
Relationship of Coping Strategies and Quality of Life: Parallel and Serial Mediating Role of Resilience and Social Participation among Older Adults in Western Philippines




Abstract
:1. Introduction
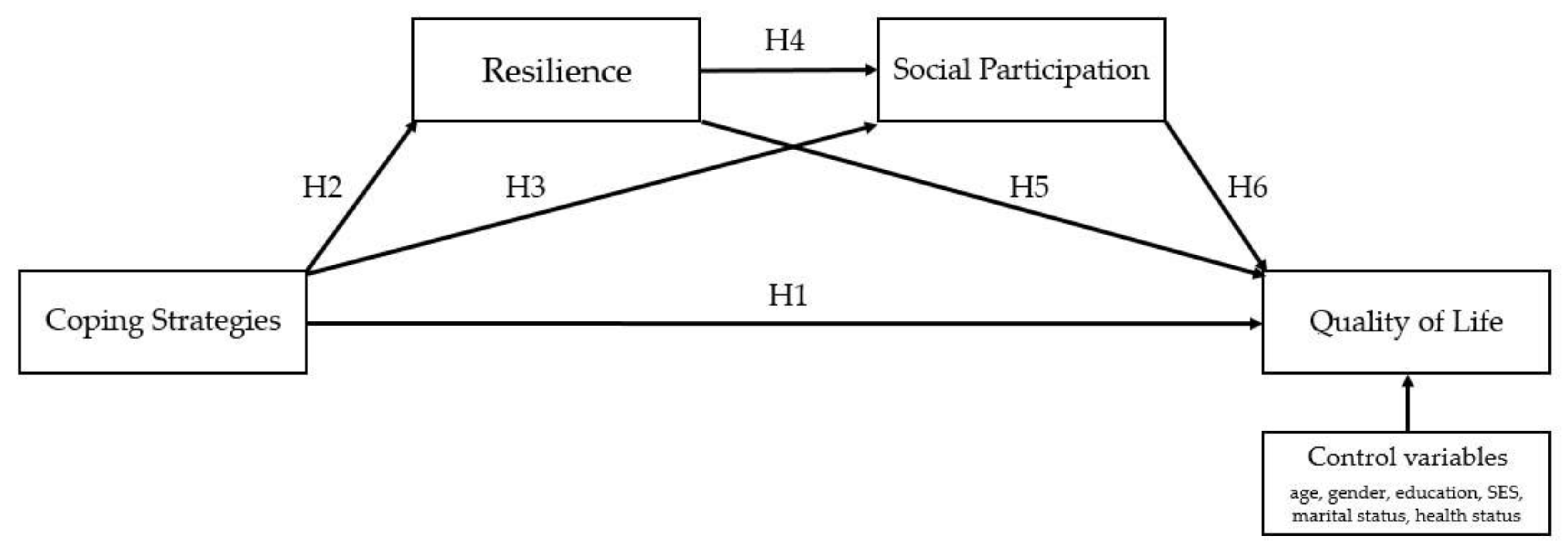
- Coping strategies are directly associated with QOL (H1).
- In terms of indirect effects through resilience, higher levels of coping strategies are associated with higher levels of resilience (H2), which in turn are associated with higher levels of QOL (H5).
- Similarly, indirect effects through social participation indicate that higher levels of coping strategies are associated with higher levels of social participation (H3), which in turn are associated with higher levels of QOL (H6).In terms of serial mediation, it has been hypothesized that coping strategies, resilience, social participation, and QOL affect each other sequentially. A more specific hypothesis is provided:
- High levels of coping strategies lead to high levels of resilience, which in turn lead to high levels of social participation, and ultimately lead to high levels of QOL (path analysis from H2, H4, to H6).
2. Method and Materials
2.1. Participants and Procedure
2.2. Research Tools
2.2.1. Coping Strategies
2.2.2. Resilience Scale
2.2.3. Social Participation
2.2.4. Quality of Life
2.3. Data Analysis
3. Results
4. Discussions
Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wang, S. Spatial patterns and social-economic influential factors of population aging: A global assessment from 1990 to 2010. Soc. Sci. Med. 2020, 253, 112963. [Google Scholar] [CrossRef] [PubMed]
- Philippine Statistics Authority. Facts on Senior Citizen; PSA: Quezon City, Philippines, 2015.
