.; Hua, Z.; Ran, J.; Pengcheng, L.; et al. A Case Series of Children with 2019 Novel Coronavirus Infection: Clinical and Epidemiological Features. Clin. Infect. Dis. 2020, 71, 1547–1551. [Google Scholar] [CrossRef] [Green Version]
- Xing, Y.H.; Ni, W.; Wu, Q.; Li, W.J.; Li, G.J.; Wang, W.D.; Tong, J.N.; Song, X.F.; Wing-Kin Wong, G.; Xing, Q.S. Prolonged Viral Shedding in Feces of Pediatric Patients with Coronavirus Disease 2019. J. Microbiol. Immunol. Infect. 2020, 53, 473–480. [Google Scholar] [CrossRef]
- Wei, M.; Yuan, J.; Liu, Y.; Fu, T.; Yu, X.; Zhang, Z.J. Novel Coronavirus Infection in Hospitalized Infants under 1 Year of Age in China. JAMA 2020, 323, 1313–1314. [Google Scholar] [CrossRef]
- Mao, L.-j.; Xu, J.; Xu, Z.-h.; Xia, X.-p.; Li, B.; He, J.-g.; Zhao, P.; Pan, J.-w.; Zhang, D.; Su, Y.; et al. A Child with Household Transmitted Covid-19. BMC Infect. Dis. 2020, 20, 329. [Google Scholar] [CrossRef]
- See, K.C.; Liew, S.M.; Ng, D.C.E.; Chew, E.L.; Khoo, E.M.; Sam, C.H.; Sheena, D.; Zahilah Filzah, Z.; Chin, S.Y.; Lee, P.Y.; et al. Covid-19: Four Paediatric Cases in Malaysia. Int. J. Infect. Dis. IJID Off. Publ. Int. Soc. Infect. Dis. 2020, 94, 125–127. [Google Scholar] [CrossRef]
- Paret, M.; Lighter, J.; Pellett Madan, R.; Raabe, V.N.; Shust, G.F.; Ratner, A.J. Severe Acute Respiratory Syndrome Coronavirus 2 (Sars-Cov-2) Infection in Febrile Infants without Respiratory Distress. Clin. Infect. Dis 2020, 71, 2243–2245. [Google Scholar] [CrossRef] [PubMed]
- Qiu, H.; Wu, J.; Hong, L.; Luo, Y.; Song, Q.; Chen, D. Clinical and Epidemiological Features of 36 Children with Coronavirus Disease 2019 (Covid-19) in Zhejiang, China: An Observational Cohort Study. Lancet Infect. Dis. 2020, 20, 689–696. [Google Scholar] [CrossRef] [Green Version]
- Gefen, A.M.; Palumbo, N.; Nathan, S.K.; Singer, P.S.; Castellanos-Reyes, L.J.; Sethna, C.B. Pediatric Covid-19-Associated Rhabdomyolysis: A Case Report. Pediatr. Nephrol. 2020, 35, 1517–1520. [Google Scholar] [CrossRef] [PubMed]
- Giacomet, V.; Manfredini, V.A.; Meraviglia, G.; Peri, C.F.; Sala, A.; Longoni, E.; Gasperetti, A.; Stracuzzi, M.; Mannarino, S.; Zuccotti, G.V. Acute Inflammation and Elevated Cardiac Markers in a Two-Month-Old Infant with Severe Acute Respiratory Syndrome Coronavirus 2 Infection Presenting with Cardiac Symptoms. Pediatr. Infect. Dis. J. 2020, 39, e149–e151. [Google Scholar] [CrossRef] [PubMed]
- Musolino, A.M.; Supino, M.C.; Buonsenso, D.; Ferro, V.; Valentini, P.; Magistrelli, A.; Lombardi, M.H.; Romani, L.; D’Argenio, P.; Campana, A.; et al. Lung Ultrasound in Children with Covid-19: Preliminary Findings. Ultrasound Med. Biol. 2020, 46, 2094–2098. [Google Scholar] [CrossRef] [PubMed]
- Qiu, L.; Jiao, R.; Zhang, A.; Chen, X.; Ning, Q.; Fang, F.; Zeng, F.; Tian, N.; Zhang, Y.; Huang, Y.; et al. A Case of Critically Ill Infant of Coronavirus Disease 2019 with Persistent Reduction of T Lymphocytes. Pediatr. Infect. Dis. J. 2020, 39, e87–e90. [Google Scholar] [CrossRef] [PubMed]
