
Remediation Strategies for Performance Anxiety across Sex, Sport and Stage: Identifying Common Approaches and a Unified Cognitive Model



Abstract
:1. Introduction
1.1. Aims of the Current Review
1.2. Methodology
2. Treatment/Remediation Strategies
2.1. Strategies Related to Remediating Sexual Anxiety
Section Summary
2.2. Strategies Related to “Choking” and Competitive Sport Anxiety
Section Summary
2.3. Strategies Related to Stage Anxiety
2.3.1. Specific Organizing Strategies
2.3.2. Cognitive-Behavioral Approaches
2.3.3. Group Approaches
2.3.4. Section Summary
2.4. A Summary of Commonalities and Contrasts
3. Intervention and Remediation: Integration
3.1. Overview of the Structure of Interventions
3.2. Intervention Delivery Formats
3.3. Examples of Core Strategies Common to the Domains
3.4. Examples of Related/Secondary Strategies
3.5. Examples of Domain-Specific Strategies
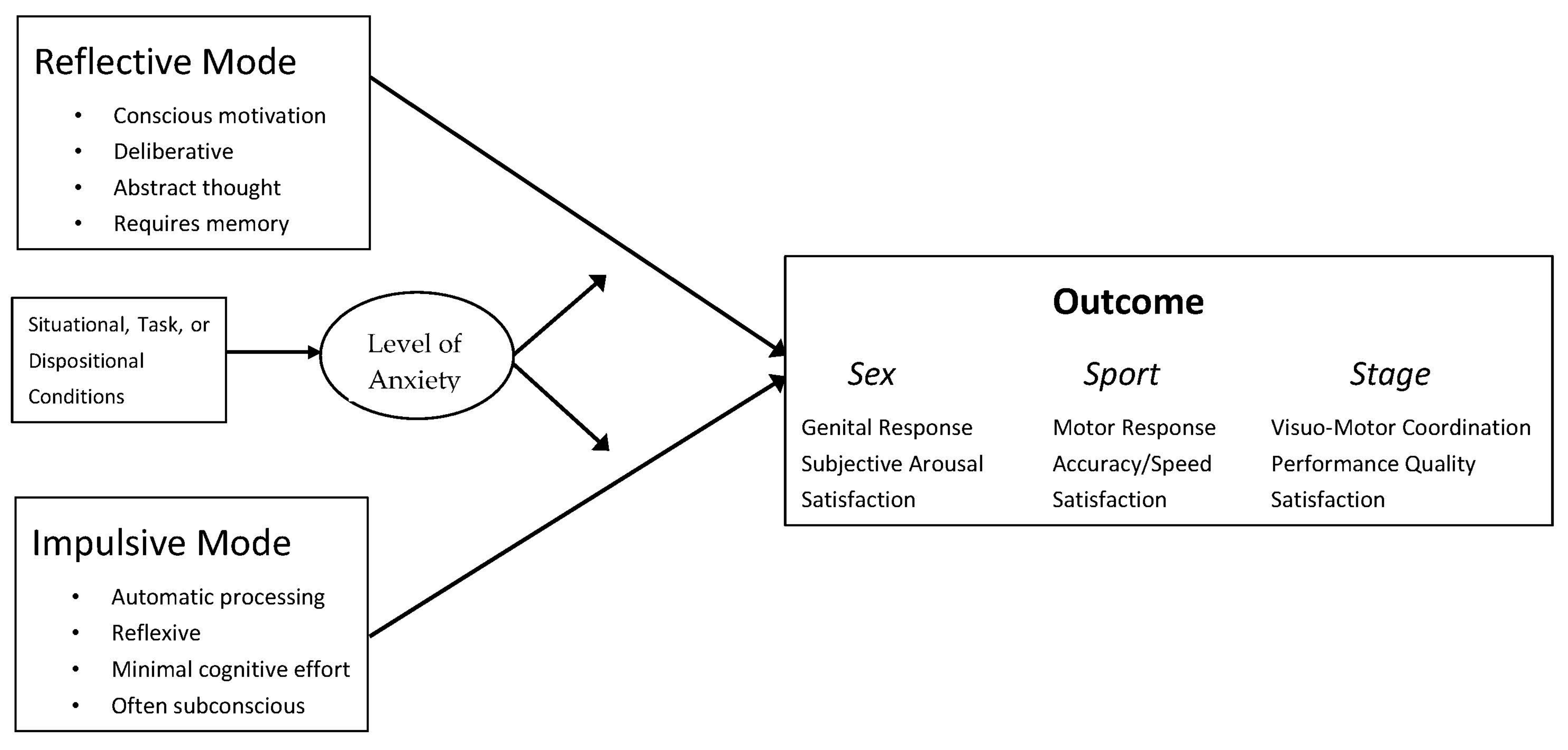
4. Relationship of Treatment Strategies to the Reflective-Impulsive Model
4.1. RIM: A Better Model to Meet the Goals of Understanding, Prediction, and Control
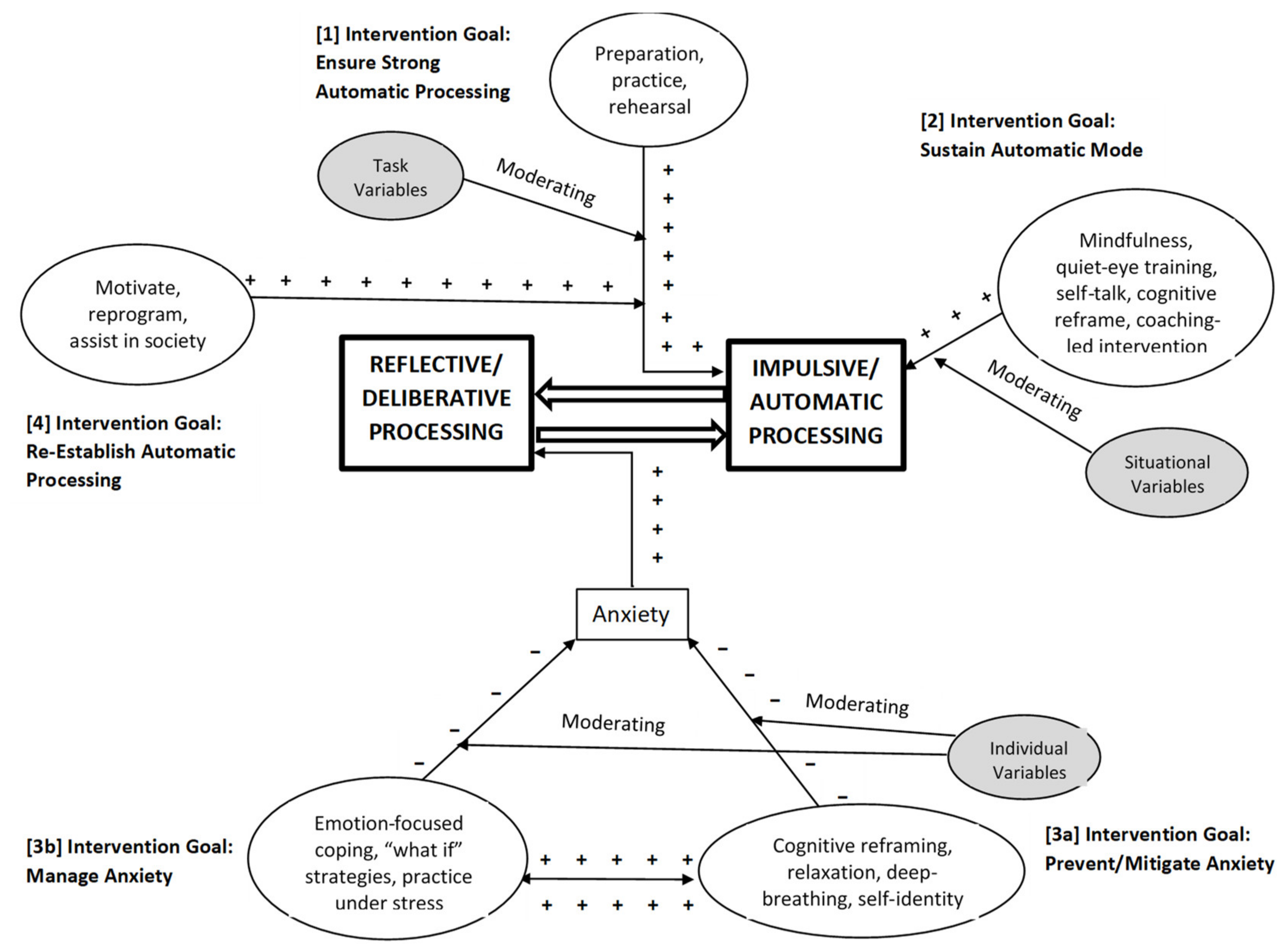
4.2. Hypothesized Connections between Intervention Strategies and RIM
5. Conclusions and Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Biasutti, M.; Concina, E. The role of coping strategy and experience in predicting music performance anxiety. Music. Sci. 2014, 18, 189–202. [Google Scholar] [CrossRef]
- Kenny, D. The Psychology of Music Performance Anxiety; Oxford University Press: Oxford, UK, 2011. [Google Scholar]
- Kleine, D. Anxiety and sport performance: A meta-analysis. Anxiety Res. 1990, 2, 113–131. [Google Scholar] [CrossRef]
- Barlow, D.H. Anxiety and Its Disorders: The Nature and Treatment of Anxiety and Panic, 2nd ed.; Guilford Press: New York, NY, USA, 2002. [Google Scholar]
- Oudejans, R.R.; Binsch, O.; Bakker, F.C. Negative instructions and choking under pressure in aiming at a far target. Int. J. Sport Psychol. 2013, 44, 294–309. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Publishing: Washington, DC, USA, 2013. [Google Scholar]
- Bögels, S.M.; Lamers, C.T.J. The causal role of self-awareness in blushing-anxious, socially-anxious and social phobics individuals. Behav. Res. Ther. 2002, 40, 1367–1384. [Google Scholar] [CrossRef]
- Hope, D.A.; Heimberg, R.G. Public and private self-consciousness and social phobia. J. Pers. Assess. 1988, 52, 626–639. [Google Scholar] [CrossRef]
- Bancroft, J. Human Sexuality and Its Problems; Churchill Livingstone: London, UK, 2009. [Google Scholar]
- Barlow, D.H. Causes of sexual dysfunction: The role of anxiety and cognitive interference. J. Consult. Clin. Psychol. 1986, 54, 140–148. [Google Scholar] [CrossRef] [PubMed]
- Dèttore, D.; Pucciarelli, M.; Santarnecchi, E. Anxiety and female sexual functioning: An empirical study. J. Sex Marital. Ther. 2013, 39, 216–240. [Google Scholar] [CrossRef] [PubMed]
- Gerrior, K.G.; Watt, M.C.; Weaver, A.D.; Gallagher, C.E. The role of anxiety sensitivity in the sexual functioning of young women. Sex. Relatsh. Ther. 2015, 30, 351–363. [Google Scholar] [CrossRef]
- Wilson, M.R. Anxiety: Attention, the brain, the body, and performance. In The Oxford Handbook of Sport and Performance Psychology; Murphy, S., Ed.; Oxford University Press: Oxford, UK, 2012; pp. 173–190. [Google Scholar]
- Mao, J.; Chang, S.; Gong, Y.; Xie, J.L. Team job-related anxiety and creativity: Investigating team-level and cross-level moderated curvilinear relationships. J. Organ. Behav. 2020, 42, 34–47. [Google Scholar] [CrossRef]
- McLarnon, M.J.W.; O’Neill, T.A.; Taras, V.; Law, D.; Donia, M.B.L.; Steel, P. Global virtual team communication, coordination, and performance across three peer feedback strategies. Can. J. Behav. Sci. 2019, 51, 207–218. [Google Scholar] [CrossRef]
