
Inpatient Hospice Palliative Care Unit and Palliative Consultation Service Enhance Comprehensive Quality of Life Outcomes in Terminally Ill Cancer Patients: A Prospective Longitudinal Study

Abstract
:1. Introduction
2. Methods
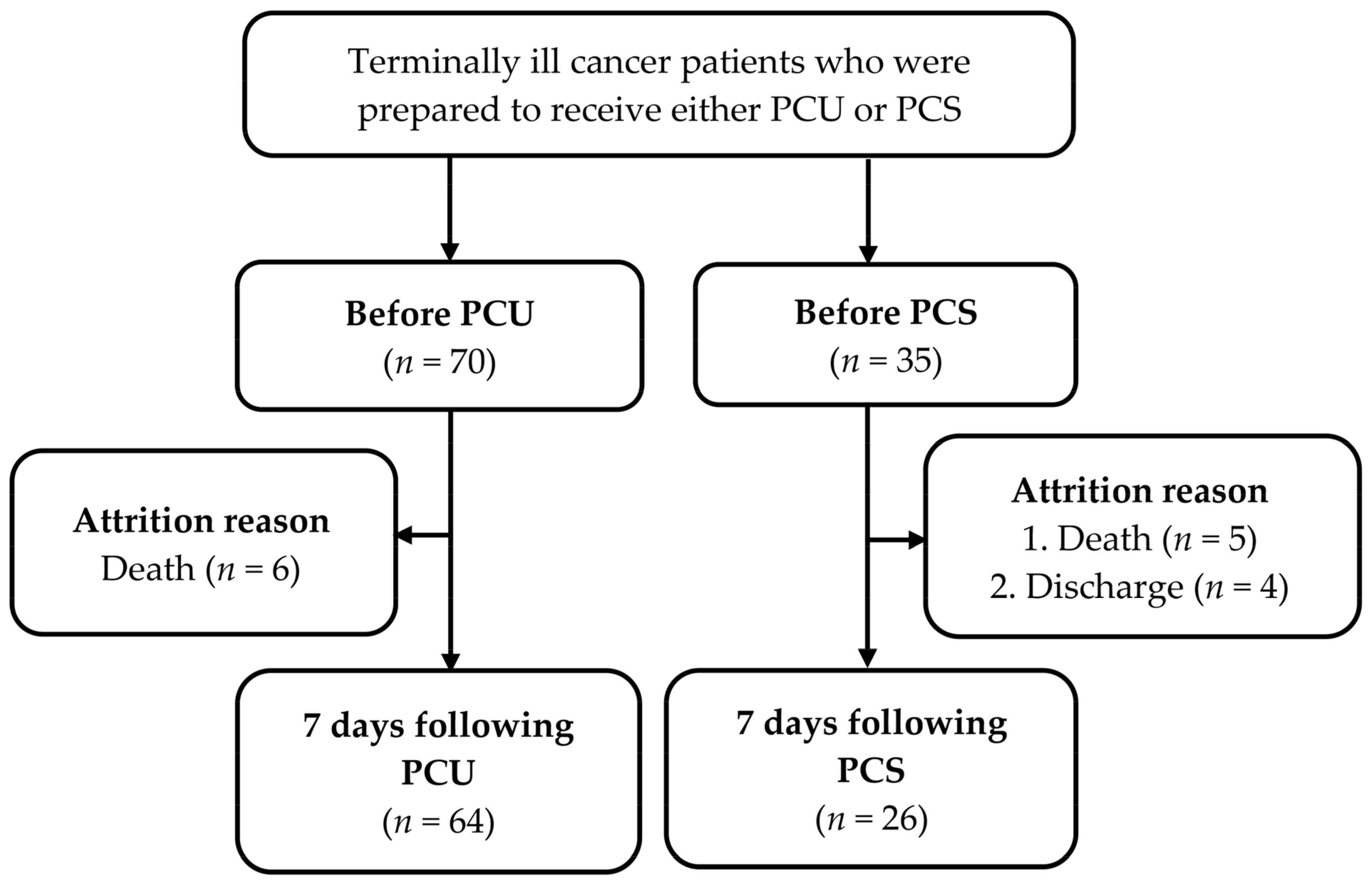
2.1. Study Design and Population
2.2. PCU and PCS
2.3. Measurements
2.3.1. Patient Characteristics
2.3.2. Palliative Prognostic Index (PPI)
2.3.3. Memorial Symptom Assessment Scale Short Form (MSAS-SF)T
2.3.4. Comprehensive Quality of Life Outcomes (CoQoLo) Inventory
2.4. Study Process
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Xu, J.; Murphy, S.L.; Kochanek, K.D.; Arias, E. Mortality in the United States. 2018. Available online: https://www.cdc.gov/nchs/data/databriefs/db355-h.pdf (accessed on 25 August 2020).