- Denina, M.; Scolfaro, C.; Silvestro, E.; Pruccoli, G.; Mignone, F.; Zoppo, M.; Ramenghi, U.; Garazzino, S. Lung Ultrasound in Children with Covid-19. Pediatrics 2020, 146, e20201157. [Google Scholar] [CrossRef] [Green Version]
- Oualha, M.; Bendavid, M.; Berteloot, L.; Corsia, A.; Lesage, F.; Vedrenne, M.; Salvador, E.; Grimaud, M.; Chareyre, J.; de Marcellus, C.; et al. Severe and Fatal Forms of Covid-19 in Children. Arch. Pediatr. Organe Off. Soc. Fr. Pediatr. 2020, 27, 235–238. [Google Scholar] [CrossRef] [PubMed]
- Jiang, S.; Liu, P.; Xiong, G.; Yang, Z.; Wang, M.; Li, Y.; Yu, X.J. Coinfection of Sars-Cov-2 and Multiple Respiratory Pathogens in Children. Clin. Chem. Lab. Med. 2020, 58, 1160–1161. [Google Scholar] [CrossRef] [Green Version]
- Pınar Senkalfa, B.; Sismanlar Eyuboglu, T.; Aslan, A.T.; Ramaslı Gursoy, T.; Soysal, A.S.; Yapar, D.; İlhan, M.N. Effect of the Covid-19 Pandemic on Anxiety among Children with Cystic Fibrosis and Their Mothers. Pediatr. Pulmonol. 2020, 55, 2128–2134. [Google Scholar] [CrossRef]
- Bapst, T.; Romano, F.; Müller, M.; Rohr, M. Special Dermatological Presentation of Paediatric Multisystem Inflammatory Syndrome Related to Covid-19: Erythema Multiforme. BMJ Case Rep. 2020, 13, e236986. [Google Scholar] [CrossRef]
- Bai, K.; Liu, W.; Liu, C.; Fu, Y.; Hu, J.; Qin, Y.; Zhang, Q.; Chen, H.; Xu, F.; Li, C. Clinical Analysis of 25 Covid-19 Infections in Children. Pediatr. Infect. Dis. J. 2020, 39, e100–e103. [Google Scholar] [CrossRef]
- De Ioris, M.A.; Scarselli, A.; Ciofi Degli Atti, M.L.; Ravà, L.; Smarrazzo, A.; Concato, C.; Romani, L.; Scrocca, R.; Geremia, C.; Carletti, M.; et al. Dynamic Viral Severe Acute Respiratory Syndrome Coronavirus 2 Rna Shedding in Children: Preliminary Data and Clinical Consideration from a Italian Regional Center. J. Pediatr. Infect. Dis. Soc. 2020, 9, 366–369. [Google Scholar] [CrossRef]
- Haslak, F.; Yildiz, M.; Adrovic, A.; Sahin, S.; Koker, O.; Aliyeva, A.; Barut, K.; Kasapcopur, O. Management of Childhood-Onset Autoinflammatory Diseases During the Covid-19 Pandemic. Rheumatol. Int. 2020, 40, 1423–1431. [Google Scholar] [CrossRef]
- Ture, E.; Korkmaz, M.F.; Aksoy, F.D.; Ceylan Demirbas, B.; Menekse, B.; Ciftci, M.; Korkmaz, M. Point-of-Care Lung Ultrasound Findings in the Pediatric Emergency Clinic During the Covid-19 Pandemic. J. Clin. Ultrasound 2021, 49, 85–90. [Google Scholar] [CrossRef] [PubMed]
- Tran, T.A.; Cezar, R.; Frandon, J.; Kabani, S.; Corbeau, P. Ct Scan Does Not Make a Diagnosis of Covid-19: A Cautionary Case Report. Int. J. Infect. Dis. 2020, 100, 182–183. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Gu, J.; Chen, Q.; Deng, N.; Li, J.; Huang, L.; Zhou, X. Clinical and Epidemiological Characteristics of Pediatric Sars-Cov-2 Infections in China: A Multicenter Case Series. PLoS Med. 2020, 17, e1003130. [Google Scholar] [CrossRef] [PubMed]
