
Analysis of Fractal Correlation Properties of Heart Rate Variability during an Initial Session of Eccentric Cycling




Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Baseline Assessment
2.3. Eccentric and Concentric Cycling Exercise Sessions
2.4. RR Measurements and Calculation of DFA a1
2.5. Blood Pressure and Biochemical Measurements
2.6. Statistics
3. Results
4. Discussion
5. Limitations and Future Directions
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Barreto, R.V.; de Lima, L.C.R.; Denadai, B.S. Moving forward with backward pedaling: A review on eccentric cycling. Eur. J. Appl. Physiol. 2021, 121, 381–407. [Google Scholar] [CrossRef] [PubMed]
- Peñailillo, L.; Blazevich, A.J.; Nosaka, K. Factors contributing to lower metabolic demand of eccentric compared with concentric cycling. J. Appl. Physiol. 1985, 123, 884–893. [Google Scholar] [CrossRef]
- Douglas, J.; Pearson, S.; Ross, A.; McGuigan, M. Eccentric Exercise: Physiological Characteristics and Acute Responses. Sports Med. 2017, 47, 663–675. [Google Scholar] [CrossRef]
- Gremeaux, V.; Duclay, J.; Deley, G.; Philipp, J.L.; Laroche, D.; Pousson, M.; Casillas, J.M. Does eccentric endurance training improve walking capacity in patients with coronary artery disease? A randomized controlled pilot study. Clin. Rehabil. 2010, 24, 590–599. [Google Scholar] [CrossRef] [PubMed]
- Touron, J.; Costes, F.; Coudeyre, E.; Perrault, H.; Richard, R. Aerobic Metabolic Adaptations in Endurance Eccentric Exercise and Training: From Whole Body to Mitochondria. Front. Physiol. 2020, 11, 596351. [Google Scholar] [CrossRef] [PubMed]
- Julian, V.; Thivel, D.; Costes, F.; Touron, J.; Boirie, Y.; Pereira, B.; Perrault, H.; Duclos, M.; Richard, R. Eccentric Training Improves Body Composition by Inducing Mechanical and Metabolic Adaptations: A Promising Approach for Overweight and Obese Individuals. Front. Physiol. 2018, 9, 1013. [Google Scholar] [CrossRef] [PubMed]
- Paulsen, G.; Eidsheim, H.Ø.; Helland, C.; Seynnes, O.; Solberg, P.A.; Rønnestad, B.R. Eccentric cycling does not improve cycling performance in amateur cyclists. PLoS ONE 2019, 14, e0208452. [Google Scholar] [CrossRef] [PubMed]
- Ritter, O.; Isacco, L.; Rakobowchuk, M.; Tordi, N.; Laroche, D.; Bouhaddi, M.; Degano, B.; Mourot, L. Cardiorespiratory and Autonomic Nervous System Responses to Prolonged Eccentric Cycling. Int. J. Sports Med. 2019, 40, 453–461. [Google Scholar] [CrossRef] [PubMed]
- Michael, S.; Graham, K.S.; Davis, G.M. Cardiac Autonomic Responses during Exercise and Post-exercise Recovery Using Heart Rate Variability and Systolic Time Intervals-A Review. Front. Physiol. 2017, 8, 301. [Google Scholar] [CrossRef] [Green Version]
- Gronwald, T.; Rogers, B.; Hoos, O. Fractal Correlation Properties of Heart Rate Variability: A New Biomarker for Intensity Distribution in Endurance Exercise and Training Prescription? Front. Physiol. 2020, 11, 550572. [Google Scholar] [CrossRef]
