
Long-Term Care Facilities and Nursing Homes during the First Wave of the COVID-19 Pandemic: A Scoping Review of the Perspectives of Professionals, Families and Residents

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Inclusion and Exclusion Criteria
2.3. Identification of Studies: Search Strategy and Terms
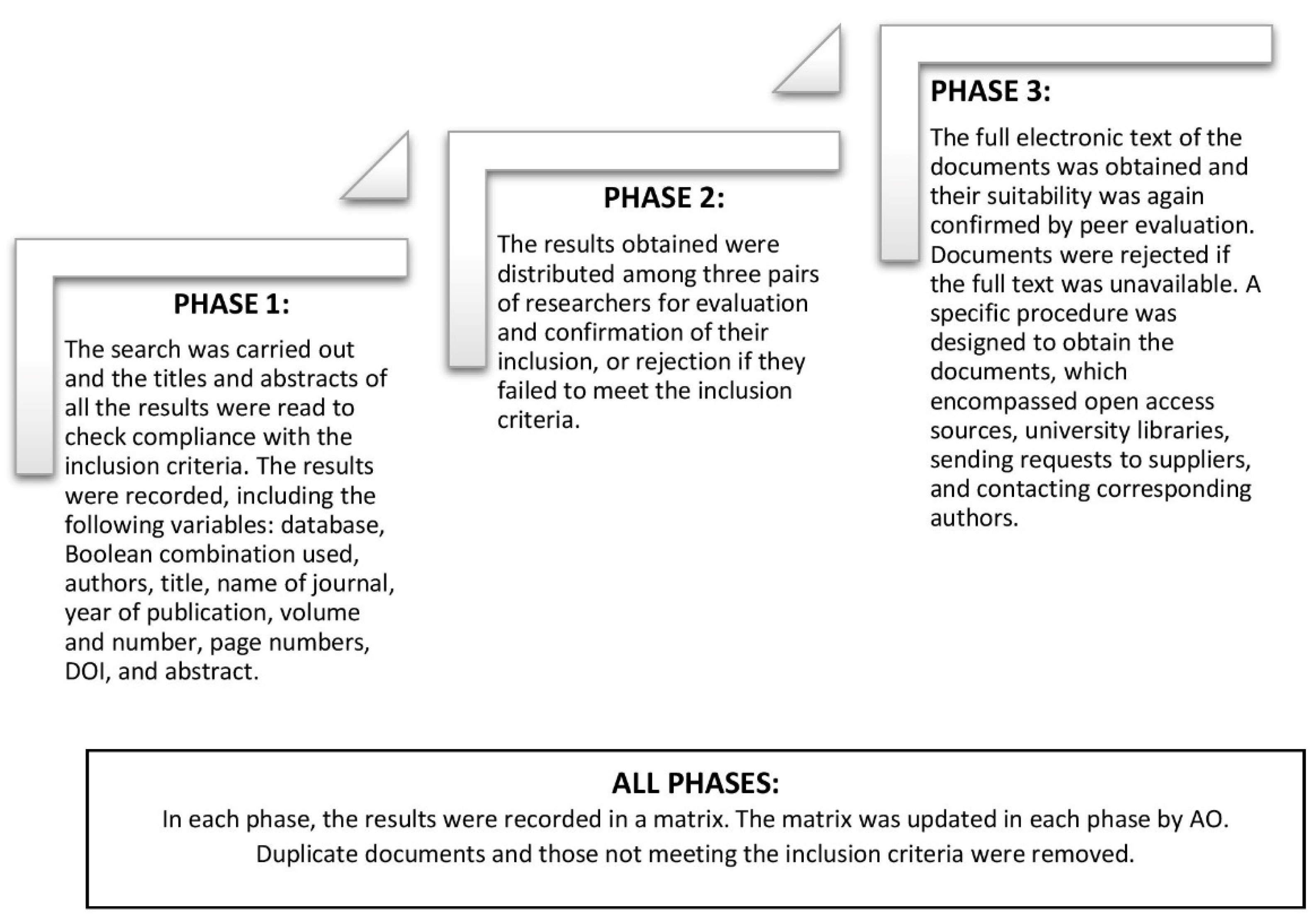
2.4. Screening for Eligibility
2.5. Data Extraction and Inclusion
2.6. Data Synthesis
3. Results
3.1. Study Characteristics
3.2. Deterioration of the Organisational Climate
3.2.1. Organisational Difficulties in Responding to the New Circumstances
3.2.2. Experiences of Emotional Exhaustion and Negative Perceptions
3.3. Adapting to Adversity
3.3.1. Innovation and Creativity in Response to Adversity
3.3.2. Acknowledging and Adapting to Shortcomings
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Weekly Epidemiological Update on COVID-19—20 April 2021. 2021. Available online: https://www.who.int/publications/m/item/weekly-epidemiological-update-on-covid-19---20-april-2021 (accessed on 24 May 2021).
