
Effectiveness of Pulmonary Rehabilitation in Severe and Critically Ill COVID-19 Patients: A Controlled Study

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
Data Analysis
3. Results
3.1. Patient Demography
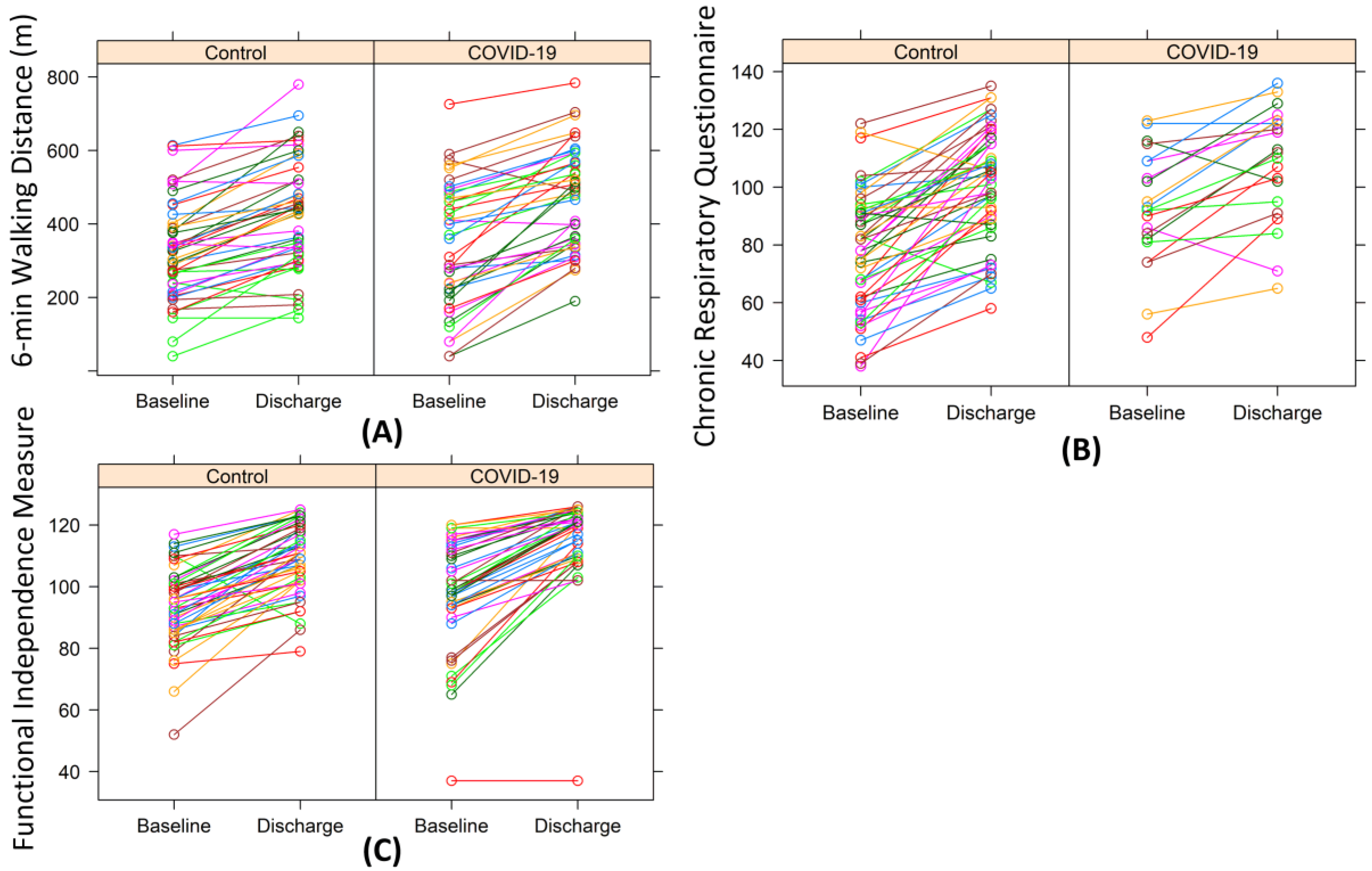
3.2. Outcome of Rehabilitation: COVID-19 Patients vs. Common Pneumonia Patients
3.3. Outcome of Rehabilitation: COVID-19 Patients ICU vs. Non-ICU
4. Discussion
5. Conclusions
6. Highlights
- Our study demonstrates the effectiveness of inpatient PR in COVID-19 patients by both comparing the PR outcomes between the COVID-19 group and a control group with common pneumonia and assessing the minimal clinically important difference.
