
Knowledge, Experience and Perception of Gender-Based Violence Health Services: A Mixed Methods Study on Adolescent Girls and Young Women in Tanzania

 , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Setting
2.2. Study Design and Population
2.3. Study Context
2.3.1. Inclusion Criteria
2.3.2. Exclusion Criteria
2.4. Part one: Quantitative Study
2.4.1. Study Design
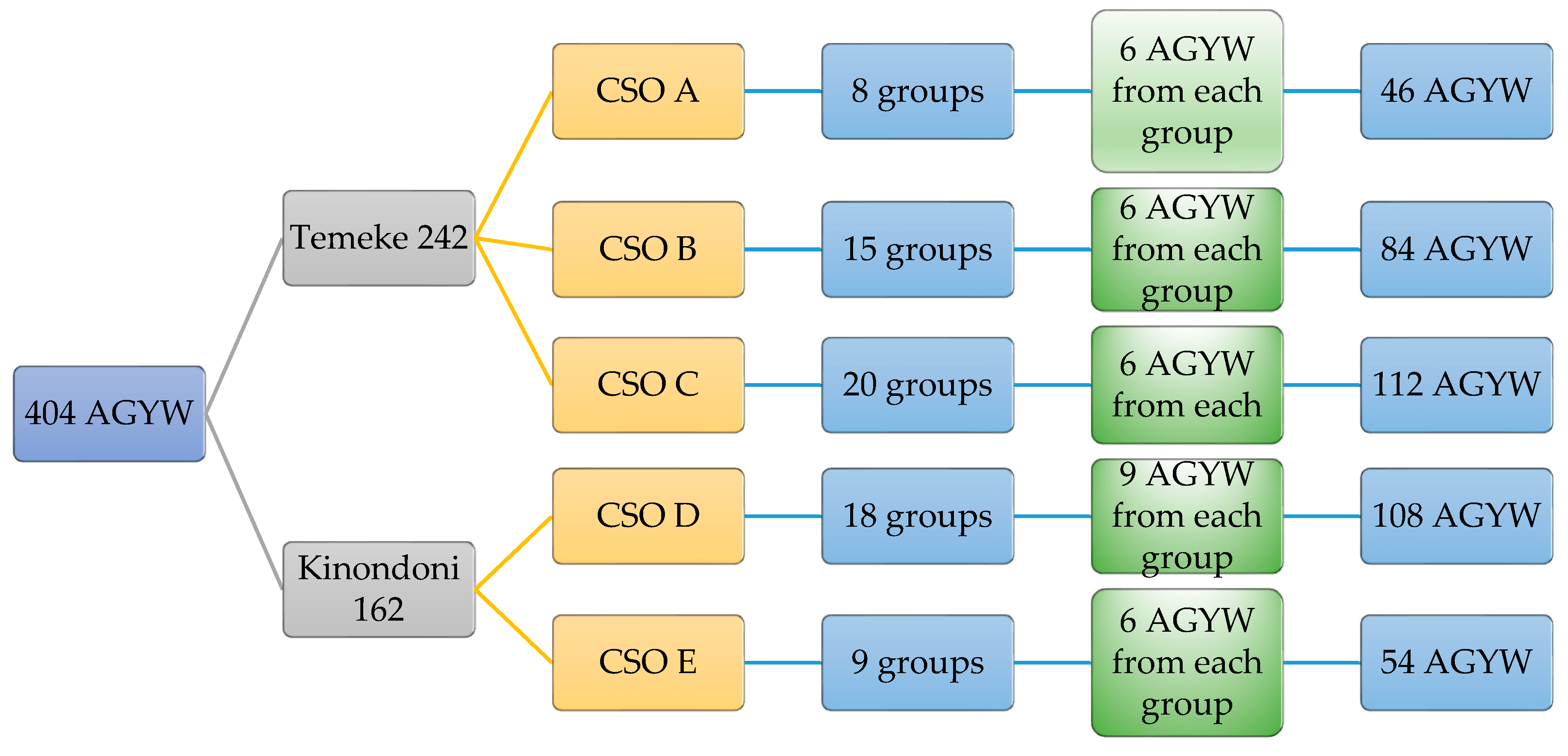
2.4.2. Sampling and Sample Size
2.4.3. Quantitative Data Collection
2.4.4. Data Analysis
2.5. Part Two: Qualitative Study
2.5.1. Study Design
2.5.2. Sampling and Sample Size
2.5.3. Qualitative Data Collection
2.5.4. Qualitative Data Analysis
2.5.5. Mixed Methods Integration
2.6. Ethical Considerations
3. Results
3.1. Socio-Demographic Characteristic of Study Participants
3.2. Knowledge of Gender-Based Violence Definition among AGYW
“My partner calls me names and abuses me all the time. He makes all of the decision when it comes to how we use all the money. I think with this, I am already used to it but am scared when he beats me”(AGYW, 19)
“GBV… it is something normal and usually happens to most of us. I know many girls who have experienced GBV including myself who has been raped and beaten. I was burnt by a cigarette when I refused a man’s advancement [proceeded to show interviewer healed burn wound]”(AGYW, 01)
“Sometimes women can be stubborn and a man can beat you to correct you, you know how women can be sometimes [chuckling] but when the beating becomes too much and without any good reason then it becomes a problem”(AGYW, 04)
“Many of us [AGYW] in this group understand what GBV is, but the problem is with men. They are the ones who beat and rape us. I think it would be good if men are involved in such [JHPIEGO SAUTI] projects and not only women”(AGYW 12)
3.3. Perceptions of and Experiences with GBV Health Services
“Haaa…it can never be…how can one remove the HIV virus from your blood after being raped by someone who has the virus…it is impossible. Likewise, how can one stop pregnancy when you have been raped and conceived. Unless one chooses to abort. I don’t think this is ever possible”(AGYW 09)
“When I was once violated, I went to the police to report it for further action, however the police were not supportive and even started asking me what I was doing late at night with men. They even started condemning me that I was prostituting. I would rather not go back to them.”(AGYW 03)
“As I told you I was raped when I went to the club on my form four graduation day [approximately 18 years old] where I ended up being raped by four strangers. My mother took me to a health facility where I was treated, and the doctor told me to forgive and forget what was done to me. How do I just forgive and forget? [starts crying angrily] And no, I was not linked to any social worker, how are they supposed to help?”(AGYW 07)
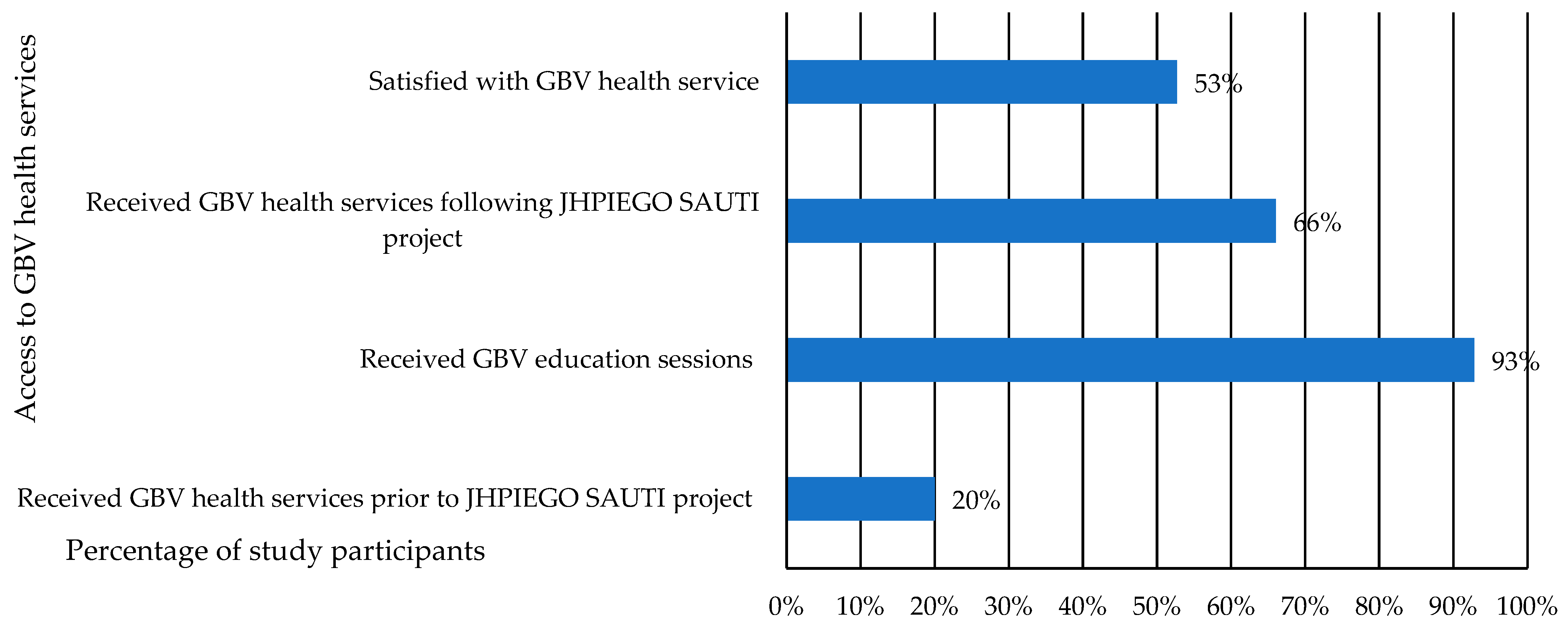
3.4. Access to Gender-Based Violence Services among AGYW
