
Identification of Network Promoters in a Regional and Intersectoral Health Promotion Network: A Qualitative Social Network Analysis in Southern Germany


Abstract
:1. Introduction
Theoretical Background
2. Materials and Methods
2.1. Study Setting
2.2. Data Collection and Analysis
3. Results
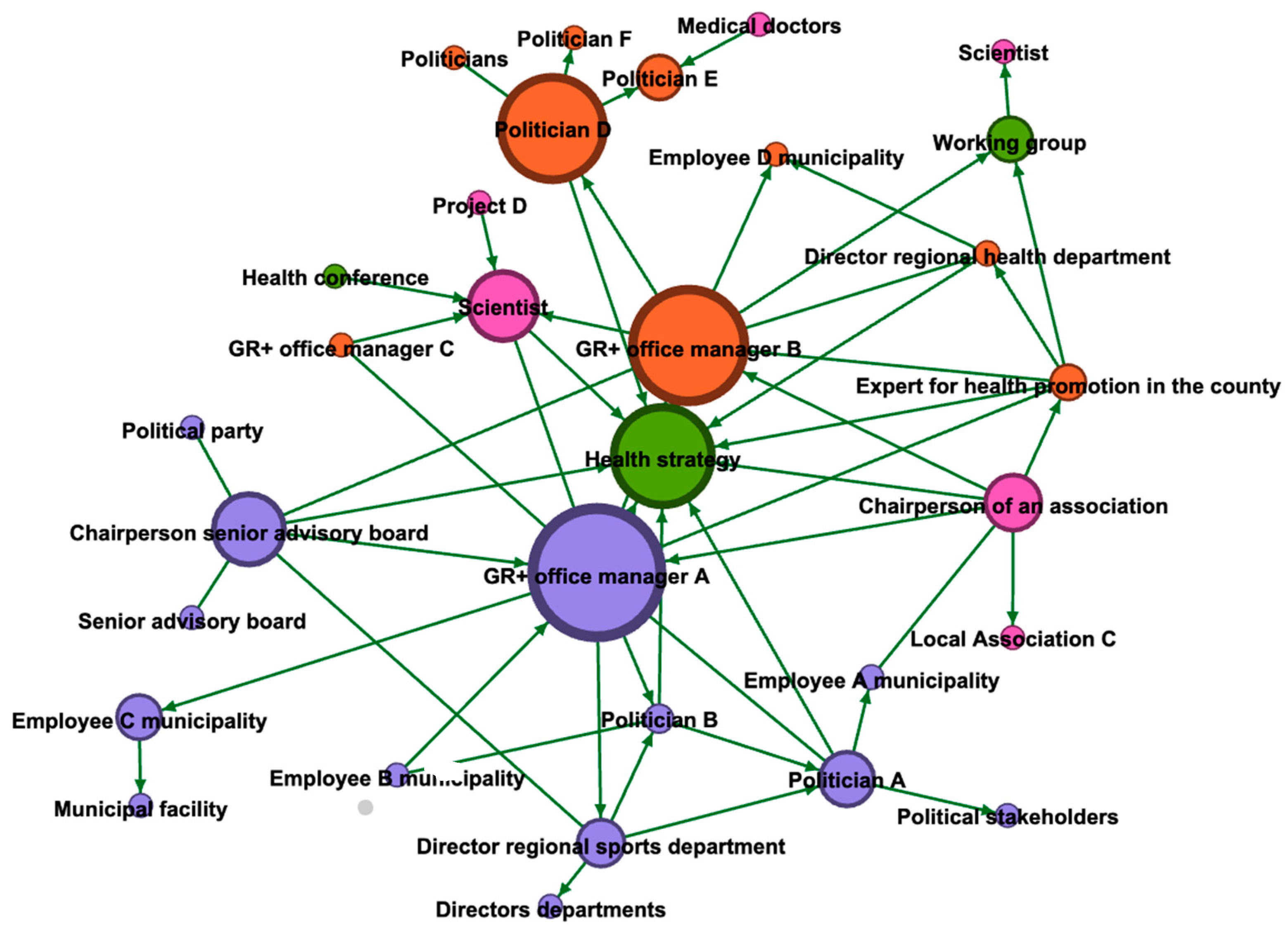
3.1. Network Structures from the Perspective of the Project Office Managers
3.2. Network Structures, as Perceived from the Perspective of the Steering Committee Members
3.3. Promoter Roles within the Steering Committee
4. Discussion
Study Limitations/Strengths and Weaknesses
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dahlgren, G.; Whitehead, M. Levelling Up (Part 2): A Discussion Paper on European Strategies for Tackling Social Inequities in Health; WHO Regional Office for Europe: Copenhagen, Denmark, 2006. [Google Scholar]
- Quilling, E.; Kruse, S.; Kuchler, M.; Leimann, J.; Walter, U. Models of Intersectoral Cooperation in Municipal Health Promotion and Prevention: Findings from a Scoping Review. Sustainability 2020, 12, 6544. [Google Scholar] [CrossRef]
- Rantala, R.; Bortz, M.; Armada, F. Intersectoral Action: Local Governments Promoting Health. Health Promot. Int. 2014, 29, i92–i102. [Google Scholar] [CrossRef] [Green Version]
- Danaher, A. Reducing Health Inequities: Enablers and Barriers to Inter-Sectoral Collaboration; Wellesley Institute: Toronto, ON, Canada, 2011. [Google Scholar]
- World Health Organization. The Ottawa Charter for Health Promotion; WHO Regional Office for Europe: Ottawa, ON, Canada, 1986. [Google Scholar]
- De Leeuw, E. Engagement of Sectors Other than Health in Integrated Health Governance, Policy, and Action. Annu. Rev. Public Health 2017, 38, 329–349. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Multisectoral and Intersectoral Action for Improved Health and Well-Being for All: Mapping of the WHO European Region. Governance for a Sustainable Future: Improving Health and Well-Being for All; WHO Regional Office for Europe: Copenhagen, Denmark, 2018. [Google Scholar]
- Storm, I.; den Hertog, F.; van Oers, H.; Schuit, A.J. How to Improve Collaboration between the Public Health Sector and Other Policy Sectors to Reduce Health Inequalities?—A Study in Sixteen Municipalities in the Netherlands. Int. J. Equity Health 2016, 15, 97. [Google Scholar] [CrossRef] [Green Version]
