
Sex Differences and Predictors of In-Hospital Mortality among Patients with COVID-19: Results from the ANCOHVID Multicentre Study

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Setting
2.2. Variables and Data Sources
2.3. Statistical Analyses
2.4. Ethical Considerations
3. Results
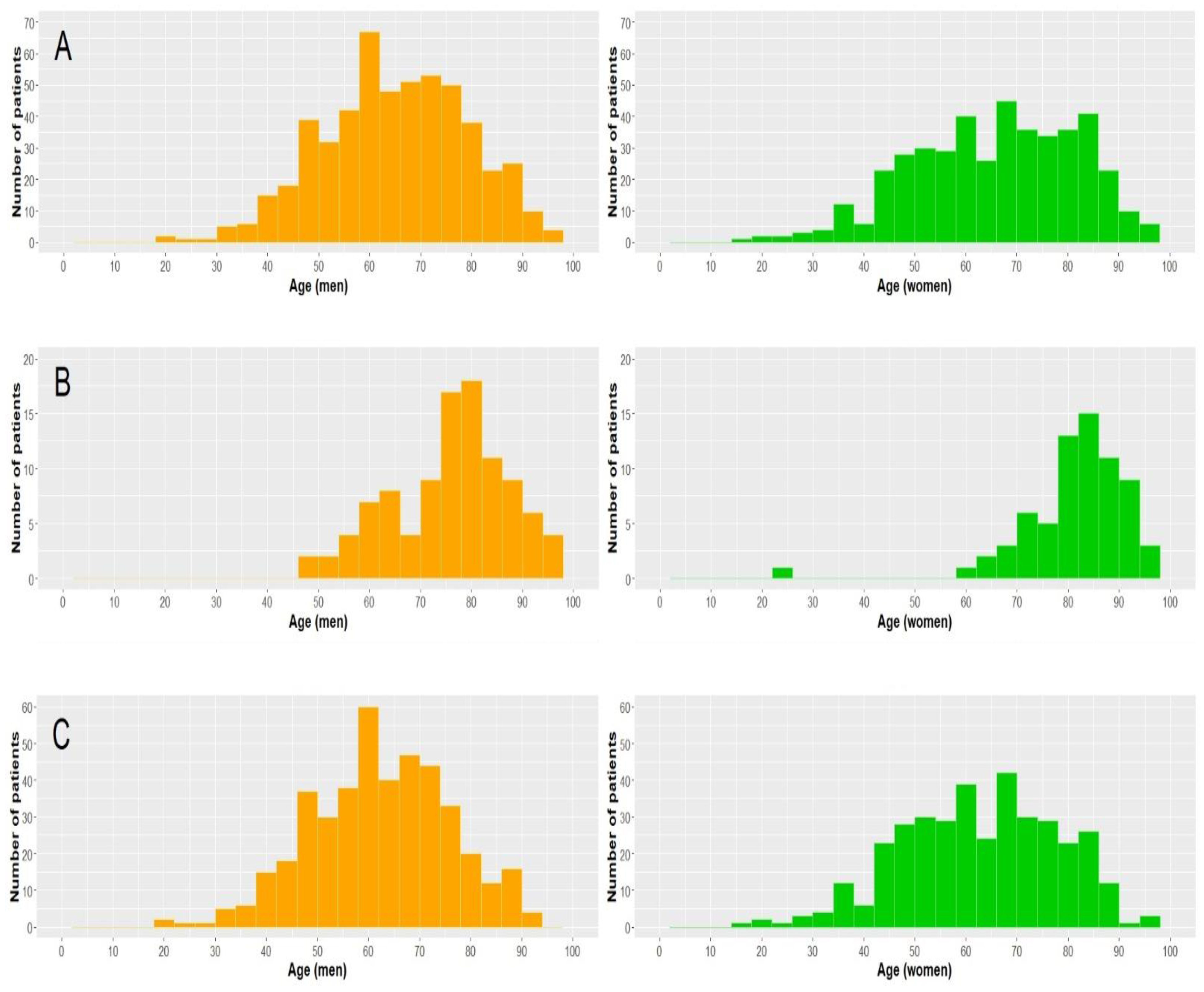
3.1. Patient Characteristics
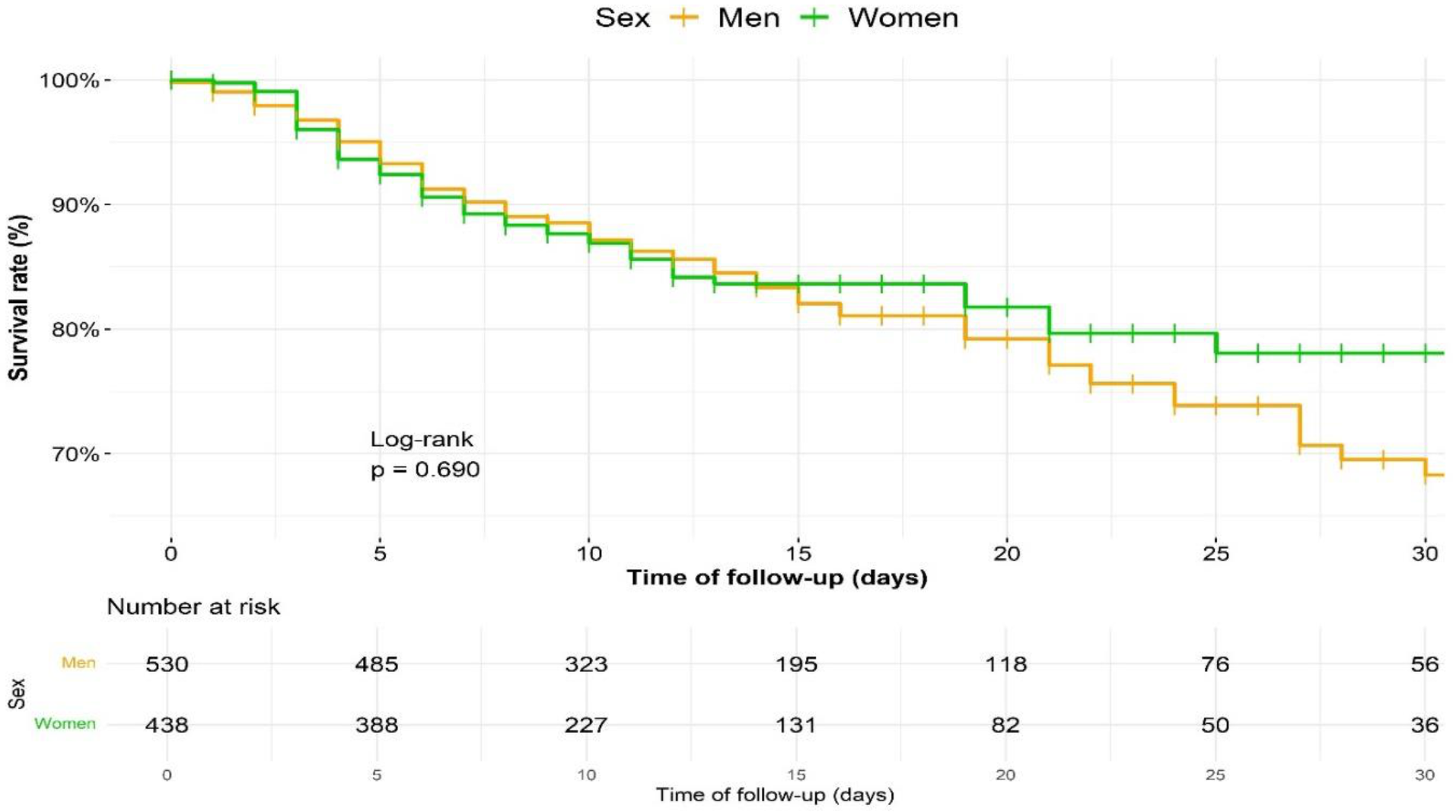
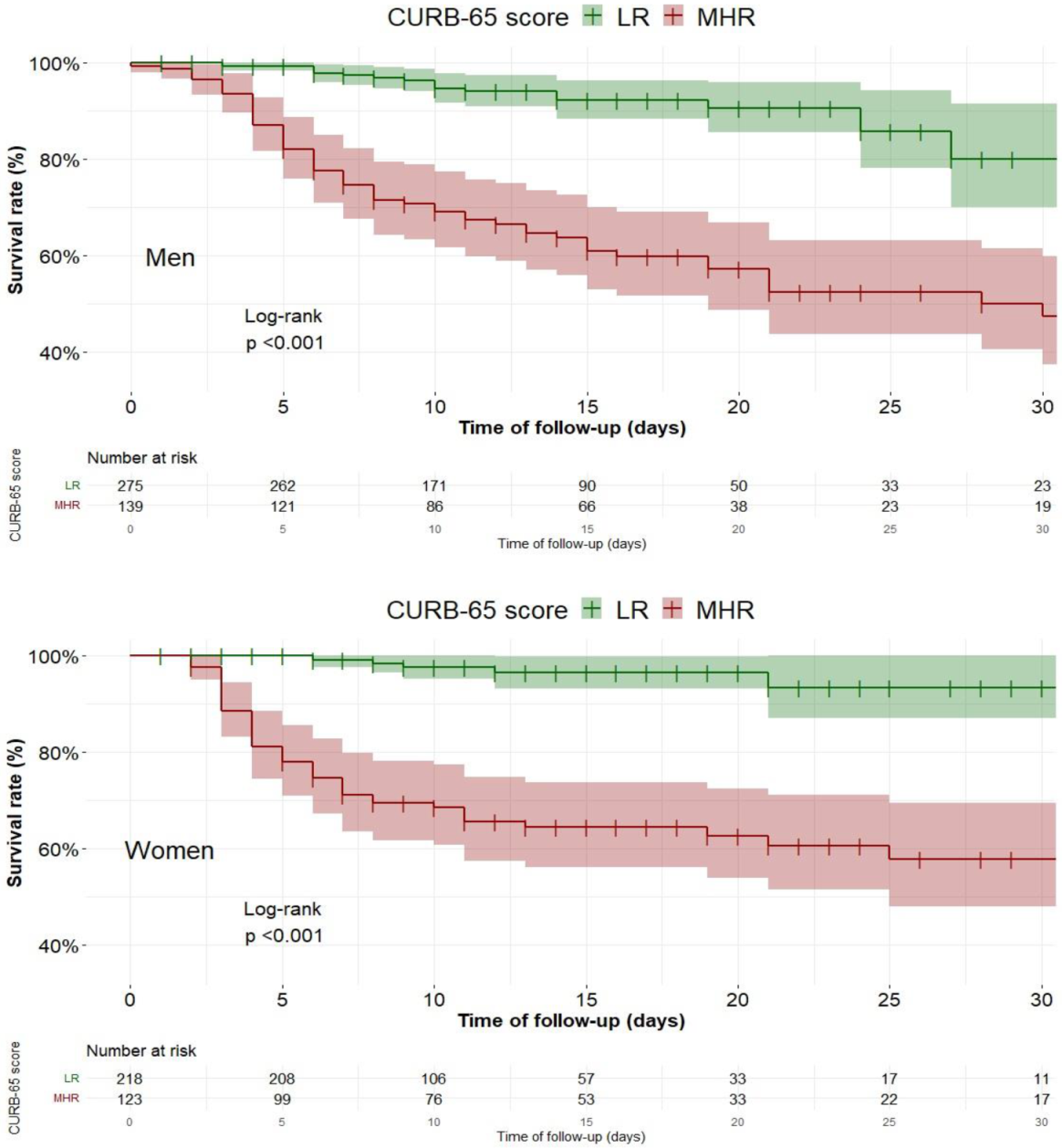
3.2. Survival Analysis
3.3. Multivariate Analysis
4. Discussion
4.1. Predictors of In-Hospital Mortality
4.2. Sex and Gender Differences
4.3. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Centro de Coordinación de Alertas y Emergencias Sanitarias (CCAES). Ministerio de Sanidad. Gobierno de España. Actualización n° 408. Enfermedad por el Coronavirus (COVID-19). 30.06.2021. Madrid. 2021. Available online: https://www.mscbs.gob.es/profesionales/saludPublica/ccayes/alertasActual/nCov/documentos/Actualizacion_408_COVID-19.pdf (accessed on 23 June 2021).
