
The Influence of Rehabilitation on Quality of Life in Breast Cancer Survivors: A Clinical Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Measures
2.2. Evaluation Scales
2.2.1. Pain
2.2.2. QoL
2.2.3. Personality Traits
2.2.4. Rehabilitative Treatment
2.2.5. First Phase
2.2.6. Second Phase
3. Results
3.1. Statistical Analyses
3.1.1. Frequencies and Descriptive
3.1.2. Time Series Analysis
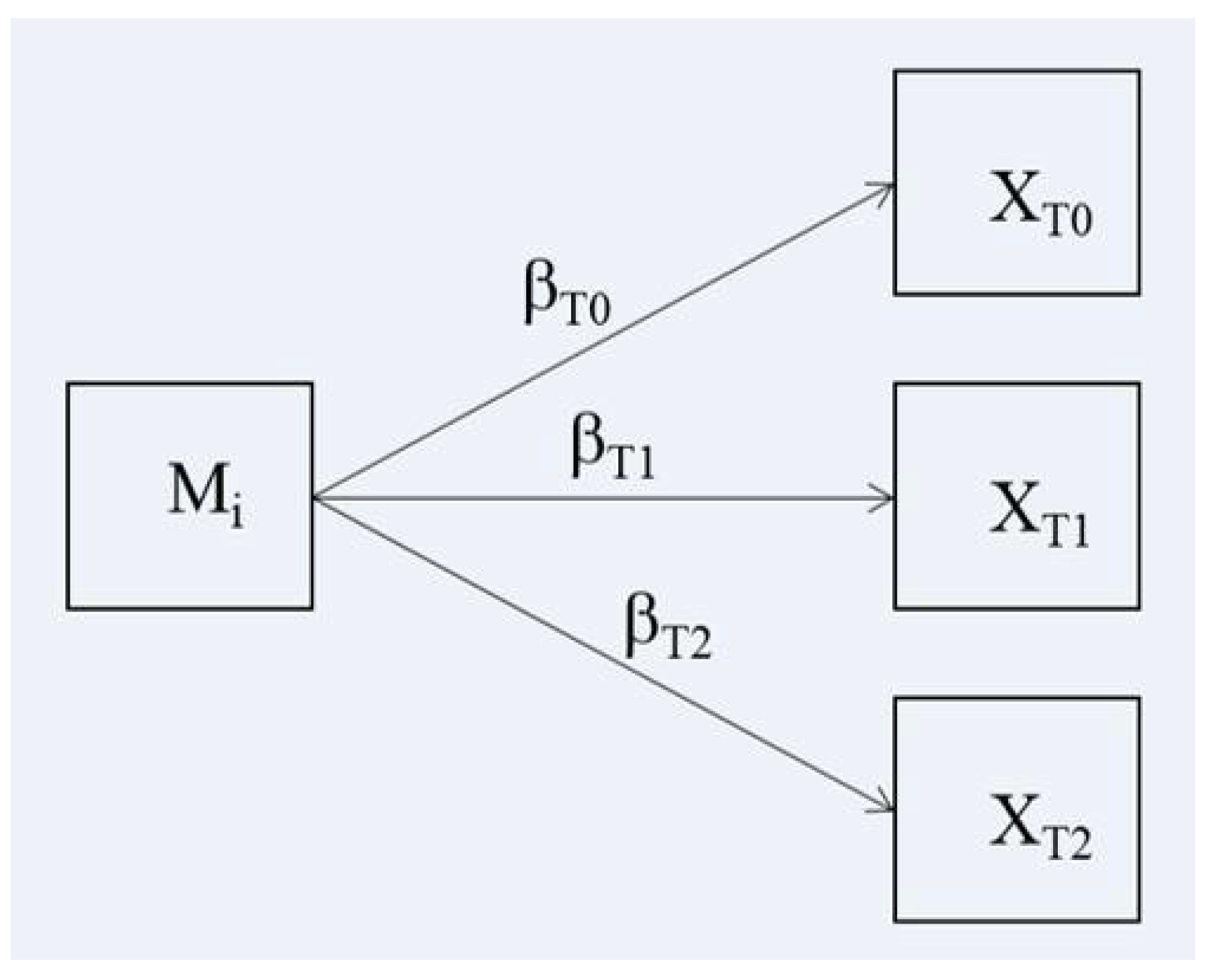
3.1.3. Moderation Effects in Time Series of Psychological Traits
3.2. Patients’ Data
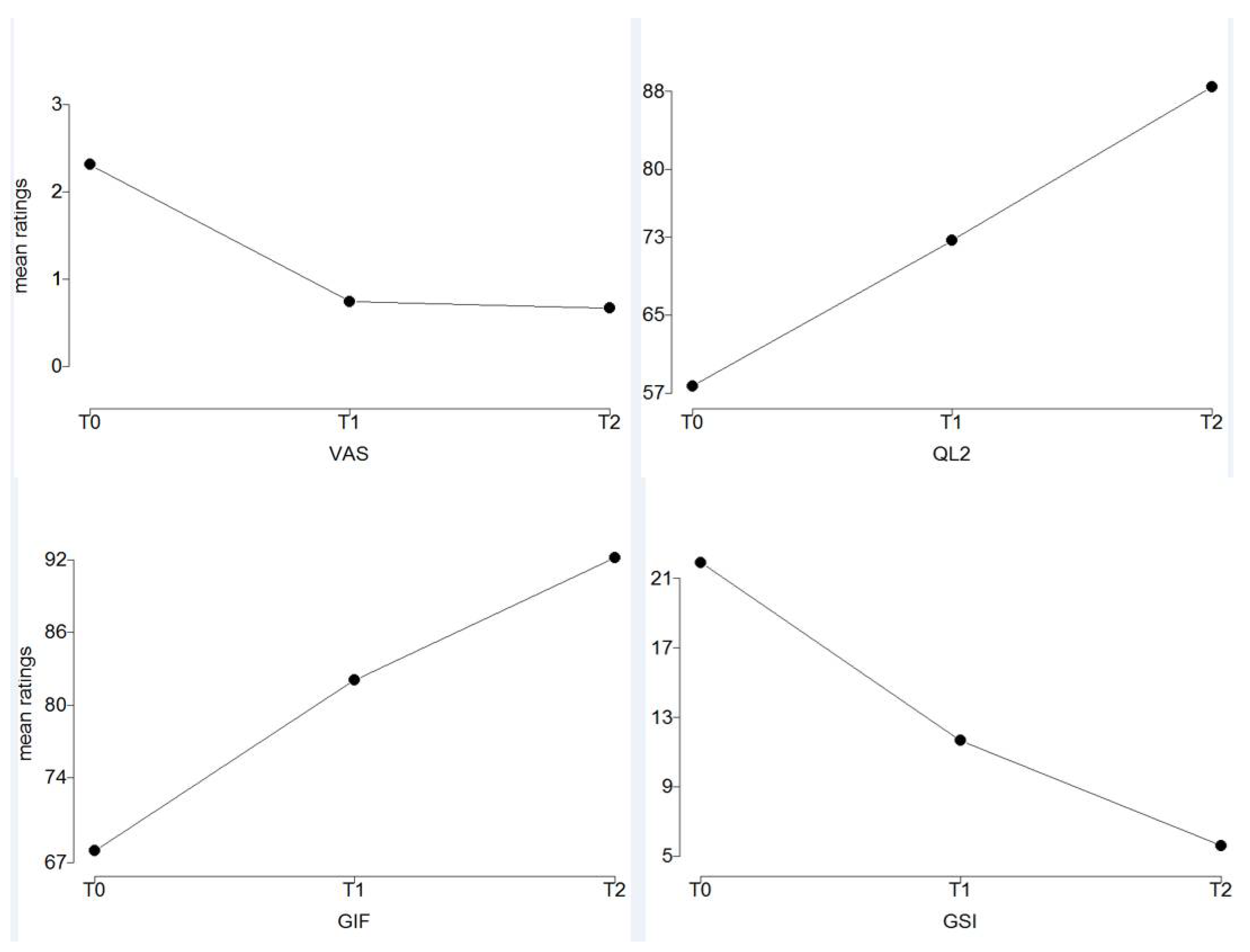
3.3. Effects of Rehabilitation on Pain, Functioning, and Severity of Physical Symptoms
3.4. Rehabilitation and Psychological Traits
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- de Sire, A.; Fusco, N.; Sajjadi, E.; Lippi, L.; Cisari, C.; Invernizzi, M. Lymphedema Rehabilitation Using Self-Adaptive Inelastic Compression in Breast Cancer: A Proof-of-Principle Study. Appl. Sci. 2021, 11, 1901. [Google Scholar] [CrossRef]
- Villar, R.R.; Fernández, S.P.; Garea, C.C.; Pillado, M.T.S.; Barreiro, V.B.; Martín, C.G. Quality of life and anxiety in women with breast cancer before and after treatment. Rev. Lat. Am. Enferm. 2017, 25, e2958. [Google Scholar] [CrossRef]
- Lopes, J.V.; Bergerot, C.D.; Barbosa, L.R.; Calux, N.M.C.T.; Elias, S.; Ashing, K.T.; Domenico, E.B.L. Impact of breast cancer and quality of life of women survivors. Rev. Bras. Enferm. 2018, 71, 2916–2921, (In English, Portuguese). [Google Scholar] [CrossRef]
- de Sire, A.; Losco, L.; Cisari, C.; Gennari, A.; Boldorini, R.; Fusco, N.; Cigna, E.; Invernizzi, M. Axillary web syndrome in women after breast cancer surgery referred to an Oncological Rehabilitation Unit: Which are the main risk factors? A retrospective case-control study. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 8028–8035. [Google Scholar] [CrossRef] [PubMed]
- Mangone, M.; Bernetti, A.; Agostini, F.; Paoloni, M.; De Cicco, F.A.; Capobianco, S.V.; Bai, A.V.; Bonifacino, A.; Santilli, V.; Paolucci, T. Changes in Spine Alignment and Postural Balance After Breast Cancer Surgery: A Rehabilitative Point of View. Biores. Open Access 2019, 8, 121–128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morone, G.; Iosa, M.; Fusco, A.; Scappaticci, A.; Alcuri, M.R.; Saraceni, V.M.; Paolucci, S.; Paolucci, T. Effects of a multidisciplinary educational rehabilitative intervention in breast cancer survivors: The role of body image on quality of life outcomes. Sci. World J. 2014, 2014, 451935. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paolucci, T.; Bernetti, A.; Paoloni, M.; Capobianco, S.V.; Bai, A.V.; Lai, C.; Pierro, L.; Rotundi, M.; Damiani, C.; Santilli, V.; et al. Therapeutic Alliance in a Single Versus Group Rehabilitative Setting After Breast Cancer Surgery: Psychological Profile and Performance Rehabilitation. Biores. Open Access 2019, 8, 101–110. [Google Scholar] [CrossRef] [Green Version]