- Rowland, D.L.; Van Lankveld, J.J.D.M. Anxiety and performance in sex, sport, and stage: Identifying common ground. Front. Psychol. 2019, 10, 1615. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, S.L.; Hanrahan, S.J. Mental skills for musicians: Managing music performance anxiety and enhancing performance. Sport Exerc. Perform. Psychol. 2012, 1, 17–28. [Google Scholar] [CrossRef]
- Strack, F.; Deutsch, R. Reflective and impulsive determinants of social behavior. Pers. Soc. Psychol. Rev. 2004, 8, 220–247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strack, F.; Deutsch, R. The reflective—Impulsive model. In Dual-Process Theories of the Social Mind; Sherman, W., Gawronski, B., Trope, Y., Eds.; The Guilford Press: New York, NY, USA, 2014; pp. 92–104. [Google Scholar]
- Masters, W.H.; Johnson, V.E. Human Sexual Inadequacy; Little, Brown and Company: Boston, MA, USA, 1970. [Google Scholar]
- Kaplan, H.S. The New Sex Therapy: Active Treatment of Sexual Dysfunctions; Brunner/Mazel: New York, NY, USA, 1974. [Google Scholar]
- Meana, M. Sexual Dysfunction in Women: Advances in Psychotherapy, Evidence-Based Practice; Hogrefe: Cambridge, MA, USA, 2012. [Google Scholar]
- Rowland, D.; Cooper, S. Practical tips for sexual counseling and psychotherapy in premature ejaculation. J. Sex. Med. 2011, 8, 342–352. [Google Scholar] [CrossRef] [PubMed]
- Brotto, L.A.; Bergeron, S.; Zdaniuk, B.; Driscoll, M.; Grabovac, A.; Sadownik, L.A.; Smith, K.B.; Basson, R. A comparison of mindfulness-based cognitive therapy vs cognitive behavioral therapy for the treatment of provoked vestibulodynia in a hospital clinic setting. J. Sex. Med. 2019, 16, 909–923. [Google Scholar] [CrossRef]
- Nobre, P.J.; Pinto-Gouveia, J. Cognitions, emotions, and sexual response: Analysis of the relationship among automatic thoughts, emotional responses, and sexual arousal. Arch. Sex. Behav. 2007, 37, 652–661. [Google Scholar] [CrossRef] [Green Version]
- Van Lankveld, J.J.; Hout, M.A.V.D.; Schouten, E.G. The effects of self-focused attention, performance demand, and dispositional sexual self-consciousness on sexual arousal of sexually functional and dysfunctional men. Behav. Res. Ther. 2004, 42, 915–935. [Google Scholar] [CrossRef]
- Rowland, D.L. Sexual Dysfunction in Men; Hogrefe Publishing: Cambridge, MA, USA, 2012. [Google Scholar]
- Brotto, L.A.; Basson, R. Group mindfulness-based therapy significantly improves sexual desire in women. Behav. Res. Ther. 2014, 57, 43–54. [Google Scholar] [CrossRef]
- Mize, S.J.; Iantaffi, A. The place of mindfulness in a sensorimotor psychotherapy intervention to improve women’s sexual health. Sex. Relatsh. Ther. 2013, 28, 63–76. [Google Scholar] [CrossRef]
- Kabat-Zinn, J. Meditation Is Not What You Think: Mindfulness and Why It Is So Important; Hachette Book Group, Inc.: Lebanon, IN, USA, 2018. [Google Scholar]
- Segal, Z.V.; Williams, J.M.G.; Teasdale, J.D. Mindfulness-Based Cognitive Therapy for Depression: A New Approach to Preventing Relapse; Guilford Press: New York, NY, USA, 2002. [Google Scholar]
- Greenberg, L. Emotion-focused therapy. Clin. Psychol. Psychother. 2004, 11, 3–16. [Google Scholar] [CrossRef]
- Chin, F.; Hayes, S.C. Acceptance and commitment therapy and the cognitive behavioral tradition: Assumptions, model, methods, and outcomes. In The Science of Cognitive Behavioral Therapy; Hofmann, S., Asmundson, G., Eds.; Elsevier Academic Press: Cambridge, MA, USA, 2017; pp. 155–173. [Google Scholar]
- Althof, S.E. Psychosexual therapy for premature ejaculation. Transl. Androl. Urol. 2016, 5, 475–481. [Google Scholar] [CrossRef] [Green Version]