- Rogers, B.; Giles, D.; Draper, N.; Hoos, O.; Gronwald, T. A New Detection Method Defining the Aerobic Threshold for Endurance Exercise and Training Prescription Based on Fractal Correlation Properties of Heart Rate Variability. Front. Physiol. 2021, 11, 596567. [Google Scholar] [CrossRef] [PubMed]
- Rogers, B.; Giles, D.; Draper, N.; Mourot, L.; Gronwald, T. Detection of the Anaerobic Threshold in Endurance Sports: Validation of a New Method Using Correlation Properties of Heart Rate Variability. J. Funct. Morphol. Kinesiology. 2021, 6, 38. [Google Scholar] [CrossRef] [PubMed]
- Hardstone, R.; Poil, S.S.; Schiavone, G.; Jansen, R.; Nikulin, V.V.; Mansvelder, H.D.; Linkenkaer-Hansen, K. Detrended fluctuation analysis: A scale-free view on neuronal oscillations. Front. Physiol. 2012, 3, 450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balagué, N.; Hristovski, R.; Almarcha, M.; Garcia-Retortillo, S.; Ivanov, P.C. Network Physiology of Exercise: Vision and Perspectives. Front. Physiol. 2020, 11, 611550. [Google Scholar] [CrossRef] [PubMed]
- Rogers, B.; Mourot, L.; Gronwald, T. Ventilatory Threshold Identification in A Cardiac Disease Population Based On Fractal Correlation Properties Of HRV. Med. Sci. Sports Exerc. 2021, 53, 438. [Google Scholar] [CrossRef]
- White, D.W.; Raven, P.B. Autonomic neural control of heart rate during dynamic exercise: Revisited. J. Physiol. 2014, 592, 2491–2500. [Google Scholar] [CrossRef] [PubMed]
- Gaskill, S.E.; Ruby, B.C.; Walker, A.J.; Sanchez, O.A.; Serfass, R.C.; Leon, A.S. Validity and reliability of combining three methods to determine ventilatory threshold. Med. Sci. Sports. Exerc. 2001, 33, 1841–1848. [Google Scholar] [CrossRef]
- Peñailillo, L.; Blazevich, A.; Numazawa, H.; Nosaka, K. Metabolic and muscle damage profiles of concentric versus repeated eccentric cycling. Med. Sci. Sports Exerc. 2013, 45, 1773–1781. [Google Scholar] [CrossRef]
- LaStayo, P.C.; Pierotti, D.J.; Pifer, J.; Hoppeler, H.; Lindstedt, S.L. Eccentric ergometry: Increases in locomotor muscle size and strength at low training intensities. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2000, 278, R1282–R1288. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tarvainen, M.P.; Niskanen, J.P.; Lipponen, J.A.; Ranta-Aho, P.O.; Karjalainen, P.A. Kubios HRV–heart rate variability analysis software. Comput. Methods Progr. Biomed. 2014, 113, 210–220. [Google Scholar] [CrossRef]
- Lipponen, J.A.; Tarvainen, M.P. A robust algorithm for heart rate variability time series artefact correction using novel beat classification. J. Med. Eng. Technol. 2019, 43, 173–181. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Ivanov, P.C.; Hu, K.; Stanley, H.E. Effect of nonstationarities on detrended fluctuation analysis. Phys. Rev. E 2002, 65, 041107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rogers, B.; Giles, D.; Draper, N.; Mourot, L.; Gronwald, T. Influence of Artefact Correction and Recording Device Type on the Practical Application of a Non-Linear Heart Rate Variability Biomarker for Aerobic Threshold Determination. Sensors 2021, 21, 821. [Google Scholar] [CrossRef] [PubMed]
