
Interferon-γ-Inducible Chemokines as Prognostic Markers for Lung Cancer

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Sample Collection and Processing
2.3. Measurement of Cytokines
2.4. Statistical Analysis
3. Results
3.1. Demographic Data
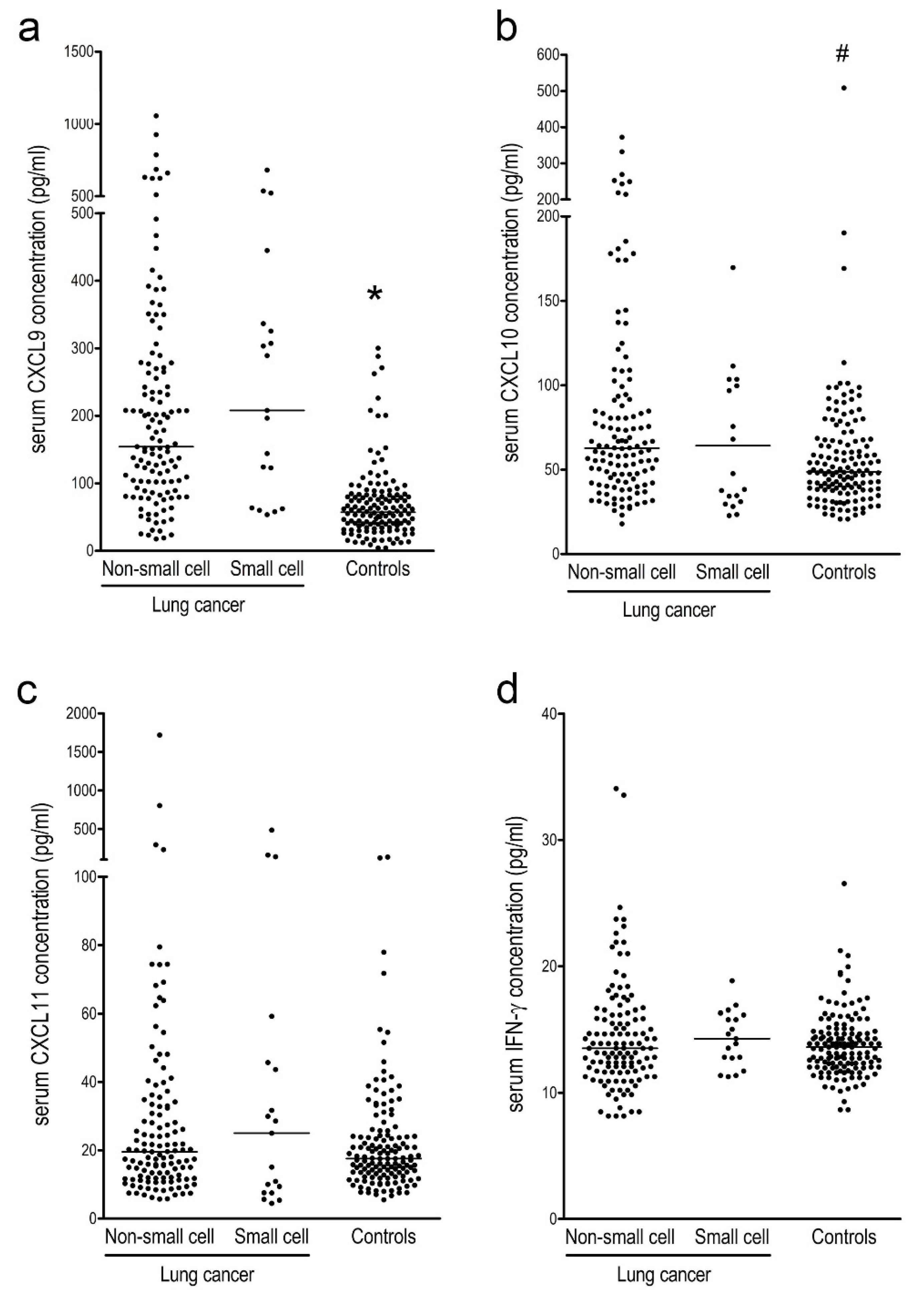
3.2. Serum IFN-γ-Inducible Chemokines and IFN-γ Levels in Lung Cancer Patients Compared to Controls
3.3. Serum IFN-γ-Inducible Chemokines and IFN-γ Levels in NSCLC and SCLC Patients
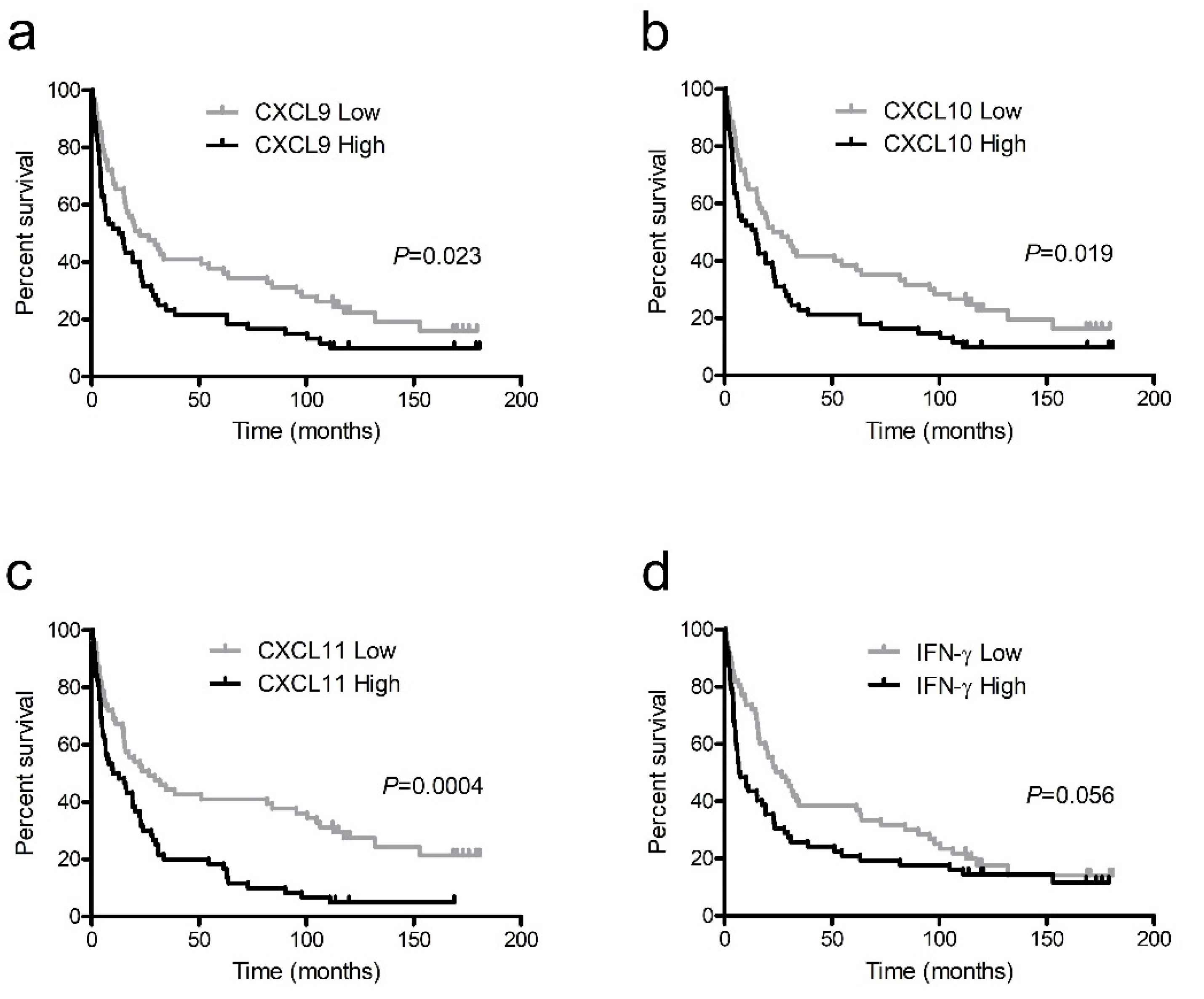
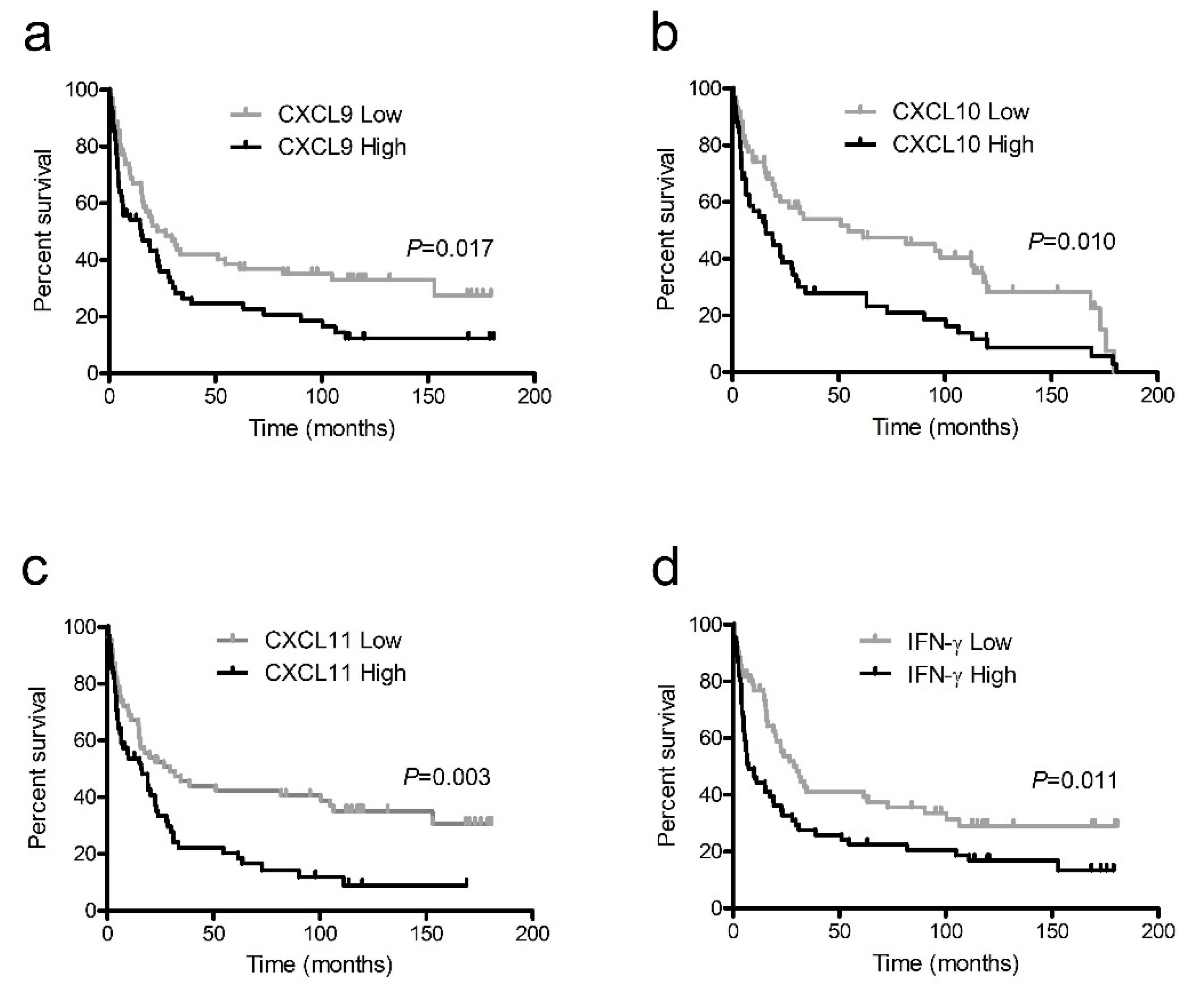
3.4. Survival Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hope, H.C.; Salmond, R.J. Targeting the tumor microenvironment and T cell metabolism for effective cancer immunotherapy. Eur. J. Immunol. 2019, 49, 1147–1152. [Google Scholar] [CrossRef] [Green Version]
- Sukari, A.; Nagasaka, M.; Al-Hadidi, A.; Lum, L.G. Cancer Immunology and Immunotherapy. Anticancer Res. 2016, 36, 5593–5606. [Google Scholar] [CrossRef]
- Nagarsheth, N.; Wicha, M.S.; Zou, W. Chemokines in the cancer microenvironment and their relevance in cancer immunotherapy. Nat. Rev. Immunol. 2017, 17, 559–572. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rainczuk, A.; Rao, J.; Gathercole, J.; Stephens, A.N. The emerging role of CXC chemokines in epithelial ovarian cancer. Reproduction 2012, 144, 303–317. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Groom, J.R.; Luster, A.D. CXCR3 in T cell function. Exp. Cell Res. 2011, 317, 620–631. [Google Scholar] [CrossRef]
- Tokunaga, R.; Zhang, W.; Naseem, M.; Puccini, A.; Berger, M.D.; Soni, S.; McSkane, M.; Baba, H.; Lenz, H.J. CXCL9, CXCL10, CXCL11/CXCR3 axis for immune activation—A target for novel cancer therapy. Cancer Treat. Rev. 2018, 63, 40–47. [Google Scholar] [CrossRef]
- Susek, K.H.; Karvouni, M.; Alici, E.; Lundqvist, A. The Role of CXC Chemokine Receptors 1–4 on Immune Cells in the Tumor Microenvironment. Front. Immunol. 2018, 9, 2159. [Google Scholar] [CrossRef] [PubMed]