- De Carufel, F.; Trudel, G. Effects of a new functional-sexological treatment for premature ejaculation. J. Sex Marital. Ther. 2006, 32, 97–114. [Google Scholar] [CrossRef]
- La Pera, G.; Nicastro, A. A new treatment for premature ejaculation: The rehabilitation of the pelvic floor. J. Sex Marital. Ther. 1996, 22, 22–26. [Google Scholar] [CrossRef]
- Rowland, D.L. A conceptual approach to understanding and managing men’s orgasmic difficulties. Urol. Clin. N. Am. 2021, 48. [Google Scholar] [CrossRef]
- Ter Kuile, M.M.; Melles, R.; De Groot, H.E.; Tuijnman-Raasveld, C.C.; Van Lankveld, J.J.D.M. Therapist-aided exposure for women with lifelong vaginismus: A randomized waiting-list control trial of efficacy. J. Consult. Clin. Psychol. 2013, 81, 1127–1136. [Google Scholar] [CrossRef]
- Van Lankveld, J.J.; Granot, M.; Schultz, W.C.W.; Binik, Y.M.; Wesselmann, U.; Pukall, C.F.; Bohm-Starke, N.; Achtrari, C. Women’s sexual pain disorders. J. Sex. Med. 2010, 7, 615–631. [Google Scholar] [CrossRef]
- Brotto, L.; Atallah, S.; Johnson-Agbakwu, C.; Rosenbaum, T.; Abdo, C.; Byers, E.S.; Graham, C.A.; Nobre, P.; Wylie, K. Psychological and interpersonal dimensions of sexual function and dysfunction. J. Sex. Med. 2016, 13, 538–571. [Google Scholar] [CrossRef] [PubMed]
- Kleinplatz, P.J.; Charest, M.; Paradis, N.; Ellis, M.; Rosen, L.; Ménard, A.D.; Ramsay, T.O. Treatment of low sexual desire or frequency using a sexual enhancement group couples therapy approach. J. Sex. Med. 2020, 17, 1288–1296. [Google Scholar] [CrossRef] [PubMed]
- Ludgate, J.; Grubr, T. The CBT Couples Toolbox: Over 45 Exercises to Improve Communication, Navigate Problems and Build Strong Relationships; Pesi Publishing & Media: Eau Claire, WI, USA, 2018. [Google Scholar]
- Christensen, A.; Doss, B.D.; Jacobson, N.S. Integrative Behavioral Couple Therapy: A Therapist’s Guide to Creating Acceptance and Change, 2nd ed.; W. W. Norton & Company: New York, NY, USA, 2020. [Google Scholar]
- Connie, E. The Solution Focused Marriage: 5 Simple Habits That Will Bring Out the Best in Your Relationship; The Connie Institute: Keller, TX, USA, 2013. [Google Scholar]
- Olson-Sigg, A.; Olson, D.H. Prepare/Enrich program for premarital and married couples. In Case Studies in Couples Therapy: Theory-Based Approaches; Carson, D., Casado-Kehoe, M., Eds.; Taylor & Francis Group: New York, NY, USA; Routledge: London, UK, 2011; pp. 1–12. [Google Scholar]
- Hawkins, P.; Ryde, J. Integrative Psychotherapy in Theory and Practice; Jessica Kingsley Publishers: Philadelphia, PA, USA, 2019. [Google Scholar]
- Norcross, J.C.; Cooper, M. Personalizing Psychotherapy: Assessing and Accommodating Patient Preferences, 1st ed.; APA Books; American Psychological Association: Washington, DC, USA, 2021. [Google Scholar]
- Kornspan, A.S. History of sport and performance psychology. In The Oxford Handbook of Sport and Performance Psychology; Murphy, S.M., Ed.; Oxford University Press: Oxford, UK, 2012; pp. 3–23. [Google Scholar]
- Williams, J.; Straub, W.F. Sport psychology: Past, present, and future. In Applied Sport Psychology: Personal Growth to Peak Performance; Williams, J.M., Ed.; McGraw-Hill: New York, NY, USA, 2010; pp. 2–11. [Google Scholar]
- Greenspan, M.J.; Feltz, D.L. Psychological interventions with athletes in competitive situations: A review. Sport Psychol. 1989, 3, 219–236. [Google Scholar] [CrossRef]
- Mesagno, C.; Hill, D.M. Definition of choking in sport: Reconceptualisation and debate. Int. J. Sport Psychol. 2014, 44, 267–277. [Google Scholar]
- Marchant, D.B. Anxiety. In Routledge Handbook of Applied Sport Psychology: A Comprehensive Guide for Students and Practitioners; Hanrahan, S.B., Andersen, M.B., Eds.; Routledge: New York, NY, USA, 2020; pp. 260–269. [Google Scholar]
