
Exploring Intraindividual Profiles for Home Buildings Based on Architectural Compositional Elements and Psychological Health Factors: A Transdisciplinary Approach


Abstract
:1. Introduction
1.1. The Salutogenic or Psychosocially Supportive Design
1.2. Aims and Hypotheses
2. Materials and Methods
2.1. Participants
2.2. Measures
2.3. Procedure
2.4. Study Design and Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Health 2020 Priority Area Four: Creating Supportive Environments and Resilient Communities; WHO: Geneva, Switzerland, 2018. [Google Scholar]
- Moore, T.H.; Kesten, J.M.; López-López, J.A.; Ijaz, S.; McAleenan, A.; Richards, A.; Gray, S.; Savović, J.; Audrey, S. The effects of changes to the built environment on the mental health and well-being of adults: Systematic review. Health Place 2018, 53, 237–257. [Google Scholar] [CrossRef]
- Friesinger, J.G.; Topor, A.; Larsen, I.B. Studies regarding supported housing and the built environment for people with mental health problems: A mixed-methods literature review. Health Place 2019, 57, 44–53. [Google Scholar] [CrossRef] [PubMed]
- Doroud, N.; Fossey, E.; Fortune, T. Place for being, doing, becoming and belonging: A meta-synthesis exploring the role of place in mental health recovery. Health Place 2018, 52, 110–120. [Google Scholar] [CrossRef] [PubMed]
- Augustin, S.; Frankel, N.; Coleman, C. Place Advantage: Applied Psychology for Interior Architecture; John Wiley & Sons: Hoboken, NJ, USA, 2009. [Google Scholar]
- Kopec, D. Environmental Psychology for Design; Bloomsbury: New York, NY, USA, 2018. [Google Scholar]
- Battisto, D.; Wilhelm, J.J. Architecture and Health: Guiding Principles for Practice; Routledge: New York, NY, USA, 2019. [Google Scholar]
- Sarah, S. Design for health. In Design for Health; Tsekleves, E., Cooper, R., Eds.; Taylor & Francis: London, UK, 2017; pp. 90–295. [Google Scholar]
- Rice, L.; Drane, M. Indicators of healthy architecture-A systematic literature review. Urban Health 2020, 97, 899–911. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Mira, R.; Uzzell, D.L.; Real, J.E.; Romay, J. Housing, Space and Quality of Life; Ashgate: Farnham, UK, 2005. [Google Scholar]
- Altman, I.; Rogoff, B. World views in psychology: Trait, interactional, organismic and transactional perspectives. In Handbook of Environmental Psychology; Stokols, D., Altman, I., Eds.; Wiley: New York, NY, USA, 1987; pp. 1–40. [Google Scholar]
- Danilov, A.B. Salutogenic design: Hidden opportunities for health improvement and well-being of the population. Ind. Civ. Constr. 2019, 7, 10–17. [Google Scholar] [CrossRef]
- Dilani, A. The beneficial health outcomes of salutogenic design. In Design for Health; Tsekleves, E., Cooper, R., Eds.; Routledge: London, UK, 2017; pp. 72–91. [Google Scholar]
- Bringslimark, T.; Hartig, T.; Patil, G.G. The psychological benefits of indoor plants: A critical review of the experimental literature. J. Environ. Psychol. 2009, 29, 422–443. [Google Scholar] [CrossRef]
- Jackson, R.J.; Kochtitzky, C. Creating a healthy environment: The impact of the built environment on public health. In Urban Design and Human Flourishing: Creating Places that Enable People to Live Healthy and Fulfilling Lives; Townshend, T.G., Ed.; Routledge: New York, NY, USA, 2017; pp. 35–36. [Google Scholar]
- Lewin, K. Field theory and experiment in social psychology: Concepts and methods. Am. J. Sociol. 1939, 44, 868–896. [Google Scholar] [CrossRef]
- Aragonés, J.; Amérigo, M. Psicología Ambiental; Pirámide: Madrid, Spain, 2000. [Google Scholar]