- Our study also shows similar effectiveness of inpatient PR between severe and critically ill COVID-19 patients.
- Our results suggest that the inpatient PR program immediately following acute hospitalization can significantly reduce the fatigue of COVID-19 patients.
- Our results suggest that COVID-19 patients discharged from acute care should attend the inpatient PR program in order to improve their physical function and quality of life, including fatigue.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Herridge, M.S.; Chu, L.M.; Matte, A.; Tomlinson, G.; Chan, L.; Thomas, C.; Friedrich, J.O.; Mehta, S.; Lamontagne, F.; Levasseur, M.; et al. The RECOVER Program: Disability Risk Groups and 1-Year Outcome after 7 or More Days of Mechanical Ventilation. Am. J. Respir. Crit. Care Med. 2016, 194, 831–844. [Google Scholar] [CrossRef] [PubMed]
- Pfoh, E.R.; Wozniak, A.W.; Colantuoni, E.; Dinglas, V.D.; Mendez-Tellez, P.A.; Shanholtz, C.; Ciesla, N.D.; Pronovost, P.J.; Needham, D.M. Physical declines occurring after hospital discharge in ARDS survivors: A 5-year longitudinal study. Intensiv. Care Med. 2016, 42, 1557–1566. [Google Scholar] [CrossRef] [PubMed]
- Mo, X.; Jian, W.; Su, Z.; Chen, M.; Peng, H.; Peng, P.; Lei, C.; Chen, R.; Zhong, N.; Li, S. Abnormal pulmonary function in COVID-19 patients at time of hospital discharge. Eur. Respir. J. 2020, 55, 2001217. [Google Scholar] [CrossRef] [PubMed]
- Belli, S.; Balbi, B.; Prince, I.; Cattaneo, D.; Masocco, F.; Zaccaria, S.; Bertalli, L.; Cattini, F.; Lomazzo, A.; Negro, F.D.; et al. Low physical functioning and impaired performance of activities of daily life in COVID-19 patients who survived hospitalisation. Eur. Respir. J. 2020, 56, 2002096. [Google Scholar] [CrossRef] [PubMed]
- Townsend, L.; Dyer, A.H.; Jones, K.; Dunne, J.; Mooney, A.; Gaffney, F.; O’Connor, L.; Leavy, D.; O’Brien, K.; Dowds, J.; et al. Persistent Fatigue Following SARS-CoV-2 Infection Is Common and Independent of Severity of Initial Infection. PLoS ONE 2020, 15, e0240784. [Google Scholar] [CrossRef]
- Huang, C.; Huang, L.; Wang, Y.; Li, X.; Ren, L.; Gu, X.; Kang, L.; Guo, L.; Liu, M.; Zhou, X.; et al. 6-month consequences of COVID-19 in patients discharged from hospital: A cohort study. Lancet 2021, 397, 220–232. [Google Scholar] [CrossRef]
- Spruit, M.A.; Holland, A.E.; Singh, S.J.; Tonia, T.; Wilson, K.C.; Troosters, T. COVID-19: Interim guidance on rehabilitation in the hospital and post-hospital phase from a European Respiratory Society- and American Thoracic Society-coordinated international task force. Eur. Respir. J. 2020, 56, 2002197. [Google Scholar] [CrossRef]