- Shapiro, J.L.; Bartlett, M. Arousal, stress, and anxiety in sport, exercise, and performance: Concepts and management strategies. In Sport, Exercise and Performance Psychology: Theories and Applications; Mugford, A., Gualberto Cremades, J., Eds.; Routledge: New York, NY, USA, 2019; pp. 88–109. [Google Scholar]
- Nieuwenhuys, A.; Oudejans, R.R.D. Anxiety and perceptual-motor performance: Toward an integrated model of concepts, mechanisms, and processes. Psychol. Res. 2011, 76, 747–759. [Google Scholar] [CrossRef] [Green Version]
- Oudejans, R.R.D.; Pijpers, R. Training with anxiety has a positive effect on expert perceptual–motor performance under pressure. Q. J. Exp. Psychol. 2009, 62, 1631–1647. [Google Scholar] [CrossRef]
- Oudejans, R.R.; Pijpers, R. Training with mild anxiety may prevent choking under higher levels of anxiety. Psychol. Sport Exerc. 2010, 11, 44–50. [Google Scholar] [CrossRef]
- Hill, D.; Hanton, S.; Matthews, N.; Fleming, S. A qualitative exploration of choking in elite golf. J. Clin. Sport Psychol. 2010, 4, 221–240. [Google Scholar] [CrossRef] [Green Version]
- Hill, D.M.; Hanton, S.; Matthews, N.; Fleming, S. Choking in sport: A review. Int. Rev. Sport Exerc. Psychol. 2010, 3, 24–39. [Google Scholar] [CrossRef]
- Hill, A.P.; Hall, H.K.; Appleton, P.R. The relationship between multidimensional perfectionism and contingencies of self-worth. Pers. Individ. Differ. 2011, 50, 238–242. [Google Scholar] [CrossRef]
- Hill, D.; Shaw, G. A qualitative examination of choking under pressure in team sport. Psychol. Sport Exerc. 2013, 14, 103–110. [Google Scholar] [CrossRef]
- Karageorghis, C.I.; Terry, P.C. Inside Sport Psychology; Human Kinetics: Champaign, IL, USA, 2011. [Google Scholar]
- Gucciardi, D.; Longbottom, J.-L.; Jackson, B.; Dimmock, J. Experienced golfers’ perspectives on choking under pressure. J. Sport Exerc. Psychol. 2010, 32, 61–83. [Google Scholar] [CrossRef]
- Vealey, R.S.; Low, W.; Pierce, S.; Quinones-Paredes, D. Choking in sport: ACT on it! J. Sport Psychol. Action 2014, 5, 156–169. [Google Scholar] [CrossRef]
- Mesagno, C.; Marchant, D.; Morris, T. A pre-performance routine to alleviate choking in “choking-susceptible” athletes. Sport Psychol. 2008, 22, 439–457. [Google Scholar] [CrossRef]
- Weiss, S.M.; Reber, A.S. Curing the dreaded “steve blass disease”. J. Sport Psychol. Action 2012, 3, 171–181. [Google Scholar] [CrossRef]
- Smith, R.E.; Smoll, F.L.; Cumming, S.P. Effects of a motivational climate intervention for coaches on young athletes’ sport performance anxiety. J. Sport Exerc. Psychol. 2007, 29, 39–59. [Google Scholar] [CrossRef] [PubMed]
- Reeves, J.L.; Tenenbaum, G.; Lidor, R. Choking in front of the Goal: The effects of self-consciousness training. Int. J. Sport Exerc. Psychol. 2007, 5, 240–254. [Google Scholar] [CrossRef]
- Gucciardi, D.; Dimmock, J. Choking under pressure in sensorimotor skills: Conscious processing or depleted attentional resources? Psychol. Sport Exerc. 2008, 9, 45–59. [Google Scholar] [CrossRef]
- Hatzigeorgiadis, A.; Biddle, S. J H. Negative self-talk during sport performance: Relationships with pre-competition anxiety and goal performance discrepancies. J. Sport Behav. 2008, 31, 237–253. [Google Scholar]
- Besharat, M.A.; Pourbohlool, S. Moderating effects of self-confidence and sport self-efficacy on the relationship between competitive anxiety and sport performance. Psychology 2011, 2, 760–765. [Google Scholar] [CrossRef] [Green Version]
- Neil, R.; Wilson, K.; Mellalieu, S.D.; Hanton, S.; Taylor, J. Competitive anxiety intensity and interpretation: A two-study investigation into their relationship with performance. Int. J. Sport Exerc. Psychol. 2012, 10, 96–111. [Google Scholar] [CrossRef]