- Gong, Y.; Palmer, S.; Gallacher, J.; Marsden, T.; Fone, D. A systematic review of the relationship between objective measurements of the urban environment and psychological distress. Environ. Int. 2016, 96, 48–57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Daykin, N.; Byrne, E.; Soteriou, T.; O′Connor, S. The impact of art, design and environment in mental healthcare: A systematic review of the literature. J. R. Soc. Promot. Health 2008, 128, 85–94. [Google Scholar] [CrossRef]
- Jovanović, N.; Campbell, J.; Priebe, S. How to design psychiatric facilities to foster positive social interaction-A systematic review. Eur. Psychiatry 2019, 60, 49–62. [Google Scholar] [CrossRef]
- McGrath, L.; Reavey, P. The Handbook of Mental Health and Space: Community and Clinical Applications; Routledge: London, UK, 2018. [Google Scholar]
- Oswald, F.; Wahl, H.W.; Naumann, D.; Mollenkopf, H.; Hieber, A. The role of the home environment in middle and late adulthood. In The Many Faces of Health, Competence and Well-Being in Old Age: Integrating Epidemiological, Psychological and Social Perspectives; Wahl, H.W., Brenner, H., Mollenkopf, H., Rothenbacher, D., Rott, C., Eds.; Springer: Dordrecht, The Netherlands, 2006; pp. 7–24. [Google Scholar]
- Antonovsky, A. Health, Stress and Coping; Jossey-Bass: San Francisco, CA, USA, 1979. [Google Scholar]
- Dilani, A. Psychosocially supportive design. In Design and Health IV: Future Trends in Healthcare Design; Dilani, A., Ed.; International Academy for Design and Health: Huddinge, Sweden, 2006; pp. 13–22. [Google Scholar]
- Herder, J.G. Myśli O Filozofii Dziejów; J. Gałecki: Warszawa, Poland, 1960. [Google Scholar]
- Wind, E.; Lloyd-Jones, H. The Eloquence of Symbols: Studies in Humanist Art; Clarendon Press: Oxford, UK, 1983. [Google Scholar]
- Norberg-Schulz, C. Existence, Space and Architecture; Praeger: Philadelphia, PA, USA, 1974. [Google Scholar]
- Norberg-Schulz, C. History of World Architecture: Baroque Architecture; Electa: Milan, Italy, 1979. [Google Scholar]
- Norberg-Schulz, C. Principles of Modern Architecture; Andreas Papadakis: London, UK, 2000. [Google Scholar]
- Lipps, T. Leitfaden Der Psychologie; W. Engelmann: Leipzig, Germany, 1906. [Google Scholar]
- Anwar, F.I.; Natheer, A.O.; Fayez, A. The effect of personality traits on architectural aesthetics’ evaluation: Familiar and non-familiar environments as evaluated by architectural and non-architectural students. Archit. Sci. Rev. 2002, 45, 197–210. [Google Scholar] [CrossRef]
- Ulrich, R. Theory of supportive design for healthcare facilities. J. Healthc. Des. 1997, 9, 3–7. [Google Scholar]
- Golembiewski, J.A. Salutogenic design: The neural basis for health promoting environments. World Health Des. Sci. Rev. 2012, 5, 62–68. [Google Scholar]
- Farrow, T.; Vanderkaay, S. Designed to Thrive: Creating Sautogenic Environments; Farrow: Toronto, ON, Canada, 2013. [Google Scholar]
- Bar, M.; Neta, M. Humans prefer curved visual objects. Psychol. Sci. 2006, 17, 645–648. [Google Scholar] [CrossRef] [PubMed]
- Silvia, P.J.; Barona, C.M. Do people prefer curved objects? Angularity, expertise, and aesthetic preference. Empir. Stud. Arts. 2009, 27, 25–42. [Google Scholar] [CrossRef]
- Hensen, J.L.M.; Lamberts, R. Building Performance Simulation for Design and Operation; Spon Press: New York, NY, USA, 2011. [Google Scholar]
- Calduch-Cervera, J. Temas De Composición Arquitectónica; Club Universitario: Alicante, Spain, 2012. [Google Scholar]
- Masiero, R. Estetica De La Arquitectura; Machado: Madrid, Spain, 2004. [Google Scholar]
