
Parental Monitoring, Individual Dispositions, and Alcohol Use Disorder: A Longitudinal Study with Young Swiss Men


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Measures
2.3.1. Alcohol Use Disorder (AUD)
2.3.2. Parental Monitoring
2.3.3. Coping Strategies
2.3.4. Sensation Seeking
2.3.5. Confounding Variables
2.4. Statistical Analysis
3. Results
3.1. Main Effects
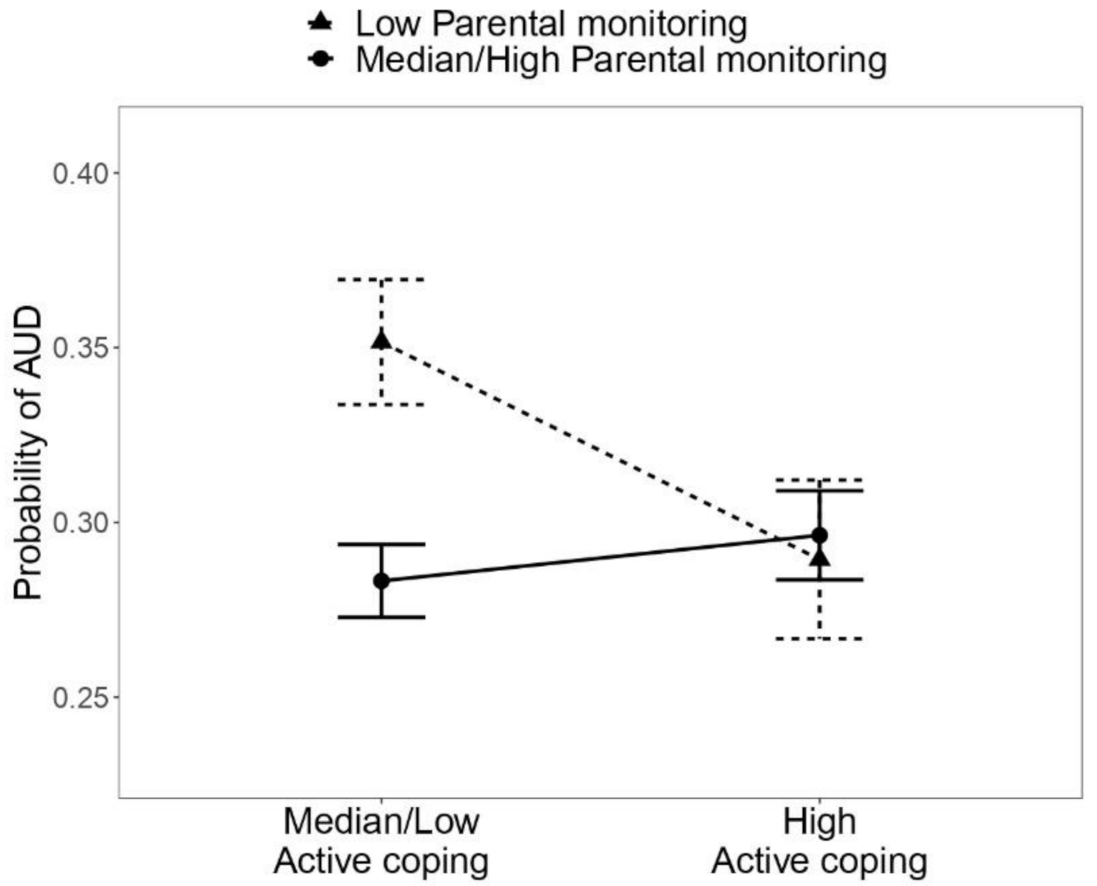
3.2. Interaction Effects
4. Discussion
5. Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Grant, B.F.; Stinson, F.S.; Dawson, D.A.; Chou, S.P.; Dufour, M.C.; Compton, W.; Pickering, R.P.; Kaplan, K. Prevalence and co-occurrence of substance use disorders and independent mood and anxiety disorders: Results from the national epidemiologic survey on alcohol and related conditions. Arch. Gen. Psychiatry 2004, 61, 807–816. [Google Scholar] [CrossRef]
- Wittchen, H.-U.; Jacobi, F.; Rehm, J.; Gustavsson, A.; Svensson, M.; Jönsson, B.; Olesen, J.; Allgulander, C.; Alonso, J.; Faravelli, C. The size and burden of mental disorders and other disorders of the brain in Europe 2010. Eur. Neuropsychopharmacol. 2011, 21, 655–679. [Google Scholar] [CrossRef] [Green Version]
- Hasin, D.S.; Stinson, F.S.; Ogburn, E.; Grant, B.F. Prevalence, correlates, disability, and comorbidity of DSM-IV alcohol abuse and dependence in the United States: Results from the national epidemiologic survey on alcohol and related conditions. Arch. Gen. Psychiatry 2007, 64, 830–842. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Global Status Report on Alcohol and Health 2018; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- DeWit, D.J.; Adlaf, E.M.; Offord, D.R.; Ogborne, A.C. Age at first alcohol use: A risk factor for the development of alcohol disorders. Am. J. Psychiatry 2000, 157, 745–750. [Google Scholar] [CrossRef]
- Grant, B.F.; Dawson, D.A. Age at onset of alcohol use and its association with DSM-IV alcohol abuse and dependence: Results from the national longitudinal alcohol epidemiologic survey. J. Subst. Abus. 1997, 9, 103–110. [Google Scholar] [CrossRef]
- Yap, M.B.H.; Cheong, T.W.K.; Zaravinos-Tsakos, F.; Lubman, D.I.; Jorm, A.F. Modifiable parenting factors associated with adolescent alcohol misuse: A systematic review and meta-analysis of longitudinal studies. Addiction 2017, 112, 1142–1162. [Google Scholar] [CrossRef] [PubMed]
- Meque, I.; Salom, C.; Betts, K.S.; Alati, R. Predictors of alcohol use disorders among young adults: A systematic review of longitudinal studies. Alcohol Alcohol. 2019, 54, 310–324. [Google Scholar] [CrossRef]