- Philippine Statistics Authority. Women and men in Western Visayas: 2019 Statistical Hanbook; PSA: Quezon City, Philippines, 2019.
- Roxas, J.N.R.; Fillone, A.M. Co-benefit analysis of the proposed Panay-Guimaras-Negros Bridge Project, Western Visayas, Philippines. Transp. Res. Procedia 2017, 25, 3564–3577. [Google Scholar] [CrossRef]
- Philippine Statistics Authority. Gross Domestic Product of the Philippines Highlights for 2018. Available online: https://psa.gov.ph/grdp/highlights-id/138509 (accessed on 30 July 2021).
- Ranola, A. Combating Elderly Poverty in the Philippines. Available online: https://borgenproject.org/elderly-poverty-in-the-philippines/ (accessed on 30 July 2021).
- Momblan, G.W. Visayas Senior Citizens Start Receiving Social Pensions. Available online: https://www.pna.gov.ph/articles/1101297 (accessed on 30 July 2021).
- Reyes, C.M.; Arboneda, A.A.; Asis, R.D. Silver Linings for the Elderly in the Philippines: Policies and Programs for Senior Citizens; Philippine Institute for Development Studies: Quezon City, Philippines, 2019.
- Badana, M.A.N.S.; Andel, R. Aging in the Philippines. Gerontologist 2018, 58, 212–218. [Google Scholar] [CrossRef] [Green Version]
- Carandang, R.R.; Asis, E.; Shibanuma, A.; Kiriya, J.; Murayama, H.; Jimba, M. Unmet Needs and Coping Mechanisms Among Community-Dwelling Senior Citizens in the Philippines: A Qualitative Study. Int. J. Environ. Res. Public Health 2019, 16, 3745. [Google Scholar] [CrossRef] [Green Version]
- Esteban, R.C. Thinking about Aging: Experience, Identity and Meaning among an Elderly Population in the Philippines. Adv. Aging Res. 2015, 04, 133–153. [Google Scholar] [CrossRef] [Green Version]
- Faner, M.R.; Chiong, M.A.D. Clinical Profiles and Outcomes of the Most Common Inherited Metabolic Diseases in the Philippines: A Review of the National Institutes of Health—Institute of Human Genetics Metabolic Registry. Acta Med. Philipp. 2020, 54. [Google Scholar] [CrossRef]
- Kerschner, H.; Pegues, J.A.M. Productive Aging: A Quality of Life Agenda. J. Am. Diet. Assoc. 1998, 98, 1445–1448. [Google Scholar] [CrossRef]
- World Health Organization. The Constitution of the World Health Organization; WHO: Geneva, Switzerland, 1947; Volume 1, pp. 29–43. [Google Scholar]
- Spitzer, W.O. State of science 1986: Quality of life and functional status as target variables for research. J. Chronic Dis. 1987, 40, 465–471. [Google Scholar] [CrossRef]
- Medvedev, O.N.; Landhuis, C.E. Exploring constructs of well-being, happiness and quality of life. PeerJ 2018, 6, e4903. [Google Scholar] [CrossRef] [PubMed]
- Aldwin, C.M.; Yancura, L.A.; Boeninger, D.K. Coping, health, and aging. In Handbook of Health Psychology and Aging; Aldwin, C.M., Park, C.L., Spiro, A., III, Eds.; The Guilford Press: New York, NY, USA, 2007; pp. 210–226. [Google Scholar]
- Borowiak, E.; Kostka, T. Predictors of quality of life in older people living at home and in institutions. Aging Clin. Exp. Res. 2004, 16, 212–220. [Google Scholar] [CrossRef] [PubMed]
- Harms, C.A.; Cohen, L.; Pooley, J.A.; Chambers, S.K.; A Galvao, D.; Newton, R.U. Quality of life and psychological distress in cancer survivors: The role of psycho-social resources for resilience. Psycho-Oncology 2018, 28, 271–277. [Google Scholar] [CrossRef] [Green Version]
