
Assessing the Impact of Integrated Community-Based Management of Severe Wasting Programs in Conflict-Stricken South Sudan: A Multi-Dimensional Approach to Scalability of Nutrition Emergency Response Programs

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source and Procedures
2.2. Study Outcomes
2.2.1. CMSW Program Scalability
- Intervention delivery pathways and harmonisation of implementation plans;
- Delivery system (reach, adoption, and expansion);
- Provision of technical assistance and strong organisational capacity at all levels CMSW program implementation;
- Integrating approaches within government systems, policies, priorities, and targets;
- Generating and disseminating evidence to inform policy and programs;
- Engaging communities as co-designers and co-implementers (ownership);
- Using monitoring and evaluation systems to extract lessons learnt;
- Building an enabling environment and strengthening the decision support;
- Facilitating partnerships and integration;
- Delineation of roles and responsibilities;
- Funding and financial sustainability.
2.2.2. Emergency Preparedness and Wasting Prevention
2.2.3. CMSW Performance
- Recovered: children discharged after a successful recovery. It is calculated as the number of children recovered/total number of discharged × 100;
- Died: children who died during treatment in CMSW programs. It is calculated as the number of deaths/total number of discharged × 100;
- Defaulted: children who did not complete treatment due to absenteeism (absent during three consecutive visits, defaulter confirmed at third absence). It is calculated as the number of defaulters/total number of discharged ×100;
- Medical transfers: children referred to hospital or health facility children outside nutritional programs for further medical investigation or medical treatment. It is calculated as the number of medical transfers/total number of discharged × 100;
- Not recovered: children who did not meet the discharge criteria for recovery after four months of treatment. It is calculated as the number of individuals not recovered/total number of discharged × 100;
- Relapse: children who completed treatment and discharged as “recovered” but developed severe wasting within a period of two months and got readmitted for further treatment. It is calculated as the number of relapse/total admission ×100;
- Weight gain velocity: calculated as weight gain (weight at discharge − weight at admission in grams)/(the weight on admission in Kilograms × length of stay in the program); expressed as g/kg/person/day;
- Length of stay: calculated as the date at discharge minus the date at admission, expressed in days.
2.3. Data Analysis
3. Results
3.1. CMSW Scalability
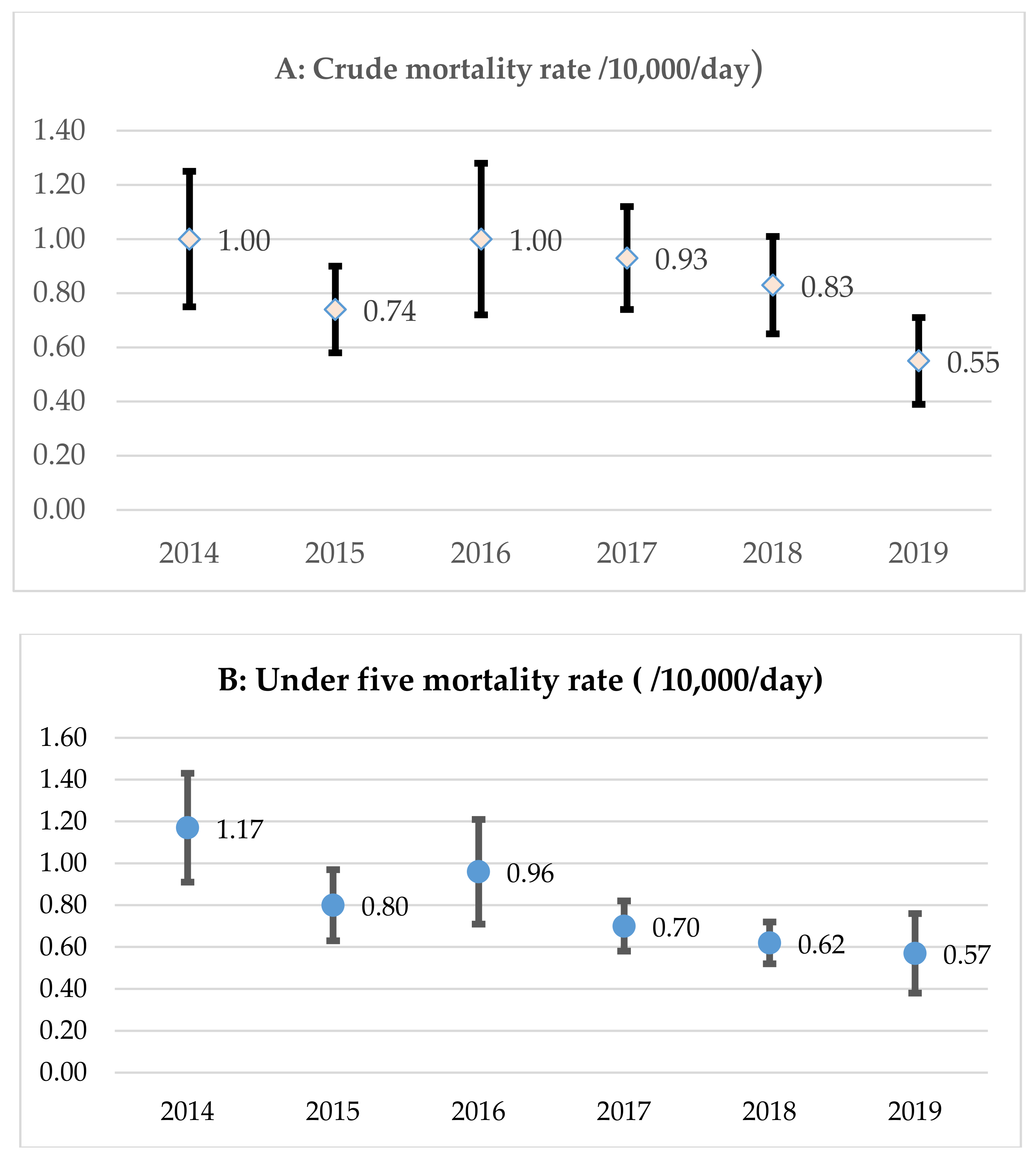
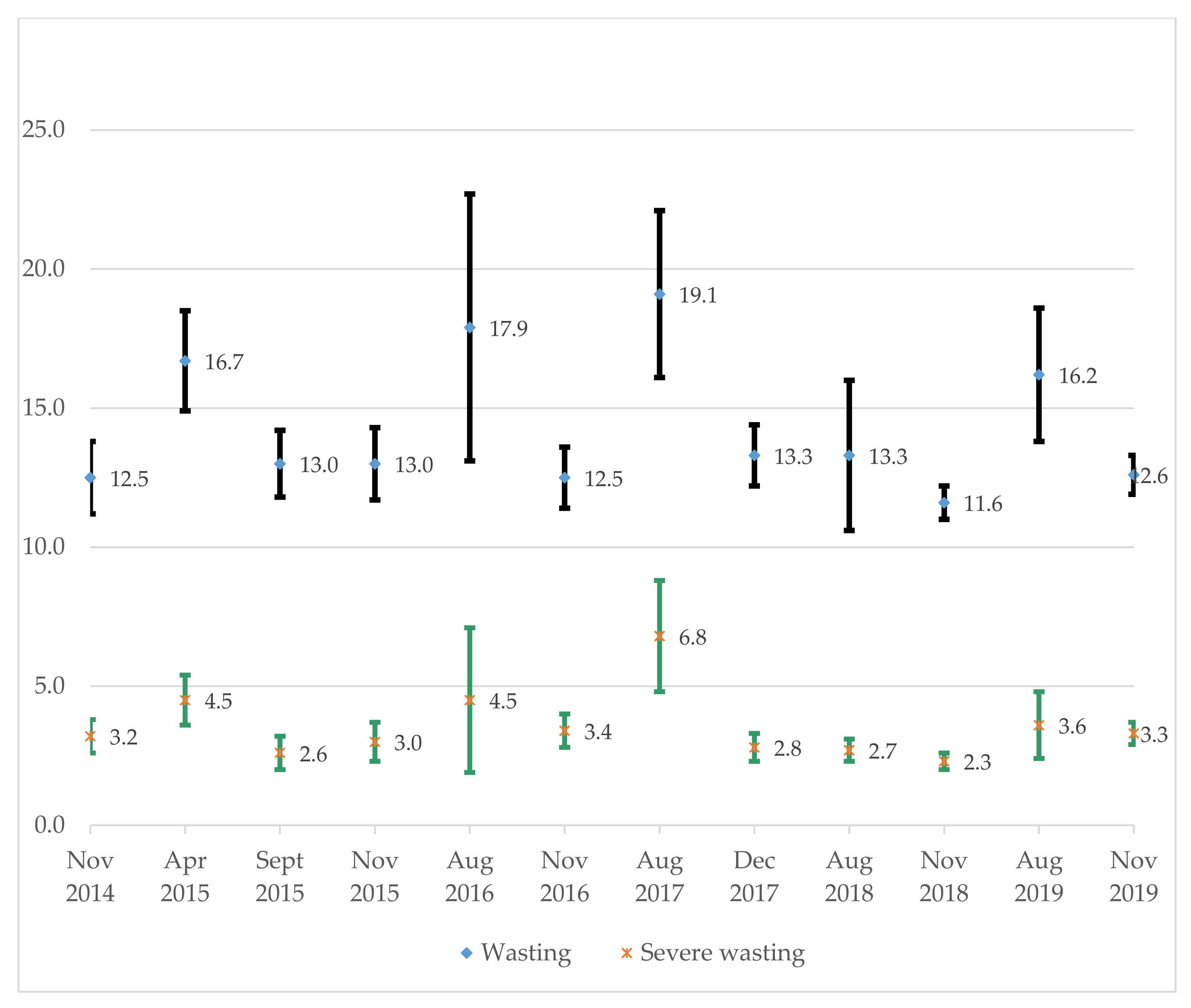
3.2. Severe Wasting Prevention and Nutrition Emergency Preparedness
3.3. Performance of CMSW
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rolandsen, Ø.H. Another civil war in South Sudan: The failure of guerrilla government? J. East. Afr. Stud. 2015, 9, 163–174. [Google Scholar] [CrossRef] [Green Version]
- Kindersley, N.; Rolandsen, Ø.H. Who are the civilians in the wars of South Sudan? Secur. Dialogue 2019, 50, 383–397. [Google Scholar] [CrossRef]
- De Waal, A. When kleptocracy becomes insolvent: Brute causes of the civil war in South Sudan. Afr. Aff. 2014, 113, 347–369. [Google Scholar] [CrossRef]
- Pinaud, C. Military Kinship, Inc.: Patronage, inter-ethnic marriages and social classes in South Sudan. Rev. Afr. Political Econ. 2016, 43, 243–259. [Google Scholar] [CrossRef]
- Food and Agriculture Organization of the United Nations; World Food Programme. Special Report-2020 FAO/WFP Crop and Food Security Assessment Mission (CFSAM) to the Republic of South Sudan; FAO: Rome, Italy, 2021. [Google Scholar] [CrossRef]
- Food and Agriculture Organization of the United Nations. Global Information and Early Warning System on Food and Agriculture Country Brief: South Sudan; FAO: Rome, Italy, 2021; Available online: http://www.fao.org/giews/country-analysis/country-briefs/country/SSD/pdf/SSD.pdf (accessed on 20 May 2021).
- International Monetary Fund. Inflation, Consumer Prices (Annual %)-South Sudan. International Financial Statistics and Data Files. 2021. Available online: https://data.worldbank.org/indicator/FP.CPI.TOTL.ZG?locations=SS&most_recent_value_desc=false (accessed on 2 August 2021).
