
Intergenerational Association of Short Maternal Stature with Stunting in Yanomami Indigenous Children from the Brazilian Amazon

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
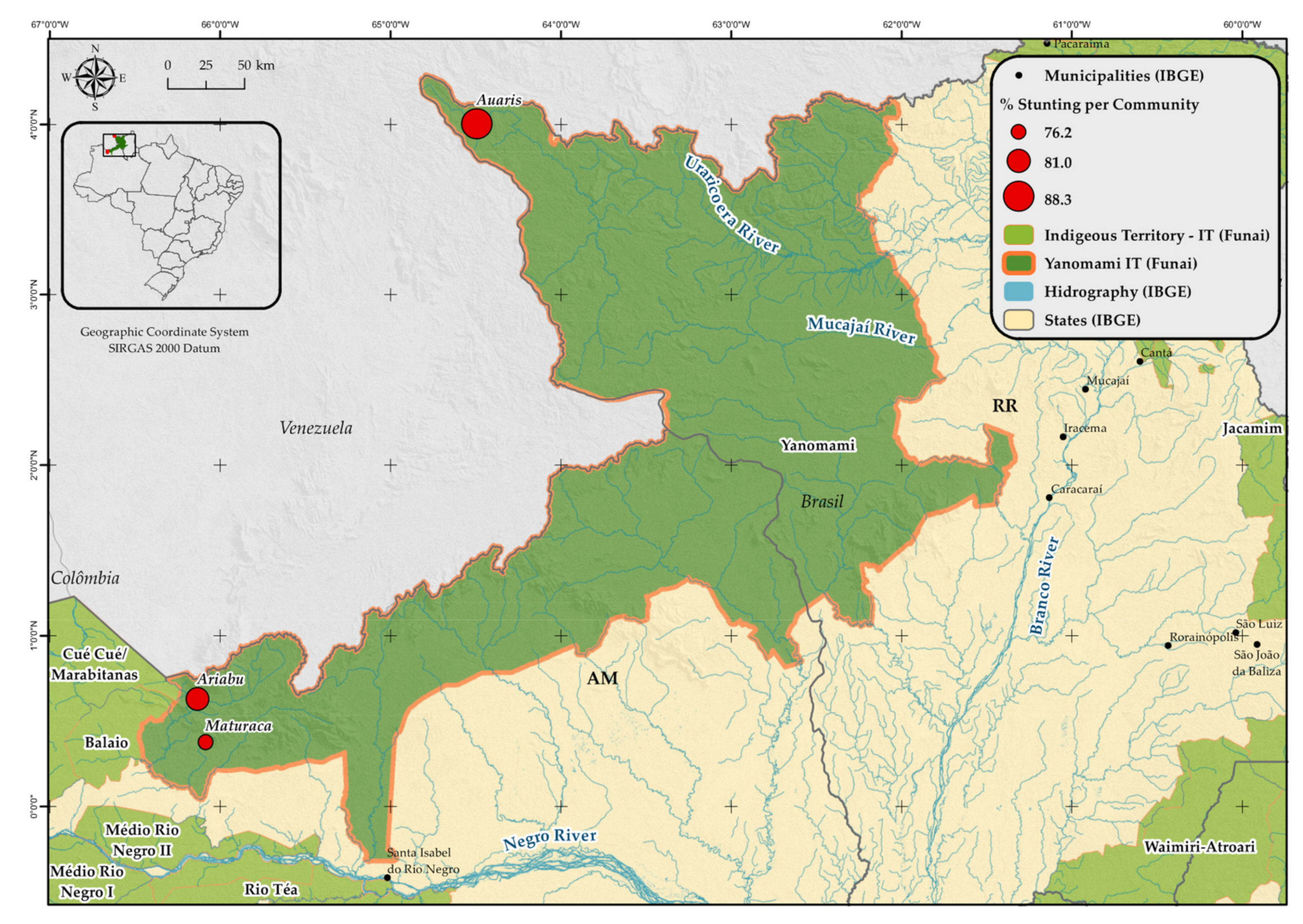
2.1. Study Area and Population
2.2. Study Design
2.3. Maternal and Child Anthropometry
2.4. Sociodemographic, Maternal and Child Characteristics
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization (WHO). WHO Child Growth Standards: Length/Height-for-Age, Weight-for-Age, Weight-for-Length, Weight-for-Height and Body Mass Index-for-Age; Methods and Development; WHO (Nonserial Publication); WHO: Geneva, Switzerland, 2006. [Google Scholar]
- Black, R.E.; Allen, L.H.; Bhutta, Z.A.; Caulfield, L.E.; De Onis, M.; Ezzati, M.; Mathers, C.; Rivera, J.; Maternal and Child Undernutrition Study Group. Maternal and child undernutrition: Global and regional exposures and health consequences. Lancet 2008, 371, 243–260. [Google Scholar] [CrossRef]
- Ozaltin, E.; Hill, K.; Subramanian, S.V. Association of maternal stature with offspring mortality, underweight, and stunting in low- to middle-income countries. JAMA 2010, 303, 1507–1516. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stein, A.D.; Wang, M.; Martorell, R.; Norris, S.A.; Adair, L.S.; Bas, I.; Sachdev, H.S.; Bhargava, S.K.; Fall, C.H.D.; Gigante, D.; et al. Growth patterns in early childhood and final attained stature: Data from five birth cohorts from low- and middle-income countries. Am. J. Hum. Biol. 2010, 22, 353–359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- United Nations (UN). Transforming Our World: The 2030 Agenda for Sustainable Development; Division for Sustainable Development Goals: New York, NY, USA, 2021. [Google Scholar]
- UNICEF; WHO; World Bank Group. Levels and Trends in Child. Malnutrition; UNICEF-WHO-World Bank Group Joint Child Malnutrition Estimates: Key Findings of the 2019 Edition; UNICEF: New York, NY, USA; WHO: Geneva, Switzerland; World Bank Group: Washington, DC, USA, 2019. [Google Scholar]
- Victora, C.G.; Christian, P.; Vidaletti, L.P.; Gatica-Domínguez, G.; Menon, P.; Black, R.E. Revisiting maternal and child undernutrition in low-income and middle-income countries: Variable progress towards an unfinished agenda. Lancet 2021, 397, 1388–1399. [Google Scholar] [CrossRef]
- World Bank Group. Indigenous Latin America in the Twenty-First Century: The First Decade. World Bank. © World Bank. 2015. Available online: https://openknowledge.worldbank.org/handle/10986/23751 (accessed on 23 June 2021).
