
Association between Osteoporosis and Low Hemoglobin Levels: A Nested Case–Control Study Using a National Health Screening Cohort


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Definition of Osteoporosis
2.3. Hemoglobin Concentration
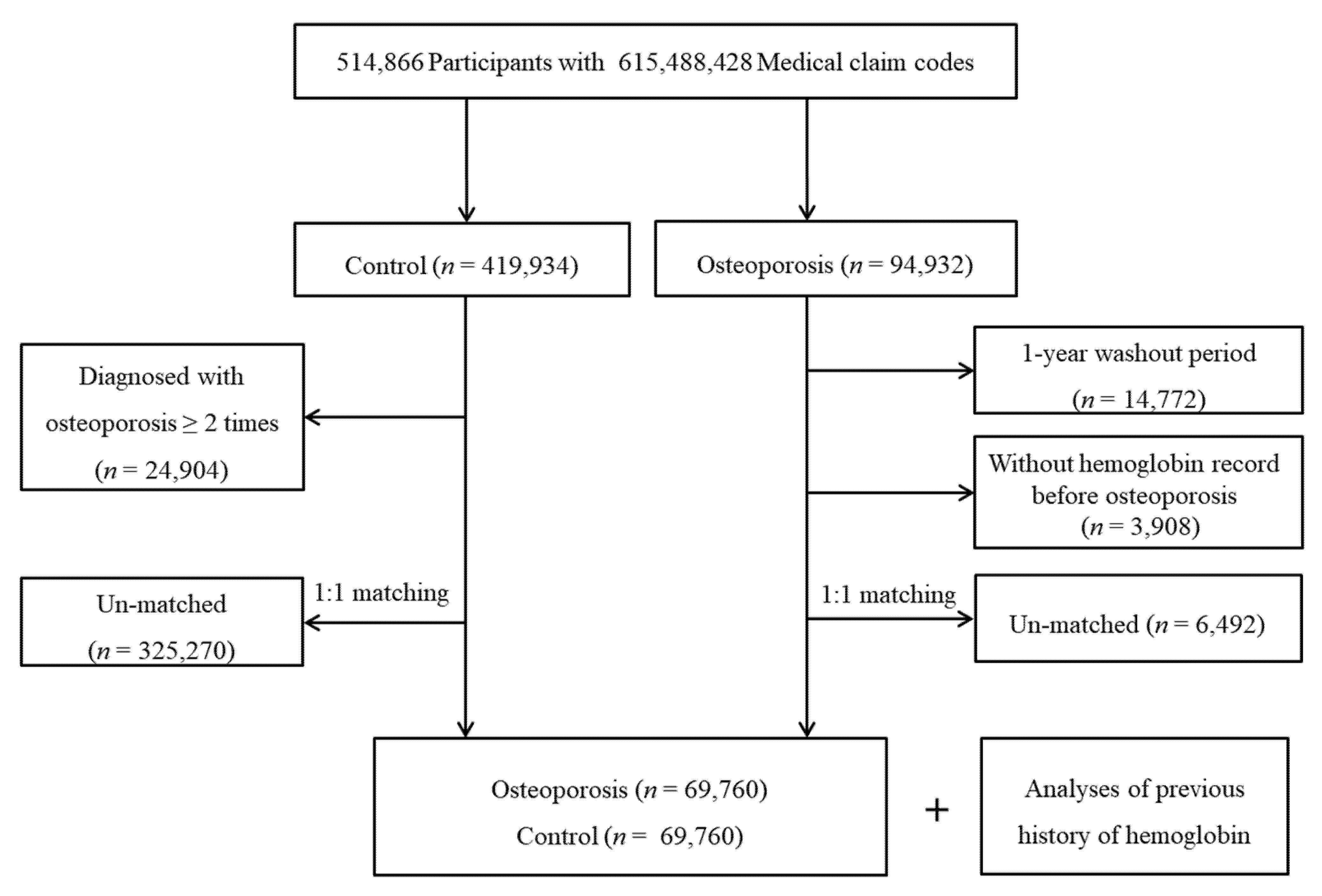
2.4. Participant Selection
2.5. Covariates
2.6. Statistical Analyses
2.7. Ethical Considerations
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Burge, R.; Dawson-Hughes, B.; Solomon, D.H.; Wong, J.B.; King, A.; Tosteson, A. Incidence and economic burden of osteoporosis-related fractures in the United States, 2005–2025. J. Bone Miner. Res. 2007, 22, 465–475. [Google Scholar] [CrossRef]
- Ray, N.F.; Chan, J.K.; Thamer, M.; Melton, L.J., 3rd. Medical expenditures for the treatment of osteoporotic fractures in the United States in 1995: Report from the National Osteoporosis Foundation. J. Bone Miner. Res. 1997, 12, 24–35. [Google Scholar] [CrossRef]
- Rachner, T.D.; Khosla, S.; Hofbauer, L.C. Osteoporosis: Now and the future. Lancet 2011, 377, 1276–1287. [Google Scholar] [CrossRef] [Green Version]
- Melton, L.J., III; Chrischilles, E.A.; Cooper, C.; Lane, A.W.; Riggs, B.L. Perspective: How many women have osteoporosis? J. Bone Miner. Res. 1992, 1992, 1005–1010. [Google Scholar] [CrossRef] [PubMed]
- Vujasinovic, M.; Nezirevic Dobrijevic, L.; Asplund, E.; Rutkowski, W.; Dugic, A.; Kahn, M.; Dahlman, I.; Saaf, M.; Hagstrom, H.; Lohr, J.M. Low Bone Mineral Density and Risk for Osteoporotic Fractures in Patients with Chronic Pancreatitis. Nutrients 2021, 13, 2386. [Google Scholar] [CrossRef] [PubMed]
- Du, X.; Zhang, C.; Zhang, X.; Qi, Z.; Cheng, S.; Le, S. The Impact of Nordic Walking on Bone Properties in Postmenopausal Women with Pre-Diabetes and Non-Alcohol Fatty Liver Disease. Int. J. Environ. Res. Public Health 2021, 18, 7570. [Google Scholar] [CrossRef] [PubMed]
- Bocker, W.; Doobare, I.U.; Khachatryan, A.; Dornstauder, E.; Bartsch, R.; Worth, G.; Singh, M.; Kahangire, D.A. Fractures in untreated patients with osteoporosis in Germany: An InGef healthcare insurance database analysis. Osteoporos. Int. 2021. [Google Scholar] [CrossRef]
- Toxqui, L.; Vaquero, M.P. Chronic iron deficiency as an emerging risk factor for osteoporosis: A hypothesis. Nutrients 2015, 7, 2324–2344. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.K.; Kang, H.S.; Kim, C.S.; Kim, Y.T. The prevalence of anemia and iron depletion in the population aged 10 years or older. Korean J. Hematol. 2011, 46, 196–199. [Google Scholar] [CrossRef] [Green Version]