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2020. CA Cancer J. Clin. 2020, 70, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health and Welfare. 2018 Cause of Death Statistics. Available online: https://www.mohw.gov.tw/lp-4650-2.html (accessed on 10 November 2019).
- Health Promotion Administration, Ministry of Health and Welfare. Hospice Care. Available online: https://www.hpa.gov.tw/Pages/List.aspx?nodeid=210 (accessed on 25 August 2020).
- Law and Regulations Database of The Republic of China Hospice Palliative Care Act. Available online: https://law.moj.gov.tw/ENG/LawClass/LawAll.aspx?pcode=L0020066 (accessed on 25 August 2020).
- National Health Insurance Administration, Ministry of Health and Welfare. 2018 National Health Insurance Annual Report. Available online: https://www.mohw.gov.tw/cp-4574-49817-2.html (accessed on 10 November 2019).
- Chang, H.T.; Lin, M.H.; Chen, C.K.; Chen, T.J.; Tsai, S.L.; Cheng, S.Y.; Chiu, T.Y.; Tsai, S.T.; Hwang, S.J. Medical care utilization and costs on end-of-life cancer patients: The role of hospice care. Medicine 2016, 95, e5216. [Google Scholar] [CrossRef] [PubMed]
- Chen, B.; Kuo, C.C.; Huang, N.; Fan, V.Y. Reducing costs at the end of life through provider incentives for hospice care: A retrospective cohort study. Palliat Med. 2018, 32, 1389–1400. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.F.; Chang, C.M.; Huang, C.Y. Home-based hospice care reduces end-of-life expenditure in Taiwan: A population-based study. Medicine 2015, 94, e1613. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.T.; Wang, Y.W.; Chi, C.W.; Hu, W.Y.; Lin, R., Jr.; Shiao, C.C.; Tang, W.R. Differences in medical costs for end-of-life patients receiving traditional care and those receiving hospice care: A retrospective study. PLoS ONE 2020, 15, e0229176. [Google Scholar] [CrossRef] [Green Version]
- Mor, V.; Wagner, T.H.; Levy, C.; Ersek, M.; Miller, S.C.; Gidwani-Marszowski, R.; Joyce, N.; Faricy-Anderson, K.; Corneau, E.A.; Lorenz, K.; et al. Association of expanded VA hospice care with aggressive care and cost for veterans with advanced lung cancer. JAMA Oncol. 2019, 5, 810–816. [Google Scholar] [CrossRef]
- Chiang, J.K.; Kao, Y.H. Impact of home hospice care on patients with advanced lung cancer: A longitudinal population-based study in Taiwan. J. Palliat. Med. 2016, 19, 380–386. [Google Scholar] [CrossRef] [PubMed]
- Shih, Y.L.; Hsu, Y.C.; Chiu, W.H.; Chao, C.C. Estimating life expectancy from Chinese medicine could improve end-of-life care in terminally ill cancer patients. Holist. Nurs. Pract. 2018, 32, 247–252. [Google Scholar] [CrossRef]
- Loke, S.S.; Rau, K.M.; Huang, C.F. Impact of combined hospice care on terminal cancer patients. J. Palliat. Med. 2011, 14, 683–687. [Google Scholar] [CrossRef] [Green Version]
- Krikorian, A.; Maldonado, C.; Pastrana, T. Patient's perspectives on the notion of a good death: A systematic review of the literature. J. Pain Symptom Manag. 2020, 59, 152–164. [Google Scholar] [CrossRef] [Green Version]