- Abdelaal, M.S.; Soebarto, V. Biophilia and salutogenesis as restorative design. Archit. Sci. 2019, 62, 195–205. [Google Scholar] [CrossRef]
- Golembiewski, J.A. Start making sense: Applying a salutogenic model to architectural design for psychiatric care. Facilities 2010, 28, 100–117. [Google Scholar] [CrossRef]
- Ulrich, R. Essay: Evidence-based health-care architecture. Lancet Med. 2006, 368, S38–S39. [Google Scholar] [CrossRef]
- Wright, F.L. An Autobiography; Duell, Sloan & Pearce: New York, NY, USA, 1943. [Google Scholar]
- Van de Ven, C. El Espacio En Arquitectura; Cátedra: Madrid, Spain, 1981. [Google Scholar]
- Brooks, A.H. Wright Y La Destrucción De La Caja; Ediciones del Serbal: Barcelona, Spain, 1990. [Google Scholar]
- Gideon, S. Espacio, Tiempo Y Arquitectura; Dossat: Madrid, Spain, 1980. [Google Scholar]
- Gideon, S. Architecture You and Me. The Diary of a Development; Harvard University Press: Cambridge, MA, USA, 1958. [Google Scholar]
- Sanchez, M.E.; Sifuentes, M. Percepción Y Manipulación Del Espacio En Proyectos Arquitectónicos Dentro De Una Sociedad Compleja. In Proceedings of the 15th Iberoamerican Congress of Digital Graphics, SiGraDi, Santa Fe, Argentina, 16–18 November 2011; pp. 223–226. [Google Scholar]
- Zevi, B. Saber Ver La Arquitectura; Poseidón: Buenos Aires, Argentina, 1958. [Google Scholar]
- Kahn, L. Forma Y Diseño; Ediciones Nueva Visión: Buenos Aires, Argentina, 1961. [Google Scholar]
- Dilani, A. A new paradigm of design and health in hospital planning. World Hosp. Health Serv. 2006, 41, 17–21. [Google Scholar]
- Dietrich, K. A Design for Architectural Education; University of Regina: Regina, SK, Canada, 2008. [Google Scholar]
- Shemesh, A.; Talmon, R.; Karp, O.; Idan, A. Affective response to architecture-Investigating human reaction to spaces with different geometry. Archit. Sci. Rev. 2016, 60, 116–125. [Google Scholar] [CrossRef]
- Winkielman, P.; Schwarz, N.; Nowak, A. Affect and processing dynamics: Perceptual fluency enhances evaluations. Emot. Cogn. Brain Behav. 2002, 44, 111–136. [Google Scholar] [CrossRef]
- Leder, H.; Tinio, P.P.L.; Bar, M. Emotional valence modulates the preference for curved objects. Perception 2011, 40, 649–655. [Google Scholar] [CrossRef]
- Lengen, C. The effects of colours, shapes and boundaries of landscapes on perception, emotion and mentalising processes promoting health and well-being. Health Place 2015, 35, 166–177. [Google Scholar] [CrossRef]
- Wilson, A.; Chatterjee, A. The assessment of preference for balance: Introducing a new test. Empir. Stud. Arts 2005, 23, 165–180. [Google Scholar] [CrossRef] [Green Version]
- Pretty, J. How nature contributes to mental and physical health. Spiritual. Health Int. 2004, 5, 68–78. [Google Scholar] [CrossRef]
- Aznar, A. Las formas del color. Rev. Iberoam. Educ. 2010, 52, 1–9. [Google Scholar] [CrossRef]
- Mehta, R.; Zhu, R. Blue or red? Exploring the effect of color on cognitive task performances. Science 2009, 323, 1226–1229. [Google Scholar] [CrossRef] [Green Version]
- Manav, B. Color-emotion associations and color preferences: A case study for residences. Color Res. Appl. 2007, 32, 144–150. [Google Scholar] [CrossRef]
- Rahimi, N.N.; Dabagh, A. Estudio del efecto mental del color en la arquitectura interior de los espacios de hospital y su efecto sobre la tranquilidad del paciente. Rev. Cient. Amazon. 2018, 1, 5–20. [Google Scholar]
- Camgöz, N.; Yener, C.; Güvenç, D. Effects of hue, saturation, and brightness on preference. Color Res. Appl. 2002, 27, 199–207. [Google Scholar] [CrossRef]