- Mayordomo, T.; Viguer, P.; Sales, A.; Satorres, E.; Melendez, J.C. Resilience and Coping as Predictors of Well-Being in Adults. J. Psychol. 2016, 150, 809–821. [Google Scholar] [CrossRef]
- Galiana, L.; Gutiérrez, M.; Sancho, P.; Francisco, E.-H.; Tomas, J.M. Socio-Demographic Variables and Successful Aging of the Angolan Elderly. Scientifica 2016, 2016, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Wieder-Huszla, S.; Szkup, M.; Jurczak, A.; Samochowiec, A.; Samochowiec, J.; Stanisławska, M.; Rotter, I.; Karakiewicz, B.; Grochans, E. Effects of Socio-Demographic, Personality and Medical Factors on Quality of Life of Postmenopausal Women. Int. J. Environ. Res. Public Health 2014, 11, 6692–6708. [Google Scholar] [CrossRef] [Green Version]
- Hajian-Tilaki, K.; Heidari, B.; Hajian-Tilaki, A. Are Gender Differences in Health-related Quality of Life Attributable to Sociodemographic Characteristics and Chronic Disease Conditions in Elderly People? Int. J. Prev. Med. 2017, 8. [Google Scholar] [CrossRef]
- Galiana, L.; Tomás, J.M.; Fernández, I.; Oliver, A. Predicting Well-Being Among the Elderly: The Role of Coping Strategies. Front. Psychol. 2020, 11, 616. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hunt, S.; Wisocki, P.; Yanko, J. Worry and use of coping strategies among older and younger adults. J. Anxiety Disord. 2002, 17, 547–560. [Google Scholar] [CrossRef]
- Peláez-Ballestas, I.; Boonen, A.; Vázquez-Mellado, J.; Reyes-Lagunes, I.; Hernández-Garduño, A.; Goycochea, M.V.; Bernard-Medina, A.G.; Rodríguez-Amado, J.; Casasola-Vargas, J.; Garza-Elizondo, M.A.; et al. Coping Strategies for Health and Daily-Life Stressors in Patients With Rheumatoid Arthritis, Ankylosing Spondylitis, and Gout. Medicine 2015, 94, e600. [Google Scholar] [CrossRef] [PubMed]
- Greenglass, E.R. Proactive coping and quality of life management. In Beyond Coping: Meeting Goals, Visions, and Challenges; Frydenberg, E., Ed.; Oxford University Press: Oxford, UK, 2002; pp. 37–62. [Google Scholar]
- Chabowski, M.; Jankowska-Polanska, B.; Lomper, K.; Janczak, D. The effect of coping strategy on quality of life in patients with NSCLC. Cancer Manag. Res. 2018, 10, 4085–4093. [Google Scholar] [CrossRef] [Green Version]
- Demers, L.; Robichaud, L.; Noreau, L.; Gélinas, I.; Desrosiers, J. Coping Strategies and Social Participation in Older Adults. Gerontology 2008, 55, 233–239. [Google Scholar] [CrossRef]
- Atal, S.; Cheng, C. Socioeconomic health disparities revisited: Coping flexibility enhances health-related quality of life for individuals low in socioeconomic status. Health Qual. Life Outcomes 2016, 14, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Gattino, S.; Rollero, C.; De Piccoli, N. The Influence of Coping Strategies on Quality of Life from a Gender Perspective. Appl. Res. Qual. Life 2014, 10, 689–701. [Google Scholar] [CrossRef]
- Kupcewicz, E.; Grochans, E.; Kadučáková, H.; Mikla, M.; Jóźwik, M. Analysis of the Relationship between Stress Intensity and Coping Strategy and the Quality of Life of Nursing Students in Poland, Spain and Slovakia. Int. J. Environ. Res. Public Health 2020, 17, 4536. [Google Scholar] [CrossRef] [PubMed]
- Dockendorff, D.C.T. Healthy Ways of Coping With Losses Related to the Aging Process. Educ. Gerontol. 2013, 40, 363–384. [Google Scholar] [CrossRef]
- Philippine Statistics Authority. Special Release: Poverty Statistics Among Families in Western Visayas; PSA: Quezon City, Philippines, 2020.
