
Tele-Rehabilitation Program in Idiopathic Pulmonary Fibrosis—A Single-Center Randomized Trial

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Participants
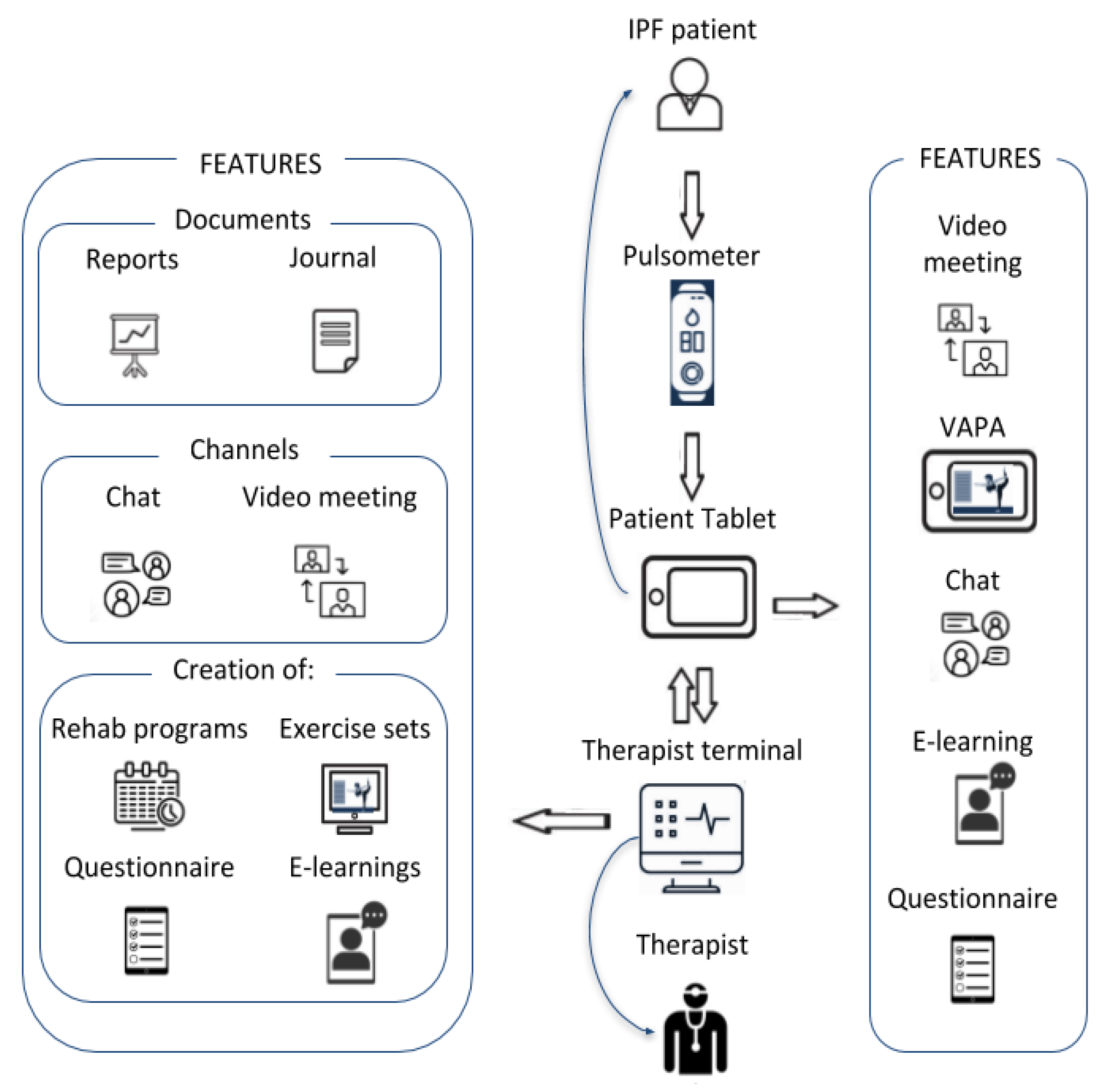
2.3. Tele-Rehabilitation
2.4. Endpoints
2.5. Statistics
3. Results
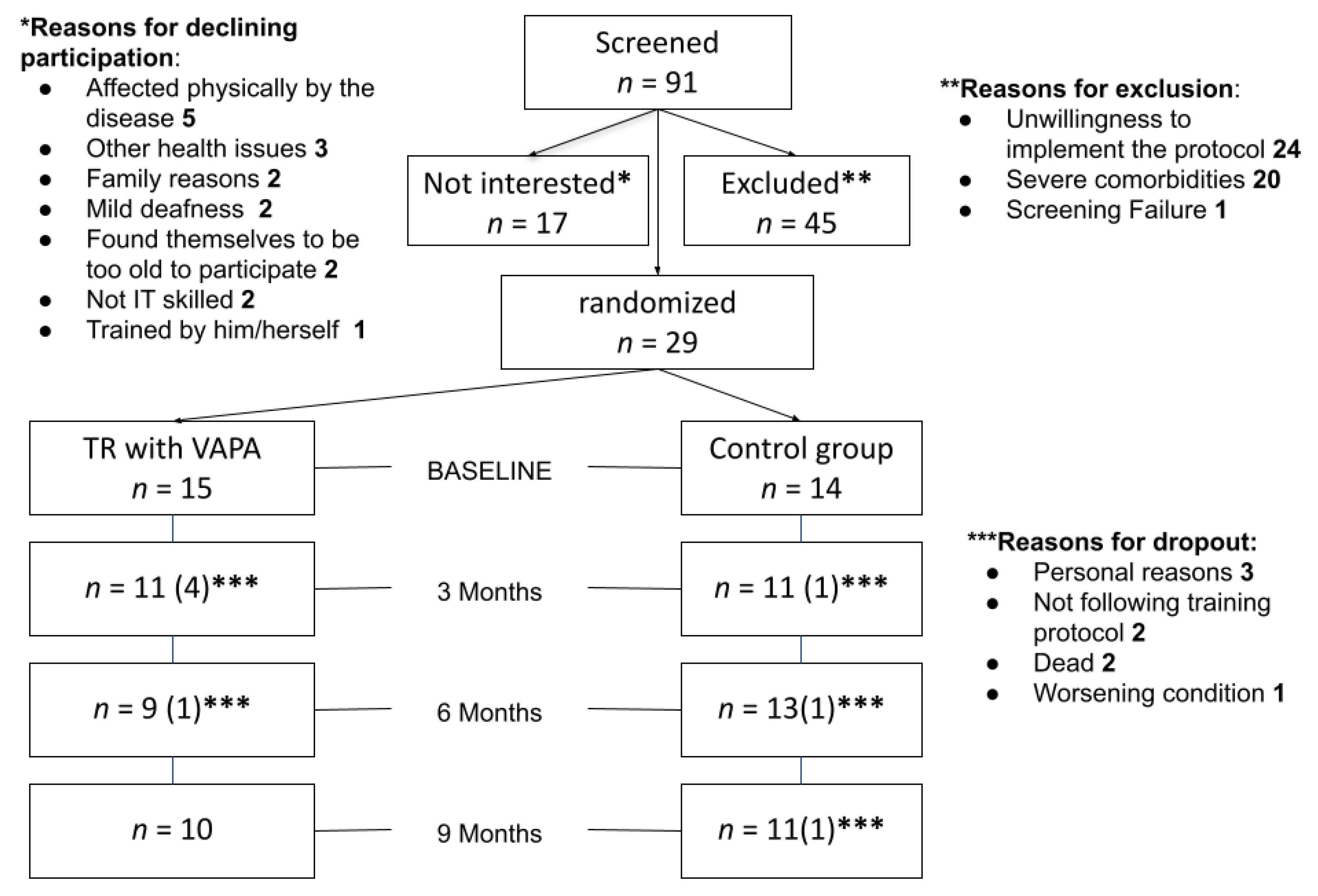
3.1. Patients
3.2. Endpoints
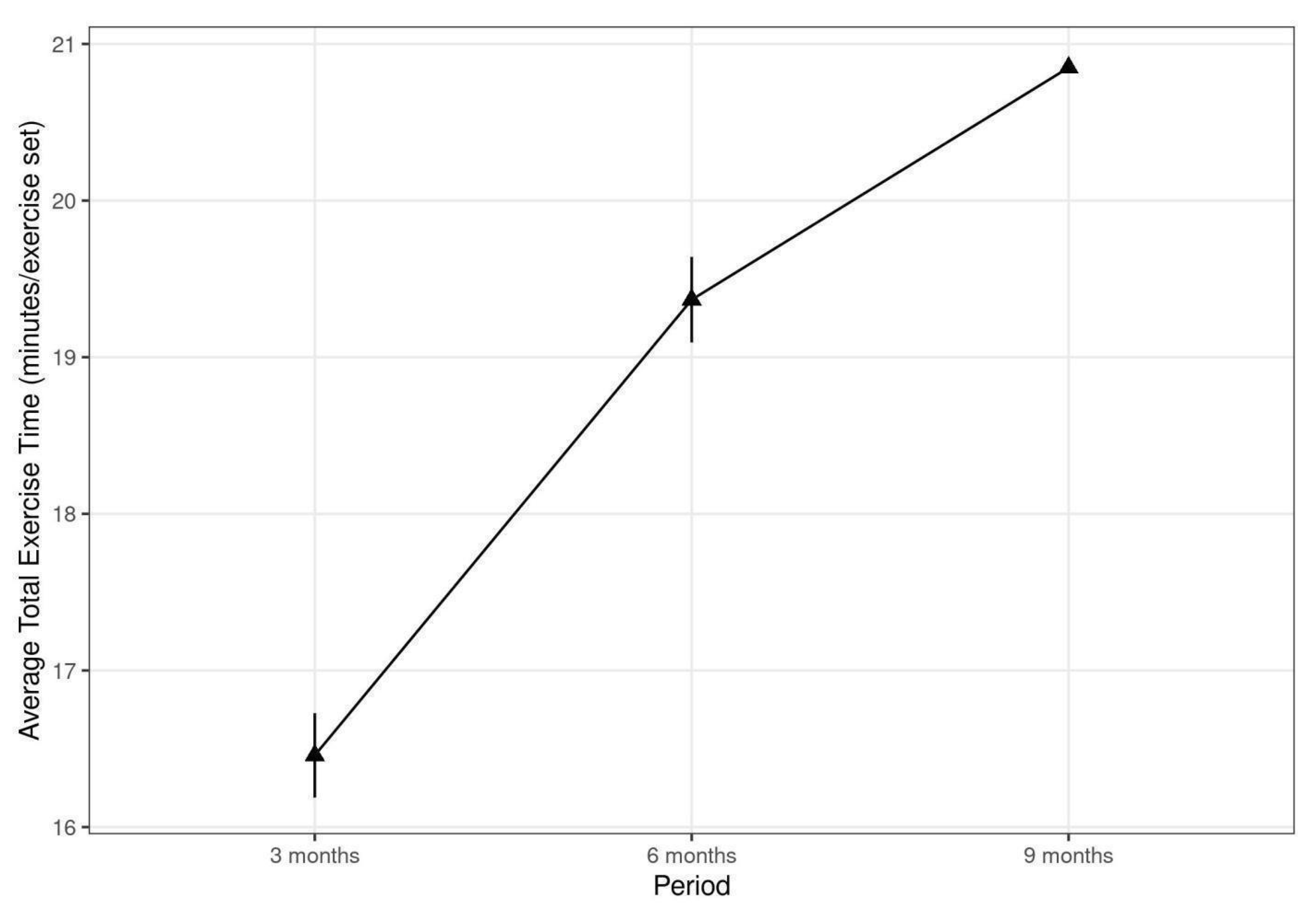
3.3. Training after End of Rele-Rehabilitation
3.4. Adherence and Patient Satisfaction
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Raghu, G.; Richeldi, L. Current Approaches to the Management of Idiopathic Pulmonary Fibrosis. Respir. Med. 2017, 129, 24–30. [Google Scholar] [CrossRef] [PubMed]
- Maher, T.M.; Bendstrup, E.; Dron, L.; Langley, J.; Smith, G.; Khalid, J.M.; Patel, H.; Kreuter, M. Global Incidence and Prevalence of Idiopathic Pulmonary Fibrosis. Respir. Res. 2021, 22, 197. [Google Scholar] [CrossRef] [PubMed]