- Ryan, S.M.; Jorm, A.F.; Lubman, D.I. Parenting factors associated with reduced adolescent alcohol use: A systematic review of longitudinal studies. Aust. N. Z. J. Psychiatry 2010, 44, 774–783. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. World Report on Violence and Health: Summary; World Health Organization: Geneva, Switzerland, 2002. [Google Scholar]
- Rougemont-Bücking, A.; Grazioli, V.S.; Daeppen, J.B.; Gmel, G.; Studer, J. Family-related stress versus external stressors: Differential impacts on alcohol and illicit drug use in young men. Eur. Addict. Res. 2017, 23, 284–297. [Google Scholar] [CrossRef]
- Zuckerman, M. Sensation Seeking: Beyond the Optimal Level of Arousal; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 1979. [Google Scholar]
- Mushquash, C.J.; Stewart, S.H.; Mushquash, A.R.; Comeau, M.N.; McGrath, P.J. Personality traits and drinking motives predict alcohol misuse among Canadian aboriginal youth. Int. J. Ment. Health Addict. 2014, 12, 270–282. [Google Scholar] [CrossRef]
- Conrod, P.J.; Pihl, R.O.; Stewart, S.H.; Dongier, M. Validation of a system of classifying female substance abusers on the basis of personality and motivational risk factors for substance abuse. Psychol. Addict. Behav. 2000, 14, 243. [Google Scholar] [CrossRef]
- Cooper, M.L.; Russell, M.; Skinner, J.B.; Frone, M.R.; Mudar, P. Stress and alcohol use: Moderating effects of gender, coping, and alcohol expectancies. J. Abnorm. Psychol. 1992, 101, 139. [Google Scholar] [CrossRef]
- Moos, R.H.; Brennan, P.L.; Schutte, K.K.; Moos, B.S. Older adults’ coping with negative life events: Common processes of managing health, interpersonal, and financial/work stressors. Int. J. Aging Hum. Dev. 2006, 62, 39–59. [Google Scholar] [CrossRef]
- Nadkarni, A.; Dabholkar, H.; McCambridge, J.; Bhat, B.; Kumar, S.; Mohanraj, R.; Murthy, P.; Patel, V. The explanatory models and coping strategies for alcohol use disorders: An exploratory qualitative study from India. Asian J. Psychiatry 2013, 6, 521–527. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bradshaw, S.D.; Shumway, S.T.; Dsauza, C.M.; Morris, N.; Hayes, N.D. Hope, coping skills, and the prefrontal cortex in alcohol use disorder recovery. Am. J. Drug Alcohol Abus. 2017, 43, 591–601. [Google Scholar] [CrossRef] [PubMed]
- Studer, J.; Baggio, S.; Mohler-Kuo, M.; Dermota, P.; Gaume, J.; Bertholet, N.; Daeppen, J.-B.; Gmel, G. Examining non-response bias in substance use research—Are late respondents proxies for non-respondents? Drug Alcohol Depend. 2013, 132, 316–323. [Google Scholar] [CrossRef] [Green Version]