- Gatica-Domínguez, G.; Victora, C.; Barros, A.J. Ethnic inequalities and trends in stunting prevalence among Guatemalan children: An analysis using national health surveys 1995–2014. Int. J. Equity Health 2019, 18, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amarante, V.; Figueroa, N.; Ullman, H. Inequalities in the reduction of child stunting over time in Latin America: Evidence from the DHS 2000–2010. Oxf. Dev. Stud. 2018, 46, 519–535. [Google Scholar] [CrossRef]
- Instituto Brasileiro de Geografia e Estatística (IBGE). Pesquisa de Orçamentos Familiares (POF): Antropometria e Estado Nutricional de Crianças, Adolescentes e Adultos no Brasil; IBGE: Rio de Janeiro, Brazil, 2010. [Google Scholar]
- Horta, B.L.; Santos, R.V.; Welch, J.R.; Cardoso, A.M.; dos Santos, J.V.; Assis, A.M.; Lira, P.C.; Coimbra, C.E., Jr. Nutritional status of indigenous children: Findings from the First National Survey of Indigenous People’s Health and Nutrition in Brazil. Int. J. Equity Health 2013, 12, 23. [Google Scholar] [CrossRef] [Green Version]
- Addo, O.Y.; Stein, A.D.; Fall, C.H.; Gigante, D.P.; Guntupalli, A.M.; Horta, B.L.; Kuzawa, C.W.; Lee, N.; Norris, S.A.; Consortium on Health Orientated Research in Transitional Societies (COHORTS) Group; et al. Maternal height and child growth patterns. J. Pediatrics 2013, 163, 549–554. [Google Scholar] [CrossRef] [Green Version]
- De Onis, M.; Branca, F. Childhood stunting: A global perspective. Matern. Child. Nutr. 2016, 12, 12–26. [Google Scholar] [CrossRef]
- Prendergast, A.J.; Humphrey, J.H. The stunting syndrome in developing countries. Paediatr. Int. Child. Health 2014, 34, 250–265. [Google Scholar] [CrossRef] [Green Version]
- Ferreira, A.A.; Welch, J.R.; Cunha, G.M.; Júnior, C.C.E.A. Physical growth curves of indigenous Xavante children in Central Brazil: Results from a longitudinal study (2009–2012). Ann. Hum. Biol. 2016, 43, 293–303. [Google Scholar] [CrossRef]
- WHO. WHO-Anthro for Personal Computers, Version 3.2.2, 2011: Software for Assessing Growth and Development of the World’s Children; WHO: Geneva, Switzerland, 2010. [Google Scholar]
- WHO. WHO-AnthroPlus for Personal Computers, Manual: Software for Assessing Growth of the World’s Children and Adolescents; WHO: Geneva, Switzerland, 2009. [Google Scholar]
- Nestel, P.; Rutstein, S. Defining nutritional status of women in developing countries. Public Health Nutr. 2002, 5, 17–27. [Google Scholar] [CrossRef] [PubMed]
- Cribari Neto, F.; Ferrari, S.L.; Cordeiro, G.M. Improved heteroscedasticity consistent covariance matrix estimators. Biometrika 2000, 87, 907–918. [Google Scholar] [CrossRef]