- Dowman, L.M.; McDonald, C.F.; Hill, C.J.; Lee, A.L.; Barker, K.; Boote, C.; Glaspole, I.; Goh, N.S.L.; Southcott, A.M.; Burge, A.T.; et al. The Evidence of Benefits of Exercise Training in Interstitial Lung Disease: A Randomised Controlled Trial. Thorax 2017, 72, 610–619. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Manen, M.J.G.; Geelhoed, J.J.M.; Tak, N.C.; Wijsenbeek, M.S. Optimizing Quality of Life in Patients with Idiopathic Pulmonary Fibrosis. Ther. Adv. Respir. Dis. 2017, 11, 157–169. [Google Scholar] [CrossRef] [PubMed]
- Dowman, L.; Hill, C.J.; May, A.; Holland, A.E. Pulmonary Rehabilitation for Interstitial Lung Disease. Cochrane Database Syst. Rev. 2021. [Google Scholar] [CrossRef] [PubMed]
- Huppmann, P.; Sczepanski, B.; Boensch, M.; Winterkamp, S.; Schönheit-Kenn, U.; Neurohr, C.; Behr, J.; Kenn, K. Effects of Inpatient Pulmonary Rehabilitation in Patients with Interstitial Lung Disease. Eur. Respir. J. 2013, 42, 444–453. [Google Scholar] [CrossRef] [Green Version]