- Mesagno, C.; Marchant, D. Characteristics of polar opposites: An exploratory investigation of choking-resistant and choking-susceptible athletes. J. Appl. Sport Psychol. 2013, 25, 72–91. [Google Scholar] [CrossRef]
- McCarthy, P.J. Positive emotion in sport performance: Current status and future directions. Int. Rev. Sport Exerc. Psychol. 2011, 4, 50–69. [Google Scholar] [CrossRef]
- Vine, S.; Wilson, M. Quiet eye training: Effects on learning and performance under pressure. J. Appl. Sport Psychol. 2010, 22, 361–376. [Google Scholar] [CrossRef] [Green Version]
- Wood, G.; Wilson, M.R. Quiet-eye training, perceived control and performing under pressure. Psychol. Sport Exerc. 2012, 13, 721–728. [Google Scholar] [CrossRef]
- Mesagno, C.; Geukes, K.; Larkin, P. Choking under pressure: A review of current debates, literature, and interventions. In Contemporary Advances in Sport Psychology: A Review; Mellalieu, S.D., Hanton, S., Eds.; Routledge: New York, NY, USA, 2015; pp. 148–174. [Google Scholar]
- Ivtzan, I.; Hart, R.; Moore, Z.E.; Jackson, S.; Fatemi, S.M.; Ward, E.D.; Langer, E.J.; Gardner, F.L.; Kaufman, K.A.; Glass, C.R.; et al. Mindfulness and Performance; Cambridge University Press: Cambridge, UK, 2015. [Google Scholar]
- Hamilton, L.H. The Person Behind the Mask: A Guide to Performing Arts Psychology; Ablex: New York, NY, USA, 1997. [Google Scholar]
- Hamilton, L.H. Advice for Dancers: Emotional Counsel and Practical Strategies; Jossey-Bass Publishers: San Francisco, CA, USA, 1998. [Google Scholar]
- Emmons, S.; Thomas, A. Power Performance for Singers: Transcending the Barriers; Oxford University Press: Oxford, UK, 1998. [Google Scholar]
- Green, B.; Gallwey, W.T. The Inner Game of Music; Anchor: Palatine, IL, USA, 1986. [Google Scholar]
- Greene, D. Audition Success; Routledge: New York, NY, USA, 2001. [Google Scholar]
- Taylor, J.; Taylor, C. Psychology of Dance; Human Kinetics: Champaign, IL, USA, 1995. [Google Scholar]
- Hays, K.F. The enhancement of performance excellence among performing artists. J. Appl. Sport Psychol. 2002, 14, 299–312. [Google Scholar] [CrossRef]
- Hays, K.F. Being fit: The ethics of practice diversification in performance psychology. Prof. Psychol. Res. Pr. 2006, 37, 223–232. [Google Scholar] [CrossRef]
- Hays, K.F. The psychology of performance in sport and other domains. In The Oxford Handbook of Sport and Performance Psychology; Murphy, S., Ed.; Oxford University Press: Oxford, UK, 2012; pp. 24–45. [Google Scholar]
- Hays, K.F. Performance psychology with performing artists. In Oxford Research Encyclopedia of Psychology; Oxford University Press: Oxford, UK, 2017. [Google Scholar]
- Hays, K.F.; Brown, C.H. You’re on! Consulting for Peak Performance; American Psychological Association: Washington, DC, USA, 2004. [Google Scholar]
- Hays, K.F. Performance anxiety. In Performance Psychology in Action: A Casebook for Working with Athletes, Performing Artists, Business Leaders, and Professionals in High-Risk Occupations; Hays, K.F., Ed.; American Psychological Association: Washington, DC, USA, 2009; pp. 101–120. [Google Scholar]
- Barrell, G.M.; Terry, P. Trait anxiety and coping strategies among ballet dancers. Med. Probl. Perform. Artist. 2003, 18, 59–64. [Google Scholar] [CrossRef]
- Klickstein, G. Musician’s Way: A Guide to Practice, Performance, and Wellness; Oxford University Press: Oxford, UK, 2009. [Google Scholar]
- Nordin-Bates, S.M. Performance psychology in the performing arts. In The Oxford Handbook of Sport and Performance Psychology; Murphy, S., Ed.; Oxford University Press: Oxford, UK, 2012; pp. 24–45. [Google Scholar]