- Chan, Y.H. Biostatistics 104: Correlational analysis. Singap. Med. J. 2003, 44, 614–619. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioural Sciences; Erlbaum: Hillsdale, MI, USA, 1988. [Google Scholar]
- Pageaux, B.; Besson, D.; Casillas, J.M.; Lepers, R.; Gremeaux, V.; Ornetti, P.; Gouteron, A.; Laroche, D. Progressively increasing the intensity of eccentric cycling over four training sessions: A feasibility study in coronary heart disease patients. Ann. Phys. Rehabil. Med. 2020, 63, 241–244. [Google Scholar] [CrossRef]
- Mezzani, A.; Hamm, L.F.; Jones, A.M.; McBride, P.E.; Moholdt, T.; Stone, J.A.; Urhausen, A.; Williams, M.A.; European Association for Cardiovascular Prevention and Rehabilitation; American Association of Cardiovascular and Pulmonary Rehabilitation; et al. Aerobic exercise intensity assessment and prescription in cardiac rehabilitation: A joint position statement of the European Association for Cardiovascular Prevention and Rehabilitation, the American Association of Cardiovascular and Pulmonary Rehabilitation and the Canadian Association of Cardiac R. Eur. J. Prev. Cardiol. 2013, 20, 442–467. [Google Scholar] [PubMed]
- Anselmi, F.; Cavigli, L.; Pagliaro, A.; Valente, S.; Valentini, F.; Cameli, M.; Focardi, M.; Mochi, N.; Dendale, P.; Hansen, D.; et al. The importance of ventilatory thresholds to define aerobic exercise intensity in cardiac patients and healthy subjects. Scand. J. Med. Sci. Sports 2021, 31, 1796–1808. [Google Scholar] [CrossRef]
- Jamnick, N.A.; Pettitt, R.W.; Granata, C.; Pyne, D.B.; Bishop, D.J. An Examination and Critique of Current Methods to Determine Exercise Intensity. Sports Med. 2020, 50, 1729–1756. [Google Scholar] [CrossRef]
- Chou, T.H.; Akins, J.D.; Crawford, C.K.; Allen, J.R.; Coyle, E.F. Low Stroke Volume during Exercise with Hot Skin Is Due to Elevated Heart Rate. Med. Sci. Sports Exerc. 2019, 51, 2025–2032. [Google Scholar] [CrossRef]
- Eiken, T.; Harrison, A.J.; Burdon, C.A.; Groeller, H.; Peoples, G.E. Elevated body temperature contributes to the increased heart rate response during eccentric compared to concentric cycling when matched for oxygen consumption. Temperature 2020, 8, 30–38. [Google Scholar] [CrossRef]
- Gronwald, T.; Berk, S.; Altini, M.; Mourot, L.; Hoos, O.; Rogers, B. Real-Time Estimation of Aerobic Threshold and Exercise Intensity Distribution Using Fractal Correlation Properties of Heart Rate Variability: A Single-Case Field Application in a Former Olympic Triathlete. Front. Sports Act. Living 2021, 3, 668812. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| T10 | T45 | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Participant | HR (bpm) | VO2 (mL/min/kg) | DFA a1 | HR (bpm) | VO2 (mL/min/kg) | DFA a1 | ||||||
| CON | ECC | CON | ECC | CON | ECC | CON | ECC | CON | ECC | CON | ECC | |
| 1 | 105 | 104 | 17.6 | 14.3 | 0.946 | 1.18 | 105 | 93 | 18.3 | 14.0 | 0.854 | 1.053 |