“When I was raped, I decided to keep quiet, I did not even tell my mother I was only 15 years old. I started to bleed [vaginal bleeding] but still kept quiet hoping it would somehow stop. After a week I started having painful abdominal pain and bad smell from my private area. I had to tell my mother who eventually took me to the hospital. The doctor blamed me for not reporting [the incident] sooner, so not much could be done. He gave me several pills and I got better eventually. That incident has affected me so badly. I still hate men, I am 23 years now and don’t wish to be with a man again.”(AGYW 17)
“After joining this [JHPIEGO SAUTI] project, they advised me to go the hospital because I was raped once. The doctor at the hospital informed me if it happens again, I should rush to the hospital immediately so that I can get pills to prevent from HIV and pregnancy and also, to get evidence for the police”(AGYW 15)
4. Discussion
4.1. Knowledge of GBV among AGYW
4.2. Perceptions of and Experiences with GBV Health Services among AGYW
4.3. Access to Gender-Based Violence Health Services among AGYW
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Griggs, D.; Stafford-Smith, M.; Gaffney, O.; Rockström, J.; Öhman, M.C.; Shyamsundar, P.; Steffen, W.; Glaser, G.; Kanie, N.; Noble, I. Policy: Sustainable development goals for people and planet. Nature 2013, 495, 305–307. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. The World Health Report 2002: Reducing Risks, Promoting Healthy Life; World Health Organization: Geneva, Switzerland, 2002. [Google Scholar]
- United Nations International Children’s Emergency Fund. Violence in the Lives of Children and Adolescents; UNICEF: New York, NY, USA, 2017. [Google Scholar]
- Humphreys, C.; Thiara, R. Mental health and domestic violence:‘I call it symptoms of abuse’. Br. J. Soc. Work 2003, 33, 209–226. [Google Scholar] [CrossRef]
- Procentese, F.; Di Napoli, I.; Tuccillo, F.; Chiurazzi, A.; Arcidiacono, C. Healthcare professionals’ perceptions and concerns towards domestic violence during pregnancy in Southern Italy. Int. J. Environ. Res. Public Health 2019, 16, 3087. [Google Scholar] [CrossRef] [Green Version]
- Saxena, S.; Sharan, P.; Garrido, M.; Saraceno, B. World Health Organization’s mental health atlas 2005: Implications for policy development. World Psychiatry 2006, 5, 179. [Google Scholar]
- Boyle, K. What’s in a name? Theorising the inter-relationships of gender and violence. Feminist Theory 2019, 20, 19–36. [Google Scholar] [CrossRef]
- Buiten, D.; Naidoo, K. Laying Claim to a Name: Towards a Sociology of “Gender-Based Violence”. S. Afr. Rev. Sociol. 2020, 1–8. [Google Scholar] [CrossRef]
- World Health Organization. Responding to Intimate Partner Violence and Sexual Violence against Women: WHO Clinical and Policy Guidelines; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- World Health Organization. The World Health Report 1999: Making a Difference; World Health Organization: Geneva, Switzerland, 1999. [Google Scholar]