- Bovero, A.; Gottardo, F.; Botto, R.; Tosi, C.; Selvatico, M.; Torta, R. Definition of a good death, attitudes toward death, and feelings of interconnectedness among people taking care of terminally ill patients with cancer: An exploratory study. Am. J. Hosp. Palliat. Care 2020, 37, 343–349. [Google Scholar] [CrossRef]
- Gafaar, T.O.; Pesambili, M.; Henke, O.; Vissoci, J.R.N.; Mmbaga, B.T.; Staton, C. Good death: An exploratory study on perceptions and attitudes of patients, relatives, and healthcare providers, in northern Tanzania. PLoS ONE 2020, 15, e0233494. [Google Scholar] [CrossRef] [PubMed]
- Cheng, S.Y.; Dy, S.; Fang, P.H.; Chen, C.Y.; Chiu, T.Y. Evaluation of inpatient multidisciplinary palliative care unit on terminally ill cancer patients from providers′ perspectives: A propensity score analysis. Jpn. J. Clin. Oncol. 2013, 43, 161–169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, J.Y.; Kong, K.A.; Chang, Y.J.; Jho, H.J.; Ahn, E.M.; Choi, S.K.; Park, S.; Lee, M.K. Effect of the duration of hospice and palliative care on the quality of dying and death in patients with terminal cancer: A nationwide multicentre study. Eur. J. Cancer Care 2018, 27, e12771. [Google Scholar] [CrossRef] [PubMed]
- Miyashita, M.; Morita, T.; Sato, K.; Tsuneto, S.; Shima, Y. A nationwide survey of quality of end-of-life cancer care in designated cancer centers, inpatient palliative care units, and home hospices in Japan: The J-HOPE study. J. Pain Symptom Manag. 2015, 50, 38–47.e3. [Google Scholar] [CrossRef] [PubMed]
- Morita, T.; Tsunoda, J.; Inoue, S.; Chihara, S. The Palliative Prognostic Index: A scoring system for survival prediction of terminally ill cancer patients. Supportive Care Cancer Off. J. Multinatl. Assoc. Supportive Care Cancer 1999, 7, 128–133. [Google Scholar] [CrossRef] [PubMed]
- Portenoy, R.K.; Thaler, H.T.; Kornblith, A.B.; Lepore, J.M.; Friedlander-Klar, H.; Kiyasu, E.; Sobel, K.; Coyle, N.; Kemeny, N.; Norton, L.; et al. The Memorial Symptom Assessment Scale: An instrument for the evaluation of symptom prevalence, characteristics and distress. Eur. J. Cancer 1994, 30, 1326–1336. [Google Scholar] [CrossRef]
- Chang, V.T.; Hwang, S.S.; Feuerman, M.; Kasimis, B.S.; Thaler, H.T. The Memorial Symptom Assessment Scale Short Form (MSAS-SF): Validity and reliability. Cancer 2000, 89, 1162–1171. [Google Scholar] [CrossRef]
- Cheng, K.K.; Wong, E.M.; Ling, W.M.; Chan, C.W.; Thompson, D.R. Measuring the symptom experience of Chinese cancer patients: A validation of the Chinese version of the memorial symptom assessment scale. J Pain Symptom Manag. 2009, 37, 44–57. [Google Scholar] [CrossRef]
- Miyashita, M.; Wada, M.; Morita, T.; Ishida, M.; Onishi, H.; Tsuneto, S.; Shima, Y. Development and validation of the Comprehensive Quality of Life Outcome (CoQoLo) inventory for patients with advanced cancer. BMJ Support. Palliat. Care 2015, 9, 75–83. [Google Scholar] [CrossRef]