- Victora, C.G.; Huttly, S.R.; Fuchs, S.C.; Olinto, M. The role of conceptual frameworks in epidemiological analysis: A hierarchical approach. Int. J. Epidemiol. 1997, 26, 224–227. [Google Scholar] [CrossRef] [Green Version]
- The R Foundation. The R Project for Statistical Computing [Internet]; The R Foundation: Vienna, Austria, 2021; Available online: http://www.r-project.org (accessed on 31 May 2021).
- Manjong, F.T.; Verla, V.S.; Egbe, T.O.; Nsagha, D.S. Undernutrition among under-five indigenous Mbororo children in the Foumban and Galim health districts of Cameroon: A cross-sectional study. Pan. Afr. Med. J. 2021, 38. [Google Scholar] [CrossRef]
- Orellana, J.D.Y.; Marrero, L.; Alves, C.L.M.; Ruiz, C.M.V.; Hacon, S.S.; Oliveira, M.W.; Basta, P.C. Associação de baixa estatura severa em crianças indígenas Yanomami com baixa estatura materna: Indícios de transmissão intergeracional. Ciência Saúde Coletiva 2019, 24, 1875–1883. [Google Scholar] [CrossRef]
- Pantoja, L.N.; Orellana, J.D.Y.; Leite, M.S.; Basta, P.C. Cobertura do Sistema de Vigilância Alimentar e Nutricional Indígena (SISVAN-I) e prevalência de desvios nutricionais em crianças Yanomami menores de 60 meses, Amazônia, Brasil. Rev. Bras. Saúde Matern. Infant. 2014, 14, 53–63. [Google Scholar] [CrossRef] [Green Version]
- Verhagen, L.M.; Incani, R.N.; Franco, C.R.; Ugarte, A.; Cadenas, Y.; Sierra Ruiz, C.I.; Hermans, P.W.; Hoek, D.; Campos Ponce, M.; de Waard, J.H.; et al. High malnutrition rate in Venezuelan Yanomami compared to Warao Amerindians and Creoles: Significant associations with intestinal parasites and anemia. PLoS ONE 2013, 8, e77581. [Google Scholar] [CrossRef] [Green Version]
- Hidalgo, G.; Marini, E.; Sanchez, W.; Contreras, M.; Estrada, I.; Comandini, O.; Buffa, R.; Magris, M.; Dominguez-Bello, M.G. The nutrition transition in the Venezuelan Amazonia: Increased overweight and obesity with transculturation. Am. J. Hum. Biol. 2014, 26, 710–712. [Google Scholar] [CrossRef]
- Pithan, O.A.; Confalonieri, U.E.; Morgado, A.F. A situação de saúde dos índios Yanomámi: Diagnóstico a partir da Casa do Índio de Boa Vista, Roraima, 1987–1989. Cad. Saúde Pública 1991, 7, 563–580. [Google Scholar] [CrossRef] [Green Version]
- Grenfell, P.; Fanello, C.I.; Magris, M.; Goncalves, J.; Metzger, W.G.; Vivas-Martínez, S.; Vivas, L.; Curtis, C. Anaemia and malaria in Yanomami communities with differing access to healthcare. Trans. R. Soc. Trop. Med. Hyg. 2008, 102, 645–652. [Google Scholar] [CrossRef] [PubMed]