- Krug, E.G.; Mercy, J.A.; Dahlberg, L.L.; Zwi, A.B. The world report on violence and health. Lancet 2002, 360, 1083–1088. [Google Scholar] [CrossRef] [Green Version]
- Njuki, R.; Okal, J.; Warren, C.E.; Obare, F.; Abuya, T.; Kanya, L.; Undie, C.-C.; Bellows, B.; Askew, I. Exploring the effectiveness of the output-based aid voucher program to increase uptake of gender-based violence recovery services in Kenya: A qualitative evaluation. BMC Public Health 2012, 12, 426. [Google Scholar] [CrossRef] [Green Version]
- Kohli, A.; Makambo, M.T.; Ramazani, P.; Zahiga, I.; Mbika, B.; Safari, O.; Bachunguye, R.; Mirindi, J.; Glass, N. A Congolese community-based health program for survivors of sexual violence. Confl. Health 2012, 6, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fennelly, K. Listening to the Experts: Provider Recommendations on the Health Needs of Immigrants and Refugees; School of International Migration and Ethnic Relations, Malmö University: Malmö, Sweden, 2004. [Google Scholar]
- Beckman, A.; Merlo, J.; Lynch, J.W.; Gerdtham, U.G.; Lindström, M.; Lithman, T. Country of birth, socioeconomic position, and healthcare expenditure: A multilevel analysis of Malmö, Sweden. J. Epidemiol. Commu. Health 2004, 58, 145–149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kamperman, A.M.; Komproe, I.H.; De Jong, J.T. Migrant mental health: A model for indicators of mental health and health care consumption. Health Psychol. 2007, 26, 96. [Google Scholar] [CrossRef]
- Muggah, E.; Dahrouge, S.; Hogg, W. Access to primary health care for immigrants: Results of a patient survey conducted in 137 primary care practices in Ontario, Canada. BMC Fam. Pract. 2012, 13, 128. [Google Scholar] [CrossRef] [Green Version]
- Heise, L.; Ellsberg, M.; Gottmoeller, M. A global overview of gender-based violence. Int. J. Gynaecol. Obstet. 2002, 78, S5–S14. [Google Scholar] [CrossRef]
- Liebling, H.; Barrett, H.; Artz, L. South Sudanese Refugee Survivors of Sexual and Gender-Based Violence and Torture: Health and Justice Service Responses in Northern Uganda. Int. J. Environ. Res. Public Health 2020, 17, 1685. [Google Scholar] [CrossRef] [Green Version]
- Melesse, D.Y.; Mutua, M.K.; Choudhury, A.; Wado, Y.D.; Faye, C.M.; Neal, S.; Boerma, T. Adolescent sexual and reproductive health in sub-Saharan Africa: Who is left behind? BMJ Global Health 2020, 5, e002231. [Google Scholar] [CrossRef] [Green Version]
- Mena-Tudela, D.; Gonzalez-Chorda, V.M.; Soriano-Vidal, F.J.; Bonanad-Carrasco, T.; Centeno-Rico, L.; Vila-Candel, R.; Castro-Sanchez, E.; Cervera Gasch, A. Changes in health sciences students’ perception of obstetric violence after an educational intervention. Nurse Educ. Today 2020, 88, 104364. [Google Scholar] [CrossRef] [PubMed]