- Food and Agriculture Organization of the United Nations. Special Report–2019 FAO/WFP Crop and Food Security Assessment Mission to the Republic of South Sudan. CFSAMs Special Reports–May 2020. 2020. Available online: https://0-doi-org.brum.beds.ac.uk/10.4060/ca9282en (accessed on 2 August 2021).
- Food Security Information Network; Global Network Against Food Crisis. Global Report on Food Crises: Joint Analysis for Better Decisions. 2021. Available online: https://www.fsinplatform.org/sites/default/files/resources/files/GRFC%202021%20050521%20med.pdf (accessed on 25 June 2021).
- Coates, J.; Swindale, A.; Bilinsky, P. Household Food Insecurity Access Scale (HFIAS) for Measurement of Food Access: Indicator Guide; FHI 360/FANTA: Washington, DC, USA, 2007. [Google Scholar]
- Young, H.; Marshak, A. Persistent Global Acute Malnutrition; Feinstein International Center, Tufts University: Boston, MA, USA, 2017. [Google Scholar]
- FAO; Unicef; WFP. Food Security and Nutrition Monitoring Report (FSNMS), Round 24-December 2019: South Sudan. 2019. Available online: https://fscluster.org/sites/default/files/documents/fsnms_r24_report_dec_2019.pdf (accessed on 12 August 2021).
- Sphere Association. The Sphere Handbook: Humanitarian Charter and Minimum Standards in Humanitarian Response, 4th ed.; Sphere Association: Geneva, Switzerland, 2018; p. 36. Available online: www.spherestandards.org/handbook (accessed on 15 July 2021).
- Olofin, I.; McDonald, C.M.; Ezzati, M.; Flaxman, S.; Black, R.E.; Fawzi, W.W.; Caulfield, L.E.; Danaei, G.; For the Nutrition Impact Model Study. Associations of suboptimal growth with all-cause and cause-specific mortality in children under five years: A pooled analysis of ten prospective studies. PLoS ONE 2013, 8, e64636. [Google Scholar] [CrossRef] [Green Version]
- Collins, S.; Dent, N.; Binns, P.; Bahwere, P.; Sadler, K.; Hallam, A. Management of severe acute malnutrition in children. Lancet 2006, 368, 1992–2000. [Google Scholar] [CrossRef]
- Collins, S. Treating severe acute malnutrition seriously. Arch. Dis. Child. 2007, 92, 453–461. [Google Scholar] [CrossRef]
- Van Roosmalen-Wiebenga, M.; Kusin, J.; De With, C. Nutrition rehabilitation in hospital—A waste of time and money? Evaluation of nutrition rehabilitation in a rural district hospital in South-West Tanzania. II. Long-term results. J. Trop. Pediatrics 1987, 33, 24–28. [Google Scholar] [CrossRef]
- Collins, S. Changing the way we address severe malnutrition during famine. Lancet 2001, 358, 498–501. [Google Scholar] [CrossRef]
- Dent, N.; Deconinck, H.; Golden, K.; Brown, R.; Walsh, A. Information-sharing to improve learning about community-based management of acute malnutrition (CMAM) and its impact. Food Nutr. Bull. 2014, 35 (Suppl. S1), S86–S89. [Google Scholar] [CrossRef] [Green Version]
- Ashworth, A. Community-Based Rehabilitation of Severely Malnourished Children: A Review of Successful Programmes; London School of Hygiene and Tropical Medicine: London, UK, 2001. [Google Scholar]
- Ashworth, A. Efficacy and effectiveness of community-based treatment of severe malnutrition. Food Nutr. Bull. 2006, 27 (Suppl. S1), S24–S48. [Google Scholar] [CrossRef]
- Chitekwe, S.; Biadgilign, S.; Tolla, A.; Myatt, M. Mid-upper-arm circumference based case-detection, admission, and discharging of under five children in a large-scale community-based management of acute malnutrition program in Nigeria. Arch. Public Health 2018, 76, 19. [Google Scholar] [CrossRef] [Green Version]
- Yebyo, H.G.; Kendall, C.; Nigusse, D.; Lemma, W. Outpatient therapeutic feeding program outcomes and determinants in treatment of severe acute malnutrition in Tigray, northern Ethiopia: A retrospective cohort study. PLoS ONE 2013, 8, e65840. [Google Scholar] [CrossRef] [Green Version]
- Burright, M. Database Reviews and Reports. Issues Sci. Technol. Librariansh. 2006, 45. Available online: http://www.istl.org/06-winter/databases2.html (accessed on 21 July 2021). [CrossRef]
- UNICEF; ACF. Nutrition Surveys and SMART Methodology in Sub-Saharan Africa. 2016. Available online: https://www.unicef.org/esa/sites/unicef.org.esa/files/2018-09/UNICEF-AAH-2016-SMART-Analytical-Report-Sub-Saharan-Africa.pdf (accessed on 12 August 2021).
