
Effects of Financial Expenditure of Prefectures/Municipalities on Regional Suicide Mortality in Japan


Abstract
:1. Introduction
2. Materials and Methods
2.1. Dependent Variables
2.2. Independent and Dependent Variables
2.3. Statistical Analysis
3. Results
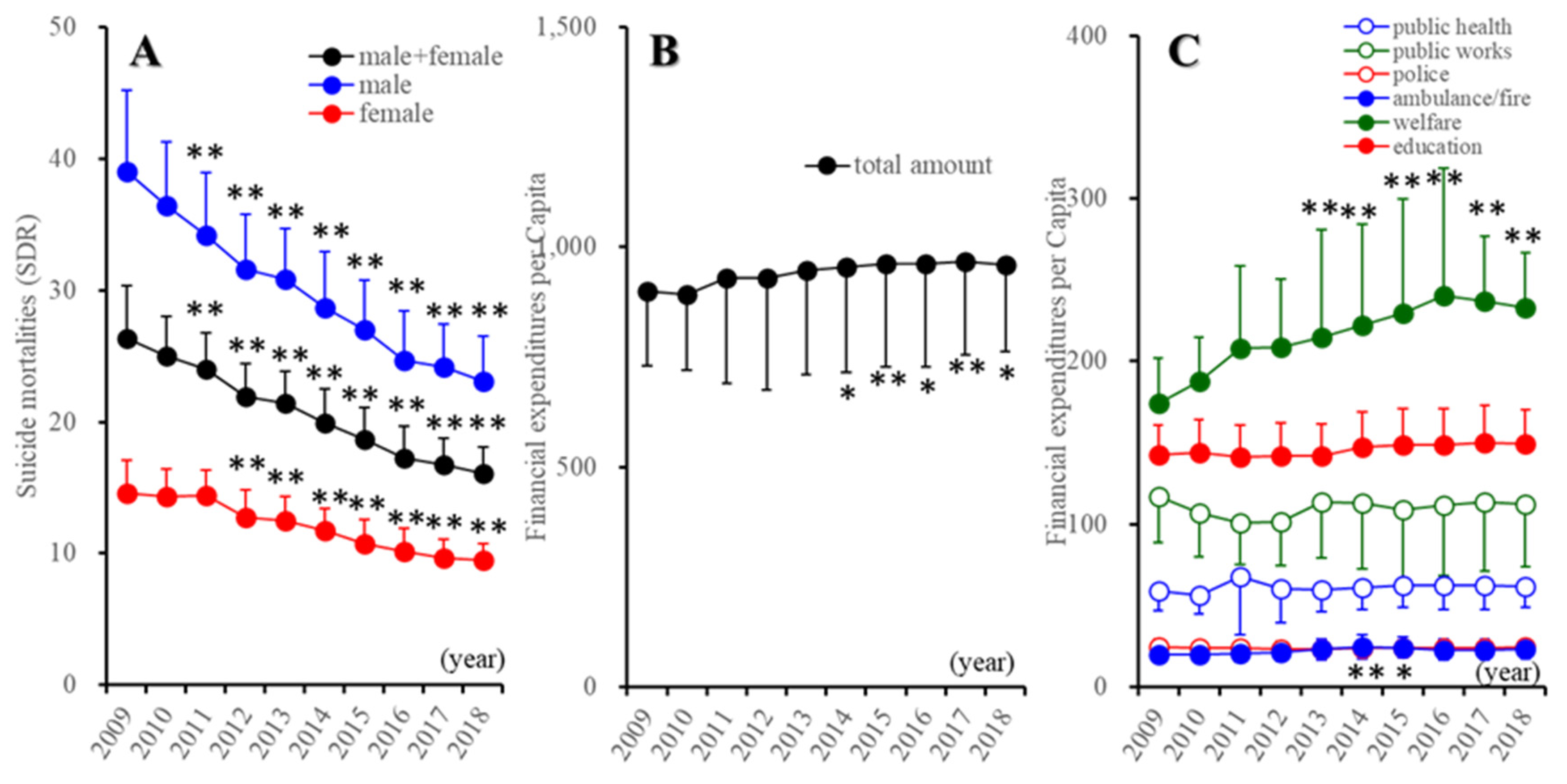
3.1. Trends of Suicide Mortality and Regional Financial Expenditure in Japan between 2009 and 2018
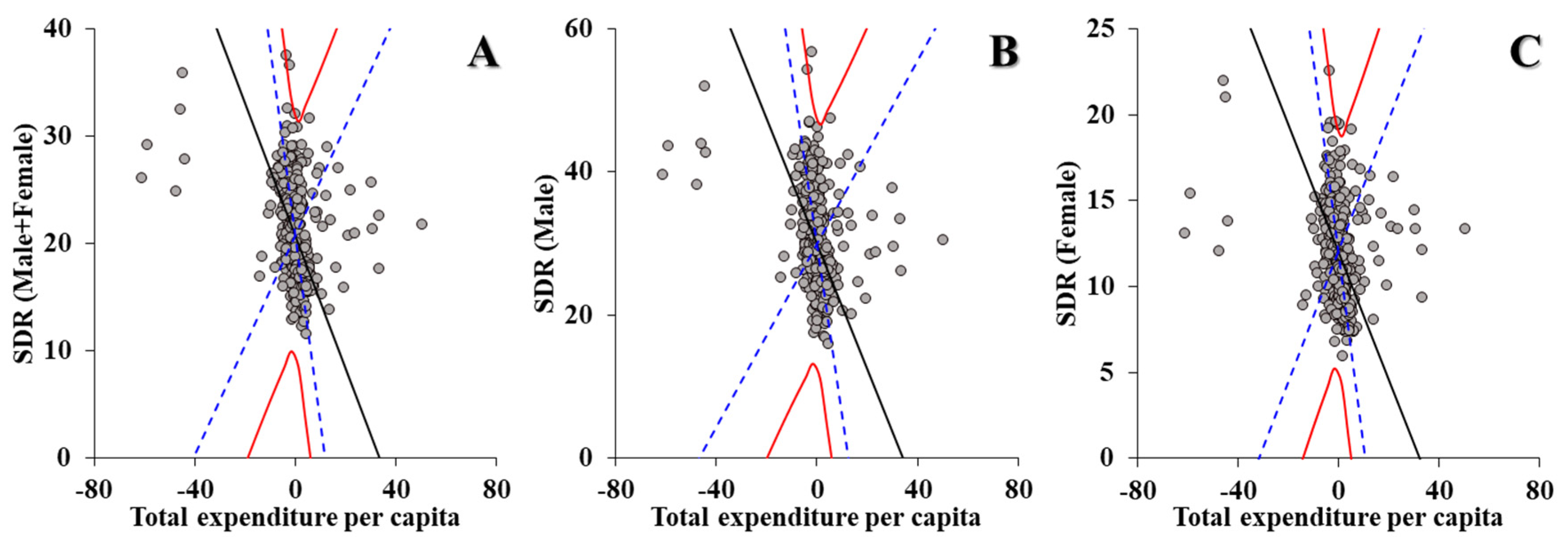