- Muuo, S.; Muthuri, S.K.; Mutua, M.K.; McAlpine, A.; Bacchus, L.J.; Ogego, H.; Bangha, M.; Hossain, M.; Izugbara, C. Barriers and facilitators to care-seeking among survivors of gender-based violence in the Dadaab refugee complex. Sexual Reprod. Health Mtters 2020, 28, 1722404. [Google Scholar] [CrossRef] [Green Version]
- Coronella, F.; Tuccillo, F.; Di Napoli, I.; Arcidiacono, C. Women and domestic violence in the professional experience of Italian general practitioners (IGP). J. Interdiscip. J. Fam. Stud. 2012, 17. [Google Scholar]
- Arcidiacono, C.; Di Napoli, I. Sono caduta dalle scale. J. Attori Luoghi Della Violenza Genere 2013, 7, 218–223. [Google Scholar]
- García-Moreno, C.; Zimmerman, C.; Morris-Gehring, A.; Heise, L.; Amin, A.; Abrahams, N.; Montoya, O.; Bhate-Deosthali, P.; Kilonzo, N.; Watts, C. Addressing violence against women: A call to action. Lancet 2015, 385, 1685–1695. [Google Scholar] [CrossRef]
- Nyato, D.; Materu, J.; Kuringe, E.; Zoungrana, J.; Mjungu, D.; Lemwayi, R.; Majani, E.; Mtenga, B.; Nnko, S.; Munisi, G. Prevalence and correlates of partner violence among adolescent girls and young women: Evidence from baseline data of a cluster randomised trial in Tanzania. PLoS ONE 2019, 14, e0222950. [Google Scholar]
- Ministry of Health. Tanzania Demographic and Health Survey and Malaria Indicator Survey 2015–2016; MoHCDGEC, MoH, NBS, OCGS, and ICF: Dar es Salaam, Tanzania, 2016. [Google Scholar]
- Abeid, M.; Muganyizi, P.; Massawe, S.; Mpembeni, R.; Darj, E.; Axemo, P. Knowledge and attitude towards rape and child sexual abuse—A community-based cross-sectional study in rural Tanzania. BMC Public Health 2015, 15, 428. [Google Scholar] [CrossRef] [Green Version]
- Mtaita, C.L.; Likindikoki, S.; Mnjokava, S.; Mbita, G.; Safary, E.; Hilliard, D.; Jahn, A. Accessibility to Gender-based Violence Health Services for Adolescent Girls and Young Women in Tanzania. J. Transl. Med. Res. Public Health 2021, 5, 125–134. [Google Scholar]
- National Bureau of Statistics. The 2012 Population and Housing Census: Basic Demographic and Socio-Economic Profile; National Bureau of Statistics: Dar es Salaam, Tanzania, 2014. [Google Scholar]
- Creswell, J.W. Research Design: Qualitative, Quantitative, and Mixed Methods Approaches; SAGE Publications: Los Angeles, CA, USA, 2009. [Google Scholar]
- Ahikire, J.; Mwiine, A.A. Addressing the Links between Gender-Based Violence and HIV in the Great Lakes Region; Country Report Uganda. Kampala, United Nations Educational, Scientific and Cultural Organization: Unpublished, 2012. [Google Scholar]
- Hsieh, H.F.; Shannon, S.E. Three approaches to qualitative content analysis. Qualitative Health Res. 2005, 15, 1277–1288. [Google Scholar] [CrossRef] [PubMed]
- Price, B. Laddered questions and qualitative data research interviews. J. Adv. Nurs. 2002, 37, 273–281. [Google Scholar] [CrossRef]
- Fetters, M.D.; Curry, L.A.; Creswell, J.W. Achieving Integration in Mixed Methods Designs—Principles and Practices. Health Serv. Res. 2013, 48, 2134–2156. [Google Scholar] [CrossRef] [Green Version]
