
Delayed Discharge for Non-Clinical Reasons in Hip Procedures: Differential Characteristics and Opportunity Cost

 ,
,  , , , , and
, , , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Location and Population
2.2. Variables
2.3. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| MBDSDH | Minimum basic data set on discharge at hospital |
| DRG | Diagnostic related groups |
| HP | Hip procedures |
| HCU | Hospital complexity unit |
| SD | Standard deviation |
| 95% CI | 95% Confidence interval |
Appendix A. Diagnosis-Related Group (DRG) Included in the Hip Procedures Group. Cantabria (Northern Spain), 2007–2015
| 210 (hip and femur procedures except major joints, over 17 years of age with complications) 211 (hip and femur procedures except major joint, over 17 years of age without complications) 235 (femur fractures) 236 (hip and pelvis fractures) 558 (major musculoskeletal procedures with major complication) 817 (hip replacement revision or hip replacement due to complications) 818 (hip replacement except for complications) |
References
- Rojas-García, A.; Turner, S.; Pizzo, E.; Hudson, E.; Thomas, J.; Raine, R. Impact and experiences of delayed discharge: A mixed-studies systematic review. Health Expect. 2018, 21, 41–56. [Google Scholar] [CrossRef]
- Landeiro, F.; Roberts, K.; Gray, A.M.; Leal, J. Delayed hospital discharges of older patients: A systematic review on prevalence and costs. Gerontologist 2019, 59, e86–e97. [Google Scholar] [CrossRef]
- National Services Scotland. Delayed Discharges in NHSScotland. Annual Summary of Occupied Bed Days and Census Figures up to March 2019. Available online: https://www.isdscotland.org/Health-Topics/Health-and-Social-Community-Care/Publications/2019-09-17/2019-09-17-DelayedDischarges-Annual-Report.pdf?73035830260 (accessed on 3 March 2020).
- Pellico-López, A.; Cantarero, D.; Fernández-Feito, A.; Parás-Bravo, P.; Cayón de Las Cuevas, J.; Paz-Zulueta, M. Factors associated with bed-blocking at a university hospital (Cantabria, Spain) between 2007 and 2015: A retrospective observational study. Int. J. Environ. Res. Public Health 2019, 16, 3304. [Google Scholar] [CrossRef] [Green Version]
- Hwang, J.I. Characteristics of patient and healthcare service utilization associated with inappropriate hospitalization days. J. Adv. Nurs. 2007, 60, 654–662. [Google Scholar] [CrossRef] [PubMed]
- Ou, L.; Young, L.; Chen, J.; Santiano, N.; Baramy, L.S.; Hillman, K. Discharge delay in acute care: Reasons and determinants of delay in general ward patients. Aust. Health Rev. 2009, 33, 513–521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barton, M.; McClean, S.; Garg, L.; Fullerton, K. Modelling costs of bed occupancy and delayed discharge of post-stroke patients. In Proceedings of the 2010 IEEE Workshop on Health Care Management (WHCM), Venice, Italy, 18–20 February 2010; pp. 1–6. [Google Scholar] [CrossRef]
- Manzano-Santaella, A. From bed-blocking to delayed discharges: Precursors and interpretations of a contested concept. Health Serv. Manag. Res. 2010, 23, 121–127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lorén Guerrero, L.; Gascón Catalán, A. Biopsychosocial factors related to the length of hospital stay in older people. Rev. Lat. Am. Enferm. 2011, 19, 1377–1384, (In English, Portuguese and Spanish). [Google Scholar] [CrossRef] [Green Version]
- Amy, C.; Zagorski, B.; Chan, V.; Parsons, D.; Vander Laan, R.; Colantonio, A. Acute care alternate-level-of-care days due to delayed discharge for traumatic and non-traumatic brain injuries. Healthc. Policy 2012, 7, 41–55. [Google Scholar]
- Holmås, T.H.; Islam, M.K.; Kjerstad, E. Interdependency between social care and hospital care: The case of hospital length of stay. Eur. J. Public Health 2013, 23, 927–933. [Google Scholar] [CrossRef] [Green Version]
- Challis, D.; Hughes, J.; Xie, C.; Jolley, D. An examination of factors influencing delayed discharge of older people from hospital. Int. J. Geriatr. Psychiatry 2014, 29, 160–168. [Google Scholar] [CrossRef]