- Costa, M.; Frumento, S.; Nese, M.; Predieri, I. Interior color and psychological functioning in a university residence hall. Front. Psychol. 2018, 9, 1580. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dael, N.; Perseguers, M.N.; Marchand, C.; Antonietti, J.P.; Mohr, C. Put on that colour, it fits your emotion: Colour appropriateness as a function of expressed emotion. Q. J. Exp. Psychol. 2016, 69, 1619–1630. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taylor, C.; Schloss, K.B.; Palmer, S.E.; Franklin, A. Color preferences in infants and adults are different. Psychon. Bull. Rev. 2013, 20, 916–922. [Google Scholar] [CrossRef] [Green Version]
- Browning, W.D.; Ryan, C.O.; Kallianpurkar, N.B. The Economics of Biophilia: Why Designing with Nature in Mind Makes Financial Sense; Terrapin Bright Green: New York, NY, USA, 2012. [Google Scholar]
- Beute, F.; de Kort, Y.A.W. Salutogenic effects of the environment: Review of health protective effects of nature and daylight. Appl. Psychol. Health Well-Being 2014, 6, 67–95. [Google Scholar] [CrossRef]
- Beute, F.; de Kort, Y.A.W. Let the sun shine! Measuring explicit and implicit preference for environments differing in naturalness, weather type and brightness. J. Environ. Psychol. 2013, 36, 162–178. [Google Scholar] [CrossRef]
- Boyce, P.; Hunter, C.; Howlett, O. The Benefits of Daylight through Windows; Rensselaer Polytechnic Institute: Troy, NY, USA, 2003. [Google Scholar]
- Beemer, C.J.; Stearns-Yoder, K.A.; Schuldt, S.J.; Kinney, K.A.; Lowry, C.A.; Postolache, T.T.; Brenner, L.A.; Hoisington, A.J. A brief review on the mental health for select elements of the built environment. Indoor Built Environ. 2021, 30, 152–165. [Google Scholar] [CrossRef]
- Sadar, J.S. Beyond blue: The non-visual effects of light and colour in architecture. Archit. Theory Rev. 2014, 19, 174–192. [Google Scholar] [CrossRef]
- Korpela, K.; de Bloom, J.; Sianoja, M.; Pasanen, T.; Kinnunen, U. Nature at home and at work: Naturally good? Links between window views, indoor plants, outdoor activities and employee well-being over one year. Landsc. Urban Plan. 2017, 160, 38–47. [Google Scholar] [CrossRef]
- Galasiu, A.D.; Reinhart, C.F. Current daylighting design practice: A survey. Build. Res. Inf. 2008, 36, 159–174. [Google Scholar] [CrossRef]
- Nutsford, D.; Pearson, A.L.; Kingham, S.; Reits, F. Residential exposure to visible blue space (but not green space) associated with lower psychological distress in a capital city. Health Place 2016, 39, 70–78. [Google Scholar] [CrossRef]
- Reinhart, C.; Fitz, A. Findings from a survey on the current use of daylight simulations in building design. Energy Build. 2006, 38, 824–835. [Google Scholar] [CrossRef] [Green Version]
- Osibona, O.; Solomon, B.D.; Fecht, D. Lighting in the home and health: A systematic review. Int. J. Environ. Res. Public Health 2021, 18, 609. [Google Scholar] [CrossRef]
- Broman, O. Aesthetic properties in knotty wood surfaces and their connection with people’s preferences. J. Wood Sci. 2001, 47, 192–198. [Google Scholar] [CrossRef]
- Karana, E.; Hekkert, P.; Kandachar, P. Material considerations in product design: A survey on crucial material aspects used by product designers. J. Mater. Des. 2008, 29, 1081–1089. [Google Scholar] [CrossRef] [Green Version]
- Karana, E.; Pedgley, O.; Rognoli, V. On materials experience. Des. Issues 2015, 31, 16–27. [Google Scholar] [CrossRef] [Green Version]