- Caldart, R.V.; Marrero, L.; Basta, P.C.; Orellana, J.D.Y. Fatores associados à pneumonia em crianças Yanomami internadas por condições sensíveis à atenção primária na região norte do Brasil. Ciência Saúde Coletiva 2016, 21, 1597–1606. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- International Labour Organization (ILO), Indigenous and Tribal Peoples Convention, C169, 27 June 1989, C169. Available online: https://www.refworld.org/docid/3ddb6d514.html (accessed on 7 June 2021).
- UN. UN Document A/61/L.67 12 September 2007: The United Nations Declaration on the Rights of Indigenous Peoples, Adopted by the UN General Assembly on 13 September 2007; UN: New York, NY, USA, 2007. [Google Scholar]
- Mesenburg, M.A.; Restrepo-Mendez, M.C.; Amigo, H.; Balandrán, A.D.; Barbosa-Verdun, M.A.; Caicedo-Velásquez, B.; Carvajal-Aguirre, L.; Coimbra, C.E., Jr.; Ferreira, L.Z.; del Pilar Flores-Quispe, M.; et al. Ethnic group inequalities in coverage with reproductive, maternal and child health interventions: Cross-sectional analyses of national surveys in 16 Latin American and Caribbean countries. Lancet Glob. Health 2018, 6, e902–e913. [Google Scholar] [CrossRef] [Green Version]
- Mignone, J.; Bartlett, J.; O’Neil, J.; Orchard, T. Best practices in intercultural health: Five case studies in Latin America. J. Ethnobiol. Ethnomedicine 2007, 3, 31. [Google Scholar] [CrossRef] [Green Version]
- Svefors, P.; Sysoev, O.; Ekstrom, E.C.; Persson, L.A.; Arifeen, S.E.; Naved, R.T.; Rahman, A.; Khan, A.I.; Selling, K. Relative importance of prenatal and postnatal determinants of stunting: Data mining approaches to the MINIMat cohort, Bangladesh. BMJ 2019, 9, e025154. [Google Scholar] [CrossRef] [Green Version]
- United Nations Children’s Fund (UNICEF). Improving Child. Nutrition: The Achievable Imperative for Global Progress; UNICEF: New York, NY, USA, 2013. [Google Scholar]
- Anderson, I.; Robson, B.; Connolly, M.; Al-Yaman, F.; Bjertness, E.; King, A.; Tynan, M.; Madden, R.; Bang, A.; Coimbra, C.E., Jr.; et al. Indigenous and tribal peoples’ health (The Lancet–Lowitja Institute Global Collaboration): A population study. Lancet 2016, 388, 131–157. [Google Scholar] [CrossRef]
- Basnayake, T.L.; Morgan, L.C.; Chang, A.B. The global burden of respiratory infections in indigenous children and adults: A review. Respirology 2017, 22, 1518–1528. [Google Scholar] [CrossRef] [Green Version]
- Valeggia, C.R.; Snodgrass, J.J. Health of indigenous peoples. Annu. Rev. Anthropol. 2015, 44, 117–135. [Google Scholar] [CrossRef] [Green Version]
- Gracey, M.; King, M. Indigenous health part 1: Determinants and disease patterns. Lancet 2009, 374, 65–75. [Google Scholar] [CrossRef]