- Southwick, S.M.; Bonanno, G.A.; Masten, A.; Panter-Brick, C.; Yehuda, R. Resilience definitions, theory, and challenges: Interdisciplinary perspectives. Eur. J. Psychotraumatol. 2014, 5, 25338. [Google Scholar] [CrossRef] [Green Version]
- Kais, S.M.; Islam, S. Community Capitals as Community Resilience to Climate Change: Conceptual Connections. Int. J. Environ. Res. Public Health 2016, 13, 1211. [Google Scholar] [CrossRef] [Green Version]
- Windle, G. What is resilience? A review and concept analysis. Rev. Clin. Gerontol. 2010, 21, 152–169. [Google Scholar] [CrossRef]
- Lawford, J.; Eiser, C. Exploring links between the concepts of Quality of Life and resilience. Pediatr. Rehabil. 2001, 4, 209–216. [Google Scholar] [CrossRef] [PubMed]
- Lu, C.; Yuan, L.; Lin, W.; Zhou, Y.; Pan, S. Depression and resilience mediates the effect of family function on quality of life of the elderly. Arch. Gerontol. Geriatr. 2017, 71, 34–42. [Google Scholar] [CrossRef] [PubMed]
- Guccione, A.A. Resilience and Self-efficacy As Mediators of Quality of Life in Geriatric Rehabilitation. Top. Geriatr. Rehabil. 2014, 30, 164–169. [Google Scholar] [CrossRef]
- Gerino, E.; Rollè, L.; Sechi, C.; Brustia, P. Loneliness, Resilience, Mental Health, and Quality of Life in Old Age: A Structural Equation Model. Front. Psychol. 2017, 8, 2003. [Google Scholar] [CrossRef] [PubMed]
- Carandang, R.; Shibanuma, A.; Asis, E.; Chavez, D.; Tuliao, M.; Jimba, M. “Are Filipinos Aging Well?”: Determinants of Subjective Well-Being among Senior Citizens of the Community-Based ENGAGE Study. Int. J. Environ. Res. Public Health 2020, 17, 7636. [Google Scholar] [CrossRef] [PubMed]
- Chung, M.S. Resilience, Coping Methods, and Quality of Life in Middle-aged Women. J. Korean Acad. Psychiatr. Ment. Health Nurs. 2011, 20, 345–354. [Google Scholar] [CrossRef] [Green Version]
- Yashin, A.I.; Arbeev, K.G.; Kulminski, A.; Akushevich, I.; Akushevich, L.; Ukraintseva, S.V. Health decline, aging and mortality: How are they related? Biogerontology 2007, 8, 291–302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacLeod, S.; Musich, S.; Hawkins, K.; Alsgaard, K.; Wicker, E.R. The impact of resilience among older adults. Geriatr. Nurs. 2016, 37, 266–272. [Google Scholar] [CrossRef] [Green Version]
- Aroogh, M.D.; Shahboulaghi, F.M. Social participation of older adults: A concept analysis. Int. J. Community Based Nurs. Midwifery 2020, 8, 55–72. [Google Scholar] [CrossRef]
- McKibbin, C.; Lee, A.; Steinman, B.A.; Carrico, C.; Bourassa, K.; Slosser, A. Health Status and Social Networks as Predictors of Resilience in Older Adults Residing in Rural and Remote Environments. J. Aging Res. 2016, 2016, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Choi, J.; Cho, Y.; Kim, Y.; Lee, S.; Lee, J.; Yi, Y.; Tak, Y.; Hwang, H.; Lee, S.; Park, E.; et al. The Relationship of Sitting Time and Physical Activity on the Quality of Life in Elderly People. Int. J. Environ. Res. Public Health 2021, 18, 1459. [Google Scholar] [CrossRef]
- Cohen, L.; Manion, L.; Morrison, K. Research Method in Education, 6th ed.; Routledge: Abingdon, UK, 2007. [Google Scholar]
- Glaziou, P. Sampsize. Available online: http://sampsize.sourceforge.net/iface/ (accessed on 14 September 2021).