- Korkmaz, M.F.; Ture, E.; Dorum, B.A.; Kilic, Z.B. The Epidemiological and Clinical Characteristics of 81 Children with Covid-19 in a Pandemic Hospital in Turkey: An Observational Cohort Study. J. Korean Med. Sci. 2020, 35, e236. [Google Scholar] [CrossRef]
- King, J.A.; Whitten, T.A.; Bakal, J.A.; McAlister, F.A. Symptoms Associated with a Positive Result for a Swab for Sars-Cov-2 Infection among Children in Alberta. CMAJ 2021, 193, E1–E9. [Google Scholar] [CrossRef]
- Garcia-Howard, M.; Herranz-Aguirre, M.; Moreno-Galarraga, L.; Urretavizcaya-Martinez, M.; Alegria-Echauri, J.; Gorria-Redondo, N.; Planas-Serra, L.; Schluter, A.; Gut, M.; Pujol, A.; et al. Case Report: Benign Infantile Seizures Temporally Associated with Covid-19. Front. Pediatr. 2020, 8, 507. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Lin, J.; Xu, H.; Liu, E.; Luo, Z.; Li, Q.; Xu, F.; He, L.; Zou, L.; Fu, Z.; et al. How Should Our Testing Behaviour Change with Time in Children in Current Covid-19 Pandemic? Eur. J. Clin. Investig. 2020, 50, e13351. [Google Scholar] [CrossRef]
- Dufort, E.M.; Koumans, E.H.; Chow, E.J.; Rosenthal, E.M.; Muse, A.; Rowlands, J.; Barranco, M.A.; Maxted, A.M.; Rosenberg, E.S.; Easton, D.; et al. Multisystem Inflammatory Syndrome in Children in New York State. N. Engl. J. Med. 2020, 383, 347–358. [Google Scholar] [CrossRef]
- Deza Leon, M.P.; Redzepi, A.; McGrath, E.; Abdel-Haq, N.; Shawaqfeh, A.; Sethuraman, U.; Tilford, B.; Chopra, T.; Arora, H.; Ang, J.; et al. Covid-19-Associated Pediatric Multisystem Inflammatory Syndrome. J. Pediatr. Infect. Dis. Soc. 2020, 9, 407–408. [Google Scholar] [CrossRef]
- Chiotos, K.; Bassiri, H.; Behrens, E.M.; Blatz, A.M.; Chang, J.; Diorio, C.; Fitzgerald, J.C.; Topjian, A.; John, A.R.O. Multisystem Inflammatory Syndrome in Children During the Coronavirus 2019 Pandemic: A Case Series. J. Pediatr. Infect. Dis. Soc. 2020, 9, 393–398. [Google Scholar] [CrossRef]
- Jones, V.G.; Mills, M.; Suarez, D.; Hogan, C.A.; Yeh, D.; Segal, J.B.; Nguyen, E.L.; Barsh, G.R.; Maskatia, S.; Mathew, R. Covid-19 and Kawasaki Disease: Novel Virus and Novel Case. Hosp. Pediatr. 2020, 10, 537–540. [Google Scholar] [CrossRef]
- Oberweis, M.L.; Codreanu, A.; Boehm, W.; Olivier, D.; Pierron, C.; Tsobo, C.; Kohnen, M.; Abdelrahman, T.T.; Nguyen, N.T.; Wagner, K.; et al. Pediatric Life-Threatening Coronavirus Disease 2019 with Myocarditis. Pediatr. Infect. Dis. J. 2020, 39, e147–e149. [Google Scholar] [CrossRef]
- Toubiana, J.; Levy, C.; Allali, S.; Jung, C.; Leruez-Ville, M.; Varon, E.; Bajolle, F.; Ouldali, N.; Chareyre, J.; Béchet, S.; et al. Association between Sars-Cov-2 Infection and Kawasaki-Like Multisystem Inflammatory Syndrome: A Retrospective Matched Case-Control Study, Paris, France, April to May 2020. Eurosurveillance 2020, 25, 2001813. [Google Scholar] [CrossRef]