- DeLoughery, T.G. Microcytic anemia. N. Engl. J. Med. 2014, 371, 1324–1331. [Google Scholar] [CrossRef] [PubMed]
- Lanier, J.B.; Park, J.J.; Callahan, R.C. Anemia in Older Adults. Am. Fam. Physician 2018, 98, 437–442. [Google Scholar]
- Pan, M.L.; Chen, L.R.; Tsao, H.M.; Chen, K.H. Iron Deficiency Anemia as a Risk Factor for Osteoporosis in Taiwan: A Nationwide Population-Based Study. Nutrients 2017, 9, 616. [Google Scholar] [CrossRef] [PubMed]
- Piccin, A.; Murphy, C.; Eakins, E.; Rondinelli, M.B.; Daves, M.; Vecchiato, C.; Wolf, D.; Mc Mahon, C.; Smith, O.P. Insight into the complex pathophysiology of sickle cell anaemia and possible treatment. Eur. J. Haematol. 2019, 102, 319–330. [Google Scholar] [CrossRef] [PubMed]
- Gaudio, A.; Morabito, N.; Catalano, A.; Rapisarda, R.; Xourafa, A.; Lasco, A. Pathogenesis of Thalassemia Major-associated Osteoporosis: A Review with Insights from Clinical Experience. J. Clin. Res. Pediatr. Endocrinol. 2019, 11, 110–117. [Google Scholar] [CrossRef] [PubMed]
- Korkmaz, U.; Korkmaz, N.; Yazici, S.; Erkan, M.; Baki, A.E.; Yazici, M.; Ozhan, H.; Ataoglu, S. Anemia as a risk factor for low bone mineral density in postmenopausal Turkish women. Eur. J. Intern. Med. 2012, 23, 154–158. [Google Scholar] [CrossRef]
- Oh, Y.H.; Moon, J.H.; Cho, B. Association between Hemoglobin Level and Bone Mineral Density in Korean Adults. J. Bone Metab. 2017, 24, 161–173. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.Y.; Min, C.; Oh, D.J.; Choi, H.G. Tobacco Smoking and Alcohol Consumption Are Related to Benign Parotid Tumor: A Nested Case-Control Study Using a National Health Screening Cohort. Clin. Exp. Otorhinolaryngol. 2019, 12, 412–419. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.Y.; Kong, I.G.; Lim, H.; Choi, H.G. Increased Risk of Sudden Sensory Neural Hearing Loss in Osteoporosis: A Longitudinal Follow-Up Study. J. Clin. Endocrinol. Metab. 2018, 103, 3103–3109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, S.Y.; Min, C.; Yoo, D.M.; Chang, J.; Lee, H.J.; Park, B.; Choi, H.G. Hearing impairment increases economic inequality. Clin. Exp. Otorhinolaryngol. 2021. [Google Scholar] [CrossRef] [PubMed]
- WHO; IASO; IOTR. The Asia-Pacific Perespective: Redefining Obesity and Its Treatment; Health Communications Australia Pty Ltd.: Balmain, Australia, 2000. [Google Scholar]