- Metzemaekers, M.; Vanheule, V.; Janssens, R.; Struyf, S.; Proost, P. Overview of the Mechanisms that May Contribute to the Non-Redundant Activities of Interferon-Inducible CXC Chemokine Receptor 3 Ligands. Front. Immunol. 2017, 8, 1970. [Google Scholar] [CrossRef]
- Zaidi, M.R. The Interferon-Gamma Paradox in Cancer. J. Interferon Cytokine Res. 2019, 39, 30–38. [Google Scholar] [CrossRef] [PubMed]
- Abron, J.D.; Singh, N.P.; Murphy, A.E.; Mishra, M.K.; Price, R.L.; Nagarkatti, M.; Nagarkatti, P.S.; Singh, U.P. Differential role of CXCR3 in inflammation and colorectal cancer. Oncotarget 2018, 9, 17928–17936. [Google Scholar] [CrossRef] [Green Version]
- Oghumu, S.; Varikuti, S.; Terrazas, C.; Kotov, D.; Nasser, M.W.; Powell, C.A.; Ganju, R.K.; Satoskar, A.R. CXCR3 deficiency enhances tumor progression by promoting macrophage M2 polarization in a murine breast cancer model. Immunology 2014, 143, 109–119. [Google Scholar] [CrossRef] [PubMed]
- Topalian, S.L.; Hodi, F.S.; Brahmer, J.R.; Gettinger, S.N.; Smith, D.C.; McDermott, D.F.; Powderly, J.D.; Carvajal, R.D.; Sosman, J.A.; Atkins, M.B.; et al. Safety, activity, and immune correlates of anti-PD-1 antibody in cancer. N. Engl. J. Med. 2012, 366, 2443–2454. [Google Scholar] [CrossRef] [PubMed]
- Utsumi, T.; Suyama, T.; Imamura, Y.; Fuse, M.; Sakamoto, S.; Nihei, N.; Ueda, T.; Suzuki, H.; Seki, N.; Ichikawa, T. The association of CXCR3 and renal cell carcinoma metastasis. J. Urol. 2014, 192, 567–574. [Google Scholar] [CrossRef] [PubMed]
- Furuya, M.; Yoneyama, T.; Miyagi, E.; Tanaka, R.; Nagahama, K.; Miyagi, Y.; Nagashima, Y.; Hirahara, F.; Inayama, Y.; Aoki, I. Differential expression patterns of CXCR3 variants and corresponding CXC chemokines in clear cell ovarian cancers and endometriosis. Gynecol. Oncol. 2011, 122, 648–655. [Google Scholar] [CrossRef]
- Balan, M.; Pal, S. A novel CXCR3-B chemokine receptor-induced growth-inhibitory signal in cancer cells is mediated through the regulation of Bach-1 protein and Nrf2 protein nuclear translocation. J. Biol. Chem. 2014, 289, 3126–3137. [Google Scholar] [CrossRef] [Green Version]