- Gaertner, J.; Frechen, S.; Sladek, M.; Ostgathe, C.; Voltz, R. Palliative care consultation service and palliative care unit: Why do we need both? Oncologist 2012, 17, 428–435. [Google Scholar] [CrossRef]
- Roza, K.A.; Lee, E.J.; Meier, D.E.; Goldstein, N.E. A survey of bereaved family members to assess quality of care on a palliative care unit. J. Palliat. Med. 2015, 18, 358–365. [Google Scholar] [CrossRef]
- Wallston, K.A.; Burger, C.; Smith, R.A.; Baugher, R.J. Comparing the quality of death for hospice and non-hospice cancer patients. Med. Care 1988, 26, 177–182. [Google Scholar] [CrossRef]
- Maeda, I.; Miyashita, M.; Yamagishi, A.; Kinoshita, H.; Shirahige, Y.; Izumi, N.; Yamaguchi, T.; Igarashi, M.; Kato, M.; Morita, T. Changes in relatives' perspectives on quality of death, quality of care, pain relief, and caregiving burden before and after a region-based palliative care intervention. J. Pain Symptom Manag. 2016, 52, 637–645. [Google Scholar] [CrossRef] [Green Version]
- Isenberg, S.R.; Lu, C.; McQuade, J.; Chan, K.K.W.; Gill, N.; Cardamone, M.; Torto, D.; Langbaum, T.; Razzak, R.; Smith, T.J. Impact of a new palliative care program on health system finances: An analysis of the palliative care program inpatient unit and consultations at Johns Hopkins Medical Institutions. J. Oncol. Pract. 2017, 13, e421–e430. [Google Scholar] [CrossRef] [PubMed]
- Lin, W.Y.; Chiu, T.Y.; Ho, C.T.; Davidson, L.E.; Hsu, H.S.; Liu, C.S.; Chiu, C.F.; Peng, C.T.; Chen, C.Y.; Hu, W.Y.; et al. Hospice shared-care saved medical expenditure and reduced the likelihood of intensive medical utilization among advanced cancer patients in Taiwan--a nationwide survey. Supportive Care Cancer Off. J. Multinatl. Assoc. Supportive Care Cancer 2014, 22, 1907–1914. [Google Scholar] [CrossRef] [PubMed]
- Huang, K.S.; Wang, S.H.; Chuah, S.K.; Rau, K.M.; Lin, Y.H.; Hsieh, M.C.; Shih, L.H.; Chen, Y.H. The effects of hospice-shared care for gastric cancer patients. PLoS ONE 2017, 12, e0171365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kehl, K.A. Moving toward peace: An analysis of the concept of a good death. Am. J. Hosp. Palliat. Care 2006, 23, 277–286. [Google Scholar] [CrossRef] [PubMed]
- Hong, S.; Cagle, J.G.; Plant, A.J.; Culler, K.L.; Carrion, I.V.; Van Dussen, D.J. Quality of death among hospice decedents: Proxy observations from a survey of community-dwelling adults in the contiguous United States. Death Stud. 2016, 40, 529–537. [Google Scholar] [CrossRef]
- Roth, A.R.; Canedo, A.R. Introduction to hospice and palliative care. Prim. Care 2019, 46, 287–302. [Google Scholar] [CrossRef]
- Cheng, S.Y.; Hu, W.Y.; Liu, W.J.; Yao, C.A.; Chen, C.Y.; Chiu, T.Y. Good death study of elderly patients with terminal cancer in Taiwan. Palliat. Med. 2008, 22, 626–632. [Google Scholar] [CrossRef] [PubMed]
- Cheng, S.Y.; Dy, S.; Hu, W.Y.; Chen, C.Y.; Chiu, T.Y. Factors affecting the improvement of quality of dying of terminally ill patients with cancer through palliative care: A ten-year experience. J. Palliat. Med. 2012, 15, 854–862. [Google Scholar] [CrossRef] [PubMed]