- Hermann, M.; Pekacka-Egli, A.-M.; Witassek, F.; Baumgaertner, R.; Schoendorf, S.; Spielmanns, M. Feasibility and Efficacy of Cardiopulmonary Rehabilitation following COVID-19. Am. J. Phys. Med. Rehabil. 2020, 99, 865–869. [Google Scholar] [CrossRef]
- Wiertz, C.M.; Vints, W.A.; Maas, G.J.; Rasquin, S.M.; van Horn, Y.Y.; Dremmen, M.P.; Hemmen, B.; Verbunt, J.A. COVID-19: Patient Characteristics in the First Phase of Postintensive Care Rehabilitation. Arch. Rehabil. Res. Clin. Transl. 2021, 3, 100108. [Google Scholar] [CrossRef]
- Gloeckl, R.; Leitl, D.; Jarosch, I.; Schneeberger, T.; Nell, C.; Stenzel, N.; Vogelmeier, C.F.; Kenn, K.; Koczulla, A.R. Benefits of pulmonary rehabilitation in COVID-19: A prospective observational cohort study. ERJ Open Res. 2021, 7. [Google Scholar] [CrossRef]
- Piquet, V.; Luczak, C.; Seiler, F.; Monaury, J.; Martini, A.; Ward, A.B.; Gracies, J.-M.; Motavasseli, D.; Lépine, E.; Chambard, L.; et al. Do Patients With COVID-19 Benefit from Rehabilitation? Functional Outcomes of the First 100 Patients in a COVID-19 Rehabilitation Unit. Arch. Phys. Med. Rehabil. 2021, 102, 1067–1074. [Google Scholar] [CrossRef]
- Al Chikhanie, Y.; Veale, D.; Schoeffler, M.; Pépin, J.L.; Verges, S.; Hérengt, F. Effectiveness of Pulmonary Rehabilitation in COVID-19 Respiratory Failure Patients Post-Icu. Respir. Physiol. Neurobiol. 2021, 287, 103639. [Google Scholar] [CrossRef]
- Zampogna, E.; Paneroni, M.; Belli, S.; Aliani, M.; Gandolfo, A.; Visca, D.; Bellanti, M.T.; Ambrosino, N.; Vitacca, M. Pulmonary Rehabilitation in Patients Recovering from COVID-19. Respiration 2021, 100, 416–422. [Google Scholar] [CrossRef]
- Spielmanns, M.; Pekacka-Egli, A.-M.; Schoendorf, S.; Windisch, W.; Hermann, M. Effects of a Comprehensive Pulmonary Rehabilitation in Severe Post-COVID-19 Patients. Int. J. Environ. Res. Public Health 2021, 18, 2695. [Google Scholar] [CrossRef]
- McGlothlin, A.E.; Lewis, R.J. Minimal Clinically Important Difference: Defining What Really Matters to Patients. JAMA 2014, 312, 1342–1343. [Google Scholar] [CrossRef] [PubMed]
- Troosters, T. How Important Is a Minimal Difference? Eur. Respir. J. 2011, 37, 755–756. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Darby, A.C.; Hiscox, J.A. COVID-19: Variants and vaccination. BMJ 2021, 372, n771. [Google Scholar] [CrossRef]
- Mahase, E. COVID-19: What New Variants Are Emerging and How Are They Being Investigated? BMJ 2021, 372, n158. [Google Scholar] [CrossRef] [PubMed]
- Fontanet, A.; Autran, B.; Lina, B.; Kieny, M.P.; Karim, S.S.A.; Sridhar, D. SARS-CoV-2 Variants and Ending the COVID-19 Pandemic. Lancet 2021, 397, 952–954. [Google Scholar] [CrossRef]
- Abu-Raddad, L.J.; Chemaitelly, H.; Butt, A.A. Effectiveness of the Bnt162b2 COVID-19 Vaccine against the B.1.1.7 and B.1.351 Variants. N. Engl. J. Med. 2021, 385, 187–189. [Google Scholar] [CrossRef] [PubMed]