- Osborne, M.; Franklin, J. Cognitive processes in music performance anxiety. Aust. J. Psychol. 2002, 54, 86–93. [Google Scholar] [CrossRef]
- Ryan, C. Gender differences in children’s experience of musical performance anxiety. Psychol. Music. 2004, 32, 89–103. [Google Scholar] [CrossRef]
- Walker, I.J.; Nordin-Bates, S.J. Performance anxiety experiences of professional dancers: The importance of control. J. Dance Med. Sci. 2010, 14, 133–145. [Google Scholar] [PubMed]
- Sadler, M.E.; Miller, C.J. Performance anxiety. Soc. Psychol. Pers. Sci. 2010, 1, 280–287. [Google Scholar] [CrossRef]
- Osborne, M.S.; Greene, D.J.; Immel, D.T. Managing performance anxiety and improving mental skills in conservatoire students through performance psychology training: A pilot study. Psychol. Well-Being 2014, 4, 18. [Google Scholar] [CrossRef] [Green Version]
- Moyle, G.M. Supervision in performance settings (dance, music, acting). In Oxford Research Encyclopedia of Psychology; Oxford University Press: Oxford, UK, 2019; pp. 1–17. [Google Scholar]
- Taylor, J.; Estanol, E. Dance Psychology for Artistic and Performance Excellence; Human Kinetics: Champaign, IL, USA, 2015. [Google Scholar]
- Kenny, D.T. Music performance anxiety: Origins, phenomenology, assessment, and treatment. J. Mus. Res. 2006, 31, 51–64. [Google Scholar]
- Schulman, M. Confidence techniques for clinical practice: Anti-anxiety procedures developed in an acting class. Behav. Ther. 2009, 32, 182–185. [Google Scholar]
- Finn, A.N.; Sawyer, C.R.; Behnke, R.R. A model of anxious arousal for public speaking. Commun. Educ. 2009, 58, 417–432. [Google Scholar] [CrossRef]
- Kim, Y. The effect of improvisation-assisted desensitization, and music-assisted progressive muscle relaxation and imagery on reducing pianists’ music performance anxiety. J. Music. Ther. 2008, 45, 165–191. [Google Scholar] [CrossRef] [PubMed]
- Sawyer, C.R.; Behnke, R.R. Behavioral inhibition and the communication of public speaking state anxiety. West. J. Commun. 2002, 66, 412–422. [Google Scholar] [CrossRef]
- Khalsa, S.B.S.; Butzer, B.; Shorter, S.M.; Reinhardt, K.M.; Cope, S. Yoga reduces performance anxiety in adolescent musicians. Altern. Ther. Health Med. 2013, 19, 34–45. [Google Scholar]
- Kaufman, K.A.; Glass, C.R.; Pineau, T.R. Mindful Sport Performance Enhancement: Mental Training for Athletes and Coaches; American Psychological Association: Washington, DC, USA, 2018. [Google Scholar]
- Gallucci, N.T. Sport Psychology: Performance Enhancement, Performance Inhibition, Individuals, and Teams, 2nd ed; Psychology Press: East Sussex, UK, 2014. [Google Scholar]
- Moyle, G.M. Skating on Olympic ice: Working with winter Olympians. Int. J. Sport Exerc. Psychol. 2014, 13, 56–73. [Google Scholar] [CrossRef]
- Moyle, G.M. Coaching performing artists. Consult. Psychol. J. Pr. Res. 2019, 71, 97–106. [Google Scholar] [CrossRef]
- Davis, J.P.; Palitz, S.A.; Knepley, M.J.; Kendall, P.C. Cognitive-behavioral therapy with youth. In Handbook of Cognitive-Behavioral Therapies; Dobson, K.S., Dozois, D.J.A., Eds.; The Guilford Press: New York, NY, USA, 2019; pp. 349–382. [Google Scholar]
- Kaiser, R.B. Stargazing: Everyday lessons from coaching elite performers. Consult. Psychol. J. Pr. Res. 2019, 71, 130–139. [Google Scholar] [CrossRef]
- Ritvo, E.C.; Glick, I.D. Family problems and sports performance. Physician Sportsmed. 2005, 33, 37–41. [Google Scholar] [CrossRef]
- Cruickshank, A.; Collins, D.; Minten, S. Driving and sustaining culture change in olympic sport performance teams: A first exploration and grounded theory. J. Sport Exerc. Psychol. 2014, 36, 107–120. [Google Scholar] [CrossRef] [Green Version]