- Quan, H.; Li, B.; Couris, C.M.; Fushimi, K.; Graham, P.; Hider, P.; Januel, J.M.; Sundararajan, V. Updating and validating the Charlson comorbidity index and score for risk adjustment in hospital discharge abstracts using data from 6 countries. Am. J. Epidemiol. 2011, 173, 676–682. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.; Cho, S.M.J.; Park, J.H.; Park, S.; Kim, H.C. 2017 ACC/AHA Blood Pressure Classification and Cardiovascular Disease in 15 Million Adults of Age 20–94 Years. J. Clin. Med. 2019, 8, 1832. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, S.Y.; Song, Y.S.; Wee, J.H.; Min, C.; Yoo, D.M.; Choi, H.G. Association between SSNHL and Thyroid Diseases. Int. J. Environ. Res. Public Health 2020, 17, 8419. [Google Scholar] [CrossRef]
- Kim, S.Y.; Wee, J.H.; Min, C.; Yoo, D.M.; Choi, H.G. Relationship between Bell's Palsy and Previous Statin Use: A Case/Non-Case Study. Int. J. Environ. Res. Public Health 2020, 17, 8408. [Google Scholar] [CrossRef]
- Laudisio, A.; Marzetti, E.; Pagano, F.; Bernabei, R.; Zuccala, G. Haemoglobin levels are associated with bone mineral density in the elderly: A population-based study. Clin. Rheumatol. 2009, 28, 145–151. [Google Scholar] [CrossRef]
- Gurevitch, O.; Slavin, S. The hematological etiology of osteoporosis. Med. Hypotheses 2006, 67, 729–735. [Google Scholar] [CrossRef]
- Fujimoto, H.; Fujimoto, K.; Ueda, A.; Ohata, M. Hypoxemia is a risk factor for bone mass loss. J. Bone Miner. Metab. 1999, 17, 211–216. [Google Scholar] [CrossRef]
- Karadag, F.; Cildag, O.; Yurekli, Y.; Gurgey, O. Should COPD patients be routinely evaluated for bone mineral density? J. Bone Miner. Metab. 2003, 21, 242–246. [Google Scholar] [CrossRef] [PubMed]
- Upala, S.; Sanguankeo, A.; Congrete, S. Association Between Obstructive Sleep Apnea and Osteoporosis: A Systematic Review and Meta-Analysis. Int. J. Endocrinol. Metab. 2016, 14, e36317. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laudisio, A.; Marzetti, E.; Antonica, L.; Cocchi, A.; Bernabei, R.; Zuccala, G. Association of left ventricular function with bone mineral density in older women: A population-based study. Calcif. Tissue Int. 2008, 82, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Leng, S.; Chaves, P.; Koenig, K.; Walston, J. Serum interleukin-6 and hemoglobin as physiological correlates in the geriatric syndrome of frailty: A pilot study. J. Am. Geriatr. Soc. 2002, 50, 1268–1271. [Google Scholar] [CrossRef] [PubMed]