- Son, J. Back translation as a documentation tool. Int. J. Transl. Interpreting Res. 2018, 10, 89–100. [Google Scholar] [CrossRef] [Green Version]
- Robichaud, L.; Lamarre, C. Developing an Instrument for Identifying Coping Strategies Used by the Elderly to Remain Autonomous. Am. J. Phys. Med. Rehabil. 2002, 81, 736–744. [Google Scholar] [CrossRef]
- Cronbach, L.J. Coefficient alpha and the internal structure of tests. Psychometrika 1951, 16, 297–334. [Google Scholar] [CrossRef] [Green Version]
- Nunnally, J.C., Jr. Introduction to Psychological Measurement; McGraw-Hill: New York, NY, USA, 1970. [Google Scholar]
- Likert, R. A Technique for the Measurement of Attitudes; Columbia University Press: New York, NY, USA, 1932. [Google Scholar]
- Wagnild, G.M. The Resilience Scale User’s Guide for the US English Version of the Resilience Scale and the 14-Item Resilience Scale (RS-14); The Resilience Center: Worden, MT, USA, 2011. [Google Scholar]
- Wagnild, G. A Review of the Resilience Scale. J. Nurs. Meas. 2009, 17, 105–113. [Google Scholar] [CrossRef] [PubMed]
- Wagnild, G.M.; Collins, J.A. Assessing Resilience. J. Psychosoc. Nurs. Ment. Health Serv. 2009, 47, 28–33. [Google Scholar] [CrossRef] [PubMed]
- Wagnild, G.M.; Young, H.M. Development and psychometric evaluation of the Resilience Scale. J. Nurs. Meas. 1993, 1, 165–178. [Google Scholar] [PubMed]
- Kubach, O. Examining Social Participation of Older Adults to Help Create an Age Friendly Community. Master’s Thesis, The University of Western Ontario, London, ON, USA, 2014. [Google Scholar]
- Bowling, A. The psychometric properties of the older people’s quality of life questionnaire, compared with the CASP-19 and the WHOQOL-OLD. Curr. Gerontol. Geriatr. Res. 2009, 2009, 298950. [Google Scholar] [CrossRef] [Green Version]
- Hayes, A.F. Beyond Baron and Kenny: Statistical Mediation Analysis in the New Millennium. Commun. Monogr. 2009, 76, 408–420. [Google Scholar] [CrossRef]
- Hu, L.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. A Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Byrne, B.M. Structural Equation Modeling with AMOS. Basic Concepts, Applications, and Programming, 2nd ed.; Taylor & Francis: New York, NY, USA, 2010. [Google Scholar]
- Spector, P.E.; Brannick, M.T. Methodological Urban Legends: The Misuse of Statistical Control Variables. Organ. Res. Methods 2010, 14, 287–305. [Google Scholar] [CrossRef]
- Frölich, M. Parametric and Nonparametric Regression in the Presence of Endogenous Control Variables. Int. Stat. Rev. 2008, 76, 214–227. [Google Scholar] [CrossRef]
- Hildon, M.Z.; Montgomery, S.; Blane, M.D.; Wiggins, R.D.; Netuveli, G. Examining Resilience of Quality of Life in the Face of Health-Related and Psychosocial Adversity at Older Ages: What is “Right” About the Way We Age? Gerontologist 2009, 50, 36–47. [Google Scholar] [CrossRef]