- Shahid, Z.; Kalayanamitra, R.; McClafferty, B.; Kepko, D.; Ramgobin, D.; Patel, R.; Aggarwal, C.S.; Vunnam, R.; Sahu, N.; Bhatt, D.; et al. COVID-19 and older adults: What we know. J. Am. Geriatr. Soc. 2020, 68, 926–929. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, K.; Chen, Y.; Lin, R.; Han, K. Clinical features of COVID-19 in elderly patients: A comparison with young and middle-aged patients. J. Infect. 2020, 80, e14–e18. [Google Scholar] [CrossRef] [Green Version]
- Ho, F.K.; Petermann-Rocha, F.; Gray, S.R.; Jani, B.D.; Katikireddi, S.V.; Niedzwiedz, C.L.; Foster, H.; Hastie, C.E.; Mackay, D.F.; Gill, J.M.R.; et al. Is older age associated with COVID-19 mortality in the absence of other risk factors? General population cohort study of 470,034 participants. PLoS ONE 2020, 15, e0241824. [Google Scholar] [CrossRef]
- Peeri, N.C.; Shrestha, N.; Rahman, M.S.; Zaki, R.; Tan, Z.; Bibi, S.; Baghbanzadeh, M.; Aghamohammadi, N.; Zhang, W.; Haque, U. The SARS, MERS and novel coronavirus (COVID-19) epidemics, the newest and biggest global health threats: What lessons have we learned? Int. J. Epidemiol. 2020, 49, 717–726. [Google Scholar] [CrossRef] [Green Version]
- Center for Disease Control (CDC). People at Increased Risk: Older Adults. Available online: https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/older-adults.html (accessed on 3 December 2020).
- Hashan, M.R.; Smoll, N.; King, C.; Ockenden-Muldoon, H.; Walker, J.; Wattiaux, A.; Graham, J.; Booy, R.; Khandaker, G. Epidemiology and clinical features of COVID-19 outbreaks in aged care facilities: A systematic review and meta-analysis. EClinicalMedicine 2021, 33, 100771. [Google Scholar] [CrossRef] [PubMed]
- Kluge, H.P. Statement—Invest in the Overlooked and Unsung: Build Sustainable People-Centred Long-Term Care in the Wake of COVID-19. Available online: https://www.euro.who.int/en/media-centre/sections/statements/2020/statement-invest-in-the-overlooked-and-unsung-build-sustainable-people-centred-long-term-care-in-the-wake-of-covid-19 (accessed on 20 May 2021).