- Rogante, M.; Kairy, D.; Giacomozzi, C.; Grigioni, M. A Quality Assessment of Systematic Reviews on Telerehabilitation: What Does the Evidence Tell Us? Ann. Ist. Super. Sanita 2015, 51, 11–18. [Google Scholar] [PubMed]
- Telehealth for Physical Therapy. Available online: https://www.physitrack.com/telehealth (accessed on 7 April 2021).
- Telehealth: Secure and HIPAA-Compliant—SimplePractice. Available online: https://www.simplepractice.com/telehealth/ (accessed on 7 April 2021).
- Optimov Website. Available online: https://optimov.com/ (accessed on 7 April 2021).
- Welfare Denmark ApS—Welfare Denmark ApS. Available online: http://www.idisplay.dk/ (accessed on 7 April 2021).
- EvolvRehab Body. Available online: https://evolvrehab.com/virtualrehab/virtualrehab_body/ (accessed on 7 April 2021).
- Raghu, G.; Remy-Jardin, M.; Myers, J.L.; Richeldi, L.; Ryerson, C.J.; Lederer, D.J.; Behr, J.; Cottin, V.; Danoff, S.K.; Morell, F.; et al. Diagnosis of Idiopathic Pulmonary Fibrosis. An Official ATS/ERS/JRS/ALAT Clinical Practice Guideline. Am. J. Respir. Crit. Care Med. 2018, 198, e44–e68. [Google Scholar] [CrossRef]
- Virtual Autonomous Physiotherapy Agent—ERA-LEARN. Available online: https://www.era-learn.eu/network-information/networks/eurostars-2/eurostars-cut-off-17-09.2015/virtual-autonomous-physiotherapy-agent (accessed on 7 April 2021).
- Cerdán de Las Heras, J.; Tulppo, M.; Kiviniemi, A.M.; Hilberg, O.; Løkke, A.; Ekholm, S.; Catalán-Matamoros, D.; Bendstrup, E. Augmented Reality Glasses as a New Tele-Rehabilitation Tool for Home Use: Patients’ Perception and Expectations. Disabil. Rehabil. Assist. Technol. 2020, 4, 1–7. [Google Scholar] [CrossRef]
- Cerdan, J.; Catalan-Matamoros, D.; Berg, S.W. Online Communication in a Rehabilitation Setting: Experiences of Patients with Chronic Conditions Using a Web Portal in Denmark. Patient Educ. Couns. 2017, 100, 2283–2289. [Google Scholar] [CrossRef]
- Solution. Available online: https://optimov.com/?page_id=3006 (accessed on 20 September 2020).