- Morita, T.; Kuriya, M.; Miyashita, M.; Sato, K.; Eguchi, K.; Akechi, T. Symptom burden and achievement of good death of elderly cancer patients. J. Palliat. Med. 2014, 17, 887–893. [Google Scholar] [CrossRef] [PubMed]
- Tang, S.T.; Chou, W.C.; Hsieh, C.H.; Chang, W.C.; Chen, J.S.; Wen, F.H. Terminally ill cancer patients' emotional preparedness for death is distinct from their accurate prognostic awareness. J. Pain Symptom Manag. 2020, 60, 774–781. [Google Scholar] [CrossRef]
- Catt, S.; Blanchard, M.; Addington-Hall, J.; Zis, M.; Blizard, R.; King, M. Older adults' attitudes to death, palliative treatment and hospice care. Palliat. Med. 2005, 19, 402–410. [Google Scholar] [CrossRef]
- Fleming, J.; Farquhar, M.; Brayne, C.; Barclay, S. Death and the oldest old: Attitudes and preferences for end-of-life vare—Qualitative tesearch within a population-based cohort study. PLoS ONE 2016, 11, e0150686. [Google Scholar] [CrossRef]
- Depaola, S.J.; Griffin, M.; Young, J.R.; Neimeyer, R.A. Death anxiety and attitudes toward the elderly among older adults: The role of gender and ethnicity. Death Stud. 2003, 27, 335–354. [Google Scholar] [CrossRef]
- Leung, K.K.; Liu, W.J.; Cheng, S.Y.; Chiu, T.Y.; Chen, C.Y. What do laypersons consider as a good death. Supportive Care Cancer Off. J. Multinatl. Assoc. Supportive Care Cancer 2009, 17, 691–699. [Google Scholar] [CrossRef]
- Kastbom, L.; Milberg, A.; Karlsson, M. A good death from the perspective of palliative cancer patients. Supportive Care Cancer Off. J. Multinatl. Assoc. Supportive Care Cancer 2017, 25, 933–939. [Google Scholar] [CrossRef]
- Chaar, E.A.; Hallit, S.; Hajj, A.; Aaraj, R.; Kattan, J.; Jabbour, H.; Khabbaz, L.R. Evaluating the impact of spirituality on the quality of life, anxiety, and depression among patients with cancer: An observational transversal study. Supportive Care Cancer Off. J. Multinatl. Assoc. Supportive Care Cancer 2018, 26, 2581–2590. [Google Scholar] [CrossRef]
- Nagoya, Y.; Miyashita, M.; Shiwaku, H. Pediatric cancer patients' important end-of-life issues, including quality of life: A survey of pediatric oncologists and nurses in Japan. J. Palliat. Med. 2017, 20, 487–493. [Google Scholar] [CrossRef] [PubMed]
- Axelsson, L.; Klang, B.; Lundh Hagelin, C.; Jacobson, S.H.; Gleissman, S.A. Meanings of being a close relative of a family member treated with haemodialysis approaching end of life. J. Clin. Nurs. 2015, 24, 447–456. [Google Scholar] [CrossRef] [Green Version]
- Vanderveken, L.; Schoenmakers, B.; De Lepeleire, J. A better understanding of the concept "a good death": How do healthcare providers define a good death? Am. J. Geriatr. Psychiatry 2019, 27, 463–471. [Google Scholar] [CrossRef] [PubMed]