- Dorjee, K.; Kim, H.; Bonomo, E.; Dolma, R. Prevalence and predictors of death and severe disease in patients hospitalized due to COVID-19: A comprehensive systematic review and meta-analysis of 77 studies and 38,000 patients. PLoS ONE 2020, 15, e0243191. Available online: https://pubmed.ncbi.nlm.nih.gov/33284825/ (accessed on 13 April 2021). [CrossRef] [PubMed]
- Wenham, C.; Smith, J.; Morgan, R. COVID-19: The gendered impacts of the outbreak. Lancet 2020, 395, 846–848. [Google Scholar] [CrossRef] [Green Version]
- Mesas, A.E.; Cavero-Redondo, I.; Álvarez-Bueno, C.; Cabrera, M.A.S.; De Andrade, S.M.; Sequí-Dominguez, I.; Martínez-Vizcaíno, V. Predictors of in-hospital COVID-19 mortality: A comprehensive systematic review and meta-analysis exploring differences by age, sex and health conditions. PLoS ONE 2020, 15, e0241742. Available online: https://pubmed.ncbi.nlm.nih.gov/33141836/ (accessed on 13 April 2021). [CrossRef]
- Schiffer, V.M.M.M.; Janssen, E.B.N.J.; van Bussel, B.C.T.; Jorissen, L.L.M.; Tas, J.; Sels, J.W.E.M.; Bergmans, D.C.J.J.; Dinh, T.H.T.; Van Kuijk, S.M.J.; Hana, A.; et al. The “sex gap” in COVID-19 trials: A scoping review. EClinicalMedicine 2020, 29, 100652. Available online: https://pubmed.ncbi.nlm.nih.gov/33283178/ (accessed on 26 June 2021).