- Garcia-Salido, A.; de Carlos Vicente, J.C.; Belda Hofheinz, S.; Balcells Ramirez, J.; Slocker Barrio, M.; Leoz Gordillo, I.; Hernandez Yuste, A.; Guitart Pardellans, C.; Cuervas-Mons Tejedor, M.; Huidobro Labarga, B.; et al. Severe Manifestations of Sars-Cov-2 in Children and Adolescents: From Covid-19 Pneumonia to Multisystem Inflammatory Syndrome: A Multicentre Study in Pediatric Intensive Care Units in Spain. Crit. Care 2020, 24, 666. [Google Scholar] [CrossRef] [PubMed]
- Lima-Setta, F.; Magalhaes-Barbosa, M.C.; Rodrigues-Santos, G.; Figueiredo, E.; Jacques, M.L.; Zeitel, R.S.; Sapolnik, R.; Borges, C.; Lanziotti, V.S.; Castro, R.E.V.; et al. Multisystem Inflammatory Syndrome in Children (Mis-C) During Sars-Cov-2 Pandemic in Brazil: A Multicenter, Prospective Cohort Study. J. Pediatr. 2021, 97, 354–361. [Google Scholar] [CrossRef] [PubMed]
- Vukomanovic, V.; Krasic, S.; Minic, P.; Petrovic, G.; Nesic, D.; Paripovic, A.; Vasiljevic, M.; Gobeljic, B. Kawasaki-Like Disease and Acute Myocarditis in the Sars-Cov-2 Pandemic—Reports of Three Adolescents. Bosn. J. Basic Med. Sci. 2021, 21, 252. [Google Scholar] [CrossRef] [PubMed]
- Navaeifar, M.R.; Shahbaznejad, L.; Sadeghi Lotfabadi, A.; Rezai, M.S. Covid-19-Associated Multisystem Inflammatory Syndrome Complicated with Giant Coronary Artery Aneurysm. Case Rep. Pediatr. 2021, 2021, 8836403. [Google Scholar] [CrossRef]
- Clemency, B.M.; Varughese, R.; Scheafer, D.K.; Ludwig, B.; Welch, J.V.; McCormack, R.F.; Ma, C.; Nan, N.; Giambra, T.; Raab, T. Symptom Criteria for Covid-19 Testing of Heath Care Workers. Acad. Emerg. Med. 2020, 27, 469–474. [Google Scholar] [CrossRef] [PubMed]
- Oozeer, N.B.; Forbes, K.; Clement, A.W.; Kubba, H. Management of Paediatric Olfactory Dysfunction: How We Do It. Clin. Otolaryngol. 2011, 36, 494–499. [Google Scholar] [CrossRef]
- LaRovere, K.L.; Riggs, B.J.; Poussaint, T.Y.; Young, C.C.; Newhams, M.M.; Maamari, M.; Walker, T.C.; Singh, A.R.; Dapul, H.; Hobbs, C.V.; et al. Neurologic Involvement in Children and Adolescents Hospitalized in the United States for Covid-19 or Multisystem Inflammatory Syndrome. JAMA Neurol. 2021, 78, 536. [Google Scholar] [CrossRef]
- Padda, I.; Khehra, N.; Jaferi, U.; Parmar, M.S. The Neurological Complexities and Prognosis of Covid-19. SN Compr. Clin. Med. 2020, 1–12. [Google Scholar] [CrossRef]
- Zhou, Z.; Zhang, M.; Wang, Y.; Zheng, F.; Huang, Y.; Huang, K.; Yu, Q.; Cai, C.; Chen, D.; Tian, Y.; et al. Clinical Characteristics of Older and Younger Patients Infected with Sars-Cov-2. Aging 2020, 12, 11296–11305. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Jiang, Y.; Wei, M.; Cheng, B.H.; Zhou, X.C.; Li, J.; Tian, J.H.; Dong, L.; Hu, R.H. Analysis of the Pregnancy Outcomes in Pregnant Women with Covid-19 in Hubei Province. Zhonghua Fu Chan Ke Za Zhi 2020, 55, 166–171. [Google Scholar] [CrossRef]