- Makin, A.D.J.; Pecchinenda, A.; Bertamini, M. Visual and emotional analysis of symmetry. J. Vis. 2013, 13, 812. [Google Scholar] [CrossRef]
- Makin, A.D.J.; Pecchinenda, A.; Bertamini, M. Implicit affective evaluation of visual symmetry. Emotion 2012, 12, 1021–1030. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arnheim, R. El Poder Del Centro; Alianza Forma: Madrid, Spain, 1984. [Google Scholar]
- Busseri, M.A.; Sadava, S.; Molnar, D.; DeCourville, N. A person-centered approach to subjective well-being. J. Happiness Stud. 2009, 10, 161–181. [Google Scholar] [CrossRef]
- Gerstorf, D.; Smith, J.; Baltes, P. A systemic-wholistic approach to differential aging: Longitudinal findings from the Berlin Aging Study. Psychol. Aging 2006, 21, 645–663. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klabbers, G.; Bosma, H.; Kempen, G.I.J.M.; Benzeval, M.; van den Akker, M.; van Eijk, J.T.M. Do psychosocial profiles predict self-rated health, morbidity and mortality in late middle-aged and older people? J. Behav. Med. 2014, 37, 357–368. [Google Scholar] [CrossRef]
- Lara, R.; Godoy-Izquierdo, D.; Vázquez, M.L.; Araque, F.; Godoy, J.F. Multidimensional psychosocial profiles in the elderly and happiness: A cluster-based identification. Aging Ment. Health 2014, 18, 489–503. [Google Scholar] [CrossRef]
- Hulley, S.B.; Cummings, S.R.; Browner, W.S.; Grady, D.; Newman, T.B. Designing Clinical Research: An Epidemiologic Approach, 4th ed.; Lippincott Williams Wilkins: Philadelphia, PA, USA, 2013. [Google Scholar]
- Hart, E.A.C.; Lakerveld, J.; McKee, M.; Oppert, J.M.; Rutter, H.; Charreire, H.; Mackenbach, J.D. Contextual correlates of happiness in European adults. PLoS ONE 2018, 13, e0190387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kwon, O.H.; Hong, I.; Yang, J.; Wohn, D.Y.; Jung, W.S.; Cha, M. Urban green space and happiness in developed countries. EPJ Data Sci. 2021, 10, 28. [Google Scholar] [CrossRef]
- Van Aart, C.J.; Michels, N.; Sioen, I.; De Decker, A.; Bijnens, E.M.; Janssen, B.G.; Nawrot, T.S. Residential landscape as a predictor of psychosocial stress in the life course from childhood to adolescence. Environ. Int. 2018, 120, 456–463. [Google Scholar] [CrossRef]
- Rammstedt, B.; John, O.P. Measuring personality in one minute or less: A 10-item short version of the Big Five Inventory in English and German. J. Res. Personal. 2007, 41, 203–212. [Google Scholar] [CrossRef]
- John, O.P.; Donahue, E.M.; Kentle, R.L. The Big Five Inventory-Versions 4a and 54; University of California, Institute of Personality and Social Research: Berkeley, CA, USA, 1991. [Google Scholar]
- Calderón, C.; Ferrando, P.J.; Lorenzo-Seva, U.; Carmona-Bayonas, A.; Jara, C.; Beato, C. Psychometric properties of Liverpool Stoicism Scale (LSS) in a cohort of patients with resected cancer in adjuvant treatment. An. Psicol. Ann. Psychol. 2017, 33, 621–629. [Google Scholar] [CrossRef] [Green Version]
- Soliño, M.; Alvarez-Farizo, B. Personal traits underlying environmental preferences: A discrete choice experiment. PLoS ONE 2014, 9, e89603. [Google Scholar] [CrossRef] [PubMed]
- Baessler, J.; Schwarcer, R. Evaluación de la autoeficacia: Adaptación española de la escala de Autoeficacia General. Ansiedad Y Estrés 1996, 2, 1–8. [Google Scholar] [CrossRef]
- Sanjuán, P.S.; Pérez-García, A.M.; Bermúdez, J. Escala de autoeficacia general: Datos psicométricos. Psicothema 2000, 12, 509–513. [Google Scholar]
- Bandura, A. Self-efficacy: Toward a unifying theory of behavioral change. Psychol. Rev. 1977, 84, 191–215. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, D.P. Manual of the General Health Questionnaire (GHQ-28); NFER-Nelson: Windsor, UK, 1981. [Google Scholar]