- Yesilkaya, U.H.; Sen, M.; Karamustafalioglu, N. New Variants and New Symptoms in COVID-19: First Episode Psychosis and Cotard’s Syndrome Two Months after Infection with the B.1.1.7 Variant of Coronavirus. Schizophr. Res. 2021. [Google Scholar] [CrossRef] [PubMed]
- Karim, S.S.A.; de Oliveira, T.; Loots, G. Appropriate names for COVID-19 variants. Science 2021, 371, 1215. [Google Scholar] [CrossRef]
- Luchsinger, L.L.; Hillyer, C.D. Vaccine efficacy probable against COVID-19 variants. Science 2021, 371, 1116. [Google Scholar] [CrossRef] [PubMed]
- van Oosterhout, C.; Hall, N.; Ly, H.; Tyler, K.M. COVID-19 Evolution During the Pandemic—Implications of New SARS-CoV-2 Variants on Disease Control and Public Health Policies. Virulence 2021, 12, 507–508. [Google Scholar] [CrossRef]
- Abobaker, A.; Nagib, T.; Alsoufi, A. The impact of certain genetic variants (single nucleotide polymorphisms) on incidence and severity of COVID-19. J. Gene Med. 2021, 23, e3310. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.M.S.; Nair, L.; Liu, S.; Iketani, Y.; Luo, Y.; Guo, M.; Wang, J.; Yu, B.; Zhang, P.D.; Kwong, B.S.; et al. Antibody Resistance of SARS-CoV-2 Variants B.1.351 and B.1.1.7. Nature 2021, 593, 130–135. [Google Scholar] [CrossRef]
- Linacre, J.M.; Heinemann, A.W.; Wright, B.D.; Granger, C.V.; Hamilton, B.B. The structure and stability of the Functional Independence Measure. Arch. Phys. Med. Rehabil. 1994, 75, 127–132. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Berman, L.B.; Townsend, M.; Pugsley, S.O.; Chambers, L.W. A measure of quality of life for clinical trials in chronic lung disease. Thorax 1987, 42, 773–778. [Google Scholar] [CrossRef] [Green Version]
- Puhan, M.A.; Behnke, M.; Frey, M.; Grueter, T.; Brandli, O.; Lichtenschopf, A.; Guyatt, G.H.; Schunemann, H.J. Self-administration and interviewer-administration of the German Chronic Respiratory Questionnaire: Instrument development and assessment of validity and reliability in two randomised studies. Heal. Qual. Life Outcomes 2004, 2, 1. [Google Scholar] [CrossRef] [Green Version]
- Spruit, M.A.; Singh, S.J.; Garvey, C.; ZuWallack, R.; Nici, L.; Rochester, C.; Hill, K.; Holland, A.; Lareau, S.C.; Man, W.D.-C.; et al. An Official American Thoracic Society/European Respiratory Society Statement: Key Concepts and Advances in Pulmonary Rehabilitation. Am. J. Respir. Crit. Care Med. 2013, 188, e13–e64. [Google Scholar] [CrossRef]
- Turk, A. Pulmonale Rehabilitationsprogramme der Schweizerischen Gesellschaft für Pneumologie: Akkreditierungsanforderungen. Available online: https://www.pneumo.ch/files/pneumo/pdf/fachpersonen/fortbildung/pulmonale_rehabilitation/Anforderung_Pulm_Rehabilitation_D_02.2020.pdf (accessed on 4 August 2020).