- Mulligan, A.M.; Raitman, I.; Feeley, L.; Pinnaduwage, D.; Nguyen, L.T.; O’Malley, F.P.; Ohashi, P.S.; Andrulis, I.L. Tumoral lymphocytic infiltration and expression of the chemokine CXCL10 in breast cancers from the Ontario Familial Breast Cancer Registry. Clin. Cancer Res. 2013, 19, 336–346. [Google Scholar] [CrossRef] [Green Version]
- Kawada, K.; Hosogi, H.; Sonoshita, M.; Sakashita, H.; Manabe, T.; Shimahara, Y.; Sakai, Y.; Takabayashi, A.; Oshima, M.; Taketo, M.M. Chemokine receptor CXCR3 promotes colon cancer metastasis to lymph nodes. Oncogene 2007, 26, 4679–4688. [Google Scholar] [CrossRef]
- Liu, C.; Luo, D.; Reynolds, B.A.; Meher, G.; Katritzky, A.R.; Lu, B.; Gerard, C.J.; Bhadha, C.P.; Harrison, J.K. Chemokine receptor CXCR3 promotes growth of glioma. Carcinogenesis 2011, 32, 129–137. [Google Scholar] [CrossRef] [PubMed]
- Ma, X.; Norsworthy, K.; Kundu, N.; Rodgers, W.H.; Gimotty, P.A.; Goloubeva, O.; Lipsky, M.; Li, Y.; Holt, D.; Fulton, A. CXCR3 expression is associated with poor survival in breast cancer and promotes metastasis in a murine model. Mol. Cancer Ther. 2009, 8, 490–498. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toiyama, Y.; Fujikawa, H.; Kawamura, M.; Matsushita, K.; Saigusa, S.; Tanaka, K.; Inoue, Y.; Uchida, K.; Mohri, Y.; Kusunoki, M. Evaluation of CXCL10 as a novel serum marker for predicting liver metastasis and prognosis in colorectal cancer. Int. J. Oncol. 2012, 40, 560–566. [Google Scholar] [CrossRef]
- Flores, R.J.; Kelly, A.J.; Li, Y.; Nakka, M.; Barkauskas, D.A.; Krailo, M.; Wang, L.L.; Perlaky, L.; Lau, C.C.; Hicks, M.J.; et al. A novel prognostic model for osteosarcoma using circulating CXCL10 and FLT3LG. Cancer 2017, 123, 144–154. [Google Scholar] [CrossRef] [Green Version]