- Stefani, S.; Torriero, A. Formal and informal networks in organizations. In Advanced Dynamic Modeling of Economic and Social Systems; Proto, A.N., Squillante, M., Kacprzyk, J., Eds.; Springer: Berlin/Heidelberg, Germany, 2013; pp. 61–77. ISBN 9783642329029. [Google Scholar]
- Borgatti, S.P.; Mehra, A.; Brass, D.J.; Labianca, G. Network Analysis in the Social Sciences. Science 2009, 323, 892–895. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hawe, P.; Webster, C.; Shiell, A. A Glossary of Terms for Navigating the Field of Social Network Analysis. J. Epidemiol. Community Health 2004, 58, 971–975. [Google Scholar] [CrossRef]
- Luke, D.A.; Harris, J.K. Network Analysis in Public Health: History, Methods, and Applications. Annu. Rev. Public Health 2007, 28, 69–93. [Google Scholar] [CrossRef] [Green Version]
- McGetrick, J.A.; Raine, K.D.; Wild, T.C.; Nykiforuk, C.I.J. Advancing Strategies for Agenda Setting by Health Policy Coalitions: A Network Analysis of the Canadian Chronic Disease Prevention Survey. Health Commun. 2019, 34, 1303–1312. [Google Scholar] [CrossRef] [PubMed]
- Ward, V.; Smith, S.; Keen, J.; West, R.; House, A. Creating and Implementing Local Health and Wellbeing Policy: Networks, Interactions and Collective Knowledge Creation amongst Public Sector Managers. Evid. Policy 2018, 14, 477–498. [Google Scholar] [CrossRef]
- Provan, K.G.; Veazie, M.A.; Staten, L.K.; Teufel-Shone, N.I. The Use of Network Analysis to Strengthen Community Partnerships. Public Adm. Rev. 2005, 65, 603–613. [Google Scholar] [CrossRef]
- West, R.M.; House, A.O.; Keen, J.; Ward, V.L. Using the Structure of Social Networks to Map Inter-Agency Relationships in Public Health Services. Soc. Sci. Med. 2015, 145, 107–114. [Google Scholar] [CrossRef] [Green Version]
- Crossley, N. The Social World of the Network. Combining Qualitative and Quantitative Elements in Social Network Analysis. Sociologica 2010. [Google Scholar] [CrossRef]
- Ahrens, P. Qualitative Network Analysis: A Useful Tool for Investigating Policy Networks in Transnational Settings? Methodol. Innov. 2018, 11. [Google Scholar] [CrossRef]
- Witte, E. Organisation Für Innovationsentscheidungen—Das Promotoren-Modell; Schwartz: Göttingen, Germany, 1973; ISBN 3-509-00616-X. [Google Scholar]
- Hauschildt, J.; Kirchmann, E. Teamwork for Innovation—The “troika” of Promotors. R D Manag. 2001, 31, 41–49. [Google Scholar] [CrossRef]
- Gemünden, H.G.; Salomo, S.; Hölzle, K. Role Models for Radical Innovations in Times of Open Innovation. Creat. Innov. Manag. 2007, 16, 408–421. [Google Scholar] [CrossRef]