- Singh, S.J.; Puhan, M.A.; Andrianopoulos, N.A.; Hernandes, K.E.; Mitchell, C.J.; Hill, A.L.; Lee, C.A.; Camillo, T.; Troosters, M.A.; Spruit, B.W.; et al. An Official Systematic Review of the European Respiratory Society/American Thoracic Society: Measurement Properties of Field Walking Tests in Chronic Respiratory Disease. Eur. Respir. J. 2014, 44, 1447–1478. [Google Scholar] [CrossRef] [PubMed]
- Jaeschke, R.; Singer, J.; Guyatt, G.H. Measurement of health status: Ascertaining the minimal clinically important difference. Control. Clin. Trials 1989, 10, 407–415. [Google Scholar] [CrossRef]
- Puhan, M.A.; Schunemann, H.J.; Buesching, G.; vanOort, E.; Spaar, A.; Frey, M. Copd Patients’ Ability to Follow Exercise Influences Short-Term Outcomes of Rehabilitation. Eur. Respir. J. 2008, 31, 304–310. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Patients with COVID-19 (n = 51) | Patients with Other Pneumonia (n = 51) | Statistical Analysis | |
|---|---|---|---|
| Male | 38 (75%) | 23 (45%) | OR: 3.5 [1.4, 9.0], p = 0.004 |
| Age | 65.8 ± 11.7, [59.0, 73.5] | 69.8 ± 9.6, [65.0, 76.0] | p = 0.028 |
| BMI | 27.3 ± 4.9, [23.8, 30.1] | 26.1 ± 6.5, [21.6, 29.3] | p = 0.28 |
| Rehabilitation days | 21.7 ± 5.8, [18.0, 27.0] | 20.4 ± 5.4, [18.0, 21.5] | p = 0.20 |
| Patients at ICU | 30 (59%) | 7 (14%) | OR: 8.8 [3.1, 27.7], p < 0.001 |
| Patients intubated | 27 (53%) | 6 (12%) | OR: 8.2 [2.8, 27.9], p < 0.001 |
| Intubation days | 13.2 ± 7.1, [8.3, 15.0] | 9.8 ± 8.3, [5.0, 12.0] | p = 0.15 |
| CIRC | 17.7 ± 11.3, [13, 20] | 13.5 ± 5.9, [9, 18] | p = 0.026 |
| Art. hypertension | 30 (59%) | 19 (37%) | OR: 2.4 [1.0, 5.8], p = 0.047 |
| ARDS | 26 (51%) | 3 (6%) | OR: 16.2 [4.3, 91.5], p < 0.001 |
| COPD | 2 (4%) | 25 (49%) | OR: 0.05 [0.005, 0.2], p < 0.001 |
| Heart diseases | 8 (16%) | 10 (20%) | OR: 0.8 [0.2, 2.4], p = 0.8 |
| Patients with COVID-19 | Patients with Other Pneumonia | Statistical Analysis | |
|---|---|---|---|
| 6 MWT entrance | 336.2 ± 169.3, | 319.8 ± 135.5, | p = 0.61 |
| [222, 470], n = 41 | [231, 389], n = 48 | ||
| 6 MWT discharge | 484.4 ± 146.6, | 416.8 ± 144.8, | p = 0.026 |
| [346, 594], n = 45 | [316, 503], n = 50 | ||
| 6 MWT improvement | 132.8 ± 92.9 *, | 102 ± 73.3 *, | p = 0.088 |
| [72, 173], n = 40 | [54, 138], n = 47 | ||
| CRQ entrance | 91.7 ± 19.8, | 77.9 ± 20.3, | p = 0.0063 |
| [82, 103], n = 25 | [62, 91], n = 51 | ||
| CRQ discharge | 105.8 ± 18.0, | 100.2 ± 19.6, | p = 0.18 |
| [92.5, 120.5], n = 36 | [88, 115], n = 51 | ||
| CRQ improvement | 15.5 ± 15.2 *, | 22.3 ± 16.9 *, | p = 0.12 |
| [5, 28], n = 21 | [13.5, 32], n = 51 | ||
| FIM entrance | 97.3 ± 17.4, | 93.3 ± 12.3, | p = 0.035 |
| [93, 111], n = 4 | [86, 100.5], n = 51 | ||
| FIM discharge | 115.8 ± 14.0, | 108.9 ± 10.9, | p < 0.001 |