- Bolomsky, A.; Schreder, M.; Hubl, W.; Zojer, N.; Hilbe, W.; Ludwig, H. Monokine induced by interferon gamma (MIG/CXCL9) is an independent prognostic factor in newly diagnosed myeloma. Leuk. Lymphoma 2016, 57, 2516–2525. [Google Scholar] [CrossRef] [PubMed]
- Hsin, L.J.; Kao, H.K.; Chen, I.H.; Tsang, N.M.; Hsu, C.L.; Liu, S.C.; Chang, Y.S.; Chang, K.P. Serum CXCL9 levels are associated with tumor progression and treatment outcome in patients with nasopharyngeal carcinoma. PLoS ONE 2013, 8, e80052. [Google Scholar] [CrossRef] [Green Version]
- Chang, K.P.; Wu, C.C.; Fang, K.H.; Tsai, C.Y.; Chang, Y.L.; Liu, S.C.; Kao, H.K. Serum levels of chemokine (C-X-C motif) ligand 9 (CXCL9) are associated with tumor progression and treatment outcome in patients with oral cavity squamous cell carcinoma. Oral Oncol. 2013, 49, 802–807. [Google Scholar] [CrossRef] [PubMed]
- Shiels, M.S.; Katki, H.A.; Hildesheim, A.; Pfeiffer, R.M.; Engels, E.A.; Williams, M.; Kemp, T.J.; Caporaso, N.E.; Pinto, L.A.; Chaturvedi, A.K. Circulating Inflammation Markers, Risk of Lung Cancer, and Utility for Risk Stratification. J. Natl. Cancer Inst. 2015, 107, djv199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spaks, A.; Jaunalksne, I.; Spaka, I.; Chudasama, D.; Pirtnieks, A.; Krievins, D. Diagnostic Value of Circulating CXC Chemokines in Non-small Cell Lung Cancer. Anticancer Res. 2015, 35, 6979–6983. [Google Scholar]
- Spaks, A. Role of CXC group chemokines in lung cancer development and progression. J. Thorac. Dis. 2017, 9, S164–S171. [Google Scholar] [CrossRef] [Green Version]
- Detterbeck, F.C.; Boffa, D.J.; Kim, A.W.; Tanoue, L.T. The Eighth Edition Lung Cancer Stage Classification. Chest 2017, 151, 193–203. [Google Scholar] [CrossRef]
- Micke, P.; Faldum, A.; Metz, T.; Beeh, K.M.; Bittinger, F.; Hengstler, J.G.; Buhl, R. Staging small cell lung cancer: Veterans Administration Lung Study Group versus International Association for the Study of Lung Cancer—What limits limited disease? Lung Cancer 2002, 37, 271–276. [Google Scholar] [CrossRef]