- Solar, O.; Irwin, A. A Conceptual Framework for Action on the Social Determinants of Health. Social Determinants of Health Discussion Paper 2 (Policy and Practice); World Health Organization: Geneva, Switzerland, 2010; Available online: http://www.who.int/sdhconference/resources/ConceptualframeworkforactiononSDH_eng.pdf (accessed on 7 June 2021).
- Muñoz-Rodríguez, J.R.; Gómez-Romero, F.J.; Pérez-Ortiz, J.M.; López-Juárez, P.; Santiago, J.L.; Serrano-Oviedo, L.; Redondo-Calvo, F.J. Characteristics and risk factors associated with mortality in a multicenter Spanish cohort of patients with COVID-19 pneumonia. Arch. Bronconeumol. 2021, 57, 34–41. [Google Scholar] [CrossRef]
- Poblador-Plou, B.; Carmona-Pírez, J.; Ioakeim-Skoufa, I.; Poncel-Falcó, A.; Bliek-Bueno, K.; Pozo, M.C.-D.; Gimeno-Feliú, L.A.; González-Rubio, F.; Aza-Pascual-Salcedo, M.; Bandrés-Liso, A.C.; et al. Baseline chronic comorbidity and mortality in laboratory-confirmed COVID-19 cases: Results from the PRECOVID study in Spain. Int. J. Environ. Res. Public Health 2020, 17, 5171. Available online: https://pubmed.ncbi.nlm.nih.gov/32709002/ (accessed on 16 April 2021). [CrossRef] [PubMed]
- Gutiérrez-Abejón, E.; Tamayo, E.; Martín-García, D.; Álvarez, J.F.; Herrera-Gómez, F. Clinical profile, treatment and predictors during the first covid-19 wave: A population-based registry analysis from Castile and Leon hospitals. Int. J. Environ. Res. Public Health 2020, 17, 9360. [Google Scholar] [CrossRef]
- Gude-Sampedro, F.; Fernández-Merino, C.; Ferreiro, L.; Lado-Bsee aleato, Ó.; Espasandín-Domínguez, J.; Hervada, X.; Cadarso, C.M.; Valdés, L. Development and validation of a prognostic model based on comorbidities to predict COVID-19 severity: A population-based study. Int. J. Epidemiol. 2021, 50, 64–74. [Google Scholar] [CrossRef] [PubMed]
- IECA. Informe COVID-19 Coronavirus en Andalucía. Instituto de Estadística y Cartografía de Andalucía. Consejería de Salud y Familias. Junta de Andalucía. 2021. Available online: https://www.juntadeandalucia.es/institutodeestadisticaycartografia/salud/COVID19.html (accessed on 7 June 2021).
- Rodríguez-Blas M del, C. Estadística de Gasto Sanitario Público 2019. Principales Resultados. 2021. Available online: https://www.mscbs.gob.es/estadEstudios/estadisticas/docs/EGSP2008/egspPrincipalesResultados.pdf (accessed on 7 June 2021).
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Lancet 2007, 370, 1453–1457. Available online: https://pubmed.ncbi.nlm.nih.gov/18064739/ (accessed on 14 April 2021). [CrossRef]
- Romero-Duarte, A.; Rivera-Izquierdo, M.; de Alba, I.G.-F.; Pérez-Contreras, M.; Fernández-Martínez, N.F.; Ruiz-Montero, R.; Serrano-Ortiz, Á.; González-Serna, R.; Salcedo-Leal, I.; Jiménez-Mejías, E.; et al. Sequelae, persistent symptomatology and outcomes after COVID-19 hospitalization: The ANCOHVID multicentre 6-month follow-up study. BMC Med. 2021, 19, 1–13. Available online: http://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pubmed/34011359 (accessed on 7 June 2021). [CrossRef] [PubMed]
- Centro de Coordinación de Alertas y Emergencias Sanitarias (CCAES). Ministerio de Sanidad. Gobierno de España. Procedimiento de Actuación Frente a Casos de Infección por el Nuevo Coronavirus (SARS-CoV-2). Actualizado a 27 de Febrero de 2020. Available online: https://www.mscbs.gob.es/profesionales/saludPublica/ccayes/alertasActual/nCov/documentos.htm (accessed on 2 August 2021).
- Casas-Rojo, J.; Antón-Santos, J.; Millán-Núñez-Cortés, J.; Lumbreras-Bermejo, C.; Ramos-Rincón, J.; Roy-Vallejo, E.; Artero-Mora, A.; Arnalich-Fernández, F.; García-Bruñén, J.; Vargas-Núñez, J.; et al. Clinical characteristics of patients hospitalized with COVID-19 in Spain: Results from the SEMI-COVID-19 Registry. Rev. Clín. Esp. 2020, 220, 480–494. [Google Scholar] [CrossRef] [PubMed]
- Berenguer, J.; Ryan, P.; Rodríguez-Baño, J.; Jarrín, I.; Carratala, J.; Pachón, J.; Yllescas, M.; Arriba, J.R.; Muñoz, E.A.; Gil Divasson, P.; et al. Characteristics and predictors of death among 4035 consecutively hospitalized patients with COVID-19 in Spain. Clin. Microbiol. Infect. 2020, 26, 1525–1536. Available online: https://pubmed.ncbi.nlm.nih.gov/32758659/ (accessed on 12 April 2021). [CrossRef]
- Josa-Laorden, C.; Crestelo-Vieitez, A.; Andreu, M.D.M.G.; Rubio-Rivas, M.; Sánchez, M.; Samaniego, N.T.; Fernández, F.A.; Bermudez, R.I.; Aizpuru, E.M.F.; Núñez, J.A.V.; et al. Gender-based differences by age range in patients hospitalized with COVID-19: A Spanish observational cohort study. J. Clin. Med. 2021, 10, 899. Available online: https://pubmed.ncbi.nlm.nih.gov/33668766/ (accessed on 17 May 2021). [CrossRef]
- Figliozzi, S.; Masci, P.G.; Ahmadi, N.; Tondi, L.; Koutli, E.; Aimo, A.; Stamatelopoulos, K.; Dimopoulos, M.; Caforio, A.L.P.; Georgiopoulos, G. Predictors of adverse prognosis in COVID-19: A systematic review and meta-analysis. Eur. J. Clin. Investig. 2020, 50, e13362. Available online: https://pubmed.ncbi.nlm.nih.gov/32726868/ (accessed on 13 April 2021). [CrossRef] [PubMed]