- Hölzle, K.; Gemünden, H.G. Schlüsselpersonen der Innovation. In Handbuch Technologie—und Innovationsmanagement: Strategie-Umsetzung-Controlling; Albers, S., Gassmann, O., Eds.; Gabler Verlag: Wiesbaden, Germany, 2011; pp. 495–512. [Google Scholar]
- Hollederer, A.; Eicher, A.; Pfister, F.; Stühler, K.; Wildner, M. Vernetzung, Koordination Und Verantwortung Durch Gesundheitsregionen plus: Neue Gesundheitspolitische Ansätze Und Entwicklungen in Bayern. Gesundheitswesen 2017, 79, 613–616. [Google Scholar] [CrossRef] [PubMed]
- Bödeker, M.; Deiters, T.; Eicher, A.; Hollederer, A.; Pfister, F.; Wildner, M. Wie Können Die Gesundheitsversorgung, -Förderung Und Prävention Regional Optimiert Werden? Die Entwicklung Der Gesundheitsregionenplus in Bayern. Public Health Forum 2016, 24, 290–293. [Google Scholar] [CrossRef]
- Hollederer, A. Regionale Gesundheitskonferenzen Und Gesundheitsregionenplus in Deutschland: Struktur-, Prozess- Und Ergebnisqualitäten. Public Health Forum 2016, 24, 22–25. [Google Scholar] [CrossRef]
- Bödeker, M.; Deiters, T.; Eicher, A.; Hollederer, A.; Pfister, F.; Wildner, M. Gesundheitsregionenplus in Bayern: Synergien im regionalen Gesundheitsmanagement. In Gesundheitswirtschaft als Motor der Regionalentwicklung; Dahlbeck, E.H.J., Ed.; Springer: Wiesbaden, Germany, 2017. [Google Scholar]
- Hollederer, A.; Eicher, A.; Pfister, F.; Stühler, K.; Wildner, M. Gesundheitsregionenplus in Bayern. In Management von Gesundheitsregionen, I.; Pfannstiel, M.A., Focke, A., Mehlich, H., Eds.; Springer: Wiesbaden, Germany, 2016; pp. 1–9. [Google Scholar]
- Hollederer, A. Struktur- Und Prozessqualität Am Beispiel Der Neuen Gesundheitsregionenplus in Bayern. Das Gesundh. 2017, 79, 299–374. [Google Scholar] [CrossRef]
- Bödeker, M.; Deiters, T.; Eicher, A.; Hollederer, A.; Pfister, F.; Wildner, M. Aufbau von Netzwerkstrukturen Für Das Regionale Gesundheitsmanagement. Ein Fortschrittbericht Aus Den Gesundheitsregionenplus in Bayern. Das Gesundh. 2017, 79, 299–374. [Google Scholar] [CrossRef]
- Majzik, Z.; Gmehling, S.; Kern, L.; Lender-Cassens, S.; Klaußner, G.; Hahn, U.; Neumann, F.; Wolff, A.; Christian, A.; Kühlein, T.; et al. Gemeinsame Gesundheitsstrategie Der Gesundheitsregionplus Erlangen-Höchstadt & Erlangen-Grundlagen, Ziele, Umsetzung: Strategiepapier; Gesundheitsregionplus Erlangen-Höchstadt & Erlangen; Erlangen, Germany, 2017; Available online: https://www.fueralleinstadtundland.de/wp-content/uploads/2017/10/2017-261-GRP-Strategiepapier-Doppelseiten.pdf (accessed on 1 August 2021).