- Bernetti, A.; Mangone, M.; Alviti, F.; Paolucci, T.; Attanasi, C.; Murgia, M.; Di Sante, L.; Agostini, F.; Vitale, M.; Paoloni, M. Spa therapy and rehabilitation of musculoskeletal pathologies: A proposal for best practice in Italy. Int. J. Biometeorol. 2020, 64, 905–914. [Google Scholar] [CrossRef]
- Lee, J.R.; Oh, P.J. A Structural Model for Chemotherapy Related Cognitive Impairment and Quality of Life in Breast Cancer Patients. J. Korean Acad. Nurs. 2019, 49, 375–385. (In Korean) [Google Scholar] [CrossRef] [PubMed]
- Stubblefield, M.D. The Underutilization of Rehabilitation to Treat Physical Impairments in Breast Cancer Survivors. PM R 2017, 9, S317–S323. [Google Scholar] [CrossRef]
- Patsou, E.D.; Alexias, G.T.; Anagnostopoulos, F.G.; Karamouzis, M.V. Physical activity and sociodemographic variables related to global health, quality of life, and psychological factors in breast cancer survivors. Psychol. Res. Behav. Manag. 2018, 11, 371–381. [Google Scholar] [CrossRef] [Green Version]
- Park, J.H.; Jung, Y.S.; Jung, Y.M.; Bae, S.H. The role of depression in the relationship between cognitive decline and quality of life among breast cancer patients. Support. Care Cancer 2019, 27, 2707–2714. [Google Scholar] [CrossRef]
- Dell’Antônio Pereira, L.; Brandão-Souza, C.; Amaral Musso, M.A.; Vieira Calmon, M.; Costa Neto, S.B.; Monteiro de Barros Miotto, M.H.; Zandonade, E.; Costa Amorim, M.H. Quality of life of women with pre-and post-operative breast cancer. Investig. Educ. Enferm. 2017, 35, 109–119. [Google Scholar] [CrossRef] [Green Version]
- Ng, E.T.; Ang, R.Z.; Tran, B.X.; Ho, C.S.; Zhang, Z.; Tan, W.; Bai, Y.; Zhang, M.; Tam, W.W.; Ho, R.C. Comparing Quality of Life in Breast Cancer Patients Who Underwent Mastectomy Versus Breast-Conserving Surgery: A Meta-Analysis. Int. J. Environ. Res. Public Health 2019, 16, 4970. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herring, B.; Paraskeva, N.; Tollow, P.; Harcourt, D. Women’s initial experiences of their appearance after mastectomy and/or breast reconstruction: A qualitative study. Psychooncology 2019, 28, 2076–2082. [Google Scholar] [CrossRef]
- Craig, A.D. Interoception: The sense of the physiological condition of the body. Curr. Opin. Neurobiol. 2003, 13, 500–505. [Google Scholar] [CrossRef]
- Craig, A.D. A new view of pain as a homeostatic emotion. Trends Neurosci. 2003, 26, 303–307. [Google Scholar] [CrossRef]