- D’Adamo, H.; Yoshikawa, T.; Ouslander, J.G. Coronavirus disease 2019 in geriatrics and long-term care: The ABCDs of COVID-19. J. Am. Geriatr. Soc. 2020, 68, 912–917. [Google Scholar] [CrossRef]
- De Pue, S.; Gillebert, C.; Dierckx, E.; Vanderhasselt, M.-A.; de Raedt, R.; Bussche, E.V.D. The impact of the COVID-19 pandemic on wellbeing and cognitive functioning of older adults. Sci. Rep. 2021, 11, 1–11. [Google Scholar] [CrossRef]
- Levere, M.; Rowan, P.; Wysocki, A. The adverse effects of the COVID-19 pandemic on nursing home resident well-being. J. Am. Med. Dir. Assoc. 2021, 22, 948–954. [Google Scholar] [CrossRef] [PubMed]
- Van der Roest, H.G.; Prins, M.; van der Velden, C.; Steinmetz, S.; Stolte, E.; van Tilburg, T.G.; de Vries, D.H. The impact of COVID-19 measures on well-being of older long-term care facility residents in the Netherlands. J. Am. Med. Dir. Assoc. 2020, 21, 1569–1570. [Google Scholar] [CrossRef] [PubMed]
- Wammes, J.D.; Kolk, D.; van den Besselaar, J.H.; MacNeil-Vroomen, J.L.; Buurman-Van Es, B.M.; van Rijn, M. Evaluating perspectives of relatives of nursing home residents on the nursing home visiting restrictions during the COVID-19 crisis: A Dutch cross-sectional survey study. J. Am. Med. Dir. Assoc. 2020, 21, 1746–1750. [Google Scholar] [CrossRef]
- White, E.M.; Wetle, T.F.; Reddy, A.; Baier, R.R. Front-line nursing home staff experiences during the COVID-19 pandemic. J. Am. Med. Dir. Assoc. 2021, 22, 199–203. [Google Scholar] [CrossRef]
- Blanco-Donoso, L.M.; Moreno-Jiménez, J.; Amutio, A.; Gallego-Alberto, L.; Moreno-Jiménez, B.; Garrosa, E. Stressors, job resources, fear of contagion, and secondary traumatic stress among nursing home workers in face of the COVID-19: The case of Spain. J. Appl. Gerontol. 2021, 40, 244–256. [Google Scholar] [CrossRef]
- Sun, N.; Wei, L.; Wang, H.; Wang, X.; Gao, M.; Hu, X.; Shi, S. Qualitative study of the psychological experience of COVID-19 patients during hospitalization. J. Affect. Disord. 2021, 278, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Wittenberg, E.; Sullivan, S.S.; Lorenz, R.A.; Chang, Y.-P. The experiences of family members of ventilated COVID-19 patients in the intensive care unit: A qualitative study. Am. J. Hosp. Palliat. Med. 2021, 38, 869–876. [Google Scholar] [CrossRef] [PubMed]
- Chegini, Z.; Arab-Zozani, M.; Rajabi, M.R.; Kakemam, E. Experiences of critical care nurses fighting against COVID-19: A qualitative phenomenological study. Nurs. Forum 2021, 56, 571–578. [Google Scholar] [CrossRef] [PubMed]
- Joo, J.Y.; Liu, M.F. Nurses’ barriers to caring for patients with COVID-19: A qualitative systematic review. Int. Nurs. Rev. 2021, 68, 202–213. [Google Scholar] [CrossRef]
- Liu, Q.; Luo, D.; Haase, J.E.; Guo, Q.; Wang, X.Q.; Liu, S.; Xia, L.; Liu, Z.; Yang, J.; Yang, B.X. The experiences of health-care providers during the COVID-19 crisis in China: A qualitative study. Lancet Glob. Health 2020, 8, e790–e798. [Google Scholar] [CrossRef]
- Fernandez, R.; Lord, H.; Halcomb, E.; Moxham, L.; Middleton, R.; Alananzeh, I.; Ellwood, L. Implications for COVID-19: A systematic review of nurses’ experiences of working in acute care hospital settings during a respiratory pandemic. Int. J. Nurs. Stud. 2020, 111, 103637. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.; Colquhoun, H.; Kastner, M.; Levac, D.; Ng, C.; Sharpe, J.P.; Wilson, K.; et al. A scoping review on the conduct and reporting of scoping reviews. BMC Med. Res. Methodol. 2016, 16, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Tricco, A.; Lillie, E.; Zarin, W.; O’Brien, K.; Al, E. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [Green Version]
- Joanna Briggs Institute. Joanna Briggs Institute Reviewers Manual; Joanna Briggs Institute: Adelaide, SA, Australia, 2014. [Google Scholar]
- Levac, D.; Colquhoun, H.; O’Brien, K. Scoping studies: Advancing the methodology. Implement. Sci. 2010, 5, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19—11 March 2020. 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 10 June 2021).