- Chung, W.; Lee, K.; Jung, Y.; Kim, Y.; Park, J.; Sheen, S.; Lee, J.; Kang, D.; Park, K. Serum CXCR3 ligands as biomarkers for the diagnosis and treatment monitoring of tuberculosis. Int. J. Tuberc. Lung Dis. 2015, 19, 1476–1484. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.; Chung, W.; Jung, Y.; Kim, Y.; Park, J.; Sheen, S.; Park, K. CXCR3 ligands as clinical markers for pulmonary tuberculosis. Int. J. Tuberc. Lung Dis. 2015, 19, 191–199. [Google Scholar] [CrossRef] [PubMed]
- Zhi, W.; Ferris, D.; Sharma, A.; Purohit, S.; Santos, C.; He, M.; Ghamande, S.; She, J.X. Twelve serum proteins progressively increase with disease stage in squamous cell cervical cancer patients. Int. J. Gynecol. Cancer 2014, 24, 1085–1092. [Google Scholar] [CrossRef] [PubMed]
- Ding, Q.; Xia, Y.; Ding, S.; Lu, P.; Sun, L.; Liu, M. An alternatively spliced variant of CXCR3 mediates the metastasis of CD133+ liver cancer cells induced by CXCL9. Oncotarget 2016, 7, 14405–14414. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baj-Krzyworzeka, M.; Weglarczyk, K.; Baran, J.; Szczepanik, A.; Szura, M.; Siedlar, M. Elevated level of some chemokines in plasma of gastric cancer patients. Cent. Eur. J. Immunol. 2016, 41, 358–362. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andersson, A.; Yang, S.C.; Huang, M.; Zhu, L.; Kar, U.K.; Batra, R.K.; Elashoff, D.; Strieter, R.M.; Dubinett, S.M.; Sharma, S. IL-7 promotes CXCR3 ligand-dependent T cell antitumor reactivity in lung cancer. J. Immunol. 2009, 182, 6951–6958. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Lung Cancer | Control | p-Value | |
|---|---|---|---|
| Number | 144 | 140 | |
| Age (years) | 69 (61–75) | 63 (58–69) | NS |
| Male | 106 (73.6) | 94 (67.1) | NS |
| Smoker | 79 (54.9) | 50 (35.7) | <0.01 |
| History of diseases | |||
| Tuberculosis | 5 | 4 | |
| Other malignancies | 7 | 0 | |
| Concomitant diseases | |||
| Diabetes mellitus | 5 | 0 | |
| Liver cirrhosis | 2 | 0 | |
| IPF | 3 | 0 | |
| Cell types | |||