- Osumi, M.; Imai, R.; Ueta, K.; Nakano, H.; Nobusako, S.; Morioka, S. Factors associated with the modulation of pain by visual distortion of body size. Front. Hum. Neurosci. 2014, 8, 137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olsson Möller, U.; Beck, I.; Rydén, L.; Malmström, M. A comprehensive approach to rehabilitation interventions following breast cancer treatment—A systematic review of systematic reviews. BMC Cancer 2019, 19, 472. [Google Scholar] [CrossRef] [Green Version]
- Des Jarlais, D.C.; Lyles, C.; Crepaz, N.; TREND Group. Improving the reporting quality of nonrandomized evaluations of behavioral and public health interventions: The TREND statement. Am. J. Public Health 2004, 94, 361–366. [Google Scholar] [CrossRef]
- Myles, P.S.; Myles, D.B.; Galagher, W.; Boyd, D.; Chew, C.; MacDonald, N.; Dennis, A. Measuring acute postoperative pain using the visual analog scale: The minimal clinically important difference and patient acceptable symptom state. Br. J. Anaesth. 2017, 118, 424–429. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campbell, W.I.; Lewis, S. Visual analogue measurement of pain. Ulster Med. J. 1990, 59, 149–154. [Google Scholar]
- Aaronson, N.K.; Ahmedzai, S.; Bergman, B.; Bullinger, M.; Cull, A.; Duez, N.J.; Filiberti, A.; Flechtner, H.; Fleishman, S.B.; de Haes, J.C.; et al. The European Organization for Research and Treatment of Cancer QLQ-C30: A quality-of-life instrument for use in international clinical trials in oncology. J. Natl. Cancer Inst. 1993, 85, 365–376. [Google Scholar] [CrossRef] [PubMed]
- Fayers, P.; Aaronson, N.K.; Bjordal, K.; Curran, D.; Groenveld, M. EORTC QLQ-C30 Scoring Manual, 2nd ed.; EORT: Brussels, Belgium, 1999. [Google Scholar]
- Apolone, G.; Filiberti, A.; Cifani, S.; Ruggiata, R.; Mosconi, P. Evaluation of the EORTC QLQ-C30 questionnaire: A comparison with SF-36 Health Survey in a cohort of Italian long-survival cancer patients. Ann. Oncol. 1998, 9, 549–557. [Google Scholar] [CrossRef] [PubMed]
- Pancheri, P.; Sirigatti, S.; Biondi, M. Adaptation of the MMPI-2 in Italy. In International Adaptation of the MMPI-2: Research and Clinical Application; Butcher, J.N., Ed.; University of Minnesota Press: Minneapolis, MN, USA, 1996. [Google Scholar]
- Graham, J.R. MMPI-2: Assessing Personality and Psychopathology, 3rd ed.; Oxford University Press: New York, NY, USA, 2000. [Google Scholar]
- Paolucci, T.; Bernetti, A.; Bai, A.V.; Segatori, L.; Monti, M.; Maggi, G.; Ippolitoni, G.; Tinelli, L.; Santilli, V.; Paoloni, M.; et al. The sequelae of mastectomy and quadrantectomy with respect to the reaching movement in breast cancer survivors: Evidence for an integrated rehabilitation protocol during oncological care. Support. Care Cancer 2021, 29, 899–908. [Google Scholar] [CrossRef] [PubMed]