3.2. Effects of Total Amount of Financial Expenditure per Capita of Prefectures and Municipalities on Suicide Mortality
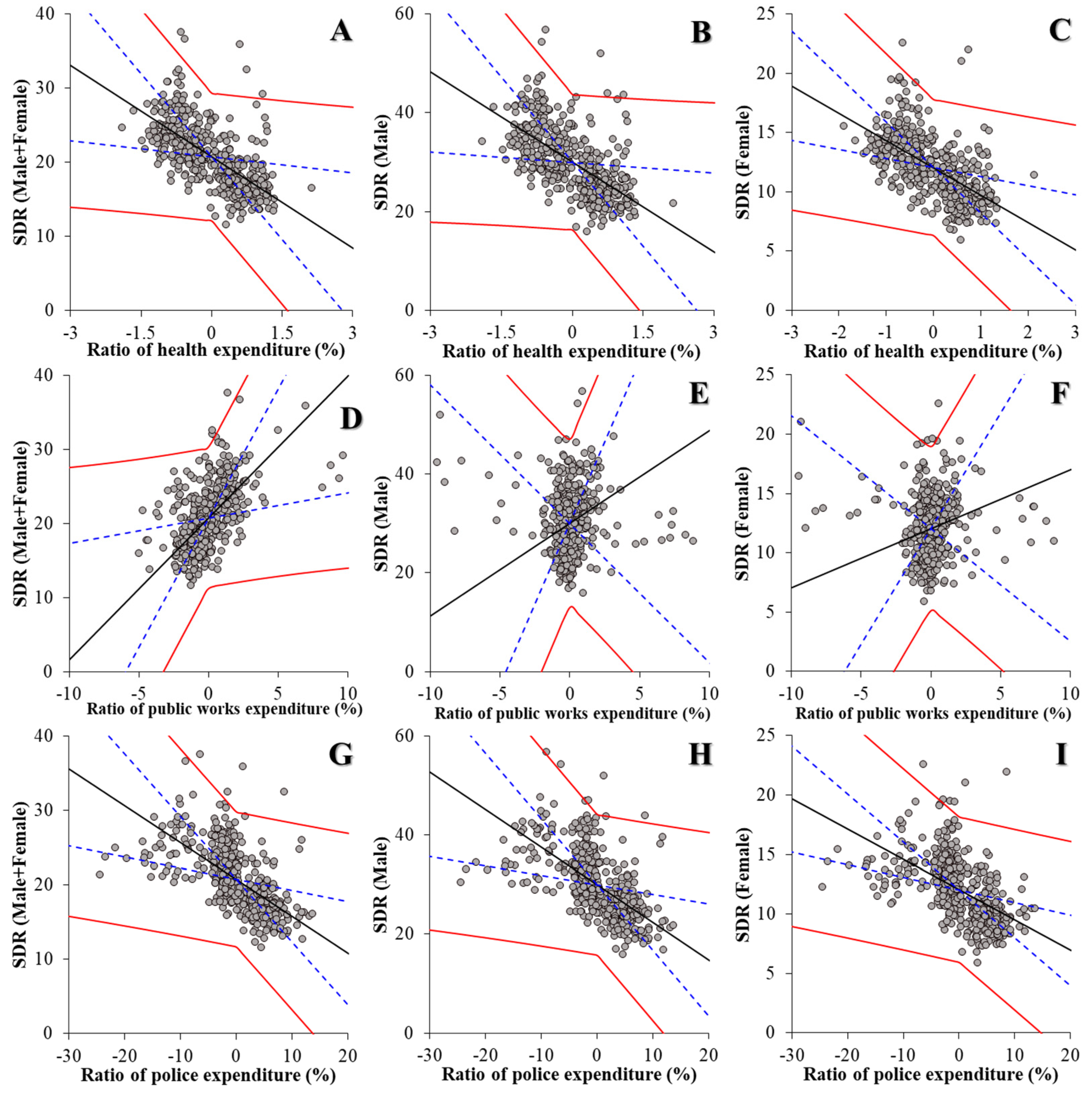
3.3. Effects of Relative Ratios of Financial Expenditure of Six Divisions of Prefectures and Municipalities on Suicide Mortality (Model 1)
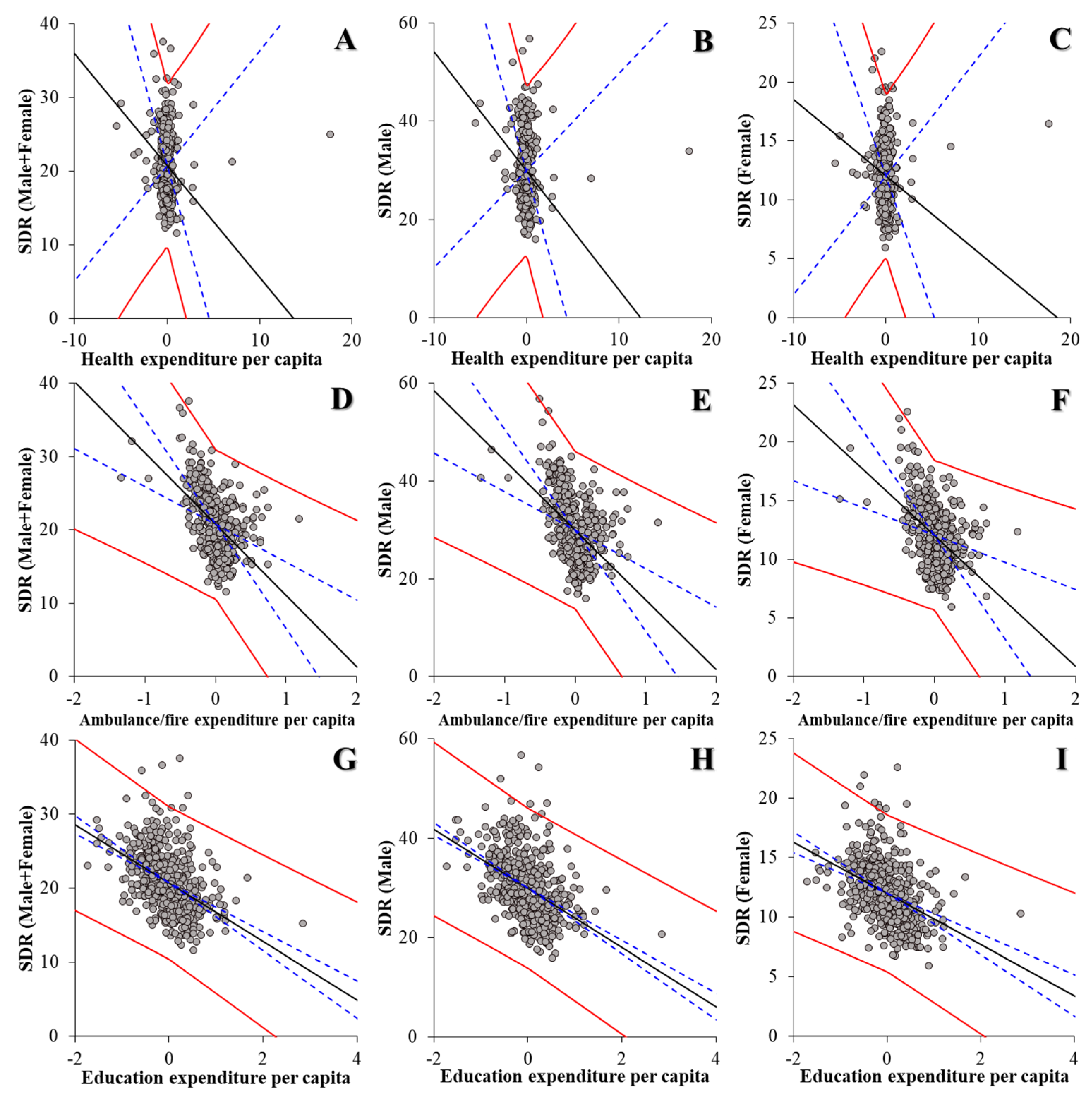
3.4. Effects of Financial Expenditure per Capita of Divisions and Subdivisions of Prefectures and Municipalities on Suicide Mortality