| NSCLC | 125 (86.8) | ||
| Squamous | 40 (27.8) | ||
| Adenocarcinoma | 68 (47.2) | ||
| Large cell | 4 (2.7) | ||
| Others | 13 (9.0) | ||
| SCLC | 19 (13.1) | ||
| Stages | |||
| NSCLC | |||
| I | 37 (25.7) | ||
| II | 13 (9.0) | ||
| III | 37 (25.7) | ||
| IV | 38 (26.4) | ||
| SCLC | |||
| Limited | 9 (6.3) | ||
| Extensive | 10 (6.9) | ||
| Treatment modalities | |||
| NSCLC | |||
| Surgical resection | 72 (50.0) | ||
| Chemotherapy alone | 12 (8.3) | ||
| Radiotherapy alone | 20 (13.9) | ||
| Chemoradiotherapy | 12 (8.3) | ||
| Palliative treatment | 9 (6.2) | ||
| SCLC | |||
| Chemotherapy alone | 5 (3.5) | ||
| Radiotherapy alone | 2 (1.4) | ||
| Chemoradiotherapy | 7 (4.9) | ||
| Palliative treatment | 5 (3.5) |
| Stage | No. | CXCL9 (pg/mL) | CXCL10 (pg/mL) | CXCL11 (pg/mL) | IFN-γ (pg/mL) |
|---|---|---|---|---|---|
| NSCLC | |||||
| I–III | 87 | 149.2 (86.2–234.9) | 58.5 (40.5–81.0) | 17.0 (11.3–30.4) | 12.8 (11.6–15.1) |
| I | 37 | 158.4 (112.0–231.5) | 50.9 (32.8–74.7) | 15.8 (11.2–26.6) | 12.8 (12.0–15.1) |
| II | 13 | 133.9 (82.7–207.6) | 66.8 (40.5–73.8) | 17.8 (12.7–37.3) | 12.8 (12.0–15.5) |
| III | 37 | 125.8 (79.8–242.9) | 60.0 (47.391.2) | 20.2 (10.8–28.5) | 13.2 (11.6–15.5) |
| IV | 38 | 207.4 (102.5–349.8) * | 79.0 (54.1–129.0) #,† | 22.9 (15.9–41.2) * | 15.0 (13.1–17.7) * |
| SCLC | |||||
| Limited | 9 | 170.3 (124.3–208.1) | 60.0 (37.6–99.7) | 21.8 (9.8–30.0) | 13.9 (12.8–15.8) |
| Extensive | 10 | 296.2 (62.3–336.5) | 34.6 (29.6–68.1) | 17.9 (7.5–59.3) | 14.3 (12.8–15.8) |
| Variable | Univariate | Multivariate | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | |
| Overall survival | ||||||
| Age (<60/≥60) | 1.98 | 1.22–3.21 | <0.001 | 1.05 | 1.02–1.07 | <0.0001 |
| Sex (male/female) | 0.86 | 0.56–1.34 | 0.513 | |||
| Smoking (smoker/non-smoker) | 0.85 | 0.58–1.25 | 0.402 | |||
| Histology (adenocarcinoma/squamous/others) | 2.86 | 0.60–1.04 | 0.092 | |||
| Stage (I/II/III/IV) | 2.20 | 1.79–2.70 | <0.0001 | 2.26 | 1.84–2.78 | <0.0001 |