- Kelada, M.; Anto, A.; Dave, K.; Saleh, S.N. the role of sex in the risk of mortality from COVID-19 amongst adult patients: A systematic review. Cureus 2020, 12. Available online: https://pubmed.ncbi.nlm.nih.gov/33005531/ (accessed on 21 May 2021). [CrossRef]
- Ortolan, A.; Lorenzin, M.; Felicetti, M.; Doria, A.; Ramonda, R. Does gender influence clinical expression and disease outcomes in COVID-19? A systematic review and meta-analysis. Int. J. Infect. Dis. 2020, 99, 496–504. Available online: https://pubmed.ncbi.nlm.nih.gov/32800858/ (accessed on 21 May 2021). [CrossRef] [PubMed]
- Pérez-López, F.R.; Tajada, M.; Savirón-Cornudella, R.; Sánchez-Prieto, M.; Chedraui, P.; Terán, E. Coronavirus disease 2019 and gender-related mortality in European countries: A meta-analysis. Maturitas 2020, 141, 59–62. Available online: https://pubmed.ncbi.nlm.nih.gov/33036704/ (accessed on 3 August 2021). [CrossRef] [PubMed]
- Lim, W.S.; Van Der Eerden, M.M.; Laing, R.; Boersma, W.G.; Karalus, N.; Town, I.G.; Lewis, A.S.; Macfarlane, J.T. Defining community acquired pneumonia severity on presentation to hospital: An international derivation and validation study. Thorax 2003, 58, 377–382. Available online: https://pubmed.ncbi.nlm.nih.gov/12728155/ (accessed on 7 June 2021). [CrossRef] [PubMed] [Green Version]
- Satici, C.; Demirkol, M.A.; Altunok, E.S.; Gursoy, B.; Alkan, M.; Kamat, S.; Demirok, B.; Surmeli, C.D.; Çalık, M.; Cavus, Z.; et al. Performance of pneumonia severity index and CURB-65 in predicting 30-day mortality in patients with COVID-19. Int. J. Infect. Dis. 2020, 98, 84–89. Available online: https://pubmed.ncbi.nlm.nih.gov/32553714/ (accessed on 21 May 2021). [CrossRef]
- Duca, A.; Piva, S.; Foca’, E.; Latronico, N.; Rizzi, M. Calculated decisions: Brescia-COVID respiratory severity scale (BCRSS)/algorithm. Emerg. Med. Pract. 2020, 22, CD1–CD2. [Google Scholar]
- Rivera-Izquierdo, M.; Valero-Ubierna, M.D.C.; R.-DelAmo, J.L.; Fernández-García, M.Á.; Martínez-Diz, S.; Tahery-Mahmoud, A.; Rodríguez-Camacho, M.; Gámiz-Molina, A.B.; Barba-Gyengo, N.; Gámez-Baeza, P.; et al. Sociodemographic, clinical and laboratory factors on admission associated with COVID-19 mortality in hospitalized patients: A retrospective observational study. PLoS ONE 2020, 15, e0235107. Available online: https://pubmed.ncbi.nlm.nih.gov/32584868/ (accessed on 21 May 2021). [CrossRef]
- Abaleke, E.; Abbas, M.; Abbasi, S.; Abbott, A.; Abdelaziz, A.; Abdelbadiee, S.; Abdelfattah, M.; Abdul, B.; Rasheed, A.A.; Abdul-Kadir, R.; et al. Azithromycin in patients admitted to hospital with COVID-19 (RECOVERY): A randomised, controlled, open-label, platform trial. Lancet 2021, 397, 605–612. Available online: https://pubmed.ncbi.nlm.nih.gov/33545096/ (accessed on 25 May 2021). [CrossRef]
- Amsden, G.W. Anti-inflammatory effects of macrolides—An underappreciated benefit in the treatment of community-acquired respiratory tract infections and chronic inflammatory pulmonary conditions? J. Antimicrob. Chemother. 2005, 55, 10–21. Available online: https://pubmed.ncbi.nlm.nih.gov/15590715/ (accessed on 25 May 2021). [CrossRef] [Green Version]
- Sterne, J.A.C.; Murthy, S.; Diaz, J.V.; Slutsky, A.S.; Villar, J.; Angus, D.C.; Marshall, J.C. Association between administration of systemic corticosteroids and mortality among critically ill patients with COVID-19: A Meta-analysis. JAMA J. Am. Med. Assoc. 2020, 24, 1330–1341. Available online: https://pubmed.ncbi.nlm.nih.gov/32876694/ (accessed on 25 May 2021).
- Nguyen, J.L.; Yang, W.; Ito, K.; Matte, T.D.; Shaman, J.; Kinney, P.L. Seasonal influenza infections and cardiovascular disease mortality. JAMA Cardiol. 2016, 1, 274–281. Available online: https://pubmed.ncbi.nlm.nih.gov/27438105/ (accessed on 7 June 2021). [CrossRef] [Green Version]
- Avila, J.; Long, B.; Holladay, D.; Gottlieb, M. Thrombotic Complications of COVID-19. Am. J. Emerg. Med. 2021, 39, 213–218. Available online: https://pubmed.ncbi.nlm.nih.gov/33036855/ (accessed on 7 May 2021). [CrossRef]
- Higham, A.; Mathioudakis, A.; Vestbo, J.; Singh, D. COVID-19 and COPD: A narrative review of the basic science and clinical outcomes. Eur. Respir. Rev. 2020, 29, 200199. [Google Scholar] [CrossRef]
- Asselta, R.; Paraboschi, E.M.; Mantovani, A.; Duga, S. ACE2 and TMPRSS2 variants and expression as candidates to sex and country differences in COVID-19 severity in Italy. Aging 2020, 12, 10087–10098. Available online: https://pubmed.ncbi.nlm.nih.gov/32501810/ (accessed on 27 May 2021). [CrossRef]
- Zhang, H.; Penninger, J.M.; Li, Y.; Zhong, N.; Slutsky, A.S. Angiotensin-converting enzyme 2 (ACE2) as a SARS-CoV-2 re-ceptor: Molecular mechanisms and potential therapeutic target. Intensive Care Med. 2020, 46, 586–590. Available online: https://pubmed.ncbi.nlm.nih.gov/32125455/ (accessed on 27 May 2021). [CrossRef] [PubMed] [Green Version]