- Mao, L.; Jin, H.; Wang, M.; Hu, Y.; Chen, S.; He, Q.; Chang, J.; Hong, C.; Zhou, Y.; Wang, D.; et al. Neurologic Manifestations of Hospitalized Patients with Coronavirus Disease 2019 in Wuhan, China. JAMA Neurol. 2020, 77, 683–690. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rowley, A.H. Multisystem Inflammatory Syndrome in Children and Kawasaki Disease: Two Different Illnesses with Overlapping Clinical Features. J. Pediatr. 2020, 224, 129–132. [Google Scholar] [CrossRef]
- Soriano, J.B.; Anzueto, A.; Bosnic Anticevich, S.; Kaplan, A.; Miravitlles, M.; Usmani, O.; Papadopoulos, N.G.; Puggioni, F.; Canonica, G.W.; Roche, N. Face Masks, Respiratory Patients and Covid-19. Eur. Respir. J. 2020, 56. [Google Scholar] [CrossRef] [PubMed]
- Halbur, M.; Kodak, T.; McKee, M.; Carroll, R.; Preas, E.; Reidy, J.; Cordeiro, M.C. Tolerance of Face Coverings for Children with Autism Spectrum Disorder. J. Appl. Behav. Anal. 2021, 54, 600–617. [Google Scholar] [CrossRef] [PubMed]
- Davies, N.G.; Abbott, S.; Barnard, R.C.; Jarvis, C.I.; Kucharski, A.J.; Munday, J.D.; Pearson, C.A.B.; Russell, T.W.; Tully, D.C.; Washburne, A.D.; et al. Estimated Transmissibility and Impact of Sars-Cov-2 Lineage B.1.1.7 in England. Science 2021, 372, eabg3055. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Study | Publication Date | Study Location | Sample | Population |
|---|---|---|---|---|
| Dong et al. [1] | April 2020 | China | 728 | Inpatients with suspected and laboratory confirmed coronavirus disease 2019 (COVID-19) |
| Cui et al. [21] | March 2020 | China | 1 | Pediatric patients admitted to hospital with confirmed COVID-19 |
| Li et al. [22] | March 2020 | China | 2 | Pediatric patients admitted to hospital with confirmed COVID-19 |
| Su et al. [23] | February 2020 | China | 9 | Children admitted to infectious disease hospital for COVID-19 |
| Ji et al. [24] | March 2020 | China | 2 | Pediatric patients admitted to hospital with confirmed COVID-19 |
| Sun et al. [25] | September 2020 | China | 8 | Intensive care unit (ICU) patients with confirmed COVID-19 |
| Dugue et al. [26] | April 2020 | North America (United States) | 1 | A 6-week-old male infant with confirmed COVID-19, inpatient |
| Lu et al. [27] | March 2020 | China | 171 | Children with COVID-19 at Wuhan Children’s Hospital, inpatient |
| Cai et al. [28] | February 2020 | China | 10 | Inpatients with confirmed COVID-19 |
| Kam et al. [29] | February 2020 | Asia (Singapore) | 1 | Confirmed pediatric case, inpatient |
| Chen et al. [30] | April 2020 | China | 12 | Inpatients with laboratory confirmed COVID-19 |
| Zhang et al. [31] | March 2020 | China | 2 | Twin girls, inpatient |
| Zhang et al. [32] | March 2020 | China | 1 | 3-month-old girl, inpatient |
| Wang et al. [33] | April 2020 | China | 31 | 24 inpatient and 7 outpatient with confirmed COVID-19 |
| Feng et al. [34] | April 2020 | China | 15 | Pediatric patients admitted to hospital with confirmed COVID-19 |
| Chen et al. [35] | February 2020 | China | 1 | Pediatric patient admitted to hospital with confirmed COVID-19 |