- Studer, J.; Mohler-Kuo, M.; Dermota, P.; Gaume, J.; Bertholet, N.; Eidenbenz, C.; Daeppen, J.-B.; Gmel, G. Need for informed consent in substance use studies—Harm of bias? J. Stud. Alcohol Drugs 2013, 74, 931–940. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®); American Psychiatric Pub: Washington, DC, USA, 2013. [Google Scholar]
- Hasin, D.S.; O’Brien, C.P.; Auriacombe, M.; Borges, G.; Bucholz, K.; Budney, A.; Compton, W.M.; Crowley, T.; Ling, W.; Petry, N.M. DSM-5 criteria for substance use disorders: Recommendations and rationale. Am. J. Psychiatry 2013, 170, 834–851. [Google Scholar] [CrossRef] [Green Version]
- Carver, C.S. You want to measure coping but your protocol’ too long: Consider the brief cope. Int. J. Behav. Med. 1997, 4, 92–100. [Google Scholar] [CrossRef]
- Muller, L.; Spitz, E. Multidimensional assessment of coping: Validation of the brief COPE among French population. L’encéphale 2003, 29, 507–518. [Google Scholar]
- Knoll, N.; Rieckmann, N.; Schwarzer, R. Coping as a mediator between personality and stress outcomes: A longitudinal study with cataract surgery patients. Eur. J. Personality 2005, 19, 229–247. [Google Scholar] [CrossRef]
- Hoyle, R.H.; Stephenson, M.T.; Palmgreen, P.; Lorch, E.P.; Donohew, R.L. Reliability and validity of a brief measure of sensation seeking. Personal. Individ. Differ. 2002, 32, 401–414. [Google Scholar] [CrossRef]
- Fox, J. Effect displays in R for generalised linear models. J. Stat. Softw. 2003, 8, 1–27. [Google Scholar] [CrossRef] [Green Version]
- R Core Team. R: A Language and Environment for Statistical Computing; R Core Team: Vienna, Austria, 2013. [Google Scholar]
- Aldao, A.; Nolen-Hoeksema, S. When are adaptive strategies most predictive of psychopathology? J. Abnorm. Psychol. 2012, 121, 276. [Google Scholar] [CrossRef] [Green Version]
- Rosenthal, J.A. Qualitative descriptors of strength of association and effect size. J. Soc. Serv. Res. 1996, 21, 37–59. [Google Scholar] [CrossRef]
- Conrod, P.J. Personality-targeted interventions for substance use and misuse. Curr. Addict. Rep. 2016, 3, 426–436. [Google Scholar] [CrossRef] [Green Version]
- Kosterman, R.; Hill, K.G.; Lee, J.O.; Meacham, M.C.; Abbott, R.D.; Catalano, R.F.; Hawkins, J.D. Young adult social development as a mediator of alcohol use disorder symptoms from age 21 to 30. Psychol. Addict. Behav. 2014, 28, 348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnstone, B.M.; Leino, E.V.; Ager, C.R.; Ferrer, H.; Fillmore, K.M. Determinants of life-course variation in the frequency of alcohol consumption: Meta-analysis of studies from the collaborative alcohol-related longitudinal project. J. Stud. Alcohol 1996, 57, 494–506. [Google Scholar] [CrossRef] [PubMed]