- Leung, K.K.; Tsai, J.S.; Cheng, S.Y.; Liu, W.J.; Chiu, T.Y.; Wu, C.H.; Chen, C.Y. Can a good death and quality of life be achieved for patients with terminal cancer in a palliative care unit? J. Palliat. Med. 2010, 13, 1433–1438. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.S.; Wen, F.H.; Chou, W.C.; Hsieh, C.H.; Chang, W.C.; Tang, S.T. Terminally ill cancer patients' distinct symptom-functional patterns/states are differentially associated with their accurate prognostic awareness in the last six months of life. J. Palliat. Med. 2019, 22, 782–789. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | PCU | PCS | |
|---|---|---|---|
| (n = 70) | (n = 35) | p Value | |
| Mean ± SD/n (%) | Mean ± SD/n (%) | ||
| Age | 67.6 ± 12.0 | 65.1 ± 14.6 | 0.348 |
| Sex | 0.779 | ||
| Male | 42 (60.0) | 20 (57.1) | |
| Female | 28 (40.0) | 15 (42.9) | |
| Educational level | 0.162 | ||
| High school and below | 44 (62.9) | 17 (48.6) | |
| Specialist or above | 26 (37.1) | 18 (51.4) | |
| Religious belief | 0.290 | ||
| No | 23 (32.9) | 8 (22.9) | |
| Yes | 47 (67.1) | 27 (77.1) | |
| Marital status | 0.238 | ||
| Single | 20 (28.6) | 14 (40.0) | |
| Married | 50 (71.4) | 21 (60.0) | |
| Child | 1.000 a | ||
| No | 7 (10.0) | 4 (11.4) | |
| Yes | 63 (90.0) | 31 (88.6) | |
| Living with others | 0.330 a | ||
| No | 2 (2.9) | 3 (8.6) | |
| Yes | 68 (97.1) | 32 (91.4) | |
| Caregiver identity | 0.336 a | ||
| None | 1 (1.4) | 3 (8.6) | |
| Spouse | 32 (45.7) | 17 (48.6) | |
| Child | 22 (31.4) | 9 (25.7) | |
| Others | 15 (21.4) | 6 (17.1) | |
| Closeness with family | 3.0 ± 1.3 | 2.9 ± 1.3 | 0.833 |
| Economic sources | 0.549 | ||
| Self | 50 (71.4) | 23 (65.7) | |
| Others | 20 (28.6) | 12 (34.3) | |
| Economic status | 0.479 | ||
| <20,000 NTD | 29 (41.4) | 12 (34.3) | |
| ≥20,000 NTD | 41 (58.6) | 23 (65.7) | |
| Experienced deaths of family and friends | 0.263 | ||
| ≤2 times | 15 (21.4) | 11 (31.4) | |
| >3 times | 55 (78.6) | 24 (68.6) | |
| Perceived disease severity | 3.3 ± 0.6 | 3.4 ± 0.8 | 0.471 |
| Duration of cancer diagnosis (years) | 4.2 ± 2.4 | 3.8 ± 2.6 | 0.828 |
| Palliative prognostic index | 4.7 ± 3.0 | 4.4 ± 2.7 | 0.640 |
| Symptom severity | 29.3 ± 11.2 | 27.7 ± 13.2 | 0.521 |
| Variables | PCU | PCS | |
|---|---|---|---|
| Mean ± SD | Mean ± SD | p Value | |
| CoQoLo level | |||
| Pre-care (70 vs. 35) | 125.6 ± 20.2 | 122.1 ± 20.3 | 0.403 |
| Seven days following care (64 vs. 26) | 136.2 ± 14.6 | 132.2 ± 16.4 | 0.211 |
| Mean difference pre- and seven days following care | 10.6 ± 14.7 | 10.1 ± 16.7 | 0.886 |
| Paired t-test | p < 0.001 | p < 0.001 |
| Variable. | Crude β (95% CI) | p Value | Adjusted β (95% CI) | p Value |
|---|---|---|---|---|
| Time * hospice palliative style | ||||
| Pre-care | ||||
| PCU/PCS | Reference | Reference | ||
| Seven days following care | ||||
| PCU/PCS | 1.7 (−3.7–7.3) | 0.838 | 3.1 (−2.3–8.5) | 0.257 |
| Time | ||||
| Pre-care | Reference | Reference | ||
| Seven days following care | 11.2 (7.0–15.4) | <0.001 | 5.3 (0.8–9.8) | 0.020 |
| Hospice palliative style | ||||
| PCU | 1.2 (−6.6–9.1) | 0.157 | 0.7 (−6.2–7.5) | 0.850 |
| PCS | Reference | Reference | ||
| Age | 0.2 (−0.002–0.5) | 0.052 | 0.3 (0.01–0.5) | 0.041 |
| Sex | ||||
| Male | Reference | Reference | ||