| Jiehao et al. [36] | February 2020 | China | 1 | Pediatric patient admitted to hospital with confirmed COVID-19 |
| Xing et al. [37] | March 2020 | China | 3 | Pediatric patient admitted to hospital with confirmed COVID-19 |
| Wei et al. [38] | February 2020 | China | 9 | Pediatric patients admitted to hospital with confirmed COVID-19 |
| Riphagen et al. [7] | May 2020 | Europe (England) | 8 | 8 children with hyperinflammatory shock, inpatient |
| Mao et al. [39] | May 2020 | China | 1 | Pediatric patient admitted to hospital with confirmed COVID-19 |
| See et al. [40] | March 2020 | Asia (Malaysia) | 4 | Pediatric patients admitted to hospital with confirmed COVID-19 |
| Paret et al. [41] | July 2020 | North America (United States) | 2 | Pediatric patients admitted to hospital with confirmed COVID-19 |
| Qui et al. [42] | April 2020 | China | 1 | Hospitilalized infant with failure to thrive and confirmed COVID-19 |
| Gefen et al. [43] | May 2020 | North America (United States) | 1 | Child with history of autism and obstructive sleep apnea with labratory confirmed COVID-19, inpatient |
| Giacomet et al. [44] | April 2020 | Europe (Italy) | 1 | Infant admitted for severe laboratory confirmed COVID-19 |
| Musolino et al. [45] | April 2020 | Europe (Italy) | 10 | Pediatric patients admitted to hospital with confirmed COVID-19 |
| Qiu et al. [46] | March 2020 | China | 36 | Pediatric patients admitted to hospital with confirmed COVID-19 |
| Denina et al. [47] | June 2020 | Europe (Italy) | 8 | Pediatric patients admitted to hospital with confirmed COVID-19 |
| Oualha et al. [48] | June 2020 | Europe (France) | 27 | Patients admitted to pediatric ICU/high-dependency unit with severe COVID-19 |
| Jiang et al. [49] | April 2020 | China | 2 | Children with COVID-19 coinfected with human respiratory viruses and Mycoplasma pneumoniae |
| Pinar Senkalfa et al. [50] | June 2020 | Turkey | 45 | Patients with cystic fibrosis and COVID-19, inpatient |
| Bapst et al. [51] | June 2020 | Europe (Switzerland) | 1 | Previously healthy 13-year-old boy with fever of 7 days, inpatient |
| Bai et al. [52] | July 2020 | China | 25 | Pediatric patients admitted to hospital with confirmed COVID-19 |
| De Ioris et al. [53] | May 2020 | Europe (Italy) | 22 | Pediatric patients admitted to hospital with confirmed COVID-19 |
| Haslak et al. [54] | July 2020 | Turkey | 404 | Confirmed COVID-19 cases, patients with contact history, or symptoms suggestive of COVID-19 (all with autoinflammatory diseases). 24 inpatient and 380 outpatient |
| Türe et al. [55] | November 2020 | Turkey | 24 | Emergeny department admits with confirmed COVID-19 |
| Tran et al. [56] | September 2020 | Europe (France) | 1 | Pediatric patients admitted to hospital with confirmed COVID-19 |
| Zhang et al. [57] | June 2020 | China | 34 | Pediatric patients admitted to hospital with confirmed COVID-19 |