- Tickell, K.D.; Atlas, H.E.; Walson, J.L. Environmental enteric dysfunction: A review of potential mechanisms, consequences and management strategies. BMC Med. 2019, 17, 1–9. [Google Scholar] [CrossRef]
- Jiménez, A.; Cortobius, M.; Kjellén, M. Water, sanitation and hygiene and indigenous peoples: A review of the literature. Water Int. 2014, 39, 277–293. [Google Scholar] [CrossRef]
- FAO; FIDA; OPS; WFP; UNICEF. Panorama de la Seguridad Alimentaria y Nutrición en América Latina y el Caribe 2020; FAO: Rome, Italy; OPS: Washington, DC, USA; WFP: Rome, Italy; UNICEF: New York, NY, USA, 2020; Available online: http://www.fao.org/documents/card/en/c/cb2242es/ (accessed on 30 June 2021). [CrossRef]
- Martorell, R.; Zongrone, A. Intergenerational influences on child growth and undernutrition. Paediatr. Perinat. Epidemiol. 2012, 26, 302–314. [Google Scholar] [CrossRef] [PubMed]
- The Guardian. Brazilian wildcat miners attack police and burn indigenous homes in Amazon [Internet]. 2021. Available online: https://www.theguardian.com/world/2021/may/28/brazil-wildcat-miners-police-indigenous-amazon (accessed on 31 May 2021).
- Fellows, M.; Paye, V.; Alencar, A.; Nicácio, M.; Castro, I.; Coelho, M.E.; Silva, C.V.J.; Bandeira, M.; Lourival, R.; Basta, P.C. Under-Reporting of COVID-19 Cases Among Indigenous Peoples in Brazil: A New Expression of Old Inequalities. Front. Psychiatry 2021, 12, 638359. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Stunting | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Age Group (Months) | Auaris | Maturacá | Ariabú | Total | ||||||||
| N | n | % | N | n | % | N | n | % | N | n | % | |
| ≤11 | 12 | 7 | 58.3 | 24 | 9 | 37.5 | 25 | 7 | 28.0 | 61 | 23 | 37.7 |
| 12 to 23 | 16 | 16 | 100.0 | 18 | 16 | 88.9 | 20 | 17 | 85.0 | 54 | 49 | 90.7 |
| 24 to 35 | 12 | 12 | 100.0 | 22 | 22 | 100.0 | 17 | 17 | 100.0 | 51 | 51 | 100.0 |
| 36 to 59 | 37 | 33 | 89.2 | 52 | 47 | 90.4 | 43 | 39 | 90.7 | 132 | 119 | 90.2 |
| Total | 77 | 68 | 88.3 | 116 | 94 | 81.0 | 105 | 80 | 76.2 | 298 | 242 | 81.2 |
| Villages of Residence | ||||
|---|---|---|---|---|
| Ariabú | Auaris | Maturacá | p-Value * | |
| n (%) | n (%) | n (%) | ||
| Sociodemographic variables | ||||
| Read or write in Portuguese | <0.001 | |||
| No | 11 (10.7%) | 35 (44.9%) | 16 (14.0%) | |
| Yes | 92 (89.3%) | 43 (55.1%) | 98 (86.0%) | |
| Source of Income | <0.001 | |||
| Federal | 12 (11.4%) | 18 (23.1%) | 11 (9.3%) | |
| Municipal/Statal | 24 (22.9%) | 4 (5.1%) | 25 (21.2%) | |
| Other | 8 (7.6%) | 5 (6.4%) | 26 (22.0%) | |
| No income | 61 (58.1%) | 51 (65.4%) | 56 (47.5%) | |
| Drinking water source | <0.001 | |||
| River or stream | 82 (78.1%) | 55 (70.5%) | 17 (14.4%) | |