- McCleary-Sills, J.; Namy, S.; Nyoni, J.; Rweyemamu, D.; Salvatory, A.; Steven, E.; ICRW. Help-Seeking Pathways and Barriers for Survivors of Gender-based Violence in Tanzania. Results from a Study in Dar Es Salaam, Mbeya, and Iringa Regions; International Center for Research on Women (ICRW): Dar es Salaam, Tanzania, 2013. [Google Scholar]
- Ochako, R.; Ulwodi, D.; Njagi, P.; Kimetu, S.; Onyango, A. Trends and determinants of Comprehensive HIV and AIDS knowledge among urban young women in Kenya. AIDS Res. Ther. 2011, 8, 11. [Google Scholar] [CrossRef] [Green Version]
- Gebre, T.; Hagos, F.; Teklu, G.; Fisseha, M.; Abera, M. The prevalence of gender-based violence and harmful traditional practices against women in the Tigray Region, Ethiopia. J. Asian Afr. Stud. 2020, 55, 58–75. [Google Scholar] [CrossRef]
- Deyessa, N.; Berhane, Y.; Ellsberg, M.; Emmelin, M.; Kullgren, G.; Högberg, U. Violence against women in relation to literacy and area of residence in Ethiopia. Glob. Health Action 2010, 3, 2070. [Google Scholar] [CrossRef]
- Okenwa, L.E.; Lawoko, S.; Jansson, B. Exposure to intimate partner violence amongst women of reproductive age in Lagos, Nigeria: Prevalence and predictors. J. Fam. Viol. 2009, 24, 517–530. [Google Scholar] [CrossRef]
- Ilika, A.L. Women’s perception of partner violence in a rural Igbo community. Afr. J. Reprod. Health 2005, 9, 77–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahlori, X.F.; Byrne, D.C.; Mabude, L.A. Perceptions of gender-based violence among university staff: Interim results. Sage Open 2018, 8, 2158244018800163. [Google Scholar] [CrossRef] [Green Version]
- Fleming, P.J.; Gruskin, S.; Rojo, F.; Dworkin, S.L. Men’s violence against women and men are inter-related: Recommendations for simultaneous intervention. Soc. Sci. Med. 2015, 146, 249–256. [Google Scholar] [CrossRef] [Green Version]
- Abeid, M.; Muganyizi, P.; Olsson, P.; Darj, E.; Axemo, P. Community perceptions of rape and child sexual abuse: A qualitative study in rural Tanzania. BMC Int. Health Hum. Rights 2014, 14, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Miura, A.; Fujiwara, T. Intimate partner violence during pregnancy and postpartum depression in Japan: A cross-sectional study. Front. Public Health 2017, 5, 81. [Google Scholar] [CrossRef] [Green Version]
- Ziaei, S.; Frith, A.L.; Ekström, E.-C.; Naved, R.T. Experiencing lifetime domestic violence: Associations with mental health and stress among pregnant women in rural Bangladesh: The MINIMat Randomized Trial. PLoS ONE 2016, 11, e0168103. [Google Scholar] [CrossRef] [Green Version]
- Laisser, R.M.; Lugina, H.I.; Lindmark, G.; Nystrom, L.; Emmelin, M. Striving to make a difference: Health care worker experiences with intimate partner violence clients in Tanzania. Health Care Women Int. 2009, 30, 64–78. [Google Scholar] [CrossRef]