- Schiffer, E.; Hauck, J. Net-Map: Collecting Social Network Data and Facilitating Network Learning through Participatory Influence Network Mapping. Field Methods 2010, 22, 231–249. [Google Scholar] [CrossRef]
- Hollstein, B. Qualitative Approaches. In The SAGE Handbook of Social Network Analysis; Scott, J., Carrington, P.J., Eds.; SAGE Publications Ltd.: London, UK, 2011; pp. 404–416. [Google Scholar]
- Merluzzi, J.; Burt, R.S. How Many Names Are Enough? Identifying Network Effects with the Least Set of Listed Contacts. Soc. Netw. 2013, 35, 331–337. [Google Scholar] [CrossRef]
- Gamper, M.; Schönhuth, M.; Kronenwett, M. Bringing qualitative and quantitative data together: Collecting network data with the help of the software tool vennmaker. In Social Networking and Community Behavior Modeling: Qualitative and Quantitative Measures; Safar, M., Mahdi, K., Eds.; IGI Global: Hershey, PA, USA, 2012; pp. 193–213. ISBN 9781613504444. [Google Scholar]
- Schmidt, L.; Neuburger, M. Trapped between Privileges and Precariousness: Tracing Transdisciplinary Research in a Postcolonial Setting. Futures 2017, 93, 54–67. [Google Scholar] [CrossRef]
- Ensor, J.E.; Park, S.E.; Attwood, S.J.; Kaminski, A.M.; Johnson, J.E. Can Community-Based Adaptation Increase Resilience? Clim. Dev. 2016, 10, 134–151. [Google Scholar] [CrossRef] [Green Version]
- Schröter, B.; Hauck, J.; Hackenberg, I.; Matzdorf, B. Bringing Transparency into the Process: Social Network Analysis as a Tool to Support the Participatory Design and Implementation Process of Payments for Ecosystem Services. Ecosyst. Serv. 2018, 34, 206–217. [Google Scholar] [CrossRef]
- Campbell, N.; Schiffer, E.; Buxbaum, A.; McLean, E.; Perry, C.; Sullivan, T.M. Taking Knowledge for Health the Extra Mile: Participatory Evaluation of a Mobile Phone Intervention for Community Health Workers in Malawi. Glob. Health Sci. Pract. 2014, 2, 23–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harris, J.; Drimie, S.; Roopnaraine, T.; Covic, N. From Coherence towards Commitment: Changes and Challenges in Zambia’s Nutrition Policy Environment. Glob. Food Secur. 2017, 13, 49–56. [Google Scholar] [CrossRef]
- Ward, V.; West, R.; Smith, S.; McDermott, S.; Keen, J.; Pawson, R.; House, A. The Role of Informal Networks in Creating Knowledge among Health-Care Managers: A Prospective Case Study; NIHR Journals Library: Southampton, UK, 2014. [Google Scholar]
- Bastian, M.; Heymann, S.; Jacomy, M. Gephi: An Open Source Software for Exploring and Manipulating Networks. In Proceedings of the Third International AAAI Conference on Weblogs and Social Media, San Jose, CA, USA, 17–20 May 2009. [Google Scholar]
- Wäsche, H.; Dickson, G.; Woll, A.; Brandes, U. Social Network Analysis in Sport Research: An Emerging Paradigm. Eur. J. Sport Soc. 2017, 14, 138–165. [Google Scholar] [CrossRef]
- Zhang, J.; Luo, Y. Degree Centrality, Betweenness Centrality, and Closeness Centrality in Social Network. In Proceedings of the 2017 2nd International Conference on Modelling, Simulation and Applied Mathematics (MSAM2017), Bangkok, Thailand, 26–27 March 2017. [Google Scholar]
- Axelsson, R.; Axelsson, S.B. Integration and Collaboration in Public Health—A Conceptual Framework. Int. J. Health Plan. Manag. 2006, 21, 75–88. [Google Scholar] [CrossRef]
- Hope Corbin, J.; Jones, J.; Barry, M.M. What Makes Intersectoral Partnerships for Health Promotion Work? A Review of the International Literature. Health Promot. Int. 2018, 33, 4–26. [Google Scholar] [CrossRef] [Green Version]
- Alderwick, H.; Hutchings, A.; Briggs, A.; Mays, N. The Impacts of Collaboration between Local Health Care and Non-Health Care Organizations and Factors Shaping How They Work: A Systematic Review of Reviews. BMC Public Health 2021, 21, 753. [Google Scholar] [CrossRef]
- Leppin, A.L.; Okamoto, J.M.; Organick, P.W.; Thota, A.D.; Barrera-Flores, F.J.; Wieland, M.L.; McCoy, R.G.; Bonacci, R.P.; Montori, V.M. Applying Social Network Analysis to Evaluate Implementation of a Multisector Population Health Collaborative That Uses a Bridging Hub Organization. Front. Public Health 2018, 6, 315. [Google Scholar] [CrossRef] [PubMed]