| Well | 23 (21.9%) | 23 (29.5%) | 101 (86.6%) | |
| Household waste destination | <0.001 | |||
| Burnt or buried | 38 (36.2%) | 6 (7.6%) | 90 (76.9%) | |
| Forest or river | 67 (63.8%) | 73 (92.4%) | 27 (23.1%) | |
| Household wall type | <0.001 | |||
| Wood/brick | 40 (38.1%) | 7 (9.0%) | 46 (49.5%) | |
| Clay | 52 (49.5%) | 58 (74.4%) | 61 (35.7%) | |
| Straw/no wall | 13 (12.4%) | 13 (16.6%) | 09 (25.7%) | |
| Household density (number of people) | 0.035 | |||
| 1 to 6 | 32 (30.5%) | 18 (23.7%) | 40 (33.9%) | |
| 7 to 9 | 27 (25.7%) | 27 (35.5%) | 47 (39.8%) | |
| 10 or more | 46 (43.8%) | 31 (40.8%) | 31 (26.3%) | |
| Maternal and perinatal variables | ||||
| Age group (years) | 0.118 | |||
| 13.0 to 24.9 | 42 (40.0%) | 20 (27.7%) | 49 (41.5%) | |
| 25.0 or more | 63 (60.0%) | 53 (72.6%) | 69 (58.5%) | |
| Short maternal stature | 0.002 | |||
| No | 35 (35.0%) | 9 (12.3%) | 37 (32.2%) | |
| Yes | 65 (65.0%) | 64 (87.7%) | 78 (67.8%) | |
| Number of antenatal consultations | <0.001 | |||
| 0 to 3 | 19 (21.1%) | 31 (52.5%) | 22 (20.2%) | |
| 4 to 6 | 50 (55.6%) | 27 (45.8%) | 71 (65.1%) | |
| 7 to 9 | 21 (23.3%) | 1 (1.7%) | 16 (14.7%) | |
| Gestational malaria | 0.205 | |||
| No | 89 (84.8%) | 68 (93.2%) | 100 (85.5%) | |
| Yes | 16 (15.2%) | 5 (6.8%) | 17 (14.5%) | |
| Place of birth | <0.001 | |||
| Household/Forest | 57 (53.8%) | 71 (91.0%) | 68 (59.6%) | |
| Primary Healthcare Center (villages) | 27 (25.5%) | 2 (2.6%) | 23 (20.2%) | |
| Hospital/CASAI 1 | 22 (20.8%) | 5 (6.4%) | 23 (20.2%) | |
| Child’s variables | ||||
| Sex | <0.001 | |||
| Female | 69 (65.7%) | 26 (32.9%) | 81 (68.6%) | |
| Male | 36 (34.3%) | 53 (67.1%) | 37 (31.4%) | |
| Age group (months) | 0.534 | |||
| ≤23 | 46 (43.4%) | 29 (36.2%) | 44 (37.3%) | |
| 24 to 59 | 60 (56.6%) | 51 (63.8%) | 74 (62.7%) | |
| Child’s caregiver | <0.001 | |||
| Mother or father | 80 (75.5%) | 40 (50.6%) | 101 (87.8%) | |
| Another family member | 26 (24.5%) | 39 (49.4%) | 14 (12.2%) | |
| Low weight at birth | 0.977 | |||
| No | 93 (89.4%) | 61 (88.4%) | 103 (88.8%) | |
| Yes | 11 (10.6%) | 8 (11.6%) | 13 (11.2%) | |
| Pneumonia treatment | 0.069 | |||
| No | 70 (66.7%) | 39 (50.0%) | 66 (56.9%) | |
| Yes | 35 (33.3%) | 39 (50.0%) | 50 (43.1%) | |
| Undernutrition treatment | 0.127 | |||
| No | 93 (87.7%) | 60 (76.9%) | 94 (79.7%) | |
| Yes | 13 (12.3%) | 18 (23.1%) | 24 (20.3%) | |
| Malaria treatment | 0.239 | |||
| No | 97 (91.5%) | 67 (84.8%) | 108 (91.5%) | |
| Yes | 9 (8.5%) | 12 (15.2%) | 10 (8.5%) | |
| Stunting prevalence | 0.118 | |||
| No | 25 (23.8%) | 9 (11.7%) | 22 (19.0%) | |
| Yes | 80 (76.2%) | 68 (88.3%) | 94 (81.0%) | |