- Tragesser, S.L.; Beauvais, F.; Swaim, R.C.; Edwards, R.W.; Oetting, E.R. Parental monitoring, peer drug involvement, and marijuana use across three ethnicities. J. Cross-Cult. Psychol. 2007, 38, 670–694. [Google Scholar] [CrossRef]
- Borsari, B.; Muellerleile, P. Collateral reports in the college setting: A meta-analytic integration. Alcohol. Clin. Exp. Res. 2009, 33, 826–838. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cooper, A.M.; Sobell, M.B.; Sobell, L.C.; Maisto, S.A. Validity of alcoholics’ self-reports: Duration data. Int. J. Addict. 1981, 16, 401–406. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| n (%)/ Mean ± SD (Range) | AUD a (Prevalence in %) | χ2 (df) d | p-Value | |
|---|---|---|---|---|
| Total | 4844 | 31.9 | ||
| Age a | 25.4 ± 1.2 (23–33) | |||
| Parental monitoring b | ||||
| Low | 1248 (25.8) | 38.3 | 31.3 (1) | <0.0001 |
| Median/High | 3596 (74.2) | 29.7 | ||
| Active coping c | ||||
| Median/Low | 2944 (60.8) | 32.5 | 1.3 (1) | 0.261 |
| High | 1900 (39.2) | 31.0 | ||
| Denial c | ||||
| Median/Low | 2924 (60.4) | 30.1 | 11.9 (1) | 0.0006 |
| High | 1920 (39.6) | 34.8 | ||
| Sensation seeking b | ||||
| Median/Low | 2607 (53.8) | 25.3 | 115.1 (1) | <0.0001 |
| High | 2237 (46.2) | 39.7 | ||
| AUD 5 years earlier b | ||||
| No | 3333 (68.8) | 21.3 | 552.8 (1) | <0.0001 |
| Yes | 1511 (31.2) | 55.3 | ||
| Level of financial autonomy a | ||||
| Financially autonomous | 2832 (58.5) | 28.2 | 45.0 (2) | <0.0001 |
| Partially financially dependent | 1476 (30.5) | 37.9 | ||
| Financially dependent | 536 (11.1) | 35.1 | ||
| Civil status a | ||||
| Single | 4046 (83.5) | 33.3 | 22.3 (1) | <0.0001 |
| Living with a partner/married | 798 (16.5) | 24.8 |
| AUD c | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Model 0 | Model 1 | Model 2 | Model 3 | |||||||||
| OR | 95% CI | p-Value | OR | 95% CI | p-Value | OR | 95% CI | p-Value | OR | 95% CI | p-Value | |
| Low parental monitoring a | 1.21 | 1.05–1.40 | 0.011 | 1.37 | 1.14–1.65 | 0.001 | 1.32 | 1.09–1.60 | 0.004 | 1.27 | 1.02–1.59 | 0.033 |
| High active coping b | 0.97 | 0.85–1.11 | 0.682 | 1.07 | 0.91–1.25 | 0.426 | 0.97 | 0.85–1.11 | 0.679 | 0.97 | 0.85–1.11 | 0.685 |
| Low parental monitoring a × High active coping b | 0.70 | 0.52–0.96 | 0.025 | |||||||||
| High denial b | 1.15 | 1.01–1.31 | 0.039 | 1.15 | 1.01–1.31 | 0.040 | 1.22 | 1.04–1.43 | 0.013 | 1.15 | 1.01–1.31 | 0.039 |