| Korkmaz et al. [58] | June 2020 | Turkey | 81 | 44 inpatient and 37 outpatient with confirmed COVID-19 |
| King et al. [59] | January 2021 | North America (Canada) | 1987 | 8 inpatient and 1979 outpatient with confirmed COVID-19 |
| Garcia-Howard et al. [60] | August 2020 | Europe (Spain) | 1 | Pediatric patient admitted to hospital with confirmed COVID-19 |
| Zhang et al. [61] | July 2020 | China | 534 | Outpatient with confirmed COVID-19 |
| Dufort et al. [62] | July 2020 | North America (United States) | 191 | Patients admitted to hospital with COVID-19 and suspected multisystem inflammatory syndrome (MIS-C) |
| Deza Leon et al. [63] | May 2020 | North America (United States) | 1 | Previously healthy child with sore throat, fever, reduced oral intake 6 days before admission |
| Chiotos et al. [64] | May 2020 | North America (United States) | 6 | Critically ill children with multisystem inflammatory syndrome, inpatient |
| Feldstein et al. [10] | July 2020 | North America (United States) | 186 | Patients with serious illness leading to hospitalization, an age of less than 21 years, fever that lasted for at least 24 h, laboratory evidence of inflammation, multisystem organ involvement, and evidence of COVID-19 |
| Jones et al. [65] | April 2020 | North America (United States) | 1 | Infant admitted due to severe presentation of COVID-19 |
| Oberweis et al. [66] | July 2020 | Europe (Luxembourg) | 1 | Hospital admission of a previously healthy child with 4-day fever, coughing, weight loss, fatigue |
| Toubiana et al. [67] | December 2020 | Europe (France) | 23 | Cases with fever admitted to hospital |
| García-Salido et al. [68] | November 2020 | Europe (Spain) | 74 | Intensive care unit patients with a diagnosis of COVID-19 and patients who met the case definition for MIS-C |
| Lima-Setta et al. [69] | November 2020 | South America (Brazil) | 56 | Patients admitted to the ICU with COVID-19 |
| Vukomanovic et al. [70] | October 2020 | Europe (Serbia) | 3 | Pediatric patients admitted to hospital with confirmed COVID-19 |
| Navaeifar et al. [71] | January 2021 | Asia (Iran) | 1 | Patients admitted to the ICU with COVID-19 |
| Yes | No | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| MIS-C | Typical | MIS-C | Typical | OR 95% CI | |||||||||
| General Characteristics | n | % | n | % | n | % | n | % | z | p | OR | Lower | Upper |
| Male | 324 | 14.2 | 1953 | 85.8 | 219 | 8.6 | 2315 | 91.4 | 6.06 | <0.001 | 1.75 | 1.46 | 2.1 |
| Fever | 530 | 21.7 | 1916 | 78.3 | 13 | 0.5 | 2352 | 99.5 | 13.86 | <0.001 | 50.05 | 28.77 | 87.05 |
| Sore throat | 17 | 1.1 | 1512 | 98.9 | 526 | 16.0 | 2756 | 84.0 | −11.4 | <0.001 | 0.06 | 0.04 | 0.1 |
| Rash | 104 | 93.7 | 7 | 6.3 | 439 | 9.3 | 4261 | 90.7 | 12.63 | <0.001 | 144.21 | 66.66 | 311.95 |
| Fatigue | 39 | 27.7 | 102 | 72.3 | 504 | 10.8 | 4166 | 89.2 | 5.93 | <0.001 | 3.16 | 2.16 | 4.62 |
| Myalgia/malaise | 53 | 36.8 | 91 | 63.2 | 490 | 10.5 | 4177 | 89.5 | 8.94 | <0.001 | 4.96 | 3.49 | 7.05 |