- Creswell, J.; Poth, C.N. Qualitative Inquiry and Research Design. Choosing Among Five Approaches, 4th ed.; Sage: Thousand Oaks, CA, USA, 2018. [Google Scholar]
- Harris, J.L.; Booth, A.; Cargo, M.; Hannes, K.; Harden, A.; Flemming, K.; Garside, R.; Pantoja, T.; Thomas, J.; Noyes, J. Cochrane qualitative and implementation methods group guidance series—Paper 2: Methods for question formulation, searching, and protocol development for qualitative evidence synthesis. J. Clin. Epidemiol. 2018, 97, 39–48. [Google Scholar] [CrossRef] [PubMed]
- Lewin, S.; Booth, A.; Glenton, C.; Munthe-Kaas, H.; Rashidian, A.; Wainwright, M.; Bohren, M.A.; Tunçalp, Ö.; Colvin, C.J.; Garside, R.; et al. Applying GRADE-CERQual to qualitative evidence synthesis findings: Introduction to the series. Implement. Sci. 2018, 13, 1–10. [Google Scholar] [CrossRef]
- Curry, L.; Nunez-Smith, M. Mixed Methods in Health Sciences Research: A Practical Primer; SAGE Publications Ltd.: New York, NY, USA, 2015. [Google Scholar]
- Pham, M.T.; Rajić, A.; Greig, J.D.; Sargeant, J.M.; Papadopoulos, A.; McEwen, S.A. A scoping review of scoping reviews: Advancing the approach and enhancing the consistency. Res. Synth. Methods 2014, 5, 371–385. [Google Scholar] [CrossRef]
- Bergman, C.; Stall, N.M.; Haimowitz, D.; Aronson, L.; Lynn, J.; Steinberg, K.; Wasserman, M. Recommendations for welcoming back nursing home visitors during the COVID-19 pandemic: Results of a Delphi panel. J. Am. Med. Dir. Assoc. 2020, 21, 1759–1766. [Google Scholar] [CrossRef]
- Cocuzzo, B.; Wrench, A.; O’Malley, C. Balancing protection from COVID-19 and the need for human touch in nursing homes. J. Am. Geriatr. Soc. 2020, 68, 2749–2751. [Google Scholar] [CrossRef]
- Cousins, E.; de Vries, K.; Dening, K.H. Ethical care during COVID-19 for care home residents with dementia. Nurs. Ethics 2021, 28, 46–57. [Google Scholar] [CrossRef] [PubMed]
- Marshall, F.; Gordon, A.; Gladman, J.R.F.; Bishop, S. Care homes, their communities, and resilience in the face of the COVID-19 pandemic: Interim findings from a qualitative study. BMC Geriatr. 2021, 21, 1–10. [Google Scholar] [CrossRef]
- Spilsbury, K.; Devi, R.; Griffiths, A.; Akrill, C.; Astle, A.; Goodman, C.; Gordon, A.; Hanratty, B.; Hodkinson, P.; Marshall, F.; et al. SEeking AnsweRs for care homes during the COVID-19 pandemic (COVID SEARCH). Age Ageing 2021, 50, 335–340. [Google Scholar] [CrossRef]
- Fearn, M.; Harper, R.; Major, G.; Bhar, S.; Bryant, C.; Dow, B.; Dunt, D.; Mnatzaganian, G.; O’Connor, D.; Ratcliffe, J.; et al. Befriending older adults in nursing homes: Volunteer perceptions of switching to remote befriending in the COVID-19 era. Clin. Gerontol. 2021, 44, 430–438. [Google Scholar] [CrossRef]
- Frahsa, A.; Altmeier, D.; John, J.M.; Gropper, H.; Granz, H.; Pomiersky, R.; Haigis, D.; Eschweiler, G.W.; Nieß, A.M.; Sudeck, G.; et al. “I trust in staff’s creativity”—The impact of COVID-19 lockdowns on physical activity promotion in nursing homes through the lenses of organizational sociology. Front. Sports Act. Living 2020, 2, 589214. [Google Scholar] [CrossRef] [PubMed]
- Havaei, F.; MacPhee, M.; Keselman, D.; Staempfli, S. Leading a long-term care facility through the COVID-19 crisis: Successes, barriers and lessons learned. Healthc Q. 2021, 23, 28–34. [Google Scholar] [CrossRef] [PubMed]
- Kabir, Z.N.; Boström, A.-M.; Konradsen, H. In conversation with a frontline worker in a care home in Sweden during the COVID-19 pandemic. J. Cross-Cult. Gerontol. 2020, 35, 493–500. [Google Scholar] [CrossRef] [PubMed]