- Lenzi, J.; Mongardi, M.; Rucci, P.; Di Ruscio, E.; Vizioli, M.; Randazzo, C.; Toschi, E.; Carradori, T.; Fantini, M.P. Sociodemographic, clinical and organisational factors associated with delayed hospital discharges: A cross-sectional study. BMC Health Serv. Res. 2014, 14, 128. [Google Scholar] [CrossRef] [Green Version]
- McCloskey, R.; Jarrett, P.; Stewart, C.; Nicholson, P. Alternate level of care patients in hospitals: What does dementia have to do with this? Can. Geriatr. J. 2014, 17, 88–94. [Google Scholar] [CrossRef] [Green Version]
- Gaughan, J.; Gravelle, H.; Santos, R.; Siciliani, L. Long-term care provision, hospital bed blocking, and discharge destination for hip fracture and stroke patients. Int. J. Health Econ. Manag. 2017, 17, 311–331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hendy, P.; Patel, J.H.; Kordbacheh, T.; Laskar, N.; Harbord, M. In-depth analysis of delays to patient discharge: A metropolitan teaching hospital experience. Clin. Med. 2012, 12, 320–323. [Google Scholar] [CrossRef]
- Salonga-Reyes, A.; Scott, I.A. Stranded: Causes and effects of discharge delays involving non-acute in-patients requiring maintenance care in a tertiary hospital general medicine service. Aust. Health Rev. 2017, 41, 54–62. [Google Scholar] [CrossRef]
- Stock, D.; Cowie, C.; Chan, V.; Colantonio, A.; Wodchis, W.P.; Alter, D.; Cullen, N. Determinants of alternate-level-of-care delayed discharge among acute care survivors of hypoxic-ischemic brain injury: A population-based cohort study. CMAJ Open 2016, 4, E689–E697. [Google Scholar] [CrossRef] [Green Version]
- Instituto Cántabro de Estadística. Población Por Sexo y Grandes Grupos de Edad. Available online: https://www.icane.es/data/municipal-register-gender-large-age-group#timeseries (accessed on 11 January 2021).
- Holmås, T.H.; Islam, M.K.; Kjerstad, E. Between two beds: Inappropriately delayed discharges from hospitals. Int. J. Health Care Financ. Econ. 2013, 13, 201–217. [Google Scholar] [CrossRef] [PubMed]
- Tan, W.S.; Chong, W.F.; Chua, K.S.; Heng, B.H.; Chan, K.F. Factors associated with delayed discharges after inpatient stroke rehabilitation in Singapore. Ann. Acad. Med. Singap. 2010, 39, 435–441. [Google Scholar]
- Mendoza Giraldo, D.; Navarro, A.; Sánchez-Quijano, A.; Villegas, A.; Asencio, R.; Lissen, E. Retraso del alta hospitalaria por motivos no médicos [Impact of delayed discharge for nonmedical reasons in a tertiary hospital internal medicine department]. Rev. Clin. Esp. 2012, 212, 229–234. [Google Scholar] [CrossRef] [PubMed]
- Landeiro, F.; Leal, J.; Gray, A.M. The impact of social isolation on delayed hospital discharges of older hip fracture patients and associated costs. Osteoporos. Int. 2016, 27, 737–745. [Google Scholar] [CrossRef]
- Sáez-López, P.; Ojeda-Thies, C.; Alarcón, T.; Muñoz Pascual, A.; Mora-Fernández, J.; González de Villaumbrosia, C.; Molina Hernández, M.J.; Montero-Fernández, N.; Cancio Trujillo, J.M.; Díez Pérez, A.; et al. Registro nacional de fracturas de cadera (RNFC): Resultados del primer año y comparación con otros registros y estudios multicéntricos españoles [Spanish national hip fracture registry (RNFC): First-year results and comparison with other registries and prospective multi-centric studies from Spain]. Rev. Esp. Salud Pública 2019, 93, e201910072. (In Spanish) [Google Scholar]
- Costa-Font, J.; Jimenez-Martin, S.; Vilaplana, C. Does long-term care subsidization reduce hospital admissions and utilization? J. Health Econ. 2018, 58, 43–66. [Google Scholar] [CrossRef]
- Ministerio de Sanidad; Consumo y Bienestar Social. Catálogo Nacional de Hospitales. Información Anual Sobre Años Anteriores. 2019. Available online: https://www.mscbs.gob.es/ciudadanos/prestaciones/centrosServiciosSNS/hospitales/aniosAnteriores.htm (accessed on 22 January 2021).
- Servicio Cántabro de Salud. Hospital Universitario Marqués de Valdecilla. 2019. Available online: http://www.scsalud.es/web/scs/hospital-marques-de-valdecilla (accessed on 11 January 2021).