- Hodge, K. Working at the Olympics. In Routledge Handbook of Applied Sport Psychology; Hanrahan, S.J., Andersen, M.B., Eds.; Routledge: New York, NY, USA, 2010; pp. 405–413. [Google Scholar]
- Cotterill, S.T.; Fransen, K. Athlete leadership in sport teams: Current understanding and future directions. Int. Rev. Sport Exerc. Psychol. 2016, 9, 116–133. [Google Scholar] [CrossRef] [Green Version]
- Bekar, C.; Carlaw, K.; Lipsey, R. General purpose technologies in theory, application and controversy: A review. J. Evol. Econ. 2017, 28, 1005–1033. [Google Scholar] [CrossRef]
- Yerkes, R.M.; Dodson, J.D. The relation of strength of stimulus to rapidity of habit-formation. J. Comp. Neurol. Psychol. 1908, 18, 459–482. [Google Scholar] [CrossRef] [Green Version]
- Teigen, K.H. Yerkes-Dodson: A law for all seasons. Theory Psychol. 1994, 4, 525–547. [Google Scholar] [CrossRef]
- Heiman, J.R.; Rowland, D.L. Affective and physiological sexual response patterns: The effects of instructions on sexually functional and dysfunctional men. J. Psychosom. Res. 1983, 27, 105–116. [Google Scholar] [CrossRef]
- Otten, M. Choking vs. clutch performance: A study of sport performance under pressure. J. Sport Exerc. Psychol. 2009, 31, 583–601. [Google Scholar] [CrossRef] [Green Version]
- Corbett, M. From law to folklore: Work stress and the Yerkes-Dodson Law. J. Manag. Psychol. 2015, 30, 741–752. [Google Scholar] [CrossRef]
- Hanoch, Y.; Vitouch, O. When less is more. Theory Psychol. 2004, 14, 427–452. [Google Scholar] [CrossRef]
- Ouimet, A.J. Integrating the reflective-impulsive model with cognitive-behavioral therapy for anxiety disorders. In Reflective and Impulsive Determinants of Human Behavior; Deutsch, R., Gawronski, B., Hofmann, W., Eds.; Taylor & Francis Group: New York, NY, USA; Routledge: London, UK, 2017; pp. 189–204. [Google Scholar]
- Evans, J.T.; Stanovich, K.E. Dual-process theories of higher cognition: Advancing the debate. Perspect. Psychol. Sci. 2013, 8, 223–241. [Google Scholar] [CrossRef]
- Newell, B.R.; Shanks, D.R. Unconscious influences on decision making: A critical review. Behav. Brain Sci. 2014, 37, 1–19. [Google Scholar] [CrossRef] [Green Version]
- Hofmann, W.; Friese, M.; Strack, F. Impulse and self-control from a dual-systems perspective. Perspect. Psychol. Sci. 2009, 4, 162–176. [Google Scholar] [CrossRef] [PubMed]
- Simon, H.A. Motivational and emotional controls of cognition. Psychol. Rev. 1967, 74, 29–39. [Google Scholar] [CrossRef] [PubMed]
- Phelps, E.A.; Ling, S.; Carrasco, M. Emotion facilitates perception and potentiates the perceptual benefits of attention. Psychol. Sci. 2006, 17, 292–299. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Domain | Sex | Sport | Stage |
|---|---|---|---|
| Shared Interventions | |||
| Cognitive | Reframing; positive self-talk; identifying and replacing faulty beliefs/coping; maintaining focus on relevant stimuli; improving attitude, self-efficacy, confidence. | Reframing; restructuring; positive self-talk; moderating expectations; thinking more productively; trust monitoring; attentional control; dual task training; coaching-led intervention. | Reframing; positive self-talk; problem focused coping strategies; positive self-efficacy; task related and emotion focused coping; modifying view of risk. |
| Mindfulness | Non-judgmental focus on thoughts, reactions, and emotions; relaxation; deep breathing; sensate focus—awareness of body sensation; reduce performance demand. | Use of mental images to relax; employing other relaxation techniques; quiet eye training. | Imagery; relaxation; breathing; being in the moment; yoga exercises and meditation; stress reduction. |