- Products—Optimov. Available online: https://optimov.com/?page_id=1879 (accessed on 20 September 2020).
- Medicin.dk—Information Om Medicin. Available online: http://medicin.dk/ (accessed on 21 August 2020).
- Lungeforeningen. Available online: https://www.lunge.dk/ (accessed on 21 August 2020).
- Helbredsprofilen.dk. Available online: https://helbredsprofilen.dk/da (accessed on 21 August 2020).
- Spis Rigtigt—Antiinflammatorisk Kost—YouTube. Available online: https://youtube.com/embed/w5fjXI6NHec (accessed on 26 August 2020).
- Spis Rigtigt—Frugt Og Grønt—YouTube. Available online: https://youtube.com/embed/5O479Caonrc (accessed on 26 August 2020).
- Råd Til Undervægtige—YouTube. Available online: https://youtube.com/embed/t1Haq6Gf5hA (accessed on 26 August 2020).
- Råd Til Overvægtige—YouTube. Available online: https://youtube.com/embed/UKdjxpVjqFA (accessed on 26 August 2020).
- Holland, A.E.; Spruit, M.A.; Troosters, T.; Puhan, M.A.; Pepin, V.; Saey, D.; McCormack, M.C.; Carlin, B.W.; Sciurba, F.C.; Pitta, F.; et al. An Official European Respiratory Society/American Thoracic Society Technical Standard: Field Walking Tests in Chronic Respiratory Disease. Eur. Respir. J. 2014, 44, 1428–1446. [Google Scholar] [CrossRef]
- Hecht, A.; Ma, S.; Porszasz, J.; Casaburi, R. Methodology for Using Long-Term Accelerometry Monitoring to Describe Daily Activity Patterns in COPD the COPD Clinical Research Network. COPD 2009, 2, 121–129. [Google Scholar] [CrossRef] [Green Version]
- Prior, T.S.; Hoyer, N.; Shaker, S.B.; Davidsen, J.R.; Yorke, J.; Hilberg, O.; Bendstrup, E. Validation of the IPF-Specific Version of St. George’s Respiratory Questionnaire. Respir. Res. 2019, 20, 199. [Google Scholar] [CrossRef] [Green Version]
- Prior, T.S.; Hilberg, O.; Shaker, S.B.; Davidsen, J.R.; Hoyer, N.; Birring, S.S.; Bendstrup, E. Validation of the King’s Brief Interstitial Lung Disease Questionnaire in Idiopathic Pulmonary Fibrosis. BMC Pulm. Med. 2019, 19, 255. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.W.; Löwe, B. A Brief Measure for Assessing Generalized Anxiety Disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [Green Version]
- McCoy, C.E. Understanding the Intention-to-Treat Principle in Randomized Controlled Trials. West. J. Emerg. Med. 2017, 18, 1075–1078. [Google Scholar] [CrossRef]
- Vainshelboim, B.; Oliveira, J.; Fox, B.D.; Soreck, Y.; Fruchter, O.; Kramer, M.R. Long-Term Effects of a 12-Week Exercise Training Program on Clinical Outcomes in Idiopathic Pulmonary Fibrosis. Lung 2015, 193, 345–354. [Google Scholar] [CrossRef] [PubMed]