- Rutten, E.P.; Franssen, F.M.; Spruit, M.A.; Wouters, E.F. Anemia is associated with bone mineral density in chronic obstructive pulmonary disease. COPD 2013, 10, 286–292. [Google Scholar] [CrossRef] [PubMed]
- Taal, M.W.; Masud, T.; Green, D.; Cassidy, M.J. Risk factors for reduced bone density in haemodialysis patients. Nephrol. Dial. Transplant. 1999, 14, 1922–1928. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Characteristics | Total Participants | |||
|---|---|---|---|---|
| Osteoporosis (n, %) | Control (n, %) | p-Value | ||
| Age (years old) | 1.000 | |||
| 40–44 | 728 (1.0) | 728 (1.0) | ||
| 45–49 | 4110 (5.9) | 4110 (5.9) | ||
| 50–54 | 9401 (13.5) | 9401 (13.5) | ||
| 55–59 | 10,982 (15.7) | 10,982 (15.7) | ||
| 60–64 | 12,559 (18.0) | 12,559 (18.0) | ||
| 65–69 | 15,698 (22.5) | 15,698 (22.5) | ||
| 70–74 | 8874 (12.7) | 8874 (12.7) | ||
| 75–79 | 5021 (7.2) | 5021 (7.2) | ||
| 80–84 | 2006 (2.9) | 2006 (2.9) | ||
| 85+ | 381 (0.6) | 381 (0.6) | ||
| Sex | 1.000 | |||
| Male | 9231 (13.2) | 9231 (13.2) | ||
| Female | 60,529 (86.8) | 60,529 (86.8) | ||
| Income | 1.000 | |||
| 1 (lowest) | 13,281 (19.0) | 13,281 (19.0) | ||
| 2 | 10,196 (14.6) | 10,196 (14.6) | ||
| 3 | 11,067 (15.9) | 11,067 (15.9) | ||
| 4 | 14,217 (20.4) | 14,217 (20.4) | ||
| 5 (highest) | 20,999 (30.1) | 20,999 (30.1) | ||
| Region of residence | 1.000 | |||
| Urban | 28,090 (40.3) | 28,090 (40.3) | ||
| Rural | 41,670 (59.7) | 41,670 (59.7) | ||
| Obesity † | <0.001 * | |||
| Underweight | 2282 (3.3) | 1687 (2.4) | ||
| Normal | 26,402 (37.9) | 23,210 (33.3) | ||
| Overweight | 18,257 (26.2) | 18,175 (26.1) | ||
| Obese I | 20,749 (29.7) | 23,565 (33.8) | ||
| Obese II | 2070 (3.0) | 3123 (4.5) | ||
| Smoking status | <0.001 * | |||
| Nonsmoker | 63,724 (91.4) | 63,273 (90.7) | ||
| Past smoker | 2449 (3.5) | 2454 (3.5) | ||
| Current smoker | 3587 (5.1) | 4033 (5.8) | ||
| Alcohol consumption | <0.001 * | |||
| <1 time a week | 61,462 (88.1) | 61,021 (87.5) | ||
| ≥1 time a week | 8298 (11.9) | 8739 (12.5) | ||
| Systolic blood pressure | <0.001 * | |||
| <120 mmHg | 21,374 (30.6) | 19,277 (27.6) | ||
| 120–139 mmHg | 31,510 (45.2) | 30,978 (44.4) | ||
| ≥140 mmHg | 16,876 (24.2) | 19,505 (28.0) | ||
| Diastolic blood pressure | <0.001 * | |||
| <80 mmHg | 33,298 (47.7) | 30,735 (44.1) | ||
| 80–89 mmHg | 23,626 (33.9) | 24,121 (34.6) | ||
| ≥90 mmHg | 12,836 (18.4) | 14,904 (21.4) | ||
| Fasting blood glucose | <0.001 * | |||
| <100 mg/dL | 48,016 (68.8) | 44,884 (64.3) | ||