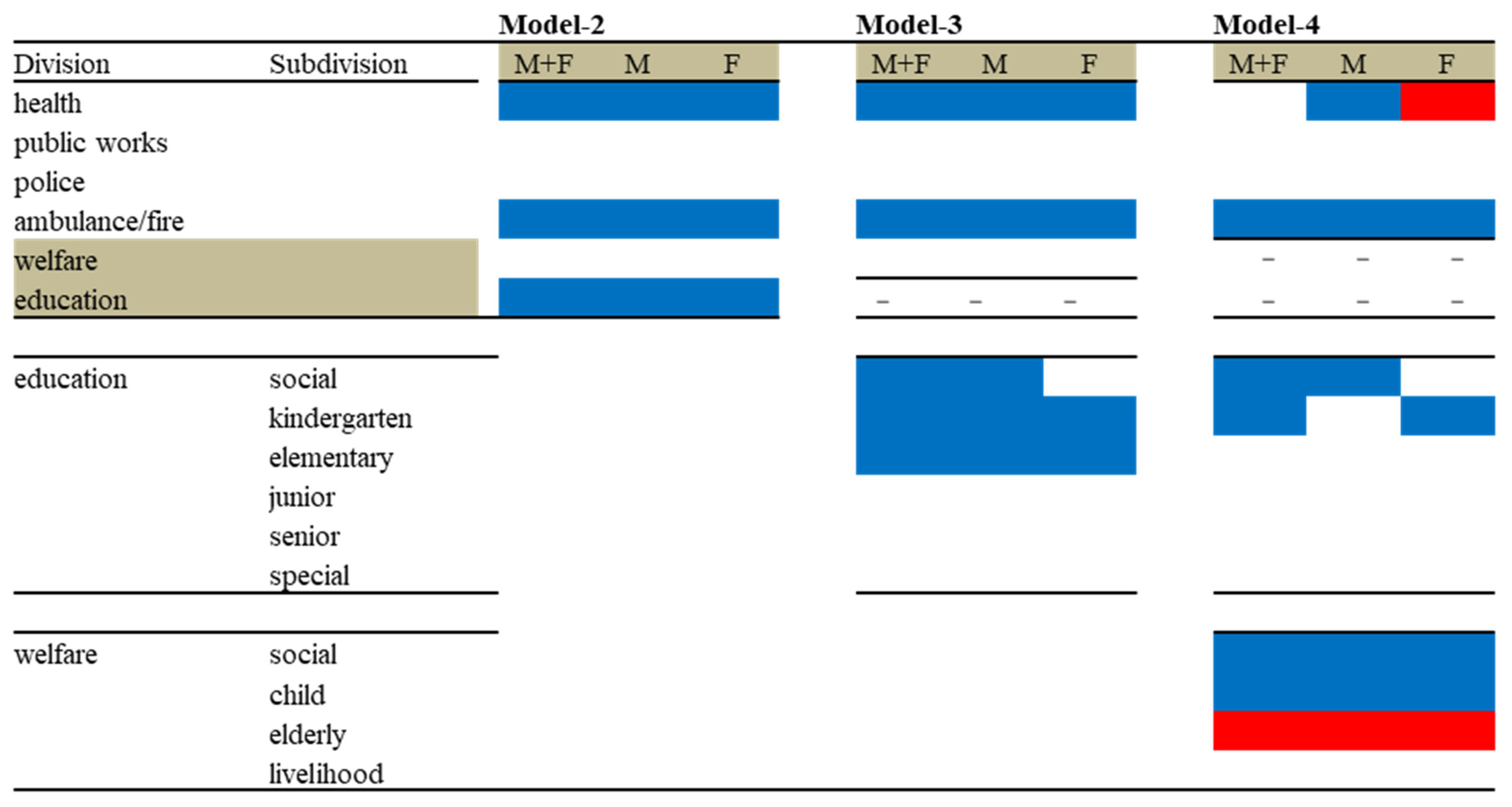
3.4.1. Effects of Regional Financial Expenditure per Capita of Six Divisions of Prefectures and Municipalities on Suicide Mortality (Model 2)
3.4.2. Effects of Regional Financial Expenditure per Capita of Divisions and Education Subdivisions on Suicide Mortality (Model 3)
3.4.3. Effects of Regional Financial Expenditure per Capita of Divisions and Subdivisions of Education and Welfare on Suicide Mortality (Model 4)