- Paolucci, T.; Bernetti, A.; Bai, A.V.; Capobianco, S.V.; Bonifacino, A.; Maggi, G.; Ippolitoni, G.; Tinelli, L.; Santilli, V.; Agostini, F.; et al. The recovery of reaching movement in breast cancer survivors: Two different rehabilitative protocols in comparison. Eur J. Phys. Rehabil. Med. 2021, 57, 137–147. [Google Scholar] [CrossRef] [PubMed]
- Gravetter, F.; Wallnau, L. Essentials of Statistics for the Behavioral Sciences, 8th ed.; Wadsworth: Belmont, CA, USA, 2014. [Google Scholar]
- Trochim, W.M.K.; Donnelly, J.P. The Research Methods Knowledge Base, 3rd ed.; Atomic Dog: Cincinnati, OH, USA, 2006. [Google Scholar]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef]
- Montoya, A.K. Moderation analysis in two-instance repeated measures designs: Probing methods and multiple moderator models. Behav. Res. Methods 2019, 51, 61–82. [Google Scholar] [CrossRef] [PubMed]
- Muthen, L.K.; Muthen, B.O. Mplus User’s Guide, 7th ed.; Muthén & Muthén: Los Angeles, CA, USA, 2012. [Google Scholar]
- Invernizzi, M.; de Sire, A.; Lippi, L.; Venetis, K.; Sajjadi, E.; Gimigliano, F.; Gennari, A.; Criscitiello, C.; Cisari, C.; Fusco, N. Impact of Rehabilitation on Breast Cancer Related Fatigue: A Pilot Study. Front. Oncol. 2020, 10, 2183. [Google Scholar] [CrossRef]
- Wirtz, P.; Baumann, F.T. Physical Activity, Exercise and Breast Cancer—What Is the Evidence for Rehabilitation, Aftercare, and Survival? A Review. Breast Care 2018, 13, 93–101. [Google Scholar] [CrossRef]
- Meneses-Echávez, J.F.; González-Jiménez, E.; Ramírez-Vélez, R. Effects of supervised exercise on cancer-related fatigue in breast cancer survivors: A systematic review and meta-analysis. BMC Cancer 2015, 15, 77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kirkham, A.A.; Bonsignore, A.; Bland, K.A.; McKenzie, D.C.; Gelmon, K.A.; VAN Patten, C.L.; Campbell, K.L. Exercise Prescription and Adherence for Breast Cancer: One Size Does Not FITT All. Med. Sci. Sports Exerc. 2018, 50, 177–186. [Google Scholar] [CrossRef] [PubMed]
- Costa, W.A.; Monteiro, M.N.; Queiroz, J.F.; Gonçalves, A.K. Pain and quality of life in breast cancer patients. Clinics 2017, 72, 758–763. [Google Scholar] [CrossRef]
- İzci, F.; Sarsanov, D.; Erdogan, Z.İ.; İlgün, A.S.; Çelebi, E.; Alço, G.; Kocaman, N.; Ordu, Ç.; Öztürk, A.; Duymaz, T.; et al. Impact of Personality Traits, Anxiety, Depression and Hopelessness Levels on Quality of Life in the Patients with Breast Cancer. Eur. J. Breast Health 2018, 14, 105–111. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Descriptive Variables | Mean ± Sd | Min, Max | Skewness | Kurtosis |
|---|---|---|---|---|
| Age | 52.00 ± 6.50 | 36, 60 | −0.53 | −0.51 |
| BMI | 23.95 ± 3.61 | 18, 32 | 0.64 | −0.56 |
| TfI (months) | 9.67 ± 5.12 | 2, 24 | 0.94 | 0.89 |
| Frequencies | Type | N | % | |