| Stunting | |||
|---|---|---|---|
| No | Yes | p-Value * | |
| n (%) | n (%) | ||
| Sociodemographic variables | |||
| Parent knows how to read or write in Portuguese | 0.877 | ||
| No | 11 (20.0%) | 49 (20.9%) | |
| Yes | 44 (80.0%) | 185 (79.1%) | |
| Source of Income | 0.305 | ||
| Federal | 11 (19.6%) | 30 (12.6%) | |
| Municipal/Statal | 12 (21.4%) | 41 (17.2%) | |
| Other | 8 (14.3%) | 30 (12.6%) | |
| No income | 25 (44.6%) | 138 (57.7%) | |
| Drinking water source | 0.799 | ||
| River or stream | 28 (50.0%) | 124 (51.9%) | |
| Well | 28 (50.0%) | 115 (48.1%) | |
| Household waste destination | 0.409 | ||
| Burnt or buried | 28 (50.0%) | 105 (43.9%) | |
| Forest or river | 28 (50.0%) | 134 (56.1%) | |
| Household wall type | 0.063 | ||
| Wood/brick | 25 (44.6%) | 68 (28.7%) | |
| Clay | 27 (48.2%) | 141 (59.5%) | |
| Straw/no wall | 4 (7.1%) | 28 (11.8%) | |
| Household density (number of people) | 0.770 | ||
| 1 to 6 | 17 (30.4%) | 71 (30.0%) | |
| 7 to 9 | 17 (30.4%) | 83 (35.0%) | |
| 10 or more | 22 (39.3%) | 83 (35.0%) | |
| Maternal and perinatal variables | |||
| Age group (years) | 0.390 | ||
| 13.0 to 24.9 | 17 (32.1%) | 91 (38.4%) | |
| 25.0 or more | 36 (67.9%) | 146 (61.6%) | |
| Short maternal stature | <0.001 | ||
| No | 28 (52.8%) | 53 (23.1%) | |
| Yes | 25 (47.2%) | 176 (76.9%) | |
| Number of antenatal consultations | 0.797 | ||
| 0 to 3 | 16 (31.4%) | 54 (26.7%) | |
| 4 to 6 | 28 (54.9%) | 117 (57.9%) | |
| 7 to 9 | 7 (13.7%) | 31 (15.3%) | |
| Gestational malaria | 0.071 | ||
| No | 52 (94.5%) | 201 (85.5%) | |
| Yes | 3 (5.5%) | 34 (14.5%) | |
| Place of birth | 0.027 | ||
| House/Forest | 33 (62.3%) | 158 (66.1%) | |
| Primary Healthcare Center (villages) | 5 (9.4%) | 46 (19.2%) | |
| Hospital/CASAI 1 | 15 (28.3%) | 35 (14.6%) | |
| Child variables | |||
| Sex | 0.479 | ||
| Female | 30 (54.5%) | 144 (59.8%) | |
| Male | 25 (45.5%) | 97 (40.2%) | |
| Age group (months) | <0.001 | ||
| ≤23 | 43 (76.8%) | 72 (29.8%) | |
| 24 to 59 | 13 (23.2%) | 170 (70.2%) | |
| Child’s caregiver | 0.089 | ||
| Mother or father | 45 (83.3%) | 170 (70.8%) | |
| Another family member | 9 (16.7%) | 70 (29.2%) | |
| Low weight at birth | 0.779 | ||
| No | 46 (90.2%) | 207 (88.8%) | |
| Yes | 5 (9.8%) | 26 (11.2%) | |
| Pneumonia treatment | <0.001 | ||
| No | 43 (78.2%) | 126 (52.9%) | |
| Yes | 12 (21.8%) | 112 (47.1%) | |
| Undernutrition treatment | 0.002 | ||
| No | 54 (96.4%) | 189 (78.8%) | |
| Yes | 2 (3.6%) | 51 (21.2%) | |
| Malaria treatment | 0.072 | ||
| No | 54 (96.4%) | 213 (88.4%) | |
| Yes | 2 (3.6%) | 28 (11.6%) | |