3.5. Effects of Financial Expenditure of Divisions and Subdivisions per Capita of Education and Welfare on Suicide Mortality Disagregated by Age
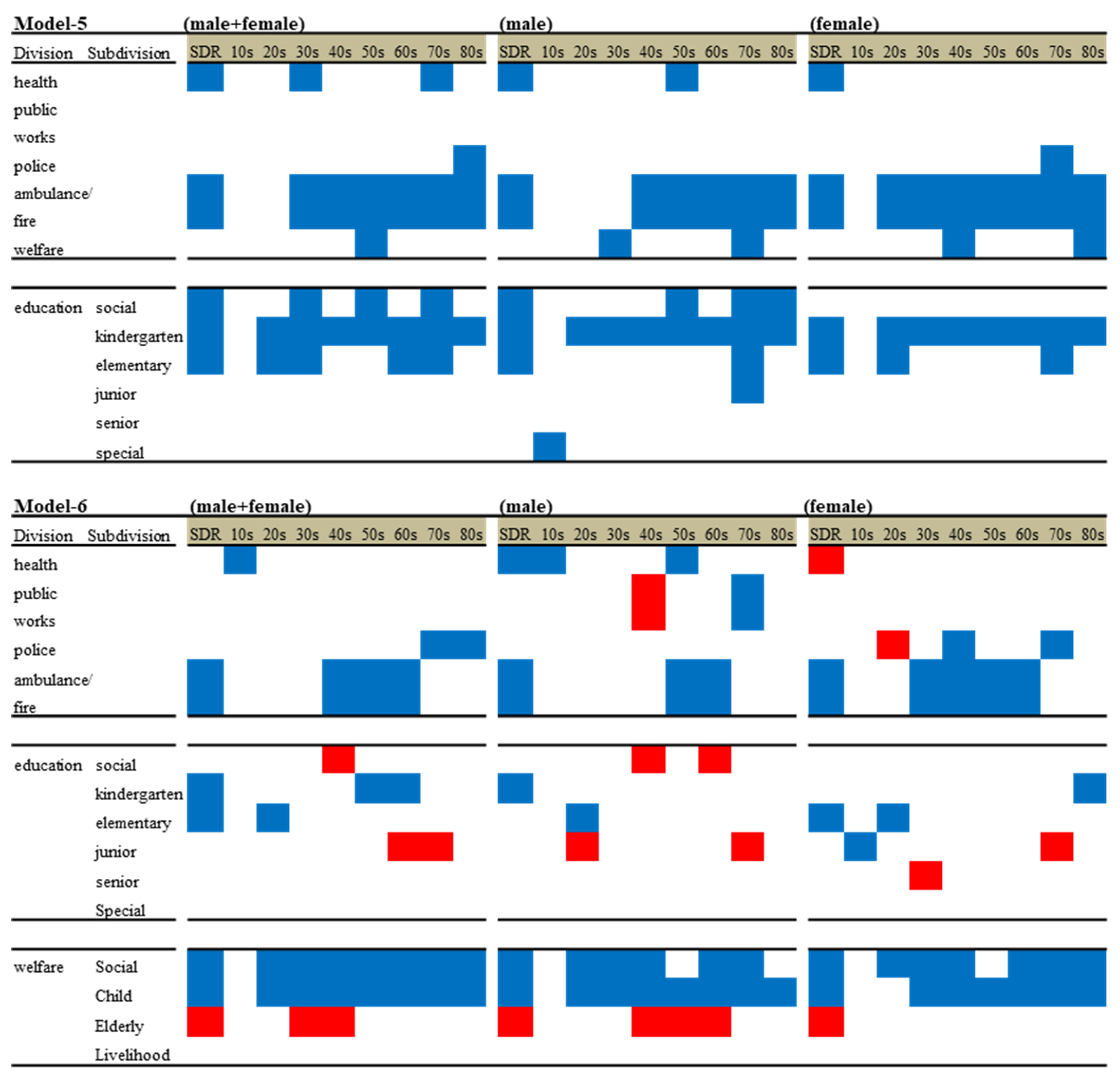
3.5.1. Effects of Regional Financial Expenditure of Divisions and Subdivisions of Education per Capita on Suicide Mortality Disaggregated by Age (Model 5)
3.5.2. Effects of Regional Financial Expenditure of Divisions and Subdivisions of Education and Welfare on Suicide Mortality Disaggregated by Ages and Genders (Model 6)
4. Discussion
4.1. Effects of Regional Governmental Expenditure on Suicide Mortality Disaggregated by Gender
4.2. Effects of Regional Governmental Expenditure on Suicide Mortality Disaggregated by Gender and Age
4.3. Limitations and Future Developments
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Suicide Data. Available online: https://www.who.int/mental_health/prevention/suicide/countrydata/en/ (accessed on 1 December 2019).