- Klein, S.L.; Flanagan, K.L. Sex differences in immune responses. Nat. Rev. Immunol. 2016, 16, 626–638. Available online: https://pubmed.ncbi.nlm.nih.gov/27546235/ (accessed on 27 May 2021). [CrossRef] [PubMed]
- Li, S.-W.; Wang, C.-Y.; Jou, Y.-J.; Huang, S.-H.; Hsiao, L.-H.; Wan, L.; Lin, Y.-J.; Kung, S.-H.; Lin, C.-W. SARS Coronavirus papain-like protease inhibits the TLR7 signaling pathway through removing Lys63-linked polyubiquitination of TRAF3 and TRAF6. Int. J. Mol. Sci. 2016, 17, 678. Available online: https://pubmed.ncbi.nlm.nih.gov/27164085/ (accessed on 7 June 2021). [CrossRef] [PubMed] [Green Version]
- Andersson, U.; Ottestad, W.; Tracey, K.J. Extracellular HMGB1: A therapeutic target in severe pulmonary inflammation including COVID-19? Mol. Med. 2020, 26, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Hu, B.; Huang, S.; Yin, L. The cytokine storm and COVID-19. J. Med. Virol. 2021, 93, 250–256. Available online: https://pubmed.ncbi.nlm.nih.gov/32592501/ (accessed on 7 June 2021). [CrossRef]
- Pradhan, A.; Olsson, P.-E. Sex differences in severity and mortality from COVID-19: Are males more vulnerable? Biol. Sex. Differ. 2020, 11, 1–11. Available online: https://pubmed.ncbi.nlm.nih.gov/32948238/ (accessed on 10 May 2021). [CrossRef]
- Illg, Z.; Muller, G.; Mueller, M.; Nippert, J.; Allen, B. Analysis of absolute lymphocyte count in patients with COVID-19. Am. J. Emerg. Med. 2021, 46, 16–19. Available online: https://pubmed.ncbi.nlm.nih.gov/33706251/ (accessed on 31 May 2021). [CrossRef]
- Zeng, F.; Dai, C.; Cai, P.; Wang, J.; Xu, L.; Li, J.; Hu, G.; Wang, Z.; Zheng, F.; Wang, L. A comparison study of SARS-CoV-2 IgG antibody between male and female COVID-19 patients: A possible reason underlying different outcome between sex. J. Med. Virol. 2020, 92, 2050–2054. Available online: https://pubmed.ncbi.nlm.nih.gov/32383183/ (accessed on 7 June 2021). [CrossRef]
- Xu, K.; Chen, Y.; Yuan, J.; Yi, P.; Ding, C.; Wu, W.; Li, Y.; Ni, Q.; Zou, R.; Li, X.; et al. Factors associated with prolonged viral RNA shedding in patients with Coronavirus Disease 2019 (COVID-19). Clin. Infect. Dis. 2020, 71, 799–806. Available online: https://pubmed.ncbi.nlm.nih.gov/32271376/ (accessed on 7 June 2021). [CrossRef]
- Jones, T.C.; Biele, G.; Mühlemann, B.; Veith, T.; Schneider, J.; Beheim-Schwarzbach, J.; Bleicker, T.; Tesch, J.; Schmidt, M.L.; Sander, L.E.; et al. Estimating infectiousness throughout SARS-CoV-2 infection course. Science 2021, 373, eabi5273. Available online: https://www.sciencemag.org/lookup/doi/10.1126/science.abi5273 (accessed on 27 May 2021). [CrossRef]
- Lotter, H.; Altfeld, M. Sex differences in immunity. Semin. Immunopathol. 2019, 41, 133–135. Available online: https://pubmed.ncbi.nlm.nih.gov/30742253/ (accessed on 7 June 2021). [CrossRef] [Green Version]
- Gadi, N.; Wu, S.C.; Spihlman, A.P.; Moulton, V.R. What’s sex got to do with COVID-19? Gender-based differences in the host immune response to coronaviruses. Front. Immunol. 2020, 11, 2147. [Google Scholar] [CrossRef] [PubMed]
- Ajayi, A.A.L.; Mathur, R.; Halushka, P.V. Testosterone increases human platelet thromboxane A2 receptor density and aggregation responses. Circulation 1995, 91, 2742–2747. Available online: https://pubmed.ncbi.nlm.nih.gov/7758179/ (accessed on 7 June 2021). [CrossRef] [PubMed]
- Kalantar-Zadeh, K.; Ward, S.A.; Kalantar-Zadeh, K.; El-Omar, E.M. Considering the effects of microbiome and diet on SARS-CoV-2 infection: Nanotechnology roles. ACS Nano 2020, 14, 5179–5182. Available online: https://pubmed.ncbi.nlm.nih.gov/32356654/ (accessed on 7 June 2021). [CrossRef] [PubMed]
- Bimpong, K.; Thomson, K.; Mcnamara, C.L.; Balaj, M.; Akhter, N.; Bambra, C.; Todd, A. The gender pain gap: Gender inequalities in pain across 19 European countries. Scand. J. Public Health 2021. Available online: https://pubmed.ncbi.nlm.nih.gov/33568013/ (accessed on 1 June 2021). [CrossRef] [PubMed]
- Mehta, L.S.; Beckie, T.M.; DeVon, H.A.; Grines, C.L.; Krumholz, H.M.; Johnson, M.N.; Lindley, K.J.; Vaccarino, V.; Wang, T.Y.; Watson, K.E.; et al. Acute myocardial infarction in women: A scientific statement from the American Heart Association. Circulation 2016, 133, 916–947. Available online: http://circ.ahajournals.org (accessed on 7 June 2021). [CrossRef] [PubMed]
- Afifi, M. Gender differences in mental health. Singap. Med. J. 2007, 48, 385–391. Available online: https://pubmed.ncbi.nlm.nih.gov/17453094/ (accessed on 1 June 2021).
- Bambra, C.; Albani, V.; Franklin, P. COVID-19 and the gender health paradox. Scand. J. Public Health 2021, 49, 17–26. [Google Scholar] [CrossRef]
- Leythienne, D.; Ronkowski, P. A Decomposition of the Unadjusted Gender Pay Gap Using Structure of Earnings Survey Data: 2018 Edition. Available online: https://ec.europa.eu/eurostat/web/products-statistical-working-papers/-/ks-tc-18-003 (accessed on 7 June 2021).