| Family status | Single | 8 | 21.05 | |
| Conjugated | 28 | 73.68 | ||
| Married | 1 | 2.63 | ||
| Divorced | 1 | 2.63 | ||
| Profession | Occupied | 29 | 74.36 | |
| Homeworking | 4 | 10.53 | ||
| Unemployed | 5 | 13.16 | ||
| Education | Secondary school | 5 | 13.16 | |
| High school | 25 | 65.79 | ||
| University | 8 | 21.05 |
| Scales for Rehabilitation Assessment | Trend | Estimated Coefficient | Std. Error | t Value | Pr(>|t|) | Cohen’s d | Effect Size Level |
|---|---|---|---|---|---|---|---|
| VAS | lin. | −1.641 | 0.222 | −7.395 | <0.001 | 2.368 | high |
| quadr. | −1.487 | 0.187 | −7.959 | <0.001 | 2.549 | high | |
| QL2 | lin. | 30.718 | 3.757 | 8.176 | <0.001 | 2.618 | high |
| quadr. | −0.821 | 4.193 | −0.196 | 0.846 | |||
| GIF | lin. | 24.230 | 3.530 | 6.865 | <0.001 | 2.199 | high |
| quadr. | 3.974 | 3.405 | 1.167 | 0.250 | |||
| GSI | lin. | −16.282 | 2.634 | −6.182 | <0.001 | 1.980 | high |
| quadr. | −4.179 | 2.434 | −1.717 | 0.094 |
| MMPI SCALES | Mean | Sd | Skewness | Kurtosis | |
|---|---|---|---|---|---|
| Validity Scales | Lie (L) | 55.667 | 7.593 | 0.093 | −0.541 |
| Frequency (F) | 51.077 | 7.600 | 0.315 | −1.042 | |
| Correction (K) | 48.385 | 8.780 | −0.148 | −0.777 | |
| Clinical/Personality Scales | Hypochondriasis (HS) | 62.359 | 12.162 | 0.486 | −0.487 |
| Depression (D) | 56.769 | 10.963 | 0.726 | 0.252 | |
| Hysteria (HY) | 57.462 | 12.185 | 0.625 | −0.032 | |
| Psychopathic Deviate (PD) | 52.949 | 8.516 | −0.414 | 1.166 | |
| Masculinity-Femininity (MF) | 51.615 | 11.502 | 1.372 | 4.100 | |
| Paranoid (PA) | 51.667 | 8.106 | 0.203 | −0.224 | |
| Psychasthenia (PT) | 50.795 | 8.865 | 0.345 | −0.386 | |
| Schizophrenia (SC) | 54.333 | 6.698 | 0.433 | −0.844 | |
| Hypomania (MA) | 45.385 | 9.101 | 0.705 | −0.039 | |
| Social Introversion (SI) | 50.103 | 10.694 | 0.348 | −0.529 | |
| Content Scales | Anxiety (ANX) | 55.513 | 9.660 | 0.017 | −0.665 |
| Fears (FRS) | 55.205 | 10.360 | 0.015 | −0.791 | |
| Obsessiveness (OBS) | 48.256 | 7.351 | 0.124 | −0.937 | |
| Depression (DEP) | 51.897 | 8.804 | 0.274 | −0.633 | |
| Health Concerns (HEA) | 59.949 | 11.693 | 0.092 | −1.067 | |
| Negative Treatment Indicators (TRT) | 51.513 | 11.541 | 0.077 | −0.827 |
| Time Periods | Mediation Analysis | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| T0 | T1 | T2 | Clinic Period | Home Period | |||||||||
| MMPI Scales | β T0 (s.e.) | β′T0 | β T1 (s.e.) | β′T1 | β T2 (s.e.) | β′T2 | βT1–βT0 (s.e.) | t | p(t) | βT2–βT1 (s.e.) | t | p(t) | |
| QL2 | HS | −0.496 (0.307) | −0.251 | −0.559 (0.301) | −0.285 | −0.225 (0.175) | −0.202 | −0.063 (0.186) | −0.340 | 0.734 | 0.335 (0.264) | 1.269 | 0.204 |