- Milat, A.; Lee, K.; Conte, K.; Grunseit, A.; Wolfenden, L.; van Nassau, F.; Orr, N.; Sreeram, P.; Bauman, A. Intervention Scalability Assessment Tool: A decision support tool for health policy makers and implementers. Health Res. Policy Syst. 2020, 18, 1–17. [Google Scholar] [CrossRef] [Green Version]
- Girum, T.; Muktar, E.; Worku, A. Comparative analysis of the survival status and treatment outcome of under-five children admitted with severe acute malnutrition among hospital-based and health center based stabilization centers, south Ethiopia. Open Public Health J. 2018, 11, 209–220. [Google Scholar] [CrossRef]
- UNICEF. Emergency Nutrition Response in Ethiopia. 2019. Available online: https://www.unicef.org/ethiopia/media/1331/file/Nutrition%20Emergency%20Response%20in%20Ethiopia%20.pdf (accessed on 21 June 2021).
- Kabalo, M.Y.; Seifu, C.N. Treatment outcomes of severe acute malnutrition in children treated within Outpatient Therapeutic Program (OTP) at Wolaita Zone, Southern Ethiopia: Retrospective cross-sectional study. J. Health Popul. Nutr. 2017, 36, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Abate, B.B.; Tilahun, B.D.; Kassie, A.M.; Kassaw, M.W. Treatment outcome of Severe Acute Malnutrition and associated factors among under-five children in outpatient therapeutics unit in Gubalafto Wereda, North Wollo Zone, Ethiopia, 2019. PLoS ONE 2020, 15, e0238231. [Google Scholar] [CrossRef]
- Government of South Sudan. Community Management of Acute Malnutrition (CMAM) Guidelines; Ministry of Health, Government of South Sudan: Juba, South Sudan, 2017. [Google Scholar]
- Clarke, V.; Braun, V. Thematic analysis. In Encyclopedia of Critical Psychology; Springer: Berlin/Heidelberg, Germany, 2014; pp. 1947–1952. [Google Scholar]
- Percy, W.H.; Kostere, K.; Kostere, S. Generic qualitative research in psychology. Qual. Rep. 2015, 20, 76–85. [Google Scholar]
- Israel, B.; Schulz, A.; Parker, E.; Becker, A. Review of community-based research: Assessing partnership approaches to improve public health. Annu. Rev. Public Health 1998, 19, 173–202. [Google Scholar] [CrossRef] [Green Version]
- Amadi, B.; Imikendu, M.; Sakala, M.; Banda, R.; Kelly, P. Integration of HIV care into community management of acute childhood malnutrition permits good outcomes: Retrospective analysis of three years of a programme in Lusaka. PLoS ONE 2016, 11, e0149218. [Google Scholar] [CrossRef]
- Fullman, N.; Yearwood, J.; Abay, S.M.; Abbafati, C.; Abd-Allah, F. Measuring performance on the Healthcare Access and Quality Index for 195 countries and territories and selected subnational locations: A systematic analysis from the Global Burden of Disease Study 2016. Lancet 2018, 391, 2236–2271. [Google Scholar] [CrossRef]
- Valadez, J.J.; Berendes, S.; Odhiambo, J.; Vargas, W.; Devkota, B.; Lako, R.; Jeffery, C. Is development aid to strengthen health systems during protracted conflict a useful investment? The case of South Sudan, 2011–2015. BMJ Global Health 2020, 5, e002093. [Google Scholar] [CrossRef]
- Collins, S.; Sadler, K.; Dent, N.; Khara, T.; Guerrero, S.; Myatt, M.; Saboya, M.; Walsh, A. Key issues in the success of community-based management of severe malnutrition. Food Nutr. Bull. 2006, 27 (Suppl. S3), S49–S82. [Google Scholar] [CrossRef]
- Maleta, K.; Amadi, B. Community-based management of acute malnutrition (CMAM) in sub-Saharan Africa: Case studies from Ghana, Malawi, and Zambia. Food Nutr. Bull. 2014, 35 (Suppl. S1), S34–S38. [Google Scholar] [CrossRef]
- Lenters, L.M.; Wazny, K.; Webb, P.; Ahmed, T.; Bhutta, Z.A. Treatment of severe and moderate acute malnutrition in low-and middle-income settings: A systematic review, meta-analysis and Delphi process. BMC Public Health 2013, 13, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Stobaugh, H.C.; Mayberry, A.; McGrath, M.; Bahwere, P.; Zagre, N.M.; Manary, M.J.; Black, R.; Lelijveld, N. Relapse after severe acute malnutrition: A systematic literature review and secondary data analysis. Matern. Child Nutr. 2019, 15, e12702. [Google Scholar] [CrossRef] [PubMed]
- Jones, K.D.; Berkley, J.A. Severe acute malnutrition and infection. Paediatr. Int. Child Health 2014, 34 (Suppl. S1), S1–S29. [Google Scholar] [CrossRef]
- Musoke, P.M.; Fergusson, P. Severe malnutrition and metabolic complications of HIV-infected children in the antiretroviral era: Clinical care and management in resource-limited settings. Am. J. Clin. Nutr. 2011, 94, 1716S–1720S. [Google Scholar] [CrossRef] [Green Version]
- Roberfroid, D.; Hammami, N.; Lachat, C.; Weise Prinzo, Z.; Sibson, V.; Guesdon, B.; Goosens, S.; Kolsteren, P. Utilization of Mid-Upper Arm Circumference Versus Weight-For-Height in Nutritional Rehabilitation Programmes: A Systematic Review of Evidence; Institut of Tropical Medicine: Antwerp, Belgium, 2013; Available online: https://www.who.int/nutrition/publications/guidelines/updates_management_SAM_infantandchildren_review1.pdf (accessed on 20 May 2021).