- Godoy-Izquierdo, D.; Godoy, J.F.; López-Torrecillas, F.; Sánchez-Barrera, M.B. Propiedades psicométricas de la versión española del “Cuestionario de Salud General de Goldberg-28”. Rev. Psicol. Salud/J. Health Psychol. 2002, 14, 49–71. [Google Scholar] [CrossRef]
- Lyubomirsky, S.; Lepper, H.S. A measure of subjective happiness: Preliminary reliability and construct validation. Soc. Indic. Res. 1999, 46, 137–155. [Google Scholar] [CrossRef]
- Extremera, N.; Fernández-Berrocal, P. The Subjective Happiness Scale: Translation and preliminary psychometric evaluation of a Spanish version. Soc. Indic. Res. 2014, 119, 473–481. [Google Scholar] [CrossRef]
- Steinley, D. K-means clustering: A half-century synthesis. Br. J. Math. Stat. Psychol. 2006, 59, 1–34. [Google Scholar] [CrossRef] [Green Version]
- Wu, J. Advances in K-Means Clustering; Springer: Berlin/Heidelberg, Germany, 2012. [Google Scholar]
- Mohamad, I.B.; Usman, D. Standardization and its effects on k-means clustering algorithm. Res. J. Appl. Sci. Eng. Technol. 2013, 6, 3299–3303. [Google Scholar] [CrossRef]
- Edwards, D.; Burnard, P.; Coyle, D.; Fothergill, A.; Hannigan, B. Stress and burnout in community mental health nursing: A review of the literature. J. Psychiatr. Ment. Health Nurs. 2000, 7, 7–14. [Google Scholar] [CrossRef]
- Smith, J.; Baltes, P.B. Profiles of psychological functioning in the old and oldest old. Psychol. Aging 1997, 12, 458–472. [Google Scholar] [CrossRef] [PubMed]
- Hitchcock, H.R.; Johnson, P. The International Style: Architecture Since 1922; W.W. Norton: New York, NY, USA, 1932. [Google Scholar]
- Canter, D.; Rees, K. A multivariate model of housing satisfaction. Appl. Psychol. 1982, 31, 185–207. [Google Scholar] [CrossRef]
- Cavanagh, B.; Haracz, K.; Lawry, M.; James, C. It’s like another world: The perceived beneficial effects of an artistically designed multisensory environment. Med. Humanit. 2019, 45, 52–59. [Google Scholar] [CrossRef]
- Cavanagh, B.; Haracz, K.; Lawry, M.; Wales, K.; James, C. Changes in emotions and perceived stress following time spent in an artistically designed multisensory environment. Med. Humanit. 2021, 011876. [Google Scholar] [CrossRef]
- Azzazy, S.; Ghaffarianhoseini, A.; GhaffarianHoseini, A.; Naismith, N.; Doborjeh, Z. A critical review on the impact of built environment on users’ measured brain activity. Archit. Sci. Rev. 2020, 1–17. [Google Scholar] [CrossRef]
- Eberhard, J.P. Brain Landscape. The Coexistence of Neuroscience and Architecture; Oxford University Press: New York, NY, USA, 2009. [Google Scholar]
- Dieleman, F.M.; Mulder, C.H. The geography of residential choice. In Residential Environments: Choice, Statisfaction, and Behavior; Aragonés, J.I., Francescato, G., Gärling, T., Eds.; Bergin & Garvey: London, UK, 2002; pp. 35–54. [Google Scholar]
- Edney, J.J. Place and space: The effects of experience with a physical locale. J. Exp. Soc. Psychol. 1972, 8, 124–135. [Google Scholar] [CrossRef]
- Gärling, T.; Friman, M. A psychological conceptualization of residential choice. In Residential Environments: Choice, Statisfaction, and Behavior; Aragonés, J.I., Francescato, G., Gärling, T., Eds.; Bergin & Garvey: London, UK, 2002; pp. 55–80. [Google Scholar]
- Nasar, J.L.; Valencia, H.; Omar, Z.A.; Chueh, S.; Hwang, J. Out of sight further from mind: Distance visibility and distance perception. Environ. Behav. 1985, 17, 627–639. [Google Scholar] [CrossRef]