- Lázaro, R.; Pinzón, S.; Díaz-Veiga, P.; Castejón Villarejo, P.; Azurmendi, M.; Uriarte, A. Conversaciones en centros residenciales de personas mayores durante la COVID-19: Impacto en las profesionales de los cuidados. Zerbitzuan 2021, 73, 25–43. [Google Scholar] [CrossRef]
- Leontjevas, R.; Knippenberg, I.A.; Smalbrugge, M.; Plouvier, A.O.; Teunisse, S.; Bakker, C.; Koopmans, R.T.; Gerritsen, D.L. Challenging behavior of nursing home residents during COVID-19 measures in the Netherlands. Aging Ment. Health 2021, 25, 1314–1319. [Google Scholar] [CrossRef] [PubMed]
- Verbeek, H.; Gerritsen, D.L.; Backhaus, R.; de Boer, B.S.; Koopmans, R.T.; Hamers, J.P. Allowing visitors back in the nursing home during the COVID-19 crisis: A Dutch national study into first experiences and impact on well-being. J. Am. Med. Dir. Assoc. 2020, 21, 900–904. [Google Scholar] [CrossRef] [PubMed]
- Bolt, S.R.; van der Steen, J.T.; Mujezinović, I.; Janssen, D.J.; Schols, J.M.; Zwakhalen, S.M.; Khemai, C.; Knapen, E.P.; Dijkstra, L.; Meijers, J.M. Practical nursing recommendations for palliative care for people with dementia living in long-term care facilities during the COVID-19 pandemic: A rapid scoping review. Int. J. Nurs. Stud. 2021, 113, 103781. [Google Scholar] [CrossRef]
- Leskovic, L.; Erjavec, K.; Leskovar, R.; Vukovič, G. Burnout and job satisfaction of healthcare workers in Slovenian nursing homes in rural areas during the COVID-19 pandemic. Ann. Agric. Environ. Med. 2020, 27, 664–671. [Google Scholar] [CrossRef]
- Chee, S.Y. COVID-19 pandemic: The lived experiences of older adults in aged care homes. Millenn. Asia 2020, 11, 299–317. [Google Scholar] [CrossRef]
- Sarabia-Cobo, C.; Pérez, V.; de Lorena, P.; Hermosilla-Grijalbo, C.; Sáenz-Jalón, M.; Fernández-Rodríguez, A.; Alconero-Camarero, A.R. Experiences of geriatric nurses in nursing home settings across four countries in the face of the COVID-19 pandemic. J. Adv. Nurs. 2021, 77, 869–878. [Google Scholar] [CrossRef] [PubMed]
- Houlding, E.; Mate, K.; Engler, K.; Ortiz-Paredes, D.; Pomey, M.; Cox, J.; Hijal, T.; Lebouché, B. Barriers to use of remote monitoring technologies used to support patients with COVID-19: Rapid review. JMIR mHealth uHealth 2021, 9, e24743. [Google Scholar] [CrossRef] [PubMed]
- Mo, S.; Shi, J. The psychological consequences of the COVID-19 on residents and staff in nursing homes. Work Aging Retire. 2020, 6, 254–259. [Google Scholar] [CrossRef]
- O’Caoimh, R.; O’Donovan, M.R.; Monahan, M.P.; O’Connor, C.D.; Buckley, C.; Kilty, C.; Fitzgerald, S.; Hartigan, I.; Cornally, N. Psychosocial impact of COVID-19 nursing home restrictions on visitors of residents with cognitive impairment: A cross-sectional study as part of the engaging remotely in care (ERiC) project. Front. Psychiatry 2020, 11, 585373. [Google Scholar] [CrossRef]
- Instituto de Mayores y Servicios Sociales (IMSERSO). Informe del Grupo de Trabajo COVID-19 y Residencias. Versión Final (24/11/2020); Instituto de Mayores y Servicios Sociales (IMSERSO): Madrid, Spain, 2020. Available online: https://www.mscbs.gob.es/ssi/imserso/docs/GTCOVID_19_RESIDENCIAS.pdf (accessed on 22 September 2021).
- Comas-Herrera, A.; Zalakaín, J.; Lemmon, E.; Henderson, D.; Litwin, C.; Hsu, A.; Schmidt, A.; Arling, G.; Kruse, F.; Fernández, J.-L. Mortality Associated with COVID-19 in Care Homes: Early International Evidence. 2020. Available online: https://ltccovid.org/wp-content/uploads/2021/02/LTC_COVID_19_international_report_January-1-February-1-2.pdf (accessed on 22 September 2021).