| Low parental monitoring a × High denial b | 0.81 | 0.61–1.09 | 0.167 | |||||||||
| High sensation seeking a | 1.56 | 1.37–1.78 | <0.0001 | 1.56 | 1.37–1.78 | <0.0001 | 1.56 | 1.37–1.78 | <0.0001 | 1.60 | 1.37–1.86 | <0.0001 |
| Low parental monitoring a × High sensation seeking a | 0.92 | 0.68–1.23 | 0.558 | |||||||||
| AUD 5 years earlier a | 4.13 | 3.61–4.72 | <0.0001 | 4.12 | 3.60–4.72 | <0.0001 | 4.12 | 3.60–4.72 | <0.0001 | 4.13 | 3.61–4.73 | <0.0001 |
| Partially financially dependent c,d | 1.54 | 1.33–1.77 | <0.0001 | 1.54 | 1.33–1.78 | <0.0001 | 1.54 | 1.33–1.78 | <0.0001 | 1.54 | 1.33–1.77 | <0.0001 |
| Financially dependent c,d | 1.41 | 1.14–1.74 | 0.002 | 1.40 | 1.13–1.73 | 0.002 | 1.41 | 1.14–1.74 | 0.001 | 1.41 | 1.14–1.74 | 0.002 |
| Living with a partner/married c,e | 0.75 | 0.62–0.90 | 0.003 | 0.75 | 0.62–0.90 | 0.002 | 0.75 | 0.62–0.90 | 0.003 | 0.75 | 0.62–0.90 | 0.003 |
| (Intercept) | 0.18 | 0.15–0.21 | <0.0001 | 0.17 | 0.15–0.20 | <0.0001 | 0.18 | 0.15–0.21 | <0.0001 | 0.18 | 0.15–0.21 | <0.0001 |
| AIC | 5440.71 | 5437.64 | 5440.80 | 5442.37 | ||||||||
| BIC | 5499.08 | 5502.49 | 5505.66 | 5507.23 | ||||||||
| Log likelihood | −2711.36 | −2708.82 | −2710.40 | −2711.19 | ||||||||
| Number of observations | 4844 | 4844 | 4844 | 4844 | ||||||||
| Parental Monitoring | ||||
|---|---|---|---|---|
| Low | Median/High | |||
| P | SE | P | SE | |
| Active coping | ||||
| Median/Low | 0.35 | 0.02 | 0.28 | 0.01 |
| High | 0.29 | 0.02 | 0.30 | 0.01 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sobrino-Piazza, J.; Foster, S.; Estévez-Lamorte, N.; Mohler-Kuo, M. Parental Monitoring, Individual Dispositions, and Alcohol Use Disorder: A Longitudinal Study with Young Swiss Men. Int. J. Environ. Res. Public Health 2021, 18, 9938. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18189938
Sobrino-Piazza J, Foster S, Estévez-Lamorte N, Mohler-Kuo M. Parental Monitoring, Individual Dispositions, and Alcohol Use Disorder: A Longitudinal Study with Young Swiss Men. International Journal of Environmental Research and Public Health. 2021; 18(18):9938. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18189938
Chicago/Turabian StyleSobrino-Piazza, Jimena, Simon Foster, Natalia Estévez-Lamorte, and Meichun Mohler-Kuo. 2021. "Parental Monitoring, Individual Dispositions, and Alcohol Use Disorder: A Longitudinal Study with Young Swiss Men" International Journal of Environmental Research and Public Health 18, no. 18: 9938. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18189938