- World Health Organization. Suicide: One Person Dies Every 40 Seconds. Available online: https://www.who.int/news/item/09-09-2019-suicide-one-person-dies-every-40-seconds (accessed on 18 November 2020).
- World Health Organization. Preventing Suicide: A Resource for Pesticide Registrars and Regulators. Available online: https://www.who.int/publications/i/item/9789241516389 (accessed on 18 November 2020).
- World Health Organization. Preventing Suicide: A Global Imperative. Available online: https://www.who.int/publications/i/item/preventing-suicide-a-global-imperative (accessed on 18 November 2020).
- World Health Organization. PREVENTING SUICIDE: A Resource for Filmmakers and Others Working on Stage and Screen. Available online: https://www.who.int/publications/i/item/preventing-suicide-a-resource-for-filmmakers-and-others-working-on-stage-and-screen (accessed on 18 November 2020).
- Kato, R.; Okada, M. Can financial support reduce suicide mortality rates? Int. J. Environ. Res. Public Health 2019, 16, 4797. [Google Scholar] [CrossRef] [Green Version]
- Kino, S.; Jang, S.N.; Gero, K.; Kato, S.; Kawachi, I. Age, period, cohort trends of suicide in Japan and Korea (1986–2015): A tale of two countries. Soc. Sci. Med. 2019, 235, 112385. [Google Scholar] [CrossRef]
- Nakamoto, M.; Nakagawa, T.; Murata, M.; Okada, M. Impacts of dual-income household rate on suicide mortalities in Japan. Int. J. Environ. Res. Public Health 2021, 18, 5670. [Google Scholar] [CrossRef]
- Nakano, T.; Hasegawa, T.; Okada, M. Analysing the impacts of financial support for regional suicide prevention programmes on suicide mortality caused by major suicide motives in Japan using statistical government data. Int. J. Environ. Res. Public Health 2021, 18, 3414. [Google Scholar] [CrossRef]
- Ministry of Health, Labour and Welfare. 2020 White Paper on Suicide Prevention. Available online: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/hukushi_kaigo/seikatsuhogo/jisatsu/jisatsuhakusyo2020.html (accessed on 1 June 2021).
- Ministry of Health, Labour and Welfare. Basic Data on Suicide in the Region. Available online: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/0000140901.html (accessed on 1 June 2021).
- Okada, M.; Hasegawa, T.; Kato, R.; Shiroyama, T. Analysing regional unemployment rates, GDP per capita and financial support for regional suicide prevention programme on suicide mortality in Japan using governmental statistical data. BMJ Open 2020, 10, e037537. [Google Scholar] [CrossRef] [PubMed]
- Orsolini, L.; Latini, R.; Pompili, M.; Serafini, G.; Volpe, U.; Vellante, F.; Fornaro, M.; Valchera, A.; Tomasetti, C.; Fraticelli, S.; et al. Understanding the complex of suicide in depression: From research to clinics. Psychiatry Investig. 2020, 17, 207–221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ministry of Health, Labour and Welfare. Survey Study on the Actual Conditions of Young Carers. Available online: https://elaws.e-gov.go.jp/search/elawsSearch/elaws_search/lsg0500/detail?lawId=501AC1000000032_20190912_000000000000000&openerCode=1 (accessed on 1 May 2021).
- Ministry of Health, Labour and Welfare. Calling Attention when Reporting on Celebrity Suicide. Available online: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/hukushi_kaigo/seikatsuhogo/jisatsu/who_tebiki.html (accessed on 1 June 2021).
- World Health Organization. Preventing Suicide: A Resource for Media Professionals—update 2017. Available online: https://www.who.int/mental_health/suicide-prevention/resource_booklet_2017/en/ (accessed on 1 December 2019).
- Fushimi, M. Increase in youth suicides during the COVID-19 pandemic: Concerns over implications for the future. Psychol. Med. 2021, 1–2. [Google Scholar] [CrossRef]
- Ministry of Health, Labour and Welfare. Grant for Enhance Community-Based Suicide Countermeasures. Available online: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/hukushi_kaigo/seikatsuhogo/jisatsu/tiikijisatsutaisakukyokazigyo.html (accessed on 1 June 2021).