- du Bois, R.M.; Weycker, D.; Albera, C.; Bradford, W.Z.; Costabel, U.; Kartashov, A.; Lancaster, L.; Noble, P.W.; Sahn, S.A.; Szwarcberg, J.; et al. Six-Minute-Walk Test in Idiopathic Pulmonary Fibrosis: Test Validation and Minimal Clinically Important Difference. Am. J. Respir. Crit. Care Med. 2011, 183, 1231–1237. [Google Scholar] [CrossRef] [PubMed]
- du Bois, R.M.; Albera, C.; Bradford, W.Z.; Costabel, U.; Leff, J.A.; Noble, P.W.; Sahn, S.A.; Valeyre, D.; Weycker, D.; King, T.E., Jr. 6-Minute Walk Distance Is an Independent Predictor of Mortality in Patients with Idiopathic Pulmonary Fibrosis. Eur. Respir. J. 2014, 43, 1421–1429. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yuen, H.K.; Lowman, J.D.; Oster, R.A.; de Andrade, J.A. Home-Based Pulmonary Rehabilitation for Patients With Idiopathic Pulmonary Fibrosis: A PILOT STUDY. J. Cardiopulm. Rehabil. Prev. 2019, 39, 281–284. [Google Scholar] [CrossRef]
- Yu, X.; Li, X.; Wang, L.; Liu, R.; Xie, Y.; Li, S.; Li, J. Pulmonary Rehabilitation for Exercise Tolerance and Quality of Life in IPF Patients: A Systematic Review and Meta-Analysis. Biomed Res. Int. 2019, 2019, 8498603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hansen, H.; Bieler, T.; Beyer, N.; Godtfredsen, N.; Kallemose, T.; Frølich, A. COPD Online-Rehabilitation versus Conventional COPD Rehabilitation—Rationale and Design for a Multicenter Randomized Controlled Trial Study Protocol (CORe Trial). BMC Pulm. Med. 2017, 17, 140. [Google Scholar] [CrossRef] [PubMed]
- Hansen, H.; Bieler, T.; Beyer, N.; Kallemose, T.; Wilcke, J.T.; Østergaard, L.M.; Frost Andeassen, H.; Martinez, G.; Lavesen, M.; Frølich, A.; et al. Supervised Pulmonary Tele-Rehabilitation versus Pulmonary Rehabilitation in Severe COPD: A Randomised Multicentre Trial. Thorax 2020, 75, 413–421. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rayce, K.; Rosenbek Minet, L.; Kidholm, K.; Vestbo, J.; Pedersen, C.D.; Huniche, L. Telemediated Training in the Home as a Part of the Everyday Life and Practice With Very Severe Chronic Obstructive Pulmonary Disease. Qual. Health Res. 2020, 30, 2132–2145. [Google Scholar] [CrossRef]
- Telemedieret Hjemmetræning Til Patienter Med Meget Svær Kronisk Obstruktiv Lungelidelse (KOL): Gensidig Konstituering Af Teknologi, Daglig Livsførelse Og Professionel Praksis. Available online: https://paperpile.com/app/p/e7f2c6ba-c9f3-073f-9942-0fb0b52c7d40 (accessed on 10 September 2020).