| CXCL9 (High/Low) | 1.62 | 1.10–2.40 | 0.015 | 1.82 | 1.22–2.70 | 0.003 |
| CXCL10 (High/Low) | 1.90 | 1.28–2.83 | 0.002 | 1.36 | 0.89–2.07 | 0.146 |
| CXCL11 (High/Low) | 1.82 | 1.23–2.71 | 0.003 | 1.70 | 1.12–2.59 | 0.013 |
| IFN-γ (High/Low) | 1.43 | 0.97–2.11 | 0.068 | 1.32 | 0.88–1.98 | 0.185 |
| Cancer-specific survival | ||||||
| Age (<60/≥60) | 1.71 | 1.03–2.82 | 0.037 | 1.05 | 1.02–1.07 | <0.0001 |
| Sex (male/female) | 0.926 | 0.58–1.47 | 0.744 | |||
| Smoking (smoker/non-smoker) | 0.81 | 0.54–1.23 | 0.326 | |||
| Histology (adenocarcinoma/ squamous/others) | 0.89 | 0.66–1.19 | 0.427 | |||
| Stage (I/II/III/IV) | 2.48 | 1.70–3.13 | <0.0001 | 2.68 | 2.12–3.38 | <0.0001 |
| CXCL9 (High/Low) | 1.68 | 1.11–2.54 | 0.015 | 1.91 | 1.25–2.93 | 0.003 |
| CXCL10 (High/Low) | 1.98 | 1.29–3.03 | 0.002 | 1.30 | 0.83–2.05 | 0.25 |
| CXCL11 (High/Low) | 1.76 | 1.15–2.68 | 0.009 | 1.50 | 0.96–2.33 | 0.074 |
| IFN-γ (High/Low) | 1.62 | 1.07–2.46 | 0.021 | 1.44 | 0.93–2.23 | 0.106 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, K.-S.; Chung, W.-Y.; Park, J.-E.; Jung, Y.-J.; Park, J.-H.; Sheen, S.-S.; Park, K.-J. Interferon-γ-Inducible Chemokines as Prognostic Markers for Lung Cancer. Int. J. Environ. Res. Public Health 2021, 18, 9345. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18179345
Lee K-S, Chung W-Y, Park J-E, Jung Y-J, Park J-H, Sheen S-S, Park K-J. Interferon-γ-Inducible Chemokines as Prognostic Markers for Lung Cancer. International Journal of Environmental Research and Public Health. 2021; 18(17):9345. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18179345
Chicago/Turabian StyleLee, Keu-Sung, Wou-Young Chung, Ji-Eun Park, Yun-Jung Jung, Joo-Hun Park, Seung-Soo Sheen, and Kwang-Joo Park. 2021. "Interferon-γ-Inducible Chemokines as Prognostic Markers for Lung Cancer" International Journal of Environmental Research and Public Health 18, no. 17: 9345. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18179345