- Takagi, D.; Kondo, K.; Kawachi, I. Social participation and mental health: Moderating effects of gender, social role and rurality. BMC Public Health 2013, 13, 701. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tobin, M.C.; Drager, K.D.; Richardson, L.F. A systematic review of social participation for adults with autism spectrum disorders: Support, social functioning, and quality of life. Res. Autism Spectr. Disord. 2014, 8, 214–229. [Google Scholar] [CrossRef]
- Masten, A.S.; Barnes, A.J. Resilience in Children: Developmental Perspectives. Children 2018, 5, 98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reivich, K.; Shatté, A. The Resilience Factor: 7 Essential Skills for Overcoming Life’s Inevitable Obstacles; Broadway Books: Portland, OR, USA, 2002. [Google Scholar]
- Yates, T.; Tyrell, F.; Masten, A. Resilience Theory and the Practice of Positive Psychology From Individuals to Societies. Posit. Psychol. Pract. Promot. Hum. Flourishing Work. Health Educ. Everyday Life 2015, 773–788. [Google Scholar] [CrossRef]
- León-Navarrete, M.M.; Flores-Villavicencio, M.E.; Mendoza-Ruvalcaba, N.; Colunga-Rodríguez, C.; Salazar-Garza, M.L.; Sarabia-López, L.E.; Albán-Pérez, G.G. Coping Strategies and Quality of Life in Elderly Population. Open J. Soc. Sci. 2017, 5, 207–216. [Google Scholar] [CrossRef] [Green Version]
- Katz, S. Busy Bodies: Activity, aging, and the management of everyday life. J. Aging Stud. 2000, 14, 135–152. [Google Scholar] [CrossRef]
- Douglas, H.; Georgiou, A.; Westbrook, J. Social participation as an indicator of successful aging: An overview of concepts and their associations with health. Aust. Health Rev. 2017, 41, 455–462. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Category | Groups | n | % |
|---|---|---|---|
| Educational Attainment | Elementary | 93 | 25 |
| High School | 114 | 29 | |
| College | 159 | 41 | |
| Graduate | 26 | 7 | |
| Marital Status | Single | 45 | 12 |
| Married | 199 | 51 | |
| Widow | 136 | 35 | |
| Separated | 12 | 3 | |
| Average Monthly Income 1 | Low (below 5000) | 92 | 24 |
| Middle (5000 to 15,000) | 187 | 48 | |
| High (above 15,000) | 113 | 29 | |
| Health Status | 0 Chronic Disease | 120 | 31 |
| 1 Chronic Disease | 167 | 43 | |
| 2 Chronic Diseases | 44 | 11 | |
| 3 Chronic Diseases | 43 | 11 | |
| 4 Chronic Diseases | 18 | 5 |
| Variables | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
|---|---|---|---|---|---|---|---|
| 1. Quality of life | 1 | ||||||
| 2. Coping strategies | 0.18 ** | 1 | |||||
| 3. Resilience | 0.31 ** | 0.25 ** | 1 | ||||
| 4. Social participation | 0.45 ** | 0.17 ** | 0.28 ** | 1 | |||
| 5. Age | ns | 0.01 * | −0.10 * | ns | 1 | ||
| 6. SES | ns | ns | ns | ns | ns | 1 | |
| 7. Health status | ns | ns | ns | ns | ns | ns | 1 |