| D | −0.445 (0.344) | −0.203 | −0.633 (0.334) | −0.290 | −0.023 (0.198) | −0.019 | −0.187 (0.205) | −0.913 | 0.361 | 0.609 (0.282) | 2.161 | 0.031 | |
| HY | −0.499 (0.306) | −0.253 | −0.548 (0.301) | −0.279 | −0.132 (0.177) | −0.119 | −0.048 (0.186) | −0.259 | 0.796 | 0.416 (0.260) | 1.599 | 0.110 | |
| PD | 0.150 (0.452) | 0.053 | 0.323 (0.446) | 0.115 | −0.234 (0.252) | −0.147 | 0.173 (0.265) | 0.653 | 0.514 | −0.558 (0.374) | −1.493 | 0.136 | |
| MF | −0.303 (0.331) | −0.145 | −0.294 (0.329) | −0.142 | −0.038 (0.189) | −0.032 | 0.008 (0.197) | 0.042 | 0.967 | 0.256 (0.281) | 0.912 | 0.362 | |
| PA | −0.094 (0.475) | −0.032 | −0.675 (0.459) | −0.229 | −0.275 (0.264) | −0.164 | −0.581 (0.264) | −2.198 | 0.028 | 0.400 (0.398) | 1.004 | 0.315 | |
| PT | −0.129 (0.434) | −0.048 | −0.444 (0.426) | −0.165 | 0.114 (0.244) | 0.075 | −0.314 (0.251) | −1.252 | 0.211 | 0.558 (0.358) | 1.559 | 0.119 | |
| SC | −0.386 (0.572) | −0.107 | −0.676 (0.561) | −0.189 | 0.024 (0.324) | 0.012 | −0.290 (0.336) | −0.864 | 0.388 | 0.700 (0.475) | 1.472 | 0.141 | |
| MA | 0.824 (0.402) | 0.312 | 0.447 (0.414) | 0.17 | −0.038 (0.239) | −0.026 | −0.377 (0.242) | −1.557 | 0.119 | −0.485 (0.351) | −1.383 | 0.167 | |
| SI | −0.281 (0.357) | −0.125 | −0.451 (0.350) | −0.202 | 0.106 (0.202) | 0.084 | −0.170 (0.211) | −0.809 | 0.419 | 0.557 (0.293) | 1.904 | 0.057 | |
| ANX | −0.969 (0.367) | −0.389 | −1.067 (0.357) | −0.431 | −0.193 (0.223) | −0.137 | −0.098 (0.234) | −0.419 | 0.676 | 0.874 (0.308) | 2.836 | 0.005 | |
| FRS | −0.626 (0.358) | −0.269 | −0.604 (0.356) | −0.262 | −0.274 (0.205) | −0.209 | 0.021 (0.219) | 0.098 | 0.922 | 0.331 (0.311) | 1.063 | 0.288 | |
| OBS | −1.014 (0.498) | −0.310 | −1.411 (0.469) | −0.434 | −0.192 (0.294) | −0.104 | −0.398 (0.302) | −1.316 | 0.188 | 1.219 (0.400) | 3.049 | 0.002 | |
| DEP | −0.623 (0.426) | −0.228 | −1.083 (0.398) | −0.399 | −0.246 (0.244) | −0.160 | −0.460 (0.247) | −1.862 | 0.063 | 0.837 (0.346) | 2.417 | 0.016 | |
| HEA | −0.349 (0.325) | −0.170 | −0.540 (0.315) | −0.264 | −0.349 (0.177) | −0.300 | −0.190 (0.192) | −0.993 | 0.321 | 0.191 (0.278) | 0.688 | 0.492 | |
| TRT | −0.603 (0.320) | −0.289 | −1.072 (0.283) | −0.518 | −0.384 (0.178) | −0.327 | −0.469 (0.182) | −2.581 | 0.010 | 0.688 (0.261) | 2.635 | 0.008 | |
| GIF | HS | −0.574 (0.273) | −0.319 | −0.390 (0.196) | −0.304 | −0.114 (0.109) | −0.165 | 0.184 (0.211) | 0.872 | 0.383 | 0.276 (0.185) | 1.494 | 0.135 |
| D | −0.550 (0.307) | −0.276 | −0.554 (0.210) | −0.389 | −0.089 (0.122) | −0.116 | −0.004 (0.236) | −0.015 | 0.988 | 0.465 (0.197) | 2.358 | 0.018 | |
| HY | −0.628 (0.269) | −0.350 | −0.531 (0.187) | −0.414 | −0.234 (0.104) | −0.340 | 0.097 (0.212) | 0.459 | 0.646 | 0.297 (0.184) | 1.619 | 0.105 | |