- You, B.S.; Jeong, K.H.; Cho, H.J. Regional suicide rate change patterns in Korea. Int. J. Environ. Res. Public Health 2020, 17, 5670. [Google Scholar] [CrossRef]
- Reeves, A.; McKee, M.; Stuckler, D. Economic suicides in the Great Recession in Europe and North America. Br. J. Psychiatry 2014, 205, 246–247. [Google Scholar] [CrossRef] [Green Version]
- Mattei, G.; Pistoresi, B. Unemployment and suicide in Italy: Evidence of a long-run association mitigated by public unemployment spending. Eur. J. Health Econ. 2019, 20, 569–577. [Google Scholar] [CrossRef]
- Mattei, G.; Pistoresi, B.; De Vogli, R. Impact of the economic crises on suicide in Italy: The moderating role of active labor market programs. Soc. Psychiatry Psychiatr. Epidemiol. 2019, 54, 201–208. [Google Scholar] [CrossRef]
- Toffolutti, V.; Suhrcke, M. Does austerity really kill? Econ. Hum. Biol. 2019, 33, 211–223. [Google Scholar] [CrossRef]
- Rambotti, S. Is there a relationship between welfare-state policies and suicide rates? Evidence from the U.S. states, 2000–2015. Soc. Sci. Med. 2020, 246, 112778. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barr, B.; Taylor-Robinson, D.; Scott-Samuel, A.; McKee, M.; Stuckler, D. Suicides associated with the 2008–10 economic recession in England: Time trend analysis. BMJ 2012, 345, e5142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barr, B.; Kinderman, P.; Whitehead, M. Trends in mental health inequalities in England during a period of recession, austerity and welfare reform 2004 to 2013. Soc. Sci. Med. 2015, 147, 324–331. [Google Scholar] [CrossRef] [PubMed]
- Biddle, L.; Brock, A.; Brookes, S.T.; Gunnell, D.J.b. Suicide rates in young men in England and Wales in the 21st century: Time trend study. BMJ 2008, 336, 539–542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Statistics Bureau of the Ministry of Internal Affairs and Communications (SBMIAC). Surveys of Population, Population Change and the Number of Households Based on the Basic Resident Registration. Available online: https://www.e-stat.go.jp/stat-search/files?page=1&toukei=00200241&tstat=000001039591 (accessed on 1 May 2021).
- Kawaguchi, H.; Koike, S. Association between the density of physicians and suicide rates in Japan: Nationwide ecological study using a spatial Bayesian model. PLoS ONE 2016, 11, e0148288. [Google Scholar] [CrossRef]
- Ministry of Internal Affairs and Communications. White Paper on Local Public Finance. Available online: https://www.soumu.go.jp/menu_seisaku/hakusyo/chihou/r03data/index.html (accessed on 1 May 2021).
- Ministry of Internal Affairs and Communications. Survey of Local Public Finance Settlement. Available online: https://www.e-stat.go.jp/stat-search/files?page=1&toukei=00200251&tstat=000001077755 (accessed on 1 May 2021).
- Okada, M.; Matsumoto, R.; Yamamoto, Y.; Fukuyama, K. Effects of subchronic administrations of Vortioxetine, Lurasidone, and Escitalopram on thalamocortical glutamatergic transmission associated with serotonin 5-HT7 receptor. Int. J. Mol. Sci. 2021, 22, 1351. [Google Scholar] [CrossRef] [PubMed]
- Okada, M.; Fukuyama, K.; Shiroyama, T.; Ueda, Y. Brivaracetam prevents astroglial l-glutamate release associated with hemichannel through modulation of synaptic vesicle protein. Biomed. Pharmacother. 2021, 138, 111462. [Google Scholar] [CrossRef] [PubMed]
- Fukuyama, K.; Okada, M. Effects of atypical antipsychotics, Clozapine, Quetiapine and Brexpiprazole on Astroglial transmission associated with Connexin43. Int. J. Mol. Sci. 2021, 22, 5623. [Google Scholar] [CrossRef]
- Fukuyama, K.; Nakano, T.; Shiroyama, T.; Okada, M. Chronic administrations of Guanfacine on mesocortical catecholaminergic and thalamocortical glutamatergic transmissions. Int. J. Mol. Sci. 2021, 22, 4122. [Google Scholar] [CrossRef]
- Ministry of Finance. Japanese Public Fibance Fact Sheet. Available online: https://www.mof.go.jp/english/policy/budget/budget/fy2020/04.pdf (accessed on 1 June 2021).