- Roussos, S.T.; Fawcett, S.B. A Review of Collaborative Partnerships as a Strategy for Improving Community Health. Annu. Rev. Public Health 2000, 21, 369–402. [Google Scholar] [CrossRef] [Green Version]
- DeHoog, R.H. Collaborations and Partnerships across Sectors: Preparing the Next Generation for Governance. J. Public Aff. Educ. 2015, 21, 401–416. [Google Scholar] [CrossRef]
- Seaton, C.L.; Holm, N.; Bottorff, J.L.; Jones-Bricker, M.; Errey, S.; Caperchione, C.M.; Lamont, S.; Johnson, S.T.; Healy, T. Factors That Impact the Success of Interorganizational Health Promotion Collaborations: A Scoping Review. Am. J. Health Promot. 2018, 32, 1095–1109. [Google Scholar] [CrossRef] [PubMed]
- Pratt, R.; Gyllstrom, B.; Gearin, K.; Hahn, D.; VanRaemdonck, L.; Peterson, K.; Baldwin, L.M. Primary Care and Public Health Perspectives on Integration at the Local Level: A Multi-State Study. J. Am. Board Fam. Med. 2017, 30, 601–607. [Google Scholar] [CrossRef] [Green Version]
- Schoen, M.W.; Moreland-Russell, S.; Prewitt, K.; Carothers, B.J. Social Network Analysis of Public Health Programs to Measure Partnership. Soc. Sci. Med. 2014, 123, 90–95. [Google Scholar] [CrossRef]
- Guldbrandsson, K.; Nordvik, M.K.; Bremberg, S. Identification of Potential Opinion Leaders in Child Health Promotion in Sweden Using Network Analysis. BMC Res. Notes 2012, 5, 424. [Google Scholar] [CrossRef] [Green Version]
- Held, F.; Hawe, P.; Roberts, N.; Conte, K.; Riley, T. Core and Peripheral Organisations in Prevention: Insights from Social Network Analysis. Health Promot. J. Aust. 2020. [Google Scholar] [CrossRef] [PubMed]
- McGlashan, J.; Nichols, M.; Korn, A.; Millar, L.; Marks, J.; Sanigorski, A.; Pachucki, M.; Swinburn, B.; Allender, S.; Economos, C. Social Network Analysis of Stakeholder Networks from Two Community-Based Obesity Prevention Interventions. PLoS ONE 2018, 13, e0196211. [Google Scholar] [CrossRef] [Green Version]
- Granner, M.L.; Sharpe, P.A. Evaluating Community Coalition Characteristics and Functioning: A Summary of Measurement Tools. Health Educ. Res. 2004, 19, 514–532. [Google Scholar] [CrossRef] [Green Version]
- Ndumbe-Eyoh, S.; Moffatt, H. Intersectoral Action for Health Equity: A Rapid Systematic Review. BMC Public Health 2013, 13, 1056. [Google Scholar] [CrossRef] [Green Version]
- Choi, B.C.K.; Pak, A.W.P. Multidisciplinarity, Interdisciplinarity, and Transdisciplinarity in Health Research, Services, Education and Policy: 2. Promotors, Barriers, and Strategies of Enhancement. Clin. Investig. Med. 2007, 30, E224–E232. [Google Scholar] [CrossRef] [Green Version]
- Wijenberg, E.; Wagemakers, A.; Herens, M.; den Hartog, F.; Koelen, M. The Value of the Participatory Network Mapping Tool to Facilitate and Evaluate Coordinated Action in Health Promotion Networks: Two Dutch Case Studies. Glob. Health Promot. 2019, 26, 32–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schröter, B.; Sattler, C.; Graef, F.; Chen, C.; Delgadillo, E.; Hackenberg, I.; Halle, E.M.; Hirt, A.; Kubatzki, A.; Matzdorf, B. Strengths and Weaknesses of the Net-Map Tool for Participatory Social Network Analysis in Resource Management: Experience from Case Studies Conducted on Four Continents. Methodol. Innov. 2018, 11, 2059799118787754. [Google Scholar] [CrossRef] [Green Version]
- Smith, B. Generalizability in Qualitative Research: Misunderstandings, Opportunities and Recommendations for the Sport and Exercise Sciences. Qual. Res. Sport Exerc. Health 2018, 10, 137–149. [Google Scholar] [CrossRef]
- Carminati, L. Generalizability in Qualitative Research: A Tale of Two Traditions. Qual. Health Res. 2018, 28, 2094–2101. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Actor | Function | Area, Sector |
|---|---|---|
| Office Manager A * | Administration and project management of the ‘Healthy Region Plus’ | City, Employee of the sports department |