- Abramsson, M.; Borgegård, L.E.; Fransson, U. Housing Careers, Some Empirical Evidence of a Complex Concept. In Proceedings of the ENHR Conference, Gävle, Sweden, 25–30 June 2000; pp. 26–30. [Google Scholar]
- Coren, S.; Porac, C.; Ward, L.M. Sensation and Perception; Academic Press: Orlando, FL, USA, 1984. [Google Scholar]
- Ærø, T. Residential choice from a lifestyle perspective. Hous. Theory Soc. 2006, 23, 109–130. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| N | % | ||
|---|---|---|---|
| Age | 18–29 yr. | 121 | 52.4 |
| 30–49 yr. | 73 | 31.6 | |
| >50 yr. | 37 | 16.0 | |
| Sex-gender | Female | 154 | 66.7 |
| Male | 77 | 33.3 | |
| Relationship status | Single | 82 | 35.5 |
| Non-stable relationship (<1 year) | 10 | 4.3 | |
| Stable relationship (≥1 year) | 134 | 58.0 | |
| Separated-divorced-widow | 5 | 2.2 | |
| Educational level | Primary | 4 | 1.7 |
| Secondary | 15 | 6.5 | |
| Professional training | 32 | 13.9 | |
| University | 180 | 77.9 | |
| Work status | Student | 98 | 42.4 |
| Employed | 110 | 47.6 | |
| Unemployed | 12 | 5.2 | |
| Homemaker | 6 | 2.6 | |
| Retired | 5 | 2.2 | |
| Family monthly income | <2000 € | 104 | 45.0 |
| >2000 € | 127 | 55.0 | |
| Nationality | Spanish | 215 | 93.1 |
| Non-Spanish residing in Spain > 1 yr. | 16 | 6.9 | |
| Location | East Andalucía | 151 | 65.4 |
| Other | 80 | 34.6 | |
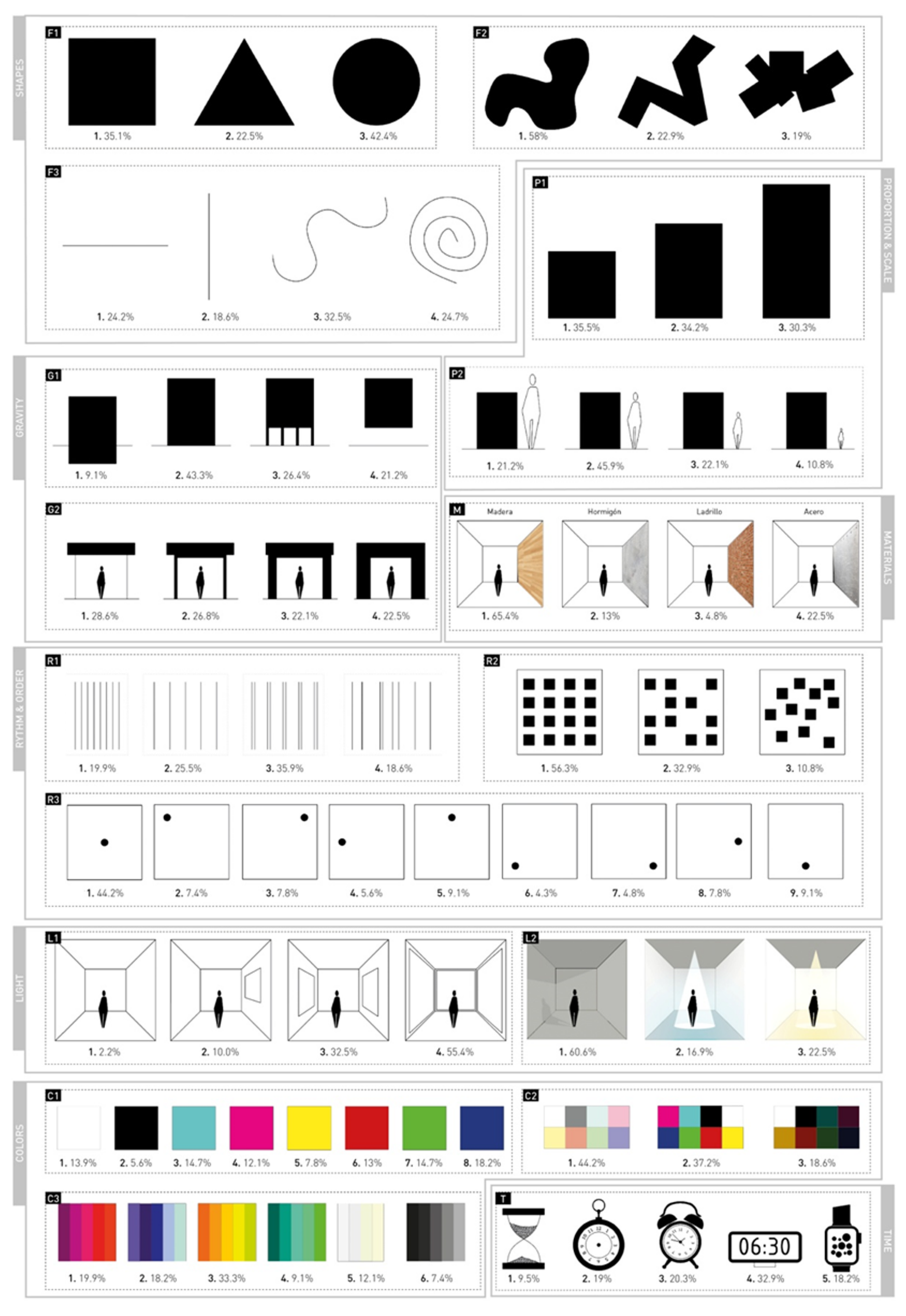
| Category | Subcategory | Figures and Assigned Values |
|---|---|---|
| Shapes (S) | S1. Simple geometry | Square (1) Triangle (2) Circle (3) |
| S2. Complex geometry | Organic shapes (1) Sharp organic shapes (2) Complex shapes by addition (3) | |
| S3. Linear geometry | Horizontal line (1) Vertical line (2) Curved line (3) Spiral line (4) | |
| Proportion and scale (P) | P1. Rectangular proportion | Square proportion (1) Golden proportion (2) Root proportion (3) |
| P2. Proportion relative to human scale | Small scale (1) Human scale (2) Domestic scale (3) Large scale (4) | |
| Gravity (G) | G1. Perception of gravity of the space with respect to the ground | Sunk in the ground (1) On the ground (2) On pilotis (3) Floating (4) |
| G2. Perception of the structure weight | Deconstructed structure (1) Lightweight structure (2) Rigid structure (3) Mass structure (4) | |
| Materials (M) | Wood (1) Concrete (2) Brick (3) Steel (4) | |
| Rhythm and order (R) | R1. Succession of equal elements | Very frequent rhythm (1) Spaced rhythm (2) Constant rhythm with duplicity (3) No order (4) |
| R2. Position of a set of elements in relation to each other | Ordered space (1) Slightly ordered space (2) Disordered space (3) | |
| R3 Global position of an object with respect to the whole space | Centered (1) Top left (2) Top right (3) Left centered (4) Top centered (5) Bottom left (6) Bottom right (7) Right centered (8) Down centered (9) | |
| Lighting (L) | L1. Natural daylight/openings | Closed space (1) Slightly open space (2) Moderately open space (3) Very open space (4) |
| L2. Artificial light/temperature of light | Daylight (1) Cold light (2) Warm light (3) | |
| Color (C) | C1. Individual color | White (1) Black (2) Cyan (3) Magenta (4) Yellow (5) Red (6) Green (7) Indigo (8) |
| C2. Color saturation/intensity | Bright color (1) Intense color (2) Unsaturated color (3) | |
| C3. Color range/temperature | Warm/red (1) Cold/blue (2) Warm/yellow (3) Cold/green (4) Neutral/white (5) Neutral/black (6) | |
| Time (T) | Archaic (1) Ancient (2) Recent past (3) Modern (4) Contemporary (5) |