- Bell, K.M.; Naugle, A.E. Intimate partner violence theoretical considerations: Moving towards a contextual framework. Clin. Psychol. Rev. 2008, 28, 1096–1107. [Google Scholar] [CrossRef] [PubMed]
- Scheppers, E.; Van Dongen, E.; Dekker, J.; Geertzen, J.; Dekker, J. Potential barriers to the use of health services among ethnic minorities: A review. Fam. Pract. 2006, 23, 325–348. [Google Scholar] [CrossRef]
- Skinner, D.; Mfecane, S.; Gumede, T.; Henda, N.; Davids, A. Barriers to accessing PMTCT services in a rural area of South Africa. Afr. J. AIDS Res. 2005, 4, 115–123. [Google Scholar] [CrossRef]
- United Nations High Commissioner for Refugees. Sexual and Gender-based Violence against Refugees, Returnees and Displaced Persons; UNHCR, United Nations High Commissioner for Refugees: Geneva, Switzerland, 2003. [Google Scholar]
- Kishor, S.; Johnson, K. Profiling domestic violence: A multi-country study. Stud. Fam. Plann. 2004, 43, 57–62. [Google Scholar] [CrossRef]
- Simkhada, B.; Teijlingen, E.R.; Porter, M.; Simkhada, P. Factors affecting the utilization of antenatal care in developing countries: Systematic review of the literature. J. Adv. Nurs. 2008, 61, 244–260. [Google Scholar] [CrossRef]
- Eaton, L.A.; Kalichman, S.C. Changes in transmission risk behaviors across stages of HIV disease among people living with HIV. J. Assoc. Nurses AIDS Care 2009, 20, 39–49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bulman, K.H.; McCourt, C. Somali refugee women’s experiences of maternity care in west London: A case study. Crit. Public Health 2002, 12, 365–380. [Google Scholar] [CrossRef]
- Norredam, M.; Krasnik, A.; Sorensen, T.M.; Keiding, N.; Michaelsen, J.J.; Nielsen, A.S. Emergency room utilization in Copenhagen: A comparison of immigrant groups and Danish-born residents. Scand. J. Public Health 2004, 32, 53–59. [Google Scholar] [CrossRef]
- Rhodes, P.; Nocon, A.; Wright, J. Access to diabetes services: The experiences of Bangladeshi people in Bradford, UK. Ethn. Health 2003, 8, 171–188. [Google Scholar] [CrossRef] [PubMed]
- Okereke, G.O. Violence against women in Africa. Afr. J. Criminol. Justice Stud. 2006, 2, 1–35. [Google Scholar]



{kind=link}
{kind=link}
| Characteristics | Frequency n (%) |
|---|---|
| District Name | |
| Kinondoni | 161 (39.7) |
| Temeke | 242 (60.3) |
| Age | |
| 15–17 | 44 (10.9) |
| 18–20 | 129 (32.0) |
| 21–24 | 230 (57.1) |
| Level of Education | |
| No Formal Education | 97 (24.1) |
| Primary Education | 240 (59.6) |
| Secondary and Higher Education | 66 (16.4) |
| Primary Occupation | |
| Employed | 48 (11.9) |
| Owned Small Business | 83 (20.6) |
| Student | 12 (3.0) |
| Sex Worker | 151 (37.5) |
| Unemployed | 109 (27.1) |
| Number of children | |
| None | 224 (55.6) |
| One | 135 (33.5) |
| Two and Above | 44 (10.6) |
| Marital Status | |
| Single | 127 (31.5) |
| Married | 97 (24.1) |
| Cohabiting | 29 (7.2) |
| Separated/Divorced | 30 (7.4) |
| Have a Partner but not Cohabitating | 120 (29.8) |
| Estimated Income (TZS.) | |
| 0–25,000 | 384 (95.3) |