| Shortness of breath | 61 | 4.9 | 1193 | 95.1 | 482 | 13.6 | 3075 | 86.4 | −8 | <0.001 | 0.33 | 0.25 | 0.43 |
| Cough | 74 | 8.5 | 797 | 91.5 | 469 | 11.9 | 3471 | 88.1 | −2.86 | 0.004 | 0.69 | 0.53 | 0.89 |
| Nausea/vomiting | 311 | 71.0 | 127 | 29.0 | 232 | 5.3 | 4141 | 94.7 | 30.2 | <0.001 | 43.71 | 34.21 | 55.85 |
| Diarrhea | 289 | 69.5 | 127 | 30.5 | 254 | 5.8 | 4141 | 94.2 | 29.01 | <0.001 | 37.1 | 29.06 | 47.36 |
| ICU admission | 365 | 85.1 | 64 | 14.9 | 178 | 4.1 | 4204 | 95.9 | 31.5 | <0.001 | 134.7 | 99.28 | 182.74 |
| Septic shock | 116 | 89.2 | 14 | 10.8 | 427 | 9.1 | 4254 | 90.9 | 15.35 | <0.001 | 82.55 | 46.99 | 145 |
| Lymphocytopenia | 231 | 78.0 | 65 | 22.0 | 312 | 6.9 | 4203 | 93.1 | 25.42 | <0.001 | 47.87 | 35.53 | 64.51 |
| Abnormal CT-Chest | 97 | 28.6 | 242 | 71.4 | 446 | 10.0 | 4026 | 90.0 | 9.88 | <0.001 | 3.62 | 2.8 | 4.67 |
| Pneumonia | 1 | 0.1 | 1084 | 99.9 | 542 | 14.5 | 3184 | 85.5 | |||||
| Elevated liver function test | 1 | 3.2 | 30 | 96.8 | 542 | 11.3 | 4238 | 88.7 | |||||
| Neurological symptoms | |||||||||||||
| Headaches | 75 | 17.9 | 344 | 82.1 | 468 | 10.7 | 3924 | 89.3 | 4.42 | <0.001 | 1.83 | 1.4 | 2.39 |
| Syncope | 1 | 100.0 | 0 | 0.0 | 542 | 11.3 | 4268 | 88.7 | |||||
| Focal deficits | 0 | 0.0 | 9 | 100.0 | 543 | 11.3 | 4259 | 88.7 | |||||
| Dizziness | 0 | 0.0 | 5 | 100.0 | 543 | 11.3 | 4263 | 88.7 | |||||
| Anosmia/hypogeusia | 0 | 0.0 | 156 | 100.0 | 543 | 11.7 | 4112 | 88.3 | |||||
| Altered mental status | 7 | 77.8 | 2 | 22.2 | 536 | 11.2 | 4266 | 88.8 | |||||
| Seizures | 2 | 20.0 | 8 | 80.0 | 541 | 11.3 | 4260 | 88.8 | |||||
| Sleep disturbance | 1 | 33.3 | 2 | 66.7 | 542 | 11.3 | 4266 | 88.7 | |||||
| Stroke | 1 | 33.3 | 2 | 66.7 | 542 | 11.3 | 4266 | 88.7 | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kornitzer, J.; Johnson, J.; Yang, M.; Pecor, K.W.; Cohen, N.; Jiang, C.; Ming, X. A Systematic Review of Characteristics Associated with COVID-19 in Children with Typical Presentation and with Multisystem Inflammatory Syndrome. Int. J. Environ. Res. Public Health 2021, 18, 8269. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18168269
Kornitzer J, Johnson J, Yang M, Pecor KW, Cohen N, Jiang C, Ming X. A Systematic Review of Characteristics Associated with COVID-19 in Children with Typical Presentation and with Multisystem Inflammatory Syndrome. International Journal of Environmental Research and Public Health. 2021; 18(16):8269. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18168269
Chicago/Turabian StyleKornitzer, Jeffrey, Jacklyn Johnson, Max Yang, Keith W. Pecor, Nicholas Cohen, Carolyn Jiang, and Xue Ming. 2021. "A Systematic Review of Characteristics Associated with COVID-19 in Children with Typical Presentation and with Multisystem Inflammatory Syndrome" International Journal of Environmental Research and Public Health 18, no. 16: 8269. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18168269