| Minimum value | 71 | 26 | 57 | 15 | 60 | 3000 | 0 |
| Maximum value | 137 | 92 | 98 | 48 | 96 | 500,000 | 4 |
| Mean | 112.51 | 60.33 | 82.55 | 35.68 | 69.27 | 16,307.33 | 1.16 |
| SD | 9.03 | 9.56 | 11.77 | 6.52 | 6.50 | 34,371.66 | 1.12 |
| Alpha reliability | 0.70 | 0.82 | 0.91 | 0.89 |
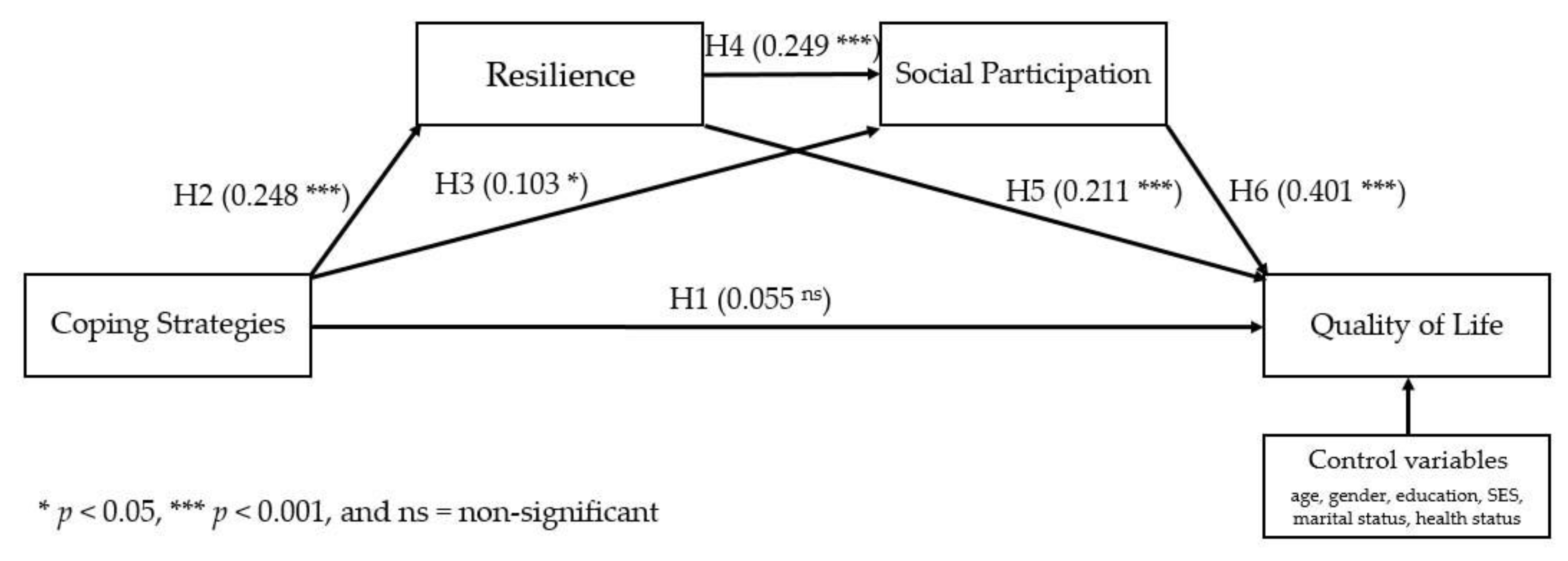
| Direct Effects | B | SE | β | 95% CI | p |
|---|---|---|---|---|---|
| A or H1: Coping strategies → Quality of life | 0.053 | 0.043 | 0.055 | [−0.02, 0.13] | 0.219 |
| H2: Coping strategies → Resilience | 0.305 | 0.060 | 0.248 | [0.16, 0.34] | <0.001 |
| H3: Coping strategies → Social participation | 0.071 | 0.034 | 0.103 | [0.02, 0.19] | 0.038 |
| H5: Resilience → Quality of life | 0.164 | 0.035 | 0.211 | [0.13, 0.29] | <0.001 |
| H4: Resilience → Social participation | 0.138 | 0.028 | 0.249 | [0.16, 0.33] | <0.001 |
| H6: Social participation → Quality of life | 0.564 | 0.063 | 0.401 | [0.32, 0.48] | <0.001 |
| Indirect Effects | B | SE | β | 95% CI | p |
|---|---|---|---|---|---|
| Parallel mediation | |||||
| Coping strategies → Resilience → Social participation 1 | 0.042 | 0.013 | 0.062 | [0.02, 0.07] | 0.001 |
| B: Coping strategies → Resilience → Quality of life 2 | 0.050 | 0.028 | 0.052 | [0.03, 0.08] | <0.001 |
| C: Coping strategies → Social participation → Quality of life 2 | 0.040 | 0.019 | 0.041 | [0.01, 0.08] | 0.046 |
| Resilience → Social participation → Quality of life 1 | 0.078 | 0.055 | 0.100 | [0.05, 0.11] | 0.001 |
| Serial mediation | |||||
| D: Coping strategies → Resilience → Social participation → Quality of life | 0.024 | 0.023 | 0.062 | [0.01, 0.04] | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Palmes, M.S.; Trajera, S.M.; Ching, G.S. Relationship of Coping Strategies and Quality of Life: Parallel and Serial Mediating Role of Resilience and Social Participation among Older Adults in Western Philippines. Int. J. Environ. Res. Public Health 2021, 18, 10006. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph181910006
Palmes MS, Trajera SM, Ching GS. Relationship of Coping Strategies and Quality of Life: Parallel and Serial Mediating Role of Resilience and Social Participation among Older Adults in Western Philippines. International Journal of Environmental Research and Public Health. 2021; 18(19):10006. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph181910006
Chicago/Turabian StylePalmes, Madonna S., Sheilla M. Trajera, and Gregory S. Ching. 2021. "Relationship of Coping Strategies and Quality of Life: Parallel and Serial Mediating Role of Resilience and Social Participation among Older Adults in Western Philippines" International Journal of Environmental Research and Public Health 18, no. 19: 10006. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph181910006