- Aguayo, V.M.; Badgaiyan, N.; Qadir, S.S.; Bugti, A.N.; Alam, M.M.; Nishtar, N.; Galvin, M. Community management of acute malnutrition (CMAM) programme in P akistan effectively treats children with uncomplicated severe wasting. Matern. Child Nutr. 2018, 14, e12623. [Google Scholar] [CrossRef] [Green Version]
- Burza, S.; Mahajan, R.; Marino, E.; Sunyoto, T.; Shandilya, C.; Tabrez, M.; Kumari, K.; Mathew, P.; Jha, A.; Salse, N. Community-based management of severe acute malnutrition in India: New evidence from Bihar. Am. J. Clin. Nutr. 2015, 101, 847–859. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Scaling up Process | Operational Documents | Implementation Plans/Reports | Strategic Plan | Monitoring and Evaluation Plans and Documents | National Guidelines | Field and Assessment Reports |
|---|---|---|---|---|---|---|
| Intervention delivery pathways and harmonisation of implementation plans | × | √ | × | √ | √ | √ |
| Delivery system: reach, adoption, and expansion | √ | √ | √ | √ | √ | √ |
| Providing technical assistance and strong organisational capacity at all levels | √ | √ | √ | √ | √ | × |
| Integrating approaches within government systems, policies, priorities, and targets | × | √ | × | × | √ | × |
| Generating and disseminating evidence (effectiveness) | × | √ | × | √ | × | √ |
| Engaging communities as co-designers and co-implementers (ownership) | × | × | × | × | × | × |
| Using monitoring and evaluation systems to inform practice and policy | √ | √ | √ | √ | √ | √ |
| Building an enabling environment and strengthening the decision support | √ | √ | √ | √ | √ | √ |
| Facilitating partnerships and integration | √ | √ | √ | √ | √ | √ |
| Delineation of roles and responsibilities | √ | √ | √ | √ | √ | √ |
| Funding and financial sustainability | × | × | × | × | × | × |
| Domain | Indicator | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | 2020 |
|---|---|---|---|---|---|---|---|---|
| Infant and young child feeding (IYCF) practices (N) | ||||||||
| Target: IYCF counselling for primary caregivers of children aged 0–23 months | No target | 230,698 | 567,366 | 590,134 | 1,201,386 | 984,701 | 1,098,241 | |
| Trained: IYCF counselling for primary caregivers of children aged 0–23 months | 118,216 (N/A) | 539,547 (233.9%) | 724,500 (127.7%) | 607,539 (102.9%) | 950,376 (79.1%) | 1,684,197 (171.0%) | 1,644,323 (149.7%) | |
| # of Government and NGO partner staff and health workers trained in IYCF | No data | 3000 | 2990 | 1885 | 2831 | 4189 | 3408 | |
| % counties that have carried out vitamin A supplementation (79 counties) | 43% | 51% | 43% | 61% | 91% | 98.7% | 84.8% | |
| Nutrition Emergency Preparedness and Response (N) | ||||||||
| Outpatient therapeutic program sites established | 351 | 462 | 580 | 736 | 858 | 1145 | 1171 | |
| UNICEF IRRM missions | 37 | 59 | 34 | 66 | 50 | 32 | 11 | |
| Children aged 6–59 months screened for wasting during IRRM missions | 92,715 | 131,545 | 84,099 | 114,674 | 76,550 | 65,869 | 11,110 | |
| Wasted children treated during IRRM missions * | 2886 (3.1%) | 1275 (1.0%) | 382 (0.5%) | 1797 (1.6%) | 1110 (1.5%) | 557 0.8%) | 367 (3.3%) | |
| Caregivers receiving maternal and child nutrition education during IRRM missions | 20,478 | 35,804 | 19,992 | 55,052 | 35,350 | 11,640 | 10,332 | |
| Children aged 6–59 months supplemented with Vitamin A during IRRM missions | 47,057 (50.8%) | 74,808 (56.9%) | 24,772 (29.5%) | 52,999 (46.2%) | 45,178 (59.0%) | 42,479 (65.5%) | 5543 (49.9%) | |
| 12–59 month-old children who received deworming tablets during IRRM missions | 40,355 (43.5%) | 62,278 (47.3%) | 27,861 (33.1%) | 44,301 (38.6%) | 34,211 (44.7%) | 34,369 (52.2%) | 6204 (55.8%) | |
| Evidence based nutrition intervention: | ||||||||
| Average reporting rate of outpatient therapeutic program (%) | NA | NA | 86% | 90% | 95% | 95% | 95% | |
| SMART surveys validated by UNICEF/Nutrition Information Working Group | 42 (100%) | 59 (100%) | 56 (100%) | 55 (100%) | 55 (100%) | 28 (100%) | 5 (100%) | |
| Existence of a national costed nutrition strategic plan | No | No | No | No | No | RD ** | RD ** | |
| Existence of a national management information system | Yes | Yes | Yes | Yes | Yes | Yes | ||
| Indicators | 2016 | 2017 | 2018 | 2019 | 2020 | All Years | Minimum Standards * |
|---|---|---|---|---|---|---|---|
| Sex | |||||||
| Girls | |||||||
| Total admissions, N | 112,487 | 113,962 | 110,751 | 129,873 | 109,741 | 576,814 | |
| Total exits, N | 92,241 (82.00) | 90,487 (79.40) | 93,322 (84.26) | 111,416 (85.79) | 91,935 (83.77) | 479,401 (83.11) | |
| Relapse rate [mean (SD] ** | 1.30 (2.28) | 2.31 (5.67) | 1.85 (3.30) | 2.48 (3.59) | 2.22 (3.35) | 2.06 (3.83) | <10% |
| Exits [mean (SD] | |||||||
| Recovered | 83.93 (18.55) | 83.89 (18.21) | 86.95 (17.73) | 89.38 (14.10) | 90.94 (15.06) | 87.22 (16.92) | >75% |
| Died | 1.16 (3.50) | 1.86 (5.72) | 2.32 (9.32) | 1.96 (8.50) | 1.61 (5.21) | 1.81 (6.92) | <10% |