- Yetano Laguna, J.; López Arbeloa, G. Manual de Descripción de los Grupos Relacionados Por el Diagnóstico (AP-GRD V 25.0); Osakidetza, Administración de la Comunidad Autónoma del País Vasco: Vitoria-Gasteiz, Spain, 2010. Available online: https://www.osakidetza.euskadi.eus/contenidos/informacion/osk_publicaciones/es_publi/adjuntos/calidad/ManualAPGRDv.25.0.pdf (accessed on 22 January 2021).
- Moore, G.; Hartley, P.; Romero-Ortuno, R. Health and social factors associated with a delayed discharge amongst inpatients in acute geriatric wards: A retrospective observational study. Geriatr. Gerontol. Int. 2018, 18, 530–537. [Google Scholar] [CrossRef]
- National Health Service. Monthly Delayed Transfers of Care Situation Report. Principles, Definitions and Guidance. 2018. Available online: https://www.england.nhs.uk/statistics/wp-content/uploads/sites/2/2018/11/Monthly-Delayed-Transfers-of-Care-Situation-Report-Principles-Definitions-and-Guidance.pdf (accessed on 22 January 2021).
- Secretaría general de Sanidad D.G. de Salud Pública, Calidad e Innovación. Sistema de información sobre listas de espera en el Sistema Nacional de Salud. 2015. Available online: https://www.mscbs.gob.es/estadEstudios/estadisticas/inforRecopilaciones/docs/Datos_ccaa_dic2015.pdf (accessed on 22 January 2020).
- Björnberg, A.; Phang, A.Y. Eurohealth Consumer Index. Health Consumer Powerhouse. 2019. Available online: https://healthpowerhouse.com/media/EHCI-2018/EHCI-2018-report.pdf (accessed on 22 January 2021).
- Bardales Mas, Y.; González Montalvo, J.I.; Abizanda Soler, P.; Alarcón Alarcón, M.T. Guías clínicas de fractura de cadera. Comparación de sus principales recomendaciones [Hip fracture guidelines. A comparison of the main recommendations]. Rev. Esp. Geriatr. Gerontol. 2012, 47, 220–227. [Google Scholar] [CrossRef]
- Azagra, R.; López-Expósito, F.; Martin-Sánchez, J.C.; Aguyé-Batista, A.; Gabriel-Escoda, P.; Zwart, M.; Díaz-Herrera, M.A.; Pujol-Salud, J.; Iglesias-Martínez, M.; Puchol-Ruiz, N. Incidencia de la fractura de fémur en España (1997–2010) [Incidence of hip fracture in Spain (1997–2010)]. Med. Clin. 2015, 145, 465–470. [Google Scholar] [CrossRef]
- Albarracin Serra, A. La producción sanitaria: Codificación de enfermedades y procedimientos. Escuela Nacional de Sanidad. 2012. Available online: http://e-spacio.uned.es/fez/eserv/bibliuned%3A500676/n8.1_La_producci__n_sanitaria.pdf (accessed on 22 February 2020).