| Level | Variable | Crude PR (CI 80%) | p-Value | Adjusted PR (CI 90%) | p-Value |
|---|---|---|---|---|---|
| Region/village of residence | |||||
| Ariabú | 1 | 1 | |||
| Auaris | 1.07 (1.06–1.27) | 0.032 | 1.09 (0.97–1.22) | 0.222 | |
| Maturacá | 1.07 (0.97–1.16) | 0.385 | 1.04 (0.93–1.17) | 0.563 | |
| 1 | Household wall type | ||||
| Wood/brick | 1 | 1 | |||
| Clay | 1.15 (1.05–1.26) | 0.055 | 1.13 (1.01–1.26) | 0.088 | |
| Straw/no wall | 1.20 (1.06–1.35) | 0.053 | 1.19 (1.01–1.40) | 0.082 | |
| Gestational malaria | |||||
| No | 1 | 1 | |||
| Yes | 1.06 (1.07–1.25) | 0.014 | 1.12 (1.01–1.25) | 0.070 a | |
| 2 | Place of birth | ||||
| Hospital/Casai | 1 | 1 | |||
| Forest | 1.10 (1.04–1.34) | 0.092 | 1.17 (0.99–1.38) | 0.118 b | |
| Primary Healthcare Center (in the villages) | 1.11 (1.13–1.47) | 0.015 | 1.26 (1.05–1.51) | 0.041 b | |
| Age group (months) | |||||
| ≤23 | 1 | 1 | |||
| 24 to 59 | 1.08 (1.35–1.63) | 0.001 | 1.48 (1.30–1.67) | 0.001 c | |
| 3 | Child’s caregiver | ||||
| Mother or father | 1 | 1 | |||
| Other family member | 1.06 (1.05–1.20) | 0.034 | 1.10 (1.01–1.20) | 0.080 d | |
| 4 | Malaria treatment | ||||
| No | 1 | 1 | |||
| Yes | 1.06 (1.09–1.26) | 0.007 | 1.05 (0.95–1.17) | 0.412 e | |
| Child stunting (outcome) | |||||
| No | 1 | 1 | |||
| Yes | 1.34 (1.20–1.49) | 0.001 | 1.22 (1.07–1.38) | 0.012 f |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Orellana, J.D.Y.; Gatica-Domínguez, G.; Vaz, J.d.S.; Neves, P.A.R.; de Vasconcellos, A.C.S.; de Souza Hacon, S.; Basta, P.C. Intergenerational Association of Short Maternal Stature with Stunting in Yanomami Indigenous Children from the Brazilian Amazon. Int. J. Environ. Res. Public Health 2021, 18, 9130. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18179130
Orellana JDY, Gatica-Domínguez G, Vaz JdS, Neves PAR, de Vasconcellos ACS, de Souza Hacon S, Basta PC. Intergenerational Association of Short Maternal Stature with Stunting in Yanomami Indigenous Children from the Brazilian Amazon. International Journal of Environmental Research and Public Health. 2021; 18(17):9130. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18179130
Chicago/Turabian StyleOrellana, Jesem Douglas Yamall, Giovanna Gatica-Domínguez, Juliana dos Santos Vaz, Paulo Augusto Ribeiro Neves, Ana Claudia Santiago de Vasconcellos, Sandra de Souza Hacon, and Paulo Cesar Basta. 2021. "Intergenerational Association of Short Maternal Stature with Stunting in Yanomami Indigenous Children from the Brazilian Amazon" International Journal of Environmental Research and Public Health 18, no. 17: 9130. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18179130