| PD | 0.470 (0.405) | 0.183 | 0.200 (0.292) | 0.109 | −0.128 (0.156) | −0.130 | −0.271 (0.301) | −0.900 | 0.368 | −0.327 (0.266) | −1.229 | 0.219 | |
| MF | −0.235 (0.302) | −0.124 | −0.114 (0.217) | −0.084 | 0.051 (0.116) | 0.07 | 0.122 (0.224) | 0.543 | 0.587 | 0.164 (0.199) | 0.825 | 0.409 | |
| PA | −0.038 (0.432) | −0.014 | −0.486 (0.299) | −0.252 | −0.197 (0.162) | −0.191 | −0.448 (0.311) | −1.440 | 0.150 | 0.289 (0.281) | 1.028 | 0.304 | |
| PT | −0.406 (0.390) | −0.164 | −0.392 (0.275) | −0.222 | −0.061 (0.151) | −0.065 | 0.014 (0.292) | 0.049 | 0.961 | 0.331 (0.255) | 1.295 | 0.195 | |
| SC | −0.582 (0.515) | −0.178 | −0.766 (0.353) | −0.328 | −0.099 (0.200) | −0.079 | −0.184 (0.385) | −0.477 | 0.633 | 0.667 (0.328) | 2.033 | 0.042 | |
| MA | 0.583 (0.374) | 0.243 | 0.181 (0.273) | 0.105 | 0.067 (0.147) | 0.073 | −0.402 (0.277) | −1.454 | 0.146 | −0.114 (0.253) | −0.449 | 0.653 | |
| SI | −0.412 (0.321) | −0.202 | −0.351 (0.227) | −0.240 | 0.100 (0.124) | 0.128 | 0.061 (0.242) | 0.254 | 0.799 | 0.451 (0.204) | 2.216 | 0.027 | |
| ANX | −0.920 (0.332) | −0.406 | −0.644 (0.238) | −0.398 | −0.238 (0.134) | −0.275 | 0.276 (0.264) | 1.044 | 0.296 | 0.406 (0.230) | 1.764 | 0.078 | |
| FRS | −0.591 (0.325) | −0.280 | −0.258 (0.238) | −0.171 | −0.091 (0.129) | −0.112 | 0.333 (0.244) | 1.363 | 0.173 | 0.167 (0.221) | 0.757 | 0.449 | |
| OBS | −1.079 (0.444) | −0.362 | −0.869 (0.311) | −0.409 | −0.175 (0.180) | −0.154 | 0.210 (0.350) | 0.601 | 0.548 | 0.693 (0.294) | 2.358 | 0.018 | |
| DEP | −0.767 (0.379) | −0.309 | −0.864 (0.248) | −0.487 | −0.289 (0.145) | −0.303 | −0.096 (0.293) | −0.328 | 0.743 | 0.575 (0.246) | 2.34 | 0.019 | |
| HEA | −0.495 (0.289) | −0.265 | −0.374 (0.205) | −0.280 | −0.170 (0.111) | −0.237 | 0.121 (0.220) | 0.551 | 0.581 | 0.204 (0.195) | 1.047 | 0.295 | |
| TRT | −0.752 (0.279) | −0.397 | −0.767 (0.179) | −0.567 | −0.165 (0.113) | −0.227 | −0.015 (0.224) | −0.066 | 0.947 | 0.602 (0.175) | 3.435 | 0.001 | |
| GSI | HS | 0.445 (0.226) | 0.300 | 0.183 (0.166) | 0.174 | 0.010 (0.101) | 0.016 | −0.262 (0.170) | −1.539 | 0.124 | −0.173 (0.109) | −1.583 | 0.113 |
| D | 0.337 (0.258) | 0.205 | 0.173 (0.185) | 0.148 | 0.024 (0.112) | 0.035 | −0.164 (0.193) | −0.850 | 0.395 | −0.149 (0.123) | −1.211 | 0.226 | |
| HY | 0.396 (0.228) | 0.268 | 0.188 (0.165) | 0.179 | 0.131 (0.099) | 0.208 | −0.208 (0.172) | −1.211 | 0.226 | −0.057 (0.110) | −0.508 | 0.611 | |
| PD | −0.572 (0.327) | −0.270 | −0.125 (0.240) | −0.083 | 0.031 (0.144) | 0.034 | 0.447 (0.240) | 1.862 | 0.063 | 0.156 (0.159) | 0.980 | 0.327 | |
| MF | 0.476 (0.239) | 0.303 | 0.245 (0.174) | 0.220 | 0.115 (0.105) | 0.172 | −0.230 (0.182) | −1.267 | 0.205 | −0.130 (0.117) | −1.110 | 0.267 | |