- Ouslander, J.; Grabowski, D. COVID-19 in nursing homes: Calming the perfect storm. J. Am. Geriatr. Soc. 2020, 10, 2153–2162. [Google Scholar] [CrossRef]
- Rodriguez-Jimenez, M.; Guerrero-Barona, E.; García-Gomez, A. Mental health and psychological capital among Spanish health care workers during COVID-19 pandemic. Med. Clin. 2021, 156, 357–358. [Google Scholar]
- Youssef, C.; Luthans, F. Positive organizational behavior in the workplace: The impact of hope, optimism, and resilience. J. Manag. 2007, 33, 774–800. [Google Scholar] [CrossRef]
- Chen, X.; Wu, L. Psychological capital in food safety social co-governance. Front. Psychol. 2019, 10, 1–6. [Google Scholar] [CrossRef]
- Luthans, F.; Youssef, C.M. Human, social, and now positive psychological capital management: Investing in people for competitive advantage. Organ. Dyn. 2004, 33, 143–160. [Google Scholar] [CrossRef]
- Carver, C.S.; Scheier, M.F.; Segertrom, S.C. Optimism. Clin. Psychol. Rev. 2010, 30, 879–889. [Google Scholar] [CrossRef] [Green Version]
- Luthans, F. The need for and meaning of positive organizational behavior. J. Organ. Behav. 2002, 23, 695–706. [Google Scholar] [CrossRef] [Green Version]
- Bandura, A. Self-Efficacy: The Exercice of Control; W.H. Freeman: New York, NY, USA, 1997. [Google Scholar]
- Hodfoll, S.E. Social and psychological resources and adaptation. Rev. Gen. Psychol. 2002, 6, 307–324. [Google Scholar] [CrossRef]
- Aviv-Reuven, S.; Rosenfeld, A. Publication patterns’ changes due to the COVID-19 pandemic: A longitudinal and short-term scientometric analysis. Scientometrics 2021, 126, 6761–6784. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Combinations | English Terms | Spanish Terms |
|---|---|---|
| First combination | (COVID* OR pandemic* OR coronavirus infection* OR SARS*) AND (Health Personnel OR Allied Health Personnel OR Health provider OR health care workers) AND (“qualitative research” OR “mixed research”) | (COVID* O pandem* O infección coronavirus* O SARS*) Y (Personal Salud O Profesional salud O Proveedor salud O trabajadores salud) Y (“investigación cualitativa” O “investigación mixta”) |
| Second combination | (COVID* OR pandemic* OR coronavirus infection* OR SARS*) AND (“Nursing homes” OR “long-term facilities” OR “Health Services for the Aged” OR “Geriatric Hospitals”) AND (“Health Personnel” OR “Allied Health Personnel” OR “Health provider” OR “health care workers”) AND (Attitude OR Attitude of Health Personnel OR Perception OR experience OR Perspective OR feeling OR knowledge) AND (“qualitative research” OR “mixed research”) | (COVID* O pandem* O * infección coronavirus* O SARS*) Y (“Residencias” O “centros cuidados prolongados” O “Servicios Salud para mayores” O “Hospitales Geriátricos”) Y (“Personal salud” O “Profesional Salud” O “Proveedor salud” O “trabajadores salud”) Y (Actitud O Actitud profesional salud O Percepción O experiencia O Perspectiva O Sentimientos O conocimiento) AND (“investigación cualitativa” O “investigación mixta”) |
| Third combination | (COVID* OR pandemic* OR coronavirus infection* OR SARS) AND (“Nursing homes” OR “long-term facilities” OR “Health Services for the Aged” OR “Geriatric Hospitals”) AND (“Health Personnel” OR “Allied Health Personnel” OR “Health provider” OR “health care workers”) AND (“qualitative research” OR “mixed research”) | (COVID* O pandem* O * infección coronavirus* O SARS*) Y (“Residencias” O “centros cuidados prolongados” O “Servicios Salud para mayores” O “Hospitales Geriátricos”) Y (“Personal salud” O “Profesional Salud” O “Proveedor salud” O “trabajadores salud”) Y (“investigación cualitativa” O “investigación mixta”) |
| Fourth combination | (COVID* OR pandemic* OR coronavirus infection* OR SARS*) AND (“Nursing homes” OR “long-term facilities” OR “Health Services for the Aged” OR “Geriatric Hospitals”) AND ( “qualitative research” OR “mixed research”) | (COVID* O pandem* O * infección coronavirus* O SARS*) Y (“Residencias” O “centros cuidados prolongados” O “Servicios Salud para mayores” O “Hospitales Geriátricos”) Y (“investigación cualitativa” O “investigación mixta”) |