- Li, Y.; Qian, H.; Yu, K.; Huang, Y. Nonadherence in Home-Based Pulmonary Rehabilitation Program for COPD Patients. Can. Respir. J. 2020, 2020, 5146765. [Google Scholar] [CrossRef] [Green Version]
- Fischer, M.J.; Scharloo, M.; Abbink, J.J.; van’t Hul, A.J.; van Ranst, D.; Rudolphus, A.; Weinman, J.; Rabe, K.F.; Kaptein, A.A. Drop-out and Attendance in Pulmonary Rehabilitation: The Role of Clinical and Psychosocial Variables. Respir. Med. 2009, 103, 1564–1571. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Features | Explanation |
|---|---|
| Video consultation sessions | Each patient met the physiotherapist in a video consultation to plan the rehabilitation program and to evaluate previous training experience. |
| E-learning packages | The patient had access to e-learning packages addressing psychological, medical, nutritional and physical aspects of IPF—in part supplied by relevant special data sources medicin.dk [19], lunge.dk [20] and helbredsprofilen.dk. [21] or created by dietitian students after in-depth interviews with pulmonary patients [22,23,24,25]. |
| Chat sessions | Allowed the patient to interact and get prompt answers from the physiotherapist. |
| Workout sessions with VAPA | The patients trained 10–20 min 3–5 times a week at home with their individual and tailored VAPA using training aids such as elastics, weights and a fitness-step to reach the highest workout intensity. The VAPA provided encouragement to keep on training during the workout. |
| Questionnaires | The patients filled out questionnaires regarding satisfaction, breathlessness, and adverse events reporting. |
| Variable | Tele-Rehabilitation with VAPA n = 15 | Control n = 14 |
|---|---|---|
| Male, n (%) | 13 (86.6%) | 8 (57.1%) |
| Age (years), mean (SD) | 70.1 (8.8) | 72.4 (7.6) |
| Months since diagnosis, median (IQR) | 8.8 (0.0–20) | 6.5 (0.0–7.5) |
| Smoking status Current, n (%) Former, n (%) Never, n (%) | 3 (20%) 11 (73.3%) 1 (6.8%) | 2 (14.3%) 9 (64.3%) 3 (21.5%) |
| Long-term oxygen therapy, n (%) | 3 (20%) | 0 (0%) |
| Antifibrotic treatment, n (%) | 12 (80%) | 14 (100%) |
| FVC (% predicted), mean (SD) | 76.73 (16.4) * | 90.8 (16.5) * |
| DLCO (% predicted), mean (SD) | 46.46 (11.0) | 55 (14.0) |
| 6MWD (m), mean (SD) | 461.5 (115.0) | 446 (63.6) |
| 7 days pedometry, mean (SD) | 13,629 (5314) | 11,883 (5237) |