- Matsubayashi, T.; Sekijima, K.; Ueda, M. Government spending, recession, and suicide: Evidence from Japan. BMC Public Health 2020, 20, 243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meurk, C.; Wittenhagen, L.; Bosley, E.; Steele, M.L.; Bunting, D.; Waterson, E.; Edwards, B.; Martain, B.; Heffernan, E. Suicide crisis calls to emergency services: Cohort profile and findings from a data linkage study in Queensland, Australia. Aust. N. Z. J. Psychiatry 2021. [Google Scholar] [CrossRef]
- Price, J.H.; Mrdjenovich, A.J.; Dake, J.A. Prevalence of state firearm mortality and mental health care resources. J. Community Health 2009, 34, 383–391. [Google Scholar] [CrossRef]
- Hamilton, E.; Klimes-Dougan, B. Gender differences in suicide prevention responses: Implications for adolescents based on an illustrative review of the literature. Int. J. Environ. Res. Public Health 2015, 12, 2359–2372. [Google Scholar] [CrossRef] [Green Version]
- Lapierre, S.; Erlangsen, A.; Waern, M.; De Leo, D.; Oyama, H.; Scocco, P.; Gallo, J.; Szanto, K.; Conwell, Y.; Draper, B.; et al. A systematic review of elderly suicide prevention programs. Crisis 2011, 32, 88–98. [Google Scholar] [CrossRef] [PubMed]
- Hasegawa, T.; Nishikawa, K.; Tamura, Y.; Oka, T.; Urawa, A.; Watanabe, S.; Mizuno, S.; Okada, M. Impacts of interaction of mental condition and quality of life between donors and recipients at decision-making of preemptive and post-dialysis living-donor kidney transplantation. J. Pers. Med. 2021, 11, 414. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health, Labour and Welfare. The Public Assistance System. Available online: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/hukushi_kaigo/seikatsuhogo/seikatuhogo/index.html (accessed on 1 June 2021).
- Cabinet Office. Outline of Measures for Society with Decreasing Birthrate. Available online: https://www8.cao.go.jp/shoushi/shoushika/law/taikou2.html (accessed on 1 June 2021).
- Statistics Bureau of the Ministry of Internal Affairs and Communications (SBMIAC). Family Income and Expenditure Survey. Available online: https://www.e-stat.go.jp/en/stat-search/files?page=1&layout=normal&toukei=00200561 (accessed on 1 May 2021).







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Divisions | Male + Female | Male | Female | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| β | SE | T Ratio | (p) | β | SE | T Ratio | (p) | β | SE | T Ratio | (p) | |
| Public health | −2.107 | 0.237 | −8.892 | ** | −2.834 | 0.398 | −7.113 | ** | −1.447 | 0.124 | −11.627 | ** |
| Public works | 0.845 | 0.127 | 6.626 | ** | 1.263 | 0.218 | 5.798 | ** | 0.485 | 0.073 | 6.636 | ** |
| Police | −0.185 | 0.028 | −6.716 | ** | −0.304 | 0.048 | −6.260 | ** | −0.075 | 0.014 | −5.285 | ** |
| Ambulance/fire | 0.016 | 0.020 | 0.820 | 0.037 | 0.036 | 1.036 | −0.007 | 0.012 | −0.603 | |||
| Welfare | −0.038 | 0.078 | −0.485 | −0.090 | 0.131 | −0.691 | 0.010 | 0.037 | 0.254 | |||
| Education | 0.111 | 0.129 | 0.858 | −0.084 | 0.186 | −0.452 | 0.297 | 0.099 | 3.018 | |||
| Divisions | Males and Females | Males | Females | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| β | SE | T Ratio | (p) | β | SE | T Ratio | (p) | β | SE | T Ratio | (p) | |
| Public health | −0.107 | 0.051 | −2.102 | * | −0.348 | 0.079 | −4.375 | ** | 0.121 | 0.040 | 3.031 | ** |
| Public works | 0.085 | 0.237 | 0.360 | 0.098 | 0.358 | 0.272 | 0.075 | 0.129 | 0.578 | |||
| Police | −1.675 | 2.046 | −0.818 | −0.401 | 2.924 | −0.137 | −2.872 | 1.443 | −1.990 | |||
| Ambulance/fire | −5.372 | 1.027 | −5.231 | ** | −7.604 | 1.450 | −5.246 | ** | −3.416 | 0.700 | −4.880 | ** |
| Welfare | −0.263 | 0.174 | −1.514 | −0.421 | 0.266 | −1.581 | −0.118 | 0.091 | −1.288 | |||
| Education | −2.123 | 0.309 | −6.877 | ** | −3.279 | 0.469 | −6.985 | ** | −1.082 | 0.207 | −5.232 | ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shiroyama, T.; Fukuyama, K.; Okada, M. Effects of Financial Expenditure of Prefectures/Municipalities on Regional Suicide Mortality in Japan. Int. J. Environ. Res. Public Health 2021, 18, 8639. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18168639
Shiroyama T, Fukuyama K, Okada M. Effects of Financial Expenditure of Prefectures/Municipalities on Regional Suicide Mortality in Japan. International Journal of Environmental Research and Public Health. 2021; 18(16):8639. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18168639
Chicago/Turabian StyleShiroyama, Takashi, Kouji Fukuyama, and Motohiro Okada. 2021. "Effects of Financial Expenditure of Prefectures/Municipalities on Regional Suicide Mortality in Japan" International Journal of Environmental Research and Public Health 18, no. 16: 8639. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18168639