- Davies, S.E.; Bennett, B. A gendered human rights analysis of Ebola and Zika: Locating gender in global health emergencies. Int. Aff. 2016, 92, 1041–1060. Available online: https://0-onlinelibrary-wiley-com.brum.beds.ac.uk/doi/full/10.1111/1468-2346.12704 (accessed on 7 June 2021). [CrossRef] [Green Version]
- Smith, J. Overcoming the ‘tyranny of the urgent’: Integrating gender into disease outbreak preparedness and response. Gend. Dev. 2019, 27, 355–369. Available online: https://0-www-tandfonline-com.brum.beds.ac.uk/doi/abs/10.1080/13552074.2019.1615288 (accessed on 10 May 2021). [CrossRef]
- Nowogrodzki, A. Clinical research: Inequality in medicine. Nature 2017, 550, S18–S19. Available online: https://pubmed.ncbi.nlm.nih.gov/28976953/ (accessed on 7 June 2021). [CrossRef] [Green Version]
- Shields, K.; Lyerly, A. Exclusion of pregnant women from industry-sponsored clinical trials. Obstet. Gynecol. 2013, 122, 1077–1081. Available online: https://pubmed.ncbi.nlm.nih.gov/24104789/ (accessed on 7 June 2021). [CrossRef]
- Harman, S. Ebola, gender and conspicuously invisible women in global health governance. Third World Q. 2016, 37, 524–541. Available online: https://0-www-tandfonline-com.brum.beds.ac.uk/doi/abs/10.1080/01436597.2015.1108827 (accessed on 1 June 2021). [CrossRef]
- Connor, J.; Madhavan, S.; Mokashi, M.; Amanuel, H.; Johnson, N.R.; Pace, L.E.; Bartz, D. Health risks and outcomes that disproportionately affect women during the Covid-19 pandemic: A review. Soc. Sci. Med. 2020, 266, 113364. Available online: https://0-www-sciencedirect-com.brum.beds.ac.uk/science/article/abs/pii/S0277953620305839 (accessed on 11 May 2021). [CrossRef]
- Hu, D.; Lou, X.; Meng, N.; Li, Z.; Teng, Y.; Zou, Y.; Wang, F. Influence of age and gender on the epidemic of COVID-19: Evidence from 177 countries and territories—An exploratory, ecological study. Wien. Klin. Wochenschr. 2021, 133, 321–330. Available online: https://pubmed.ncbi.nlm.nih.gov/33547492/ (accessed on 7 June 2021). [CrossRef]
- Burki, T. Global shortage of personal protective equipment. Lancet Infect. Dis. 2020, 20, 785–786. Available online: https://pubmed.ncbi.nlm.nih.gov/32592673/ (accessed on 2 June 2021). [CrossRef]
- del Río Lozano, M.; García-Calvente, M.M.; Calle-Romero, J.; Machón-Sobrado, M.; Larrañaga-Padilla, I. Health-related quality of life in Spanish informal caregivers: Gender differences and support received. Qual. Life Res. 2017, 26, 3227–3238. Available online: https://pubmed.ncbi.nlm.nih.gov/28780713/ (accessed on 7 June 2021). [CrossRef] [PubMed]
- Wang, Y.; Hunt, K.; Nazareth, I.; Freemantle, N.; Petersen, I. Do men consult less than women? An analysis of routinely collected UK general practice data. BMJ Open 2013, 3, e003320. Available online: https://pubmed.ncbi.nlm.nih.gov/23959757/ (accessed on 7 June 2021). [CrossRef] [PubMed] [Green Version]
- Ministerio de Sanidad, Consumo y Bienestar Social. Encuesta Nacional de Salud de España 2017. Available online: https://www.mscbs.gob.es/estadEstudios/estadisticas/encuestaNacional/encuestaNac2017/encuestaResDetall2017.htm (accessed on 14 June 2021).
- Czeisler, M.; Tynan, M.A.; Howard, M.E.; Honeycutt, S.; Fulmer, E.B.; Kidder, D.P.; Robbins, R.; Barger, L.K.; Facer-Childs, E.R.; Baldwin, G.; et al. Public attitudes, behaviors, and beliefs related to COVID-19, stay-at-home orders, nonessential business closures, and public health guidance—United States, New York City, and Los Angeles, May 5–12, 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 751–758. Available online: https://www.cdc.gov/mmwr/volumes/69/wr/mm6924e1.htm (accessed on 2 June 2021). [CrossRef] [PubMed]
- Gunnell, D.; Appleby, L.; Arensman, E.; Hawton, K.; John, A.; Kapur, N.; Khan, M.; O’Connor, R.C.; Pirkis, J.; COVID-19 Suicide Prevention Research Collaboration. Suicide risk and prevention during the COVID-19 pandemic. Lancet Psychiatry 2020, 7, 468–471. Available online: https://pubmed.ncbi.nlm.nih.gov/32330430/ (accessed on 3 June 2021). [CrossRef]
- Tucci, V.; Moukaddam, N.; Meadows, J.; Shah, S.; Galwankar, S.C.; Kapur, G.B. The forgotten plague: Psychiatric manifestations of ebola, zika, and emerging infectious diseases. J. Glob. Infect. Dis. 2017, 9, 151–156. Available online: https://pubmed.ncbi.nlm.nih.gov/29302150/ (accessed on 7 June 2021). [CrossRef]
- Matar, R.; Alrahmani, L.; Monzer, N.; Debiane, L.G.; Berbari, E.; Fares, J.; Fitzpatrick, F.; Murad, M.H. Clinical presentation and outcomes of pregnant women with coronavirus disease 2019: A systematic review and meta-analysis. Clin. Infect. Dis. 2021, 72, 521–533. Available online: https://pubmed.ncbi.nlm.nih.gov/32575114/ (accessed on 7 June 2021). [CrossRef] [PubMed]
- Wolfe, T.; Rodgers, Y.V.D.M. Abortion during the COVID-19 Pandemic: Racial disparities and barriers to care in the USA. Sex. Res. Soc. Policy 2021, 1–8. Available online: http://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pubmed/33777258 (accessed on 3 June 2021). [CrossRef]
- Rodriguez-Jimenez, R.; Fares-Otero, N.E.; García-Fernández, L. Gender-based violence during COVID-19 outbreak in Spain. Psychol. Med. 2020, 1–2. Available online: https://pubmed.ncbi.nlm.nih.gov/33280627/ (accessed on 3 June 2021). [CrossRef]
- Rieker, P.P.; Bird, C.E. Rethinking gender differences in health: Why we need to integrate social and biological perspectives. J. Gerontol. Ser. B 2005, 60, S40–S47. Available online: https://pubmed.ncbi.nlm.nih.gov/16251589/ (accessed on 2 June 2021). [CrossRef] [PubMed]
- Springer, K.W.; Mager Stellman, J.; Jordan-Young, R.M. Beyond a catalogue of differences: A theoretical frame and good practice guidelines for researching sex/gender in human health. Soc. Sci. Med. 2012, 74, 1817–1824. Available online: https://pubmed.ncbi.nlm.nih.gov/21724313/ (accessed on 7 June 2021). [CrossRef] [PubMed]
- Redondo-Bravo, L.; Moros, M.J.S.; Sanchez, E.V.M.; Lorusso, N.; Ubago, A.C.; Garcia, V.G.; Villanueva, P.S.; Azón, A.P.; Bescós, J.G.; Boone, A.L.; et al. The first wave of the COVID-19 pandemic in Spain: Characterisation of cases and risk factors for severe outcomes, as at 27 April 2020. Eurosurveillance 2020, 25, 2001431. Available online: https://pubmed.ncbi.nlm.nih.gov/33334400/ (accessed on 12 April 2021).
- Peinado, F. Así fue el tapón a las Residencias de Mayores de Madrid, Hospital por Hospital: El 73% de Muertos no Fueron Trasladados a un Centro Médico. EL PAÍS 7 June 2021. Available online: https://elpais.com/espana/elecciones-madrid/2021-05-01/asi-fue-el-tapon-a-las-residencias-de-mayores-de-madrid-hospital-por-hospital-el-73-de-muertos-no-fue-trasladado.html (accessed on 7 June 2021). (In Spanish).