| Variable (Possible Range of Scores) | M | SD | S1 | S2 | S3 | P1 | G1 | G2 | R1 | R2 | R3 | L1 | C2 | C3 | T |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Extraversion (2–10) | 6.48 | 1.97 | −0.17 | 0.14 | |||||||||||
| Neuroticism (2–10) | 5.97 | 2.07 | 0.15 | −0.13 | |||||||||||
| Openness (2–10) | 7.81 | 1.78 | 0.15 | 0.13 | |||||||||||
| Agreeableness (2–10) | 6.74 | 1.56 | 0.11 | −0.13 | −0.12 | ||||||||||
| Conscientiousness (2–10) | 7.48 | 1.74 | 0.14 | 0.17 | −0.12 | ||||||||||
| Self-efficacy (10–40) | 28.77 | 5.04 | 0.11 | ||||||||||||
| GHQ_Total score (0–84) | 62.07 | 11.49 | |||||||||||||
| Happiness (4–28) | 20.97 | 4.53 | 0.13 | −0.15 | 0.12 | −0.11 | 0.28 | −0.13 | −0.11 |
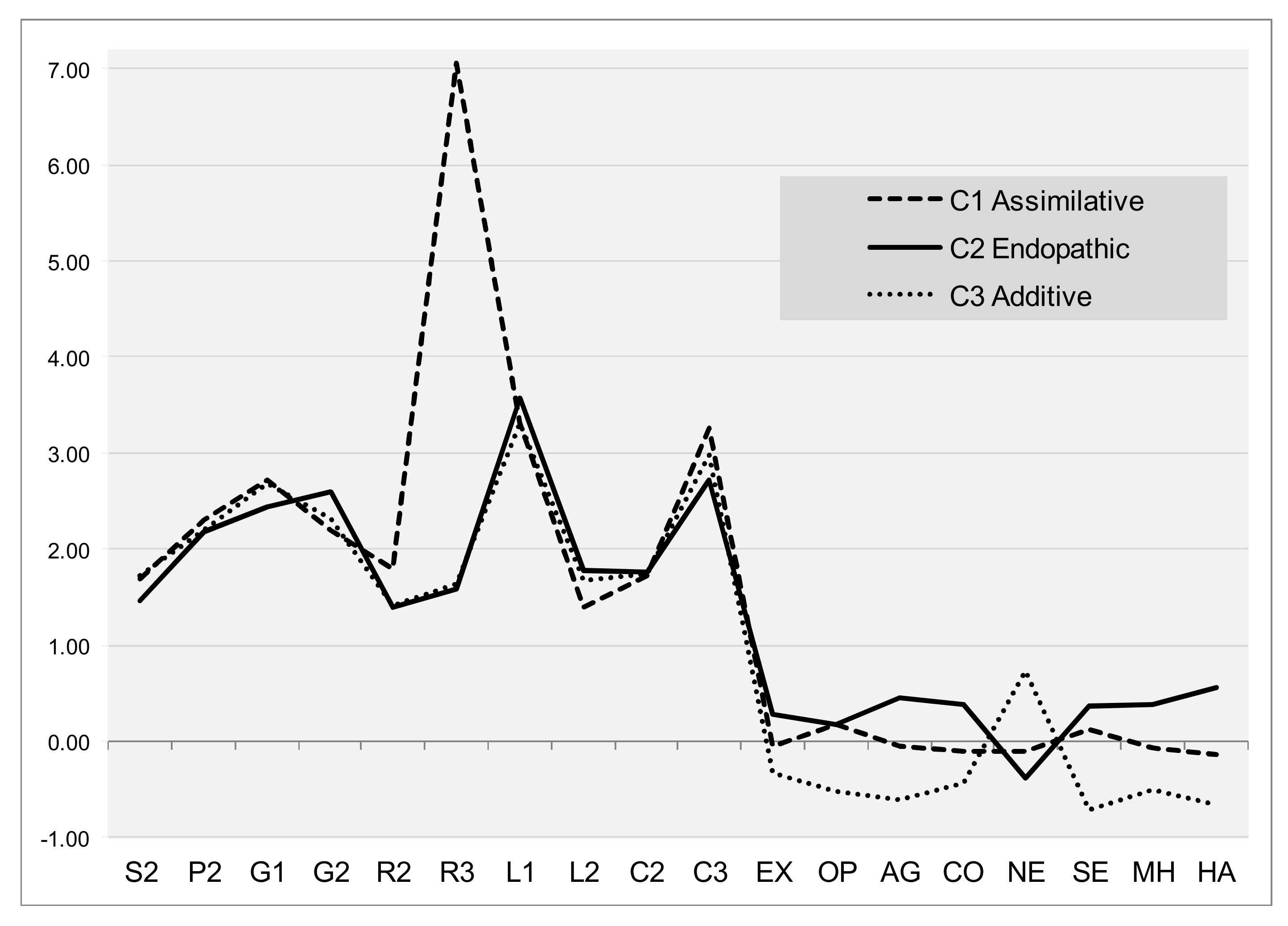
| Regulatory Parameters | Assimilative N = 82 | Endopathic N = 90 | Additive N = 59 | F | p | |||
|---|---|---|---|---|---|---|---|---|
| M | SD | M | SD | M | SD | |||
| Extraversion | −0.056 | 1.001 | 0.272 | 0.965 | −0.337 | 0.950 | 7.155 | 0.001 ** |
| Neuroticism | −0.105 | 1.023 | −0.385 | 0.846 | 0.733 | 0.784 | 28.437 | 0.000 ** |
| Agreeableness | −0.050 | 1.006 | 0.448 | 0.740 | −0.615 | 1.006 | 24.411 | 0.000 ** |
| Conscientiousness | −0.108 | 1.005 | 0.382 | 0.915 | −0.433 | 0.912 | 14.007 | 0.000 ** |
| Openness | 0.182 | 0.981 | 0.182 | 0.902 | −0.530 | 0.996 | 12.210 | 0.000 ** |
| General self-efficacy GHQ Total score Happiness | 0.121 −0.063 −0.133 | 0.866 1.016 0.994 | 0.363 0.383 0.558 | 0.898 0.711 0.687 | −0.722 −0.496 −0.667 | 0.962 1.124 0.949 | 26.836 15.822 36.459 | 0.000 ** 0.000 ** 0.000 ** |
| Architectural Variables | Assimilative N = 82 Value a | Endopathic N = 90 Value | Additive N = 59 Value | F | p |
|---|---|---|---|---|---|
| S2. Complex geometric shapes | 2 | 1 | 2 | 2.542 | 0.081 † |
| P2. Proportion relative to the human scale | 2 | 2 | 2 | 0.367 | 0.693 |
| G1. Gravity of the space with respect to the ground | 3 | 2 | 3 | 2.398 | 0.093 † |
| G2. Weight of the supporting structure | 2 | 3 | 2 | 2.957 | 0.054 † |
| R2. Position of a set of elements in relation to each other | 2 | 1 | 1 | 9.935 | 0.000 ** |
| R3. Position of an object with respect to the whole space | 7 | 2 | 2 | 497.568 | 0.000 ** |
| L1. Natural daylight/openings | 3 | 4 | 3 | 3.167 | 0.044 * |
| L2. Artificial light/temperature of light | 1 | 2 | 2 | 4.735 | 0.010 * |
| C2. Color saturation/intensity | 2 | 2 | 2 | 0.022 | 0.979 |
| C3. Color range/temperature | 3 | 3 | 3 | 2.912 | 0.056 † |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lara-Moreno, R.; Lara, E.; Godoy-Izquierdo, D. Exploring Intraindividual Profiles for Home Buildings Based on Architectural Compositional Elements and Psychological Health Factors: A Transdisciplinary Approach. Int. J. Environ. Res. Public Health 2021, 18, 8308. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18168308
Lara-Moreno R, Lara E, Godoy-Izquierdo D. Exploring Intraindividual Profiles for Home Buildings Based on Architectural Compositional Elements and Psychological Health Factors: A Transdisciplinary Approach. International Journal of Environmental Research and Public Health. 2021; 18(16):8308. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18168308
Chicago/Turabian StyleLara-Moreno, Raquel, Ester Lara, and Débora Godoy-Izquierdo. 2021. "Exploring Intraindividual Profiles for Home Buildings Based on Architectural Compositional Elements and Psychological Health Factors: A Transdisciplinary Approach" International Journal of Environmental Research and Public Health 18, no. 16: 8308. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18168308