| Items | Observations |
|---|---|
| Language | English, French, Portuguese, Spanish |
| Objectives/aims | To identify each study’s objectives and research questions. |
| Design | Qualitative research (phenomenology, grounded theory, etc.), mixed methods research (sequential, embedded, etc.) |
| Participants | Total number, distribution by type (residents, family members, healthcare professionals, social care professionals) and sex. |
| Setting and/or context | Nursing homes, long-term care facilities. |
| Sampling strategies | Purposive, convenience. Identification of end of recruitment (theoretical saturation of data, information redundancy, etc.) |
| Data collection tools | Interviews, observation, focus groups, questionnaires with open-ended questions. Identification of end of recruitment (theoretical saturation of data, information redundancy, etc.) |
| Findings | Identification of results obtained, description and classification into categories, themes, metacategories, etc. |
| Identification of other references | Identification of other references that may meet the inclusion criteria in the bibliography. Cross references obtained after reading document. The full screening process was applied to each additional reference. |
| Deterioration of the Organisational Climate | Adapting to Adversity | |||
|---|---|---|---|---|
| Authors | Organisational Difficulties in Responding to the New Circumstances | Experiences of Emotional Exhaustion and Negative Perceptions | Innovation and Creativity in Responses to Adversity | Acknowledging and Adapting to Shortcomings |
| Bergman et al., 2020 [32] β | X | X | X | |
| Bolt et al., 2021 [44] β | X | X | X | |
| Chee, 2020 [46] * | X | |||
| Cocuzzo et al., 2020 [33] * | X | |||
| Cousins et al., 2021 [34] β | X | X | X | X |
| Fearn et al., 2021 [37] β | X | X | ||
| Frahsa et al., 2020 [38] β,& | X | X | X | X |
| Havaei et al., 2021 [39] β | X | X | X | |
| Kabir et al., 2020 [40] β | X | X | X | X |
| Lázaro et al., 2020 [41] β | X | X | X | X |
| Leontjevas et al., 2020 [42] β | X | X | X | X |
| Leskovic et al., 2020 [45] β | X | X | X | X |
| Marshall et al., 2021 [35] β | X | X | X | X |
| Sarabia-Cobo et al., 2020 [47] β | X | X | X | X |
| Spilsbury et al., 2020 [36] β | X | X | X | |
| Verbeek et al., 2020 [43] β | X | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Palacios-Ceña, D.; Fernández-Peña, R.; Ortega-López, A.; Fernández-Feito, A.; Bautista-Villaécija, O.; Rodrigo-Pedrosa, O.; Arnau-Sánchez, J.; Lizcano-Álvarez, Á. Long-Term Care Facilities and Nursing Homes during the First Wave of the COVID-19 Pandemic: A Scoping Review of the Perspectives of Professionals, Families and Residents. Int. J. Environ. Res. Public Health 2021, 18, 10099. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph181910099
Palacios-Ceña D, Fernández-Peña R, Ortega-López A, Fernández-Feito A, Bautista-Villaécija O, Rodrigo-Pedrosa O, Arnau-Sánchez J, Lizcano-Álvarez Á. Long-Term Care Facilities and Nursing Homes during the First Wave of the COVID-19 Pandemic: A Scoping Review of the Perspectives of Professionals, Families and Residents. International Journal of Environmental Research and Public Health. 2021; 18(19):10099. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph181910099
Chicago/Turabian StylePalacios-Ceña, Domingo, Rosario Fernández-Peña, Angela Ortega-López, Ana Fernández-Feito, Oscar Bautista-Villaécija, Olga Rodrigo-Pedrosa, José Arnau-Sánchez, and Ángel Lizcano-Álvarez. 2021. "Long-Term Care Facilities and Nursing Homes during the First Wave of the COVID-19 Pandemic: A Scoping Review of the Perspectives of Professionals, Families and Residents" International Journal of Environmental Research and Public Health 18, no. 19: 10099. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph181910099