| Defaulters | 7.48 (11.83) | 6.91 (12.77) | 4.58 (7.20) | 3.87 (5.77) | 2.19 (3.27) | 4.85 (8.87) | <15% |
| Not- recovered | 1.95 (3.50) | 1.8 (5.01) | 2 (7.93) | 1.47 (2.44) | 1 (2.06) | 1.63 (4.76) | |
| Transferred | 5.49 (13.04) | 5.54 (12.8) | 4.15 (11.02) | 3.33 (10.17) | 4.26 (14.37) | 4.50 (12.34) | |
| Weight gain velocity | 3.51 (2.91) | 1.09 (2.20) | 2.86 (5.02) | 4.17 (4.11) | 3.30 (2.68) | 3.01 (3.72) | ≥8 g/kg/day |
| LOS in the program *** | 4.81 (2.48) | 6.68 (4.89) | 5.11 (2.75) | 4.81 (2.59) | 5.12 (2.79) | 5.29 (3.27) | <8 weeks |
| Boys | |||||||
| Total admissions, N | 103,833 | 103,114 | 102,458 | 118,909 | 95,370 | 523,684 | |
| Total exits, N | 83,029 (79.96) | 83,486 (80.96) | 86,181 (84.11) | 104,046 (87.50) | 80,853 (84.78) | 437,595 (83.56) | |
| Relapse rate [mean (SD] | 1.21 (2.10) | 2.30 (4.87) | 2.48 (5.28) | 2.98 (5.17) | 2.44 (4.57) | 2.33 (4.65) | <10% |
| Exits [mean (SD] | |||||||
| Recovered | 84.94 (16.77) | 83.92 (18.49) | 87.59 (13.64) | 88.07 (14.65) | 91.71 (13.29) | 87.43 (15.56) | >75% |
| Died | 2.46 (9.69) | 2.3 (8.70) | 1.54 (4.06) | 1.87 (4.56) | 1.72 (4.85) | 1.95 (6.57) | <10% |
| Defaulters | 6.79 (10.74) | 6.93 (10.18) | 5.51 (9.86) | 4.13 (6.07) | 2.26 (3.21) | 5.01 (8.54) | <15% |
| Not- recovered | 1.91 (3.76) | 1.7 (4.41) | 1.44 (2.60) | 1.53 (4.00) | 0.82 (1.55) | 1.45 (3.39) | |
| Transferred | 3.91 (8.84) | 5.14 (13.38) | 3.92 (9.28) | 4.41 (12.94) | 3.49 (12.08) | 4.16 (11.50) | |
| Weight gain velocity | 3.57 (3.00) | 1.27 (2.66) | 2.94 (4.27) | 3.93 (3.03) | 3.41 (2.80) | 3.04 (3.35) | ≥8 g/kg/day |
| LOS in the program | 4.72 (2.41) | 6.87 (5.43) | 5.17 (2.73) | 4.76 (2.50) | 5.09 (2.71) | 5.31 (3.41) | <8 weeks |
| Other | |||||||
| Total admissions, N | 1787 | 784 | 1256 | 572 | 649 | 5048 | |
| Total exits, N | 356 (19.92) | 663 (84.57) | 639 (50.88) | 570 (99.65) | 514 (79.20) | 2751 (54.50) | |
| Relapse rate [mean (SD] | 1.42 (8.33) | 2.31 (5.50) | 1.38 (4.47) | 2.02 (7.67) | 3.35 (9.15) | 2.09 (7.21) | <10% |
| Exits [mean (SD] | |||||||
| Recovered | 79.88 (28.94) | 76.15 (29.17) | 74.83 (37.42) | 83.82 (28.73) | 82.72 (33.26) | 79.56 (32.12) | >75% |
| Died | 4.84 (13.66) | 1.58 (5.70) | 5.56 (17.86) | 2.05 (6.47) | 3.3 (16.02) | 3.57 (13.29) | <10% |
| Defaulters | 9.26 (25.60) | 8.16 (11.73) | 6.02 (15.57) | 5.01 (15.68) | 7.62 (23.46) | 6.87 (18.60) | <15% |
| Not- recovered | 3.16 (8.02) | 4.57 (9.84) | 1.95 (8.14) | 5.14 (19.95) | 1.43 (7.96) | 3.20 (12.33) | |
| Transferred | 2.86 (10.60) | 9.54 (25.95) | 11.64 (30.15) | 3.98 (16.23) | 4.93 (17.78) | 6.30 (21.96) | |
| Weight gain velocity | 3.53 (2.83) | 1.15 (2.01) | 2.03 (11.66) | 4.07 (3.77) | 3.65 (5.08) | 2.90 (6.32) | ≥8 g/kg/day |
| LOS in the program | 4.87 (2.47) | 6.63 (5.24) | 5.15 (2.90) | 4.94 (2.59) | 5.11 (2.50) | 5.32 (3.34) | <8 weeks |
| Age group | |||||||
| <6 months | |||||||
| Total admissions, N | 443 | 440 | 735 | 787 | 524 | 2929 | |
| Total exits, N | 352 (79.46) | 438 (99.55) | 730 (99.32) | 455 (57.81) | 458 (87.40) | 2433 (83.07) | |
| Relapse rate [mean (SD] | 0.21 (1.14) | 3.44 (10.41) | 2.34 (7.54) | 2.21 (5.13) | 1.06 (3.11) | 1.91 (6.64) | <10% |
| Exits [mean (SD] | |||||||
| Recovered | 82.24 (31.43) | 82.21 (26.80) | 89.02 (22.73) | 85.13 (30.04) | 90.42 (21.3) | 86.05 (26.23) | >75% |
| Died | 4.13 (15.7) | 3.17 (8.43) | 3.39 (13.85) | 3.99 (16.41) | 2.87 (9.57) | 3.46 (12.80) | <10% |
| Defaulters | 7.89 (21.98) | 4.03 (15.07) | 1.36 (3.73) | 0.93 (3.38) | 0.69 (2.80) | 2.86 (11.97) | <15% |
| Not- recovered | 0 (0) | 0.15 (1.15) | 1.92 (12.09) | 0.1 (0.62) | 0.17 (1.23) | 0.58 (6.26) | |
| Transferred | 5.73 (17.72) | 10.44 (23.35) | 4.3 (12.61) | 9.86 (26.79) | 5.85 (19.71) | 7.05 (20.01) | |
| Weight gain velocity | 3.41 (2.57) | 1.16 (2.21) | 2.77 (5.73) | 4.03 (3.59) | 3.20 (2.54) | 2.91 (3.76) | ≥8 g/kg/day |
| LOS in the program | 4.90 (2.45) | 6.81 (5.24) | 5.12 (2.67) | 4.98 (2.86) | 5.15 (2.88) | 5.39 (3.43) | <8 weeks |
| 6–59 months | |||||||
| Total admissions, N | 215,877 | 216,636 | 212,474 | 247,995 | 204,587 | 1,097,569 | |
| Total exits, N | 174,918 (81.03) | 173,520 (80.10) | 178,728 (84.12) | 215,007 (86.70) | 172,330 (84.23) | 914,503 (83.32) | |
| Relapse rate [mean (SD] | 1.51 (2.31) | 2.03 (2.91) | 2.12 (3.03 | 2.83 (4.34) | 2.57 (4.11) | 2.25 (3.52) | <10% |
| Exits [mean (SD] | |||||||
| Recovered | 84.89 (13.1) | 84.34 (15.53) | 86.8 (13.39) | 89.25 (10.31) | 91.5 (12.44) | 87.59 (13.23) | >75% |
| Died | 1.31 (3.36) | 1.81 (7.05) | 1.54 (3.78) | 1.61 (3.79) | 1.44 (3.57) | 1.57 (4.48) | <10% |
| Defaulters | 6.98 (7.33) | 7.65 (10.35) | 6.02 (9.28) | 4.44 (6.07) | 2.51 (3.23) | 5.37 (7.78) | <15% |
| Not- recovered | 2.34 (3.87) | 2.15 (5.16) | 1.67 (2.36) | 1.7 (3.48) | 1.05 (1.88) | 1.74 (3.500 | |
| Transferred | 4.49 (9.26) | 4.06 (8.41) | 3.97 (9.45) | 3 (6.85) | 3.5 (11.67) | 3.76 (9.29) | |