- Fernández Castañer, M.; Salazar Soler, A.; Bartolomé Sarvisé, C.; Ridao March, M.L.; Casado Garcia, M.A.; Castilla Fuentes, M.; Ortiga Fontgivell, B.; García Díaz, A.; Corbella, X. Impacto de la crisis económica en la actividad y eficiencia de un hospital terciario universitario [Impact of the financial crisis on activity and efficiency at a high-technology university hospital]. Rev. Esp. Salud Pública 2018, 92, e201808052. (In Spanish) [Google Scholar]
- Gonçalves-Bradley, D.C.; Lannin, N.A.; Clemson, L.M.; Cameron, I.D.; Shepperd, S. Discharge planning from hospital. Cochrane Database Syst. Rev. 2016, 2016, CD000313. [Google Scholar] [CrossRef] [PubMed]
- Coindre, J.P.; Crochette, R.; Breuer, C.; Piccoli, G.B. Why are hospitalisations too long? A simple checklist for identifying the main social barriers to hospital discharge from a nephrology ward. BMC Nephrol. 2018, 19, 227. [Google Scholar] [CrossRef] [Green Version]
- Bryan, K. Policies for reducing delayed discharge from hospital. Br. Med. Bull. 2010, 95, 33–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dahl, U.; Johnsen, R.; Sætre, R.; Steinsbekk, A. The influence of an intermediate care hospital on health care utilization among elderly patients—A retrospective comparative cohort study. BMC Health Serv. Res. 2015, 15, 48. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
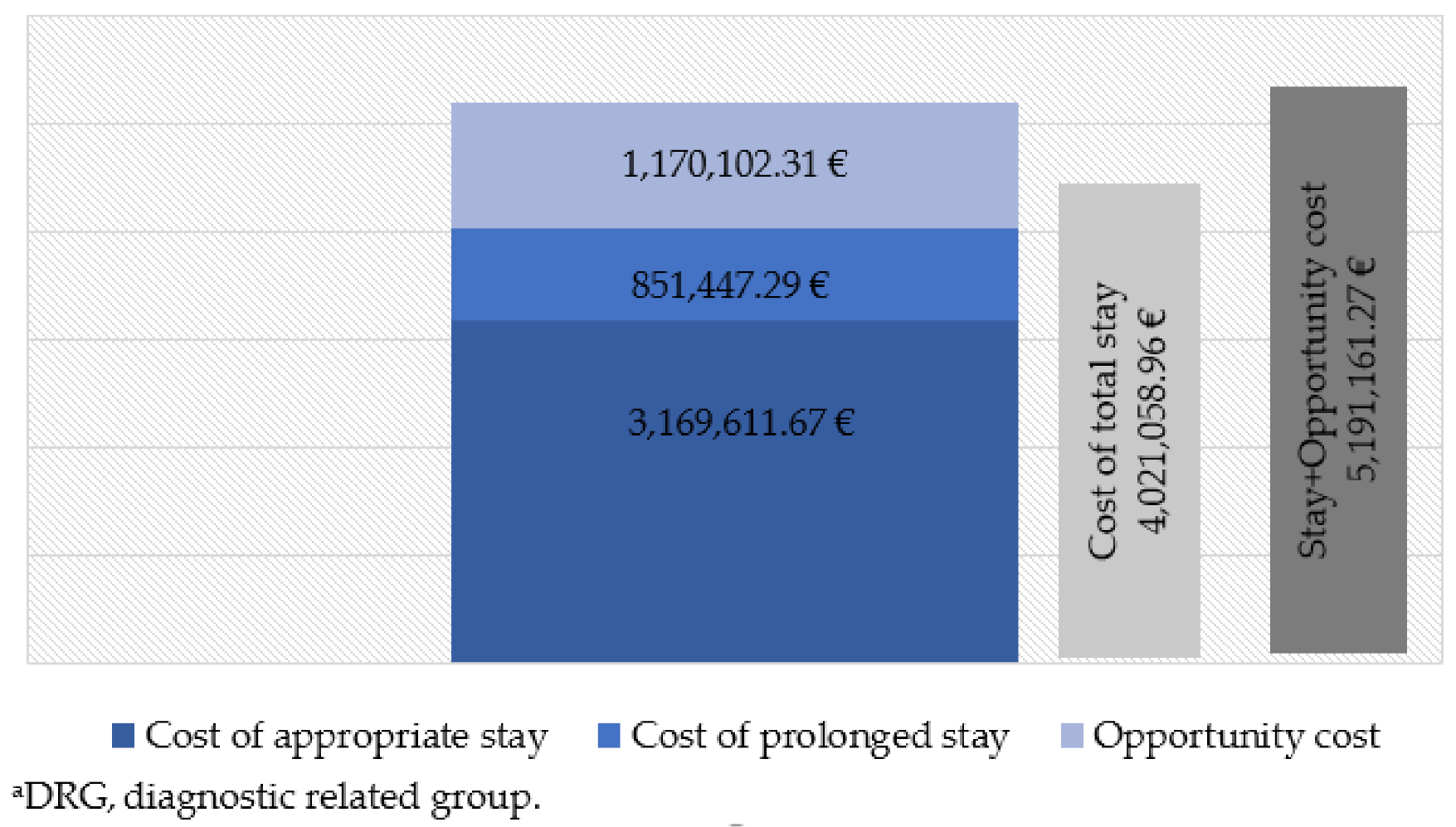
| Cost of appropriate stay = Days of appropriate stay × cost stay per DRG a |
| Cost of prolonged stay = Days of prolonged stay × cost stay in hospitalization unit |
| Opportunity cost = ((Prolonged stay/Average length of stay) × Average DRG weight a) × Cost according to HCU b |
| Hip Procedures (n = 306) | SD a | Non-Hip Procedures (n = 2709) | SD a | p-Value | |
|---|---|---|---|---|---|
| Total stay (days) | 22.69 | [29.65] | 29.18 | [30.08] | <0.001 |
| Appropriate stay (days) | 15.58 | [21.13] | 21.82 | [23.31] | <0.001 |
| Prolonged stay (days) | 7.12 | [13.78] | 7.36 | [16.11] | 0.800 |
| Cost of appropriate hospital stay (euros) | 12,411.25 | [13,899.74] | 15,237.43 | [24,609.78] | 0.049 |
| Cost of prolonged stay (euros) | 2094.78 | [4250.07] | 2128.64 | [4482.92] | 0.900 |
| Total cost of hospital stay (euros) | 14,506.03 | [16,029.90] | 17,366.07 | [25,577.87] | 0.056 |
| Opportunity cost (euros) | 3016.33 | [4265.95] | 3432.74 | [6832.01] | 0.297 |
| Hip Procedures (n = 306) | SD a, 95% CI b | Non-Hip Procedures (n = 2709) | SD a, 95% CI b | p-Value | ||
|---|---|---|---|---|---|---|
| Sex | Male | 74 (24.18%) | (19.49–29.39) | 1370 (50.57%) | (4867–5247) | <0.001 |
| Female | 232 (75.82%) | (70.62–80.51) | 1339 (49.43%) | (47.53–51.33) | ||
| Age (years) | 82.73 | [9.505] | 76.78 | [12.055] | <0.001 | |
| DRG c Weight | 3.401 | [1.464] | 3.805 | [6.782] | 0.299 | |