| Office Manager B * | Administration and project management of the ‘Healthy Region Plus’ | County, Employee of the health department |
| Expert for health promotion in the county * | Representative and officer for health promotion and health equity | County, Employee of the health department |
| Director regional health department | Official lead of the ‘Healthy Region Plus’ | County, Employee of the health department |
| Chairperson senior advisory board * | Representative for the elderly and medical topics, General practitioner | City, Volunteer association, Part of the city council |
| Politician D * | Representative of the county | County, Part of the county council |
| Politician A * | Representative of the city | City, Major—Part of the city council |
| Chairperson of an association | Representative for medical issues and health promotion, General practitioner | City/County, Volunteer association |
| Employee C municipality * | Bridging function to communities and underrepresented population groups | City, Employee of the office for socio-cultural affairs |
| Actors/Topics | Degree | Betweenness Centrality | |
|---|---|---|---|
| 1. | GR+ office manager A | 12 | 144.57 |
| 2. | GR+ office manager B | 10 | 121.90 |
| 3. | Health Strategy | 10 | 102.58 |
| 4. | Expert for health promotion in the county | 6 | 16.65 |
| 5. | Scientist | 6 | 62.07 |
| 6. | Chairperson senior advisory board | 6 | 64.74 |
| 7. | Politician A | 6 | 42.24 |
| 8. | Chairperson of an association | 6 | 44.22 |
| 9. | Politician D | 5 | 109.0 |
| 10. | Politician B | 5 | 7.20 |
| 11. | Director regional sports department | 5 | 32.5 |
| 12. | Director regional health department | 4 | 2.0 |
| 13. | Working group | 3 | 29.0 |
| 14. | Employee C municipality | 2 | 29.0 |
| 15. | Politician E | 2 | 29.0 |
| 16. | Employee A municipality | 2 | 1.33 |
| 17. | GR+ office manager C | 2 | 0.0 |
| 18. | Employee B municipality | 2 | 0.0 |
| 19. | Employee D municipality | 2 | 0.0 |
| Actors/Artifacts | Degree | Betweenness Centrality | |
|---|---|---|---|
| 1. | Politician D | 15 | 431.25 |
| 2. | Chairperson senior advisory board | 11 | 383.54 |
| 3. | Politician A | 10 | 429.21 |
| 4. | GR+ office manager A | 8 | 276.0 |
| 5. | Chairperson of an association | 4 | 113.25 |
| 6. | Employee D municipality | 4 | 129.0 |
| 7. | Public relation | 3 | 238.26 |
| 8. | Health conference | 3 | 22.05 |
| 9. | Needs assessment | 3 | 22.05 |
| 10. | Project B | 3 | 118.0 |
| 11. | Politician H | 3 | 162.0 |
| 12. | Expert for health promotion in the county | 3 | 91.0 |
| 13. | Employee C municipality | 3 | 93.0 |
| 14. | Project A | 2 | 56.25 |
| 15. | Network B | 2 | 22.05 |
| 16. | Health strategy | 2 | 22.05 |
| 17. | Rules of procedure | 2 | 22.05 |
| 18. | Politicians | 2 | 105.0 |
| 19. | GR+ office manager B | 2 | 164.0 |
| 20. | Project E | 2 | 84.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fleuren, T.; Thiel, A.; Frahsa, A. Identification of Network Promoters in a Regional and Intersectoral Health Promotion Network: A Qualitative Social Network Analysis in Southern Germany. Int. J. Environ. Res. Public Health 2021, 18, 8372. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18168372
Fleuren T, Thiel A, Frahsa A. Identification of Network Promoters in a Regional and Intersectoral Health Promotion Network: A Qualitative Social Network Analysis in Southern Germany. International Journal of Environmental Research and Public Health. 2021; 18(16):8372. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18168372
Chicago/Turabian StyleFleuren, Tobias, Ansgar Thiel, and Annika Frahsa. 2021. "Identification of Network Promoters in a Regional and Intersectoral Health Promotion Network: A Qualitative Social Network Analysis in Southern Germany" International Journal of Environmental Research and Public Health 18, no. 16: 8372. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18168372