| Female | 2.3 (−3.5–8.1) | 0.443 | 0.5 (−4.8–5.8) | 0.858 |
| Educational level | ||||
| High school and below | Reference | Reference | ||
| Specialized or above | −1.6 (−7.8–4.6) | 0.614 | 4.5 (−1.1–10.1) | 0.117 |
| Religious belief | ||||
| No | Reference | Reference | ||
| Yes | 6.4 (−0.3–13.0) | 0.061 | 8.7 (1.8–15.5) | 0.013 |
| Marital status | ||||
| Single | Reference | Reference | ||
| Married | −5.3 (−11.4–0.8) | 0.089 | −7.8 (−14.9–−0.8) | 0.029 |
| Child | ||||
| No | Reference | Reference | ||
| Yes | 2.2 (5.0–−7.6) | 0.661 | −4.8 (−17.2–7.5) | 0.442 |
| Living with others | ||||
| No | Reference | Reference | ||
| Yes | −3.6 (−14.1–6.9) | 0.501 | −15.7 (−34.1–2.7) | 0.095 |
| Caregiver | ||||
| No | Reference | Reference | ||
| Spouse | −4.4 (−20.5–11.6) | 0.589 | 10.7 (−13.2–34.6) | 0.379 |
| Child | −1.6 (−17.8–14.6) | 0.038 | 10.2 (−13.8–34.1) | 0.405 |
| Others | −5.5 (−21.6–10.7) | 0.507 | 2.1 (−20.7–24.9) | 0.858 |
| Closeness with family | 2.5 (0.1–4.8) | 0.041 | 2.8 (0.6–5.0) | 0.011 |
| Economic source | ||||
| Self | Reference | Reference | ||
| Others | −0.4 (−6.0–5.2) | 0.881 | 1.2 (−4.2–6.6) | 0.659 |
| Economic status | ||||
| <20,000 NTD | Reference | Reference | ||
| ≥20,000 NTD | −1.7 (−8.0–4.6) | 0.598 | −5.0 (−10.2–0.2) | 0.061 |
| Experienced deaths of family and friends | ||||
| <3 times | Reference | Reference | ||
| ≥3 times | 5.3 (−1.4–12.0) | 0.119 | 2.0 (−5.1–9.0) | 0.581 |
| Perceived disease severity | 0.7 (−4.5–5.9) | 0.797 | 0.02 (−4.5–4.5) | 0.995 |
| Duration of cancer diagnosis (years) | −0.2 (−1.2–0.9) | 0.736 | 0.2 (−0.8–1.1) | 0.733 |
| Palliative prognostic index | 1.5 (0.6–2.4) | 0.002 | 1.5 (0.6–2.4) | 0.001 |
| Symptom severity | −0.6 (−0.8–−0.4) | <0.001 | −0.4 (−0.6–−0.2) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, L.-F.; Wu, L.-F.; Lin, C.-K.; Ho, C.-L.; Hung, Y.-C.; Pan, H.-H. Inpatient Hospice Palliative Care Unit and Palliative Consultation Service Enhance Comprehensive Quality of Life Outcomes in Terminally Ill Cancer Patients: A Prospective Longitudinal Study. Int. J. Environ. Res. Public Health 2021, 18, 8992. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18178992
Chang L-F, Wu L-F, Lin C-K, Ho C-L, Hung Y-C, Pan H-H. Inpatient Hospice Palliative Care Unit and Palliative Consultation Service Enhance Comprehensive Quality of Life Outcomes in Terminally Ill Cancer Patients: A Prospective Longitudinal Study. International Journal of Environmental Research and Public Health. 2021; 18(17):8992. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18178992
Chicago/Turabian StyleChang, Li-Fang, Li-Fen Wu, Chi-Kang Lin, Ching-Liang Ho, Yu-Chun Hung, and Hsueh-Hsing Pan. 2021. "Inpatient Hospice Palliative Care Unit and Palliative Consultation Service Enhance Comprehensive Quality of Life Outcomes in Terminally Ill Cancer Patients: A Prospective Longitudinal Study" International Journal of Environmental Research and Public Health 18, no. 17: 8992. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18178992