| 7dVMCPM, mean (SD) | 480.3 (115.0) | 412.5 (178.3) |
| SGRQ-I total, mean (SD) | 49.8 (14.9) | 47.7 (16.7) |
| KBILD total, mean (SD) | 60.14 (12.1) | 58.6 (10.0) |
| GAD7, mean (SD) | 1.63 (2.5) | 2.36 (3.9) |
| Variable | Baseline | Three Months | Six Months | NINE MONTHS | ||||
|---|---|---|---|---|---|---|---|---|
| VAPA | Control | VAPA | Control | VAPA | Control | VAPA | Control | |
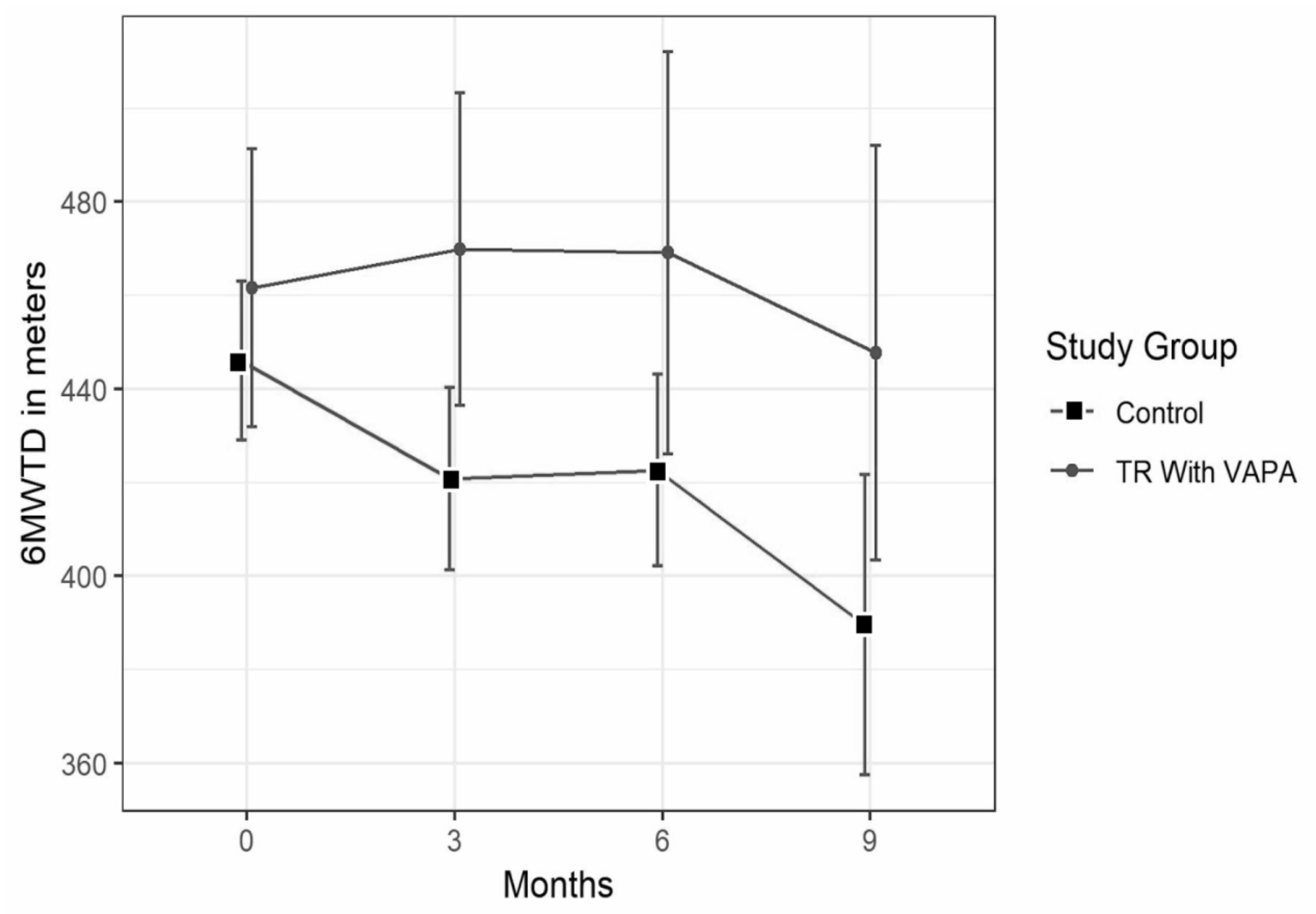
| 6MWTD | 461.5 ± 115 | 446 ± 63.6 | 470 ± 115 * | 421 ± 70 † | 469 ± 136 * | 423 ± 76 † | 448 ± 133 | 390 ± 85 |
| 7 days pedometer | 13,629 ± 5314 | 11,883 ± 5237 | 13,574 ± 8973 | 14,017 ± 9663 | 14,317 ± 12993 | 11,758 ± 6969 | 11,908 ± 7919 | 9936 ± 5804 |
| 7d VMCPM | 480.3 ± 115 | 412.5 ± 178 | 444 ± 180 | 393 ± 186 | 408 ± 161 | 368 ± 182 | 426 ± 205 | 321 ± 151 |
| SGRQ-I | 49.8 ± 14.9 | 47.7 ± 16.7 | 51.2 ± 17.8 | 43.3 ± 16.4 | 48.3 ± 13.3 | 49.7 ± 22.2 | 43.9 ± 19.4 | 45.9 ± 16.6 |
| K-BILD | 60.14 ± 12.1 | 58.6 ± 10 | 60.5 ± 10 | 59.6 ± 13.0 † | 63 ± 11.8 | 54.1 ± 6.6 | 61.7 ± 10.8 | 59.5 ± 10.6 |
| GAD7 | 1.63 ± 2.5 | 2.36 ± 3.9 | 3.27 ± 3.9 | 2.55 ± 3.3 | 2.9 ± 3.1 | 0.8 ± 1.7 | 2.1 ± 3.2 | 4.6 ± 3.7 |
| Expected | Trained | |||
|---|---|---|---|---|
| Patients | Period | Number | % | |
| 15 | 0–3 Months | 720 * | 463 * | 64 |
| 5 | 3–6 Months | 720 * | 775 * | 108 |
| 3 | 6–9 Months | 720 * | 792 * | 110 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cerdán-de-las-Heras, J.; Balbino, F.; Løkke, A.; Catalán-Matamoros, D.; Hilberg, O.; Bendstrup, E. Tele-Rehabilitation Program in Idiopathic Pulmonary Fibrosis—A Single-Center Randomized Trial. Int. J. Environ. Res. Public Health 2021, 18, 10016. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph181910016
Cerdán-de-las-Heras J, Balbino F, Løkke A, Catalán-Matamoros D, Hilberg O, Bendstrup E. Tele-Rehabilitation Program in Idiopathic Pulmonary Fibrosis—A Single-Center Randomized Trial. International Journal of Environmental Research and Public Health. 2021; 18(19):10016. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph181910016
Chicago/Turabian StyleCerdán-de-las-Heras, Jose, Fernanda Balbino, Anders Løkke, Daniel Catalán-Matamoros, Ole Hilberg, and Elisabeth Bendstrup. 2021. "Tele-Rehabilitation Program in Idiopathic Pulmonary Fibrosis—A Single-Center Randomized Trial" International Journal of Environmental Research and Public Health 18, no. 19: 10016. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph181910016