| Weight gain velocity | 3.60 (3.13) | 1.20 (2.54) | 2.97 (4.02) | 4.06 (3.63) | 3.43 (2.82) | 3.07 (3.43) | ≥8 g/kg/day |
| LOS in the program | 4.70 (2.44) | 6.76 (5.12) | 5.15 (2.77) | 4.69 (2.38) | 5.09 (2.69) | 5.26 (3.30) | <8 weeks |
| >=60 months | |||||||
| Total admissions, N | 1787 | 784 | 1256 | 572 | 649 | 5048 | |
| Total exits, N | 356 (19.92) | 663 (84.57) | 639 (50.88) | 572 (100.00) | 514 (79.20) | 2744 (54.36) | |
| Relapse rate [mean (SD] | 1.42 (8.33) | 2.31 (5.50) | 1.38 (4.47) | 2.02 (7.67) | 3.35 (9.15) | 2.09 (7.21) | <10% |
| Exits [mean (SD] | |||||||
| Recovered | 79.88 (28.94) | 76.15 (29.17) | 74.83 (37.42) | 83.82 (28.73) | 82.72 (33.26) | 79.56 (32.12) | >75% |
| Died | 4.84 (13.66) | 1.58 (5.70) | 5.56 (17.86) | 2.05 (6.47) | 3.3 (16.02) | 3.57 (13.12) | <10% |
| Defaulters | 9.26 (25.6) | 8.16 (11.73) | 6.02 (15.57) | 5.01 (15.68) | 7.62 (23.46) | 6.87 (18.60) | <15% |
| Not- recovered | 3.16 (8.02) | 4.57 (9.84) | 1.95 (8.14) | 5.14 (19.95) | 1.43 (7.96) | 3.20 (12.33) | |
| Transferred | 2.86 (10.6) | 9.54 (25.95) | 11.64 (30.15) | 3.98 (16.23) | 4.93 (17.78) | 6.80 (21.96) | |
| Weight gain velocity | 3.60 (2.89) | 1.40 (2.34) | 1.19 (2.03) | 4.12 (3.80) | 3.50 (4.98) | 3.01 (5.87) | ≥8 g/kg/day |
| LOS in the program | 4.99 (2.59) | 6.68 (5.30) | 6.70 (5.31) | 4.98 (2.60) | 5.18 (2.57) | 5.40 (3.42) | <8 weeks |
| All | |||||||
| Total admissions, N | 218,107 | 217,860 | 214,465 | 249,354 | 205,760 | 1,105,546 | |
| Total exits, N | 175,626 (80.52) | 174,636 (80.16) | 180,142 (84.00) | 216,041 (86.64) | 173,302 (84.23) | 919,747 (83.19) | |
| Relapse rate [mean (SD] | 1.27 (3.46) | 2.31 (5.29) | 2.06 (4.43) | 2.65 (4.95) | 2.45 (4.91) | 2.18 (4.70) | <10% |
| Exits [mean (SD] | |||||||
| Recovered | 83.96 (19.12) | 83.24 (19.55) | 85.59 (20.48) | 88.07 (17.02) | 90.44 (17.3) | 86.44 (18.89) | >75% |
| Died | 2.11 (8.18) | 2.04 (7.22) | 2.42 (9.41) | 1.93 (6.77) | 1.83 (6.99) | 2.07 (7.78) | <10% |
| Defaulters | 7.35 (13.43) | 7.03 (11.53) | 5.17 (9.83) | 4.13 (7.91) | 2.78 (8.24) | 5.15 (10.32) | <15% |
| Not- recovered | 2.06 (4.29) | 1.99 (5.38) | 1.75 (6.24) | 1.98 (7.94) | 0.96 (3.07) | 1.73 (5.71) | |
| Transferred | 4.51 (11.11) | 5.7 (14.62) | 5.06 (14.72) | 3.88 (12.31) | 3.98 (13.78) | 4.61 (13.46) | |
| Weight gain velocity | 3.47 (23.73) | 3.08 (3.29) | 2.81 (4.29) | 3.34 (3.62) | 3.43 (3.49) | 3.30 (14.97) | ≥8 g/kg/day |
| LOS in the program | 6.91 (3.87) | 6.61 (3.26) | 5.88 (2.65) | 5.67 (2.76) | 5.12 (2.67) | 6.65 (3.65) | <8 weeks |
| Variable | Recovered | Died | Defaulted | Non-Recovered | Transferred | Readmitted | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| β | 95% CI | p-Value | β | 95% CI | p-Value | β | 95% CI | p-Value | β | 95% CI | p-Value | β | 95% CI | p-Value | β | 95% CI | p-Value | |||||||
| Sex | ||||||||||||||||||||||||
| Girls | Ref | Ref | Ref | Ref | Ref | Ref | ||||||||||||||||||
| Boys | 0.21 | −1.62 | 2.05 | 0.820 | 0.14 | −0.62 | 0.90 | 0.720 | 0.16 | −0.85 | 1.17 | 0.762 | −0.18 | −0.73 | 0.38 | 0.536 | −0.33 | −1.65 | 0.98 | 0.620 | 0.27 | −0.18 | 0.73 | 0.239 |
| Other | −7.66 | −10.53 | −4.78 | 0.000 | 1.77 | 0.58 | 2.96 | 0.004 | 2.02 | 0.44 | 3.60 | 0.012 | 1.57 | 0.70 | 2.44 | 0.000 | 2.30 | 0.24 | 4.36 | 0.029 | 0.04 | −0.67 | 0.74 | 0.915 |
| Age-group | ||||||||||||||||||||||||
| <6 months | Ref | Ref | Ref | Ref | Ref | Ref | ||||||||||||||||||
| 6–59 months | 1.53 | −0.88 | 3.95 | 0.214 | −1.91 | −2.91 | −0.91 | 0.000 | 2.51 | 1.18 | 3.84 | 0.000 | 1.16 | 0.43 | 1.89 | 0.002 | −3.29 | −5.02 | −1.56 | 0.000 | 0.34 | −0.25 | 0.93 | 0.256 |
| >=60 months | −6.50 | −9.87 | −3.12 | 0.000 | 0.12 | −1.28 | 1.51 | 0.869 | 4.01 | 2.16 | 5.87 | 0.000 | 2.62 | 1.59 | 3.64 | 0.000 | −0.25 | −2.67 | 2.16 | 0.839 | 0.18 | −0.64 | 1.00 | 0.667 |
| Years | ||||||||||||||||||||||||
| 2016 | Ref | Ref | Ref | Ref | Ref | Ref | ||||||||||||||||||
| 2017 | −0.72 | −3.63 | 2.19 | 0.629 | −0.07 | −1.29 | 1.14 | 0.904 | −0.33 | −1.91 | 1.26 | 0.685 | −0.07 | −0.95 | 0.82 | 0.885 | 1.18 | −0.91 | 3.28 | 0.267 | 1.04 | 0.32 | 1.75 | 0.004 |
| 2018 | 1.63 | −1.17 | 4.43 | 0.253 | 0.30 | −0.86 | 1.47 | 0.610 | −2.18 | −3.71 | −0.66 | 0.005 | −0.30 | −1.15 | 0.55 | 0.487 | 0.55 | −1.47 | 2.56 | 0.595 | 0.79 | 0.11 | 1.48 | 0.024 |
| 2019 | 4.11 | 1.28 | 6.94 | 0.004 | −0.18 | −1.36 | 0.99 | 0.759 | −3.22 | −4.76 | −1.68 | 0.000 | −0.07 | −0.94 | 0.79 | 0.865 | −0.63 | −2.67 | 1.40 | 0.542 | 1.38 | 0.68 | 2.08 | 0.000 |
| 2020 | 6.48 | 3.65 | 9.30 | 0.000 | −0.28 | −1.45 | 0.90 | 0.641 | −4.57 | −6.11 | −3.03 | 0.000 | −1.09 | −1.95 | −0.23 | 0.013 | −0.53 | −2.56 | 1.50 | 0.607 | 1.18 | 0.49 | 1.88 | 0.001 |
| States | ||||||||||||||||||||||||
| Central Equatoria | Ref | Ref | Ref | Ref | Ref | Ref | ||||||||||||||||||
| Eastern Equatoria | 7.52 | 3.38 | 11.66 | 0.000 | −0.18 | −1.92 | 1.57 | 0.844 | −3.91 | −6.22 | −1.61 | 0.001 | −1.18 | −2.47 | 0.10 | 0.071 | −2.25 | −5.20 | 0.70 | 0.136 | 0.35 | −0.67 | 1.38 | 0.500 |