| Emotion-focused | Increasing emotional awareness and regulation; reducing focus on fear/anxiety; replacing negative with positive emotion; productive channeling. | Adapting to pressure; performing under pressure; facilitative anxiety interpretation; countering negative self-talk. | Countering anxious habits; systematic desensitization; imagery; reinterpreting anxiety as facilitative. |
| Behavioral | Re-conditioning; altering stimuli and modifying responses; regulating arousal through use of stimuli. | Preparation; quiet eye training; pre-shot routines; controlling the controllables; mental/physical pre-performance routines; performing under pressure. | Practice strategies; rehearsal, controlling the controllables; using confidence stimulus; changing problematic behaviors stemming from anxiety. |
| General lifestyle/perspective | Emphasis on reducing lifestyle factors that increase risk of sexual problem (e.g., smoking). Expanding identity beyond sexual self. | Emphasis on healthy lifestyle; nutrition; proper care of body; self-regulation; energy management. Expanding identity beyond athlete. | Emphasis on healthy lifestyle, nutrition, proper care of body; self-regulation; energy management. Expanding identity beyond performer. |
| Related or Secondary Approaches | |||
| Couples/team approaches | Diminishing evaluative component; couple working as a team; shared problem-solving; removing shame. | Developing high performance teams; culture of helping; shared problem solving and goal setting. | Using peer social support; developing shared strategies with colleagues; culture of helping; shared problem solving and goal setting. |
| Personality traits/dispositions | Mitigating negative traits and dispositions with cognitive approaches designed to counter perfectionism, lack of confidence, high self-consciousness, etc. | Mitigating negative traits and dispositions with cognitive approaches designed to counter perfectionism, lack of confidence, high self-consciousness, etc. | Mitigating negative traits and dispositions with cognitive approaches designed to counter perfectionism, lack of confidence, high self-consciousness, etc. |
| Domain-Specific Strategies | |||
| Physio-pharmacological | Increasing or decreasing autonomic motor response via medication. | Using medication to alleviate autonomic symptoms thereby reducing anxiety triggers. | |
| Preparation/practice | Pre-performance routines; rehearsals and practice; controlling the controllables. | Pre-performance routines; rehearsals and practice; controlling the controllables | |
| Specific behavioral approaches | Using biofeedback and feedback from teammates and coach/director; reprogramming and correction of responses. | Using feedback from teammates and coach/director; reprogramming and correction of responses. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rowland, D.L.; Moyle, G.; Cooper, S.E. Remediation Strategies for Performance Anxiety across Sex, Sport and Stage: Identifying Common Approaches and a Unified Cognitive Model. Int. J. Environ. Res. Public Health 2021, 18, 10160. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph181910160
Rowland DL, Moyle G, Cooper SE. Remediation Strategies for Performance Anxiety across Sex, Sport and Stage: Identifying Common Approaches and a Unified Cognitive Model. International Journal of Environmental Research and Public Health. 2021; 18(19):10160. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph181910160
Chicago/Turabian StyleRowland, David L., Gene Moyle, and Stewart E. Cooper. 2021. "Remediation Strategies for Performance Anxiety across Sex, Sport and Stage: Identifying Common Approaches and a Unified Cognitive Model" International Journal of Environmental Research and Public Health 18, no. 19: 10160. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph181910160