| [111, 124], n = 45 | [102, 117.5], n = 51 | ||
| FIM improvement | 18.0 ± 11.4 *, | 15.6 ± 9.6 *, | p = 0.48 |
| [10, 23], n = 45 | [10, 21], n = 51 |
| 6MWT at Discharge (Adjusted R2 = 0.75) | CRQ at Discharge (Adjusted R2 = 0.75) | FIM at Discharge (Adjusted R2 = 0.75) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Estimate | Std. Error | p-Value | Estimate | Std. Error | p-Value | Estimate | Std. Error | p-Value | |
| Age | −2.06 | 0.81 | 0.0134 | −0.23 | 0.18 | 0.202 | −0.05 | 0.06 | 0.432 |
| Sex:m | 34.11 | 17.56 | 0.0557 | 1.33 | 3.77 | 0.726 | 2.45 | 1.35 | 0.072 |
| 6MWT entrance | 0.70 | 0.06 | <0.0001 | / | / | / | / | / | / |
| CRQ entrance | / | / | / | 0.62 | 0.09 | <0.0001 | / | / | / |
| FIM entrance | / | / | / | / | / | / | 0.45 | 0.05 | <0.0001 |
| CIRC | −1.64 | 0.92 | 0.0787 | −0.42 | 0.62 | 0.184 | 0.005 | 0.075 | 0.942 |
| COVID-19: Control | 26.55 | 17.61 | 0.136 | −2.70 | 4.45 | 0.545 | 4.16 | 1.39 | 0.00364 |
| 6MWT at Discharge (Adjusted R2 = 0.77) | CRQ at Discharge (Adjusted R2 = 0.40) | FIM at Discharge (Adjusted R2 = 0.61) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Estimate | Std. Error | p-Value | Estimate | Std. Error | p-Value | Estimate | Std. Error | p-Value | |
| Age | −2.37 | 1.09 | 0.0379 | −0.11 | 0.31 | 0.722 | −0.11 | 0.069 | 0.11 |
| Sex: m | 55.38 | 26.77 | 0.047 | 8.91 | 7.96 | 0.280 | 3.71 | 1.62 | 0.027 |
| 6MWT entrance | 0.57 | 0.073 | <0.0001 | / | / | / | / | / | / |
| CRQ entrance | / | / | / | 0.68 | 0.18 | 0.0021 | / | / | / |
| FIM entrance | / | / | / | / | / | / | 0.36 | 0.051 | <0.0001 |
| CIRS | −1.50 | 0.98 | 0.14 | −0.039 | 0.66 | 0.954 | 0.003 | 0.065 | 0.97 |
| ICU: non-ICU | 31.12 | 25.90 | 0.239 | −5.09 | 7.87 | 0.528 | 1.89 | 1.63 | 0.25 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Büsching, G.; Zhang, Z.; Schmid, J.-P.; Sigrist, T.; Khatami, R. Effectiveness of Pulmonary Rehabilitation in Severe and Critically Ill COVID-19 Patients: A Controlled Study. Int. J. Environ. Res. Public Health 2021, 18, 8956. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18178956
Büsching G, Zhang Z, Schmid J-P, Sigrist T, Khatami R. Effectiveness of Pulmonary Rehabilitation in Severe and Critically Ill COVID-19 Patients: A Controlled Study. International Journal of Environmental Research and Public Health. 2021; 18(17):8956. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18178956
Chicago/Turabian StyleBüsching, Gilbert, Zhongxing Zhang, Jean-Paul Schmid, Thomas Sigrist, and Ramin Khatami. 2021. "Effectiveness of Pulmonary Rehabilitation in Severe and Critically Ill COVID-19 Patients: A Controlled Study" International Journal of Environmental Research and Public Health 18, no. 17: 8956. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18178956