| Lakes | 12.93 | 8.76 | 17.10 | 0.000 | −1.84 | −3.60 | −0.07 | 0.041 | −5.25 | −7.57 | −2.93 | 0.000 | −1.39 | −2.68 | −0.09 | 0.035 | −4.45 | −7.43 | −1.48 | 0.003 | −0.51 | −1.55 | 0.54 | 0.343 |
| Jonglei | 13.76 | 9.86 | 17.66 | 0.000 | −2.95 | −4.60 | −1.30 | 0.000 | −6.23 | −8.40 | −4.06 | 0.000 | −0.63 | −1.84 | 0.58 | 0.309 | −3.94 | −6.73 | −1.16 | 0.005 | 0.05 | −0.91 | 1.02 | 0.912 |
| Northern Bahr el Ghazal | −1.61 | −6.14 | 2.93 | 0.487 | −0.82 | −2.74 | 1.09 | 0.401 | −6.43 | −8.95 | −3.91 | 0.000 | 0.28 | −1.13 | 1.69 | 0.697 | 8.58 | 5.34 | 11.81 | 0.000 | 2.50 | 1.37 | 3.64 | 0.000 |
| Unity | 12.76 | 8.72 | 16.80 | 0.000 | −2.13 | −3.84 | −0.43 | 0.014 | −6.95 | −9.19 | −4.70 | 0.000 | −1.45 | −2.70 | −0.19 | 0.024 | −2.23 | −5.11 | 0.65 | 0.129 | −0.20 | −1.21 | 0.81 | 0.699 |
| Upper Nile | 9.23 | 5.11 | 13.36 | 0.000 | −1.76 | −3.51 | −0.02 | 0.047 | −4.01 | −6.31 | −1.72 | 0.001 | −0.89 | −2.17 | 0.40 | 0.176 | −2.57 | −5.52 | 0.37 | 0.086 | −0.58 | −1.59 | 0.44 | 0.266 |
| Warrap | 6.50 | 2.35 | 10.65 | 0.002 | −1.64 | −3.39 | 0.11 | 0.067 | −4.57 | −6.88 | −2.27 | 0.000 | −1.06 | −2.35 | 0.22 | 0.106 | 0.78 | −2.18 | 3.74 | 0.606 | 1.03 | −0.01 | 2.06 | 0.053 |
| Western Bahr el Ghazal | 10.40 | 4.78 | 16.02 | 0.000 | −1.81 | −4.18 | 0.56 | 0.135 | −3.44 | −6.56 | −0.31 | 0.031 | 0.12 | −1.62 | 1.87 | 0.892 | −5.28 | −9.28 | −1.27 | 0.010 | 0.31 | −1.10 | 1.72 | 0.668 |
| Western Equatoria | 9.81 | 5.60 | 14.03 | 0.000 | −0.90 | −2.68 | 0.88 | 0.321 | −5.89 | −8.24 | −3.55 | 0.000 | −0.50 | −1.81 | 0.81 | 0.456 | −2.52 | −5.53 | 0.49 | 0.101 | −0.46 | −1.52 | 0.59 | 0.392 |
| Type of program | ||||||||||||||||||||||||
| SC | Ref | Ref | Ref | Ref | Ref | Ref | ||||||||||||||||||
| OTP | 0.23 | −1.52 | 1.97 | 0.799 | −2.90 | −3.61 | −2.20 | 0.000 | 4.67 | 3.74 | 5.60 | 0.000 | 2.22 | 1.70 | 2.74 | 0.000 | −4.21 | −5.44 | −2.98 | 0.000 | 0.86 | 0.43 | 1.28 | 0.000 |
| Length of stay | ||||||||||||||||||||||||
| <=5 weeks | Ref | Ref | Ref | Ref | Ref | Ref | ||||||||||||||||||
| 6–8 Weeks | −1.21 | −4.09 | 1.68 | 0.412 | 0.28 | −0.91 | 1.47 | 0.648 | 0.22 | −1.36 | 1.80 | 0.784 | 0.15 | −0.72 | 1.02 | 0.739 | 0.56 | −1.50 | 2.62 | 0.593 | 0.32 | −0.38 | 1.03 | 0.367 |
| >=9 weeks | 2.06 | −0.31 | 4.43 | 0.088 | −0.27 | −1.25 | 0.71 | 0.588 | −0.37 | −1.66 | 0.93 | 0.578 | −0.42 | −1.13 | 0.30 | 0.254 | −1.01 | −2.70 | 0.68 | 0.242 | 0.22 | −0.36 | 0.81 | 0.456 |
| Weight velocity | ||||||||||||||||||||||||
| <=3 g/kg/day | Ref | Ref | Ref | Ref | Ref | Ref | ||||||||||||||||||
| 4–7 g/kg/day | −0.42 | −2.41 | 1.58 | 0.680 | −0.22 | −1.05 | 0.60 | 0.593 | −0.18 | −1.27 | 0.91 | 0.743 | −0.31 | −0.92 | 0.29 | 0.306 | 1.14 | −0.28 | 2.56 | 0.116 | 0.26 | −0.23 | 0.75 | 0.298 |
| >=8 g/gg/day | 0.27 | −3.07 | 3.61 | 0.875 | 0.19 | −1.18 | 1.57 | 0.784 | −0.01 | −1.83 | 1.82 | 0.995 | −0.48 | −1.49 | 0.53 | 0.350 | 0.03 | −2.36 | 2.41 | 0.983 | 0.22 | −0.60 | 1.05 | 0.595 |
| Variable | Recovered | Died | Defaulted | Non-Recovered | Transferred | Readmitted | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| β | 95% CI | p-Value | β | 95% CI | p-Value | β | 95% CI | p-Value | β | 95% CI | p-Value | β | 95% CI | p-Value | β | 95% CI | p-Value | |||||||
| Sex | ||||||||||||||||||||||||
| Girls | Ref | Ref | Ref | Ref | Ref | Ref | ||||||||||||||||||
| Boys | 0.21 | −1.56 | 1.98 | 0.815 | 0.14 | −0.60 | 0.89 | 0.703 | 0.14 | −0.82 | 1.11 | 0.769 | −0.19 | −0.73 | 0.36 | 0.502 | −0.31 | −1.58 | 0.95 | 0.628 | 0.28 | −0.17 | 0.73 | 0.219 |
| Other | −7.01 | −10.66 | −3.35 | 0.000 | 2.27 | 0.73 | 3.80 | 0.004 | 0.93 | −1.06 | 2.92 | 0.361 | 0.94 | −0.19 | 2.07 | 0.103 | 2.87 | 0.26 | 5.49 | 0.031 | −0.50 | −1.42 | 0.41 | 0.282 |
| Age-group | ||||||||||||||||||||||||
| <6 months | Ref | Ref | Ref | Ref | Ref | Ref | ||||||||||||||||||
| 6–59 months | 0.61 | −2.00 | 3.22 | 0.645 | −0.10 | −1.19 | 1.00 | 0.863 | −0.04 | −1.46 | 1.39 | 0.961 | −0.10 | −0.91 | 0.71 | 0.811 | −0.38 | −2.25 | 1.48 | 0.687 | −0.24 | −0.89 | 0.40 | 0.462 |
| >=60 months | NED | NED | NED | NED | NED | NED | ||||||||||||||||||
| Years | ||||||||||||||||||||||||
| 2016 | Ref | Ref | Ref | Ref | Ref | Ref | ||||||||||||||||||
| 2017 | −1.25 | −4.15 | 1.65 | 0.399 | −0.24 | −1.46 | 0.98 | 0.703 | −0.12 | −1.70 | 1.46 | 0.881 | 0.02 | −0.88 | 0.91 | 0.972 | 1.59 | −0.48 | 3.66 | 0.133 | 1.04 | 0.31 | 1.77 | 0.005 |
| 2018 | 1.73 | −0.99 | 4.45 | 0.213 | −0.04 | −1.19 | 1.11 | 0.945 | −2.11 | −3.59 | −0.62 | 0.005 | −0.24 | −1.08 | 0.60 | 0.572 | 0.66 | −1.29 | 2.61 | 0.506 | 0.96 | 0.27 | 1.64 | 0.006 |
| 2019 | 4.20 | 1.45 | 6.96 | 0.003 | −0.38 | −1.54 | 0.78 | 0.522 | −3.18 | −4.68 | −1.67 | 0.000 | 0.01 | −0.84 | 0.87 | 0.973 | −0.66 | −2.63 | 1.31 | 0.509 | 1.48 | 0.79 | 2.17 | 0.000 |
| 2020 | 6.34 | 3.60 | 9.08 | 0.000 | −0.53 | −1.68 | 0.62 | 0.367 | −4.41 | −5.90 | −2.91 | 0.000 | −0.98 | −1.83 | −0.13 | 0.024 | −0.43 | −2.39 | 1.53 | 0.669 | 1.33 | 0.65 | 2.02 | 0.000 |