| 2 | 93 | 88 | 18.7 | 15.1 | 1.381 | 1.323 | 97 | 103 | 18.6 | 12.9 | 1.595 | 1.187 |
| 3 | 101 | 120 | 19.5 | 35.9 | 1.537 | 0.722 | 102 | 150 | 21.7 | 20.4 | 1.202 | 0.404 |
| 4 | 107 | 103 | 15.4 | 17.9 | 0.926 | 1.272 | 115 | 146 | 14.4 | 19.4 | 1.109 | 0.736 |
| 5 | 83 | 75 | 17.3 | 12.8 | 1.155 | 1.004 | 90 | 98 | 17.9 | 15.9 | 1.339 | 0.79 |
| 6 | 97 | 115 | 14.9 | 20.0 | 0.761 | 1.083 | 101 | 125 | 14.9 | 19.3 | 0.903 | 0.965 |
| 7 | 100 | 102 | 15.5 | 13.5 | 0.973 | 1.403 | 110 | 119 | 17.2 | 17.6 | 1.076 | 1.077 |
| 8 | 97 | 107 | 20.0 | 19.8 | 1.004 | 0.707 | 100 | 115 | 20.1 | 15.4 | 0.682 | 0.666 |
| 9 | 105 | 90 | 18.4 | 15.1 | 0.856 | 0.81 | 110 | 108 | 19.7 | 14.5 | 0.706 | 0.86 |
| 10 | 118 | 113 | 16.8 | 13.4 | 1.188 | 0.971 | 120 | 123 | 15.4 | 15.6 | 0.804 | 0.795 |
| 11 | 114 | 108 | 13.9 | 9.6 | 0.851 | 1.161 | 122 | 121 | 15.7 | 10.7 | 0.756 | 1.118 |
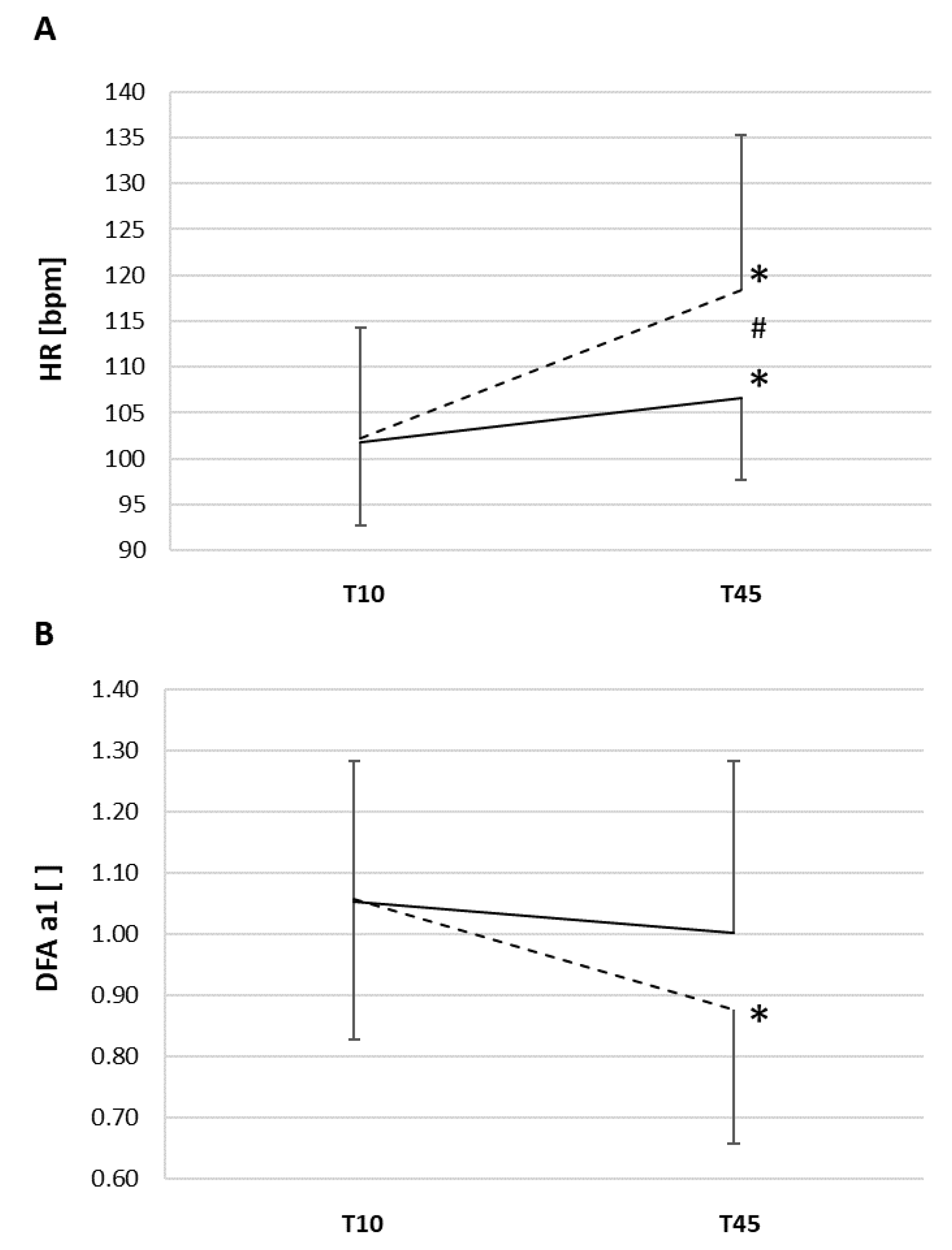
| Mean (±SD) | 102 (±9) | 102 (±13) | 17.1 (±1.9) | 17.0 (±6.7) | 1.053 (±0.228) | 1.058 (±0.228) | 107 (±9) * | 118 (±17) *# | 17.6 (±2.2) | 16.0 (±2.9) | 1.002 (±0.277) | 0.877 (±0.221) * |
| Participant | Norepinephrine (pg/mL) | Serum Lactate (mmol/L) | Systolic BP (mmHg) | Diastolic BP (mmHg) | ||||
|---|---|---|---|---|---|---|---|---|
| CON | ECC | CON | ECC | CON | ECC | CON | ECC | |
| 1 | 715 | 513 | 1.79 | 1.33 | 127 | 141 | 57 | 76 |
| 2 | 696 | 783 | 1.72 | 2.36 | 128 | 143 | 61 | 71 |
| 3 | 580 | 753 | 1.55 | 1.89 | 135 | 115 | 56 | 62 |
| 4 | 820 | 1355 | 2.10 | 2.22 | 121 | 149 | 61 | 85 |
| 5 | 363 | 317 | 1.73 | 1.45 | 144 | 135 | 70 | 65 |
| 6 | 476 | 810 | 1.46 | 2.06 | 186 | 158 | 82 | 78 |
| 7 | 359 | 489 | 1.53 | 1.93 | 148 | 153 | 68 | 81 |
| 8 | 482 | 475 | 1.28 | 1.20 | 118 | 148 | 58 | 80 |
| 9 | 449 | 365 | 2.18 | 1.41 | 147 | 148 | 85 | 84 |
| 10 | 568 | 446 | 1.64 | 1.70 | 129 | 136 | 69 | 74 |
| 11 | 423 | 440 | 1.91 | 1.90 | 140 | 147 | 73 | 86 |
| Mean (±SD) | 539 (±144) | 613 (±284) | 1.72 (±0.26) | 1.77 (±0.36) | 138 (±18) | 143 (±11) | 67 (±9) | 77 (±7) # |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rogers, B.; Gronwald, T.; Mourot, L. Analysis of Fractal Correlation Properties of Heart Rate Variability during an Initial Session of Eccentric Cycling. Int. J. Environ. Res. Public Health 2021, 18, 10426. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph181910426
Rogers B, Gronwald T, Mourot L. Analysis of Fractal Correlation Properties of Heart Rate Variability during an Initial Session of Eccentric Cycling. International Journal of Environmental Research and Public Health. 2021; 18(19):10426. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph181910426
Chicago/Turabian StyleRogers, Bruce, Thomas Gronwald, and Laurent Mourot. 2021. "Analysis of Fractal Correlation Properties of Heart Rate Variability during an Initial Session of Eccentric Cycling" International Journal of Environmental Research and Public Health 18, no. 19: 10426. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph181910426