- Spagnolo, P.A.; Manson, J.E.; Joffe, H. Sex and gender differences in health: What the COVID-19 pandemic can teach us. Ann. Intern. Med. 2020, 173, 385–386. Available online: https://www.acpjournals.org/doi/abs/10.7326/m20-1941 (accessed on 26 May 2021). [CrossRef]
- Bambra, C.; Riordan, R.; Ford, J.; Matthews, F. The COVID-19 pandemic and health inequalities. J. Epidemiol. Community Health 2020, 74, 964–968. Available online: https://pubmed.ncbi.nlm.nih.gov/32535550/ (accessed on 7 June 2021). [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Total (n = 968) | Men, Dead (n = 101) | Men, Alive (n = 429) | p Value (men) a | Women, Dead (n = 70) | Women, Alive (n = 368) | p Value (women) a |
|---|---|---|---|---|---|---|---|
| Age, years | <0.001 | < 0.001 | |||||
| <40 | 44 (5.5%) | 0 (0.0%) | 19 (4.4%) | 1 (1.4%) | 25 (6.8%) | ||
| 40–49 | 93 (11.7%) | 2 (2.0%) | 50 (11.7%) | 0 (0.0%) | 43 (11.7%) | ||
| 50–59 | 181 (22.7%) | 8 (7.9%) | 100 (23.3%) | 0 (0.0%) | 81 (22.0%) | ||
| 60–69 | 207 (26.0%) | 16 (15.8%) | 120 (28.0%) | 6 (8.6%) | 88 (23.9%) | ||
| 70–79 | 164 (20.6%) | 30 (29.7%) | 94 (21.9%) | 15 (21.4%) | 69 (18.8%) | ||
| 80–89 | 95 (11.9%) | 32 (31.7%) | 39 (9.1%) | 33 (47.1%) | 56 (15.2%) | ||
| ≥90 | 13 (1.6%) | 13 (12.9%) | 7 (1.6%) | 15 (21.4%) | 6 (1.6%) | ||
| Mean (IQR) | 67 (55–77) | 77 (68–84) | 63 (54–72) | 83 (77.5–88) | 63 (52–75) | ||
| Country of birth | 0.509 | 0.392 | |||||
| Non-native | 36 (3.9%) | 1 (1.0%) | 34 (4.4%) | 1 (1.5%) | 19 (5.4%) | ||
| Centre | 0.257 | 0.692 | |||||
| Granada (SCUH) | 441 (45.6%) | 52 (51.5%) | 191 (44.5%) | 28 (40.0%) | 170 (46.2%) | ||
| Jaén (CJUH) | 270 (45.6%) | 26 (25.7%) | 125 (29.1%) | 20 (28.6%) | 99 (26.9%) | ||
| Córdoba (RSUH) | 220 (22.7%) | 16 (15.8%) | 95 (22.1%) | 19 (27.1%) | 90 (24.5%) | ||
| Cádiz (PRUH) | 37 (3.8%) | 7 (6.9%) | 18 (4.2%) | 3 (4.3%) | 9 (2.5%) | ||
| Dependence in activities of daily living | 207 (21.5%) | 41 (41.0%) | 53 (12.4%) | <0.001 | 47 (68.1%) | 66 (18.0%) | <0.001 |
| Place of residence | |||||||
| Living at home | 826 (85.6%) | 72 (72.7%) | 393 (91.8%) | <0.001 | 42 (60.0%) | 319 (86.7%) | <0.001 |
| Nursing homes | 104 (10.9%) | 24 (24.2%) | 17 (4.0%) | <0.001 | 26 (37.7%) | 37 (11.5%) | <0.001 |
| Institutions for disabled people | 39 (4.1%) | 3 (3.1%) | 20 (4.7%) | 0.594 | 3 (4.3%) | 13 (3.6%) | 0.731 |
| Missing data | 33 (3.4%) | ||||||
| Chronic conditions | |||||||
| No. of chronic conditions; median (IQR) | 1 (0–2) | 2 (1–4) | 1 (0–2) | <0.001 | 2 (1–4) | 1 (0–2) | <0.001 |
| Arterial hypertension | 542 (56.0%) | 75 (74.3%) | 226 (52.7%) | <0.001 | 56 (80.0%) | 185 (50.3%) | <0.001 |
| Diabetes mellitus | 226 (23.3%) | 32 (31.7%) | 95 (22.1%) | 0.059 | 27 (38.6%9 | 72 (19.6%) | <0.001 |
| Cardiovascular disease | 243 (25.1%) | 46 (45.5%) | 101 (23.5%) | <0.001 | 32 (45.7%) | 64 (17.4%) | <0.001 |
| Chronic lung disease | 154 (15.9%) | 29 (28.7%) | 62 (14.5%) | 0.001 | 19 (27.1%) | 44 (12.0%) | 0.002 |
| COPD | 65 (6.7%) | 21 (20.8%) | 36 (8.4%) | <0.001 | 4 (5.7%) | 4 (1.1%) | 0.025 |
| Asthma | 69 (7.1%) | 6 (5.9%) | 24 (5.6%) | 1.000 | 4 (5.7%) | 35 (9.5%) | 0.428 |
| Chronic kidney disease | 112 (11.6%) | 21 (20.8%) | 41 (9.6%) | 0.003 | 23 (32.9%) | 27 (7.3%) | <0.001 |
| Autoimmune disease | 74 (7.6%) | 9 (8.9%) | 22 (5.1%) | 0.222 | 4 (5.7%) | 39 (10.6%) | 0.299 |
| Immunosuppression | 41 (4.2%) | 4 (4.0%) | 16 (3.7%) | 1.000 | 7 (10.0%) | 14 (3.8%) | 0.059 |
| Polymedication (≥6 drugs prior to admission) | 403 (42.6%) | 59 (59.6%) | 152 (36.3%) | <0.001 | 49 (72.1%) | 143 (39.7%) | <0.001 |
| Missing data | 22 (2.3%) | ||||||
| Active cancer | 50 (5.2%) | 14 (13.9%) | 20 (4.7%) | 0.002 | 4 (5.7%) | 12 (3.3%) | 0.301 |
| History of cancer in the previous 5 years | 62 (6.4%) | 9 (8.9%) | 35 (8.2%) | 0.963 | 6 (8.6%) | 12 (3.3%) | 0.051 |
| Solid organ or HSC transplantation | 10 (1.0%) | 0 (0.0%) | 6 (1.4%) | 0.601 | 2 (2.9%) | 2 (0.5%) | 0.122 |
| In-hospital variables | |||||||
| Length of stay (days); median (IQR) | 11 (7–17) | 8 (4–15) | 12 (8–18) | <0.001 | 6 (4–11) | 10 (7–17) | <0.001 |
| Length of ICU stay (days); median (IQR) | 12 (6–3.25) | 13 (9–26) | 13 (5.5–30) | 0.533 | 10 (6–13) | 12 (4.5–15) | 0.840 |
| Abnormal admission chest X-ray | 801 (87.8%) | 80 (89.9%) | 373 (90.3%) | 0.941 | 53 (85.5%) | 295 (84.8%) | 0.962 |