| 100–125 mg/dL | 16,988 (24.4) | 18,004 (25.8) | ||
| ≥126 mg/dL | 4756 (6.8) | 6872 (9.9) | ||
| Total cholesterol | <0.001 * | |||
| <200 mg/dL | 33,337 (47.8) | 32,716 (46.9) | ||
| 200–239 mg/dL | 24,819 (35.6) | 24,575 (35.2) | ||
| ≥240 mg/dL | 11,604 (16.6) | 12,469 (17.9) | ||
| CCI score | ||||
| 0 | 43,316 (62.1) | 45,502 (65.2) | <0.001 * | |
| 1 | 11,832 (17.0) | 10,305 (14.8) | ||
| 2 | 6697 (9.6) | 5890 (8.4) | ||
| 3 | 3500 (5.0) | 3229 (4.6) | ||
| ≥4 | 4415 (6.3) | 4834 (6.9) | ||
| Anemia severity ‡ | <0.001 * | |||
| Normal | 59,197 (84.9) | 59,878 (85.8) | ||
| Mild | 8256 (11.8) | 7508 (10.8) | ||
| Moderate | 2223 (3.2) | 2249 (3.2) | ||
| Severe | 84 (0.1) | 125 (0.2) | ||
| Characteristics | Odds Ratios for Osteoporosis | ||||
|---|---|---|---|---|---|
| Crude † | p-Value | Adjusted †,‡ | p-Value | ||
| Total participants (n = 139,520) | |||||
| Hemoglobin | 0.96 (0.95–0.97) | <0.001 * | 0.98 (0.97–0.99) | <0.001 * | |
| Age < 65 years old, men (n = 4588) | |||||
| Hemoglobin | 0.82 (0.78–0.87) | <0.001 * | 0.87 (0.83–0.92) | <0.001 * | |
| Age < 65 years old, women (n = 70,972) | |||||
| Hemoglobin | 0.98 (0.97–0.99) | 0.002 * | 1.01 (0.99–1.02) | 0.355 | |
| Age ≥ 65 years old, men (n = 13,874) | |||||
| Hemoglobin | 0.91 (0.89–0.94) | <0.001 * | 0.94 (0.92–0.97) | <0.001 * | |
| Age ≥ 65 years old, women (n = 50,086) | |||||
| Hemoglobin | 0.96 (0.94–0.97) | <0.001 * | 0.98 (0.96–0.99) | 0.011 * | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, S.-Y.; Yoo, D.-M.; Min, C.; Choi, H.-G. Association between Osteoporosis and Low Hemoglobin Levels: A Nested Case–Control Study Using a National Health Screening Cohort. Int. J. Environ. Res. Public Health 2021, 18, 8598. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18168598
Kim S-Y, Yoo D-M, Min C, Choi H-G. Association between Osteoporosis and Low Hemoglobin Levels: A Nested Case–Control Study Using a National Health Screening Cohort. International Journal of Environmental Research and Public Health. 2021; 18(16):8598. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18168598
Chicago/Turabian StyleKim, So-Young, Dae-Myoung Yoo, Chanyang Min, and Hyo-Geun Choi. 2021. "Association between Osteoporosis and Low Hemoglobin Levels: A Nested Case–Control Study Using a National Health Screening Cohort" International Journal of Environmental Research and Public Health 18, no. 16: 8598. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18168598