| 25,001–50,000 | 11 (2.8) |
| 50,001 and Above | 8 (2.0) |
| Level of Knowledge | |||
|---|---|---|---|
| Good | Moderate | Limited | |
| Ability to Define GBV | 108 (26.8%) | 206 (51.1%) | 89 (22.1) |
| Yes (%) | No (%) | ||
| Forms of Violence | |||
| Sexual Violence | 322 (79.9%) | 81 (20.1%) | |
| Physical Violence | 262 (65.0%) | 141 (35.0%) | |
| Emotional Violence | 166 (41.2%) | 237 (58.8%) | |
| Economic Violence | 107 (26.6%) | 296 (73.4%) | |
| Statement | Strongly Agree/Agree | Neutral | Disagree/Strongly Disagree |
|---|---|---|---|
| 1. HCWs can Prevent Violence from Reoccurring | 117 (29.1%) | 94 (23.3%) | 192 (47.6%) |
| 2. HCWs offer PEP for the Prevention of HIV Following Rape | 146 (36.2%) | 78 (19.4%) | 179 (44.4%) |
| 3. HCWs offer EC for Prevention of Pregnancy Following Rape | 82 (20.3%) | 87 (21.6%) | 234 (58.1%) |
| 4. HCWs offer Psychological and Counselling Services to GBV Survivors | 87 (21.6%) | 109 (27.0%) | 207 (51.4%) |
| 5. HCWs can Link GBV Survivors to Psychosocial Support (Counselling) | 59 (14.6%) | 102 (25.3%) | 242 (60.1%) |
| 6. HCWs can Link GBV Survivors to Legal Aid Services | 203 (50.4%) | 84 (20.8%) | 116 (28.8%) |
| 7. HCWs can Assist in Collection of Evidence for Forensic Medical Services | 43 (10.7%) | 95 (23.8%) | 264 (65.5%) |
| 8. GBV Survivors can Access GBV Health Services for the Treatment of Physical Injuries | 259 (64.3%) | 62 (15.4%) | 82 (20.3%) |
| Main Reason for Refusing a GBV Escorted Referral | n = 155 | % |
|---|---|---|
| Fear of HIV Testing | 49 | 31.4 |
| Fear of Confirming an HIV-Positive Status | 29 | 18.6 |
| GBV Occurred a Long Time Ago | 21 | 14.1 |
| Accessed Health Facility Prior to JHPIEGO SAUTI Project | 19 | 12.2 |
| Felt physically healthy | 37 | 23.7 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mtaita, C.; Likindikoki, S.; McGowan, M.; Mpembeni, R.; Safary, E.; Jahn, A. Knowledge, Experience and Perception of Gender-Based Violence Health Services: A Mixed Methods Study on Adolescent Girls and Young Women in Tanzania. Int. J. Environ. Res. Public Health 2021, 18, 8575. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18168575
Mtaita C, Likindikoki S, McGowan M, Mpembeni R, Safary E, Jahn A. Knowledge, Experience and Perception of Gender-Based Violence Health Services: A Mixed Methods Study on Adolescent Girls and Young Women in Tanzania. International Journal of Environmental Research and Public Health. 2021; 18(16):8575. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18168575
Chicago/Turabian StyleMtaita, Caroline, Samuel Likindikoki, Maureen McGowan, Rose Mpembeni, Elvis Safary, and Albrecht Jahn. 2021. "Knowledge, Experience and Perception of Gender-Based Violence Health Services: A Mixed Methods Study on Adolescent Girls and Young Women in Tanzania" International Journal of Environmental Research and Public Health 18, no. 16: 8575. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18168575