| Place of residence | Rural d | 45 (14.71%) | (10.93–19.18) | 633 (23.37%) | (21.78–25.01) | 0.001 |
| Urban e | 261 (85.29%) | (80.82–89.07) | 2076 (76.63%) | (74.99–78.22) | ||
| Type of admission | Programmed | 28 (9.15%) | (6.17–12.95) | 183 (6.75%) | (5.84–7.77) | 0.150 |
| Urgent | 278 (90.85%) | (87.05–93.83) | 2526 (93.25%) | (92.23–94.16) | ||
| Discharge destination | Long term stay | 255 (83.33%) | (78.68–87.33) | 2122 (78.33%) | (76.73–79.87) | 0.001 |
| Home | 46 (15.03%) | (11.22–19.54) | 366 (13.51%) | (12.25–14.86) | ||
| Deceased | 4 (1.31%) | (0.36–3.31) | 194 (7.16%) | (6.22–8.19) | ||
| Other f | 1 (0.33%) | (0.01–1.81) | 27 (0.99%) | (0.66–1.45) | ||
| Year of medical discharge | 2007 | 42 (13.73%) | (10.07–18.09) | 332 (12.25%) | (11.04–13.55) | 0.939 |
| 2008 | 47 (15.36%) | (11.51–19.89) | 400 (14.77%) | (13.45–16.16) | ||
| 2009 | 37 (12.09%) | (8.66–16.28) | 336 (12.40%) | (11.18–13.70) | ||
| 2010 | 35 (11.44%) | (8.09–15.55) | 331 (12.22%) | (11.01–13.51) | ||
| 2011 | 46 (15.03%) | (11.22–19.54) | 350 (12.92%) | (11.68–14.24) | ||
| 2012 | 28 (9.15%) | (6.17–12.95) | 264 (9.75%) | (8.65–10.92) | ||
| 2013 | 26 (8.49%) | (5.63–12.20) | 252 (9.30%) | (8.23–10.46) | ||
| 2014 | 23 (7.52%) | (4.82–11.06) | 201 (7.42%) | (6.46–8.47) | ||
| 2015 | 22 (7.19%) | (4.56–10.68) | 243 (8.97%) | (7.92–10.11) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pellico-López, A.; Fernández-Feito, A.; Cantarero, D.; Herrero-Montes, M.; Cayón-De Las Cuevas, J.; Parás-Bravo, P.; Paz-Zulueta, M. Delayed Discharge for Non-Clinical Reasons in Hip Procedures: Differential Characteristics and Opportunity Cost. Int. J. Environ. Res. Public Health 2021, 18, 9407. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18179407
Pellico-López A, Fernández-Feito A, Cantarero D, Herrero-Montes M, Cayón-De Las Cuevas J, Parás-Bravo P, Paz-Zulueta M. Delayed Discharge for Non-Clinical Reasons in Hip Procedures: Differential Characteristics and Opportunity Cost. International Journal of Environmental Research and Public Health. 2021; 18(17):9407. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18179407
Chicago/Turabian StylePellico-López, Amada, Ana Fernández-Feito, David Cantarero, Manuel Herrero-Montes, Joaquín Cayón-De Las Cuevas, Paula Parás-Bravo, and María Paz-Zulueta. 2021. "Delayed Discharge for Non-Clinical Reasons in Hip Procedures: Differential Characteristics and Opportunity Cost" International Journal of Environmental Research and Public Health 18, no. 17: 9407. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18179407