| Ferritin upon admission (µg/L); median (IQR) | 478.2 (246.8–866.7) | 732.8 (453.4–1229.9) | 654.0 (393.1–1093.8) | 0.109 | 349.6 (149.0–712.8) | 277.2 (132.7–505.5) | 0.123 |
| CURB-65 score upon admission; median (IQR) | 1 (0–2) | 2 (1–3) | 1 (0–1) | <0.001 | 2 (2–3) | 1 (0–2) | <0.001 |
| Low risk (CURB-65 = 0–1) | 493 (63.3%) | 22 (25.9%) | 252 (76.9%) | 9 (16.1%) | 209 (73.3%) | ||
| Medium risk (CURB-65 = 2) | 186 (24.6%) | 34 (40.0%) | 62 (18.8%) | 23 (41.1%) | 67 (23.5%) | ||
| High risk (CURB-65 = 3–5) | 76 (10.1%) | 29 (34.1%) | 14 (4.3%) | 24 (42.9%) | 9 (3.2%) | ||
| Missing data | 213 (22.0%) | ||||||
| Concurrent infection | 166 (22.0%) | 41 (51.3%) | 66 (20.2%) | <0.001 | 13 (25.0%) | 46 (15.6%) | 0.143 |
| Missing data | 214 (22.1%) | ||||||
| Hydroxychloroquine | 804 (86.3%) | 61 (64.2%) | 381 (92.3%) | <0.001 | 39 (58.2%) | 323 (90.5%) | <0.001 |
| Missing data | 36 (3.7%) | ||||||
| High-dose corticosteroids | 362 (41.1%) | 50 (55.6%) | 182 (46.4%) | 0.148 | 27 (42.2%) | 103 (30.8%) | 0.100 |
| Missing data | 87 (9.0%) | ||||||
| Lopinavir-ritonavir | 569 (62.0%) | 54 (56.8%) | 278 (68.0%) | 0.052 | 26 (39.4%) | 211 (60.6%) | 0.002 |
| Missing data | 50 (5.2%) | ||||||
| Azithromycin | 680 (74.6%) | 48 (53.3%) | 317 (77.9%) | <0.001 | 30 (47.6%) | 285 (81.0%) | <0.001 |
| Missing data | 56 (5.8%) | ||||||
| Other antibiotics | 581 (65.1%) | 63 (70.8%) | 268 (67.9%) | 0.680 | 41 (64.1%) | 209 (60.8%) | 0.720 |
| Missing data | 76 (7.9%) | ||||||
| Tocilizumab | 100 (11.8%) | 14 (16.1%) | 58 (15.6%) | 0.982 | 4 (6.8%) | 24 (7.3%) | 0.890 |
| Missing data | 120 (12.4%) | ||||||
| Invasive mechanical ventilation | 81 (8.4%) | 23 (22.8%) | 34 (7.9%) | <0.001 | 7 (10.0%) | 17 (4.6%) | 0.084 |
| Non-invasive mechanical ventilation | 88 (9.1%) | 11 (10.9%) | 49 (11.4%) | 1.000 | 4 (5.7%) | 24 (6.5%) | 1.000 |
| ICU admission | 117 (12.1%) | 25 (24.8%) | 56 (13.1%) | 0.005 | 9 (12.9%) | 27 (7.3%) | 0.192 |
| Predictors | Crude HR a (95% CI) b | p Value c | Adjusted HR (95% CI) | p Value c |
|---|---|---|---|---|
| Men | ||||
| Age (years) | 1.08 (1.06–1.10) | <0.001 | 1.05 (1.02–1.07) | <0.001 |
| Active cancer | 2.26 (1.28–3.98) | 0.005 | 2.78 (1.37–5.65) | 0.005 |
| Autoimmune disease | 1.73 (0.87–3.43) | 0.119 | 3.22 (1.55–6.69) | 0.002 |
| CURB-65 score | 2.32 (1.88–2.86) | <0.001 | 1.64 (1.28–2.11) | <0.001 |
| Azithromycin treatment | 0.38 (0.61–2.30) | <0.001 | 0.53 (0.33–0.84) | 0.008 |
| Women | ||||
| Age (years) | 1.09 (1.07–1.12) | <0.001 | 1.06 (1.02–1.09) | 0.002 |
| Cardiovascular disease | 3.00 (1.86–4.82) | <0.001 | 1.80 (1.02–3.18) | 0.044 |
| Chronic lung disease | 1.76 (1.02–3.02) | 0.042 | 1.84 (1.01–3.36) | 0.045 |
| CURB-65 score | 3.31 (2.54–4.32) | <0.001 | 2.67 (1.93–3.69) | <0.001 |
| Azithromycin treatment | 0.24 (0.15–0.40) | <0.001 | 0.50 (0.29–0.88) | 0.016 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fernández-Martínez, N.F.; Ortiz-González-Serna, R.; Serrano-Ortiz, Á.; Rivera-Izquierdo, M.; Ruiz-Montero, R.; Pérez-Contreras, M.; Guerrero-Fernández de Alba, I.; Romero-Duarte, Á.; Salcedo-Leal, I. Sex Differences and Predictors of In-Hospital Mortality among Patients with COVID-19: Results from the ANCOHVID Multicentre Study. Int. J. Environ. Res. Public Health 2021, 18, 9018. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18179018
Fernández-Martínez NF, Ortiz-González-Serna R, Serrano-Ortiz Á, Rivera-Izquierdo M, Ruiz-Montero R, Pérez-Contreras M, Guerrero-Fernández de Alba I, Romero-Duarte Á, Salcedo-Leal I. Sex Differences and Predictors of In-Hospital Mortality among Patients with COVID-19: Results from the ANCOHVID Multicentre Study. International Journal of Environmental Research and Public Health. 2021; 18(17):9018. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18179018
Chicago/Turabian StyleFernández-Martínez, Nicolás Francisco, Rocío Ortiz-González-Serna, Álvaro Serrano-Ortiz, Mario Rivera-Izquierdo, Rafael Ruiz-Montero, Marina Pérez-Contreras, Inmaculada Guerrero-Fernández de Alba, Álvaro Romero-Duarte, and Inmaculada Salcedo-Leal. 2021. "Sex Differences and Predictors of In-Hospital Mortality among Patients with COVID-19: Results from the ANCOHVID Multicentre Study" International Journal of Environmental Research and Public Health 18, no. 17: 9018. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18179018