| PA | −0.072 (0.356) | −0.032 | 0.398 (0.245) | 0.252 | 0.250 (0.146) | 0.264 | 0.470 (0.252) | 1.864 | 0.062 | −0.148 (0.167) | −0.883 | 0.377 | |
| PT | 0.172 (0.325) | 0.085 | 0.042 (0.231) | 0.029 | −0.023 (0.139) | −0.026 | −0.130 (0.240) | −0.541 | 0.588 | −0.065 (0.154) | −0.422 | 0.673 | |
| SC | 0.352 (0.427) | 0.131 | 0.210 (0.304) | 0.110 | 0.032 (0.184) | 0.028 | −0.141 (0.318) | −0.445 | 0.656 | −0.179 (0.202) | −0.882 | 0.378 | |
| MA | −0.468 (0.308) | −0.236 | −0.165 (0.224) | −0.117 | −0.033 (0.135) | −0.039 | 0.304 (0.229) | 1.323 | 0.186 | 0.132 (0.149) | 0.887 | 0.375 | |
| SI | 0.101 (0.270) | 0.06 | 0.016 (0.192) | 0.013 | −0.183 (0.111) | −0.255 | −0.085 (0.199) | −0.428 | 0.669 | −0.199 (0.124) | −1.602 | 0.109 | |
| ANX | 0.686 (0.278) | 0.368 | 0.351 (0.205) | 0.265 | 0.141 (0.125) | 0.177 | −0.335 (0.214) | −1.564 | 0.118 | −0.210 (0.138) | −1.525 | 0.127 | |
| FRS | 0.491 (0.267) | 0.282 | 0.071 (0.197) | 0.058 | −0.033 (0.119) | −0.045 | −0.420 (0.195) | −2.156 | 0.031 | −0.104 (0.131) | −0.796 | 0.426 | |
| OBS | 0.885 (0.366) | 0.361 | 0.534 (0.265) | 0.307 | 0.096 (0.167) | 0.092 | −0.350 (0.285) | −1.230 | 0.219 | −0.438 (0.173) | −2.538 | 0.011 | |
| DEP | 0.639 (0.312) | 0.312 | 0.448 (0.221) | 0.308 | 0.175 (0.137) | 0.201 | −0.190 (0.240) | −0.792 | 0.428 | −0.273 (0.149) | −1.831 | 0.067 | |
| HEA | 0.410 (0.238) | 0.266 | 0.202 (0.172) | 0.184 | 0.063 (0.105) | 0.096 | −0.209 (0.179) | −1.163 | 0.245 | −0.139 (0.115) | −1.205 | 0.228 | |
| TRT | 0.730 (0.221) | 0.467 | 0.542 (0.155) | 0.489 | 0.171 (0.103) | 0.257 | −0.187 (0.182) | −1.027 | 0.305 | −0.371 (0.103) | −3.617 | 0.000 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Paolucci, T.; Saggino, A.; Agostini, F.; Paoloni, M.; Bernetti, A.; Mangone, M.; Santilli, V.; Saggini, R.; Tommasi, M. The Influence of Rehabilitation on Quality of Life in Breast Cancer Survivors: A Clinical Study. Int. J. Environ. Res. Public Health 2021, 18, 8585. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18168585
Paolucci T, Saggino A, Agostini F, Paoloni M, Bernetti A, Mangone M, Santilli V, Saggini R, Tommasi M. The Influence of Rehabilitation on Quality of Life in Breast Cancer Survivors: A Clinical Study. International Journal of Environmental Research and Public Health. 2021; 18(16):8585. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18168585
Chicago/Turabian StylePaolucci, Teresa, Aristide Saggino, Francesco Agostini, Marco Paoloni, Andrea Bernetti, Massimiliano Mangone, Valter Santilli, Raoul Saggini, and Marco Tommasi. 2021. "The Influence of Rehabilitation on Quality of Life in Breast Cancer Survivors: A Clinical Study" International Journal of Environmental Research and Public Health 18, no. 16: 8585. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18168585