| States | ||||||||||||||||||||||||
| Central Equatoria | Ref | Ref | Ref | Ref | Ref | Ref | ||||||||||||||||||
| Eastern Equatoria | 7.14 | 3.04 | 11.25 | 0.001 | −0.41 | −2.14 | 1.32 | 0.640 | −3.59 | −5.83 | −1.35 | 0.002 | −0.99 | −2.26 | 0.28 | 0.126 | −2.15 | −5.09 | 0.78 | 0.151 | 0.46 | −0.56 | 1.48 | 0.378 |
| Lakes | 12.54 | 8.42 | 16.66 | 0.000 | −2.03 | −3.77 | −0.30 | 0.021 | −4.88 | −7.13 | −2.64 | 0.000 | −1.13 | −2.40 | 0.15 | 0.083 | −4.50 | −7.44 | −1.56 | 0.003 | −0.33 | −1.37 | 0.71 | 0.537 |
| Jonglei | 13.00 | 9.12 | 16.87 | 0.000 | −3.06 | −4.69 | −1.43 | 0.000 | −5.87 | −7.98 | −3.75 | 0.000 | −0.36 | −1.56 | 0.84 | 0.555 | −3.71 | −6.48 | −0.94 | 0.009 | 0.20 | −0.77 | 1.16 | 0.689 |
| Northern Bahr el Ghazal | −1.52 | −6.03 | 2.98 | 0.507 | −1.20 | −3.09 | 0.70 | 0.215 | −6.25 | −8.71 | −3.80 | 0.000 | 0.47 | −0.92 | 1.86 | 0.509 | 8.51 | 5.29 | 11.73 | 0.000 | 2.77 | 1.63 | 3.91 | 0.000 |
| Unity | 12.37 | 8.37 | 16.37 | 0.000 | −2.42 | −4.10 | −0.74 | 0.005 | −6.46 | −8.64 | −4.28 | 0.000 | −1.20 | −2.44 | 0.04 | 0.057 | −2.29 | −5.15 | 0.57 | 0.117 | −0.03 | −1.05 | 0.98 | 0.949 |
| Upper Nile | 8.25 | 4.14 | 12.36 | 0.000 | −1.57 | −3.30 | 0.16 | 0.075 | −4.06 | −6.30 | −1.82 | 0.000 | −0.82 | −2.09 | 0.45 | 0.208 | −1.80 | −4.74 | 1.14 | 0.230 | −0.42 | −1.44 | 0.61 | 0.425 |
| Warrap | 6.30 | 2.18 | 10.43 | 0.003 | −2.11 | −3.85 | −0.38 | 0.017 | −3.68 | −5.93 | −1.43 | 0.001 | −0.51 | −1.79 | 0.76 | 0.432 | 0.00 | −2.95 | 2.95 | 1.000 | 1.29 | 0.25 | 2.33 | 0.015 |
| Western Bahr el Ghazal | 10.72 | 5.17 | 16.28 | 0.000 | −1.90 | −4.23 | 0.44 | 0.112 | −3.74 | −6.77 | −0.71 | 0.015 | 0.12 | −1.60 | 1.84 | 0.891 | −5.21 | −9.18 | −1.24 | 0.010 | 0.40 | −1.00 | 1.81 | 0.576 |
| Western Equatoria | 8.86 | 4.65 | 13.08 | 0.000 | −0.95 | −2.73 | 0.82 | 0.291 | −5.46 | −7.75 | −3.16 | 0.000 | −0.39 | −1.70 | 0.91 | 0.553 | −2.06 | −5.07 | 0.95 | 0.180 | −0.45 | −1.51 | 0.61 | 0.406 |
| Type of program | ||||||||||||||||||||||||
| SC | Ref | Ref | Ref | Ref | Ref | Ref | ||||||||||||||||||
| OTP | 0.90 | −0.98 | 2.78 | 0.349 | −3.17 | −3.97 | −2.38 | 0.000 | 4.40 | 3.38 | 5.43 | 0.000 | 2.10 | 1.52 | 2.68 | 0.000 | −4.23 | −5.58 | −2.89 | 0.000 | 1.12 | 0.64 | 1.59 | 0.000 |
| Length of stay | ||||||||||||||||||||||||
| <=5 weeks | Ref | Ref | Ref | Ref | Ref | Ref | ||||||||||||||||||
| 6–8 Weeks | −1.06 | −3.85 | 1.73 | 0.457 | 0.18 | −1.00 | 1.35 | 0.765 | 0.19 | −1.34 | 1.71 | 0.810 | 0.05 | −0.81 | 0.92 | 0.904 | 0.64 | −1.35 | 2.64 | 0.529 | 0.36 | −0.34 | 1.06 | 0.310 |
| >=9 weeks | 2.10 | −0.28 | 4.48 | 0.084 | −0.35 | −1.35 | 0.65 | 0.497 | −0.44 | −1.74 | 0.85 | 0.503 | −0.48 | −1.21 | 0.26 | 0.205 | −0.84 | −2.54 | 0.87 | 0.336 | 0.32 | −0.28 | 0.92 | 0.293 |
| Weight velocity | ||||||||||||||||||||||||
| <=3 g/kg/day | Ref | Ref | Ref | Ref | Ref | Ref | ||||||||||||||||||
| 4–7 g/kg/day | −0.87 | −2.93 | 1.18 | 0.406 | −0.10 | −0.96 | 0.77 | 0.825 | −0.25 | −1.37 | 0.87 | 0.667 | −0.38 | −1.01 | 0.26 | 0.246 | 1.59 | 0.12 | 3.06 | 0.034 | 0.18 | −0.34 | 0.69 | 0.508 |
| >=8 g/gg/day | −0.24 | −3.53 | 3.04 | 0.886 | 0.23 | −1.15 | 1.61 | 0.746 | 0.30 | −1.49 | 2.09 | 0.741 | −0.58 | −1.60 | 0.44 | 0.263 | 0.29 | −2.06 | 2.64 | 0.808 | 0.04 | −0.79 | 0.88 | 0.919 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Renzaho, A.M.N.; Dachi, G.; Tesfaselassie, K.; Abebe, K.T.; Kassim, I.; Alam, Q.; Shaban, N.S.; Shiweredo, T.; Vinathan, H.; Jaiswal, C.; et al. Assessing the Impact of Integrated Community-Based Management of Severe Wasting Programs in Conflict-Stricken South Sudan: A Multi-Dimensional Approach to Scalability of Nutrition Emergency Response Programs. Int. J. Environ. Res. Public Health 2021, 18, 9113. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18179113
Renzaho AMN, Dachi G, Tesfaselassie K, Abebe KT, Kassim I, Alam Q, Shaban NS, Shiweredo T, Vinathan H, Jaiswal C, et al. Assessing the Impact of Integrated Community-Based Management of Severe Wasting Programs in Conflict-Stricken South Sudan: A Multi-Dimensional Approach to Scalability of Nutrition Emergency Response Programs. International Journal of Environmental Research and Public Health. 2021; 18(17):9113. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18179113
Chicago/Turabian StyleRenzaho, Andre M. N., Gilbert Dachi, Kibrom Tesfaselassie, Kiross Tefera Abebe, Ismail Kassim, Qutab Alam, Nawal Sadick Shaban, Tesfatsion Shiweredo, Hari Vinathan, Chandrakala Jaiswal, and et al. 2021. "Assessing the Impact of Integrated Community-Based Management of Severe Wasting Programs in Conflict-Stricken South Sudan: A Multi-Dimensional Approach to Scalability of Nutrition Emergency Response Programs" International Journal of Environmental Research and Public Health 18, no. 17: 9113. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18179113