
Complex Multimorbidity and Incidence of Long-Term Care Needs in Japan: A Prospective Cohort Study


Abstract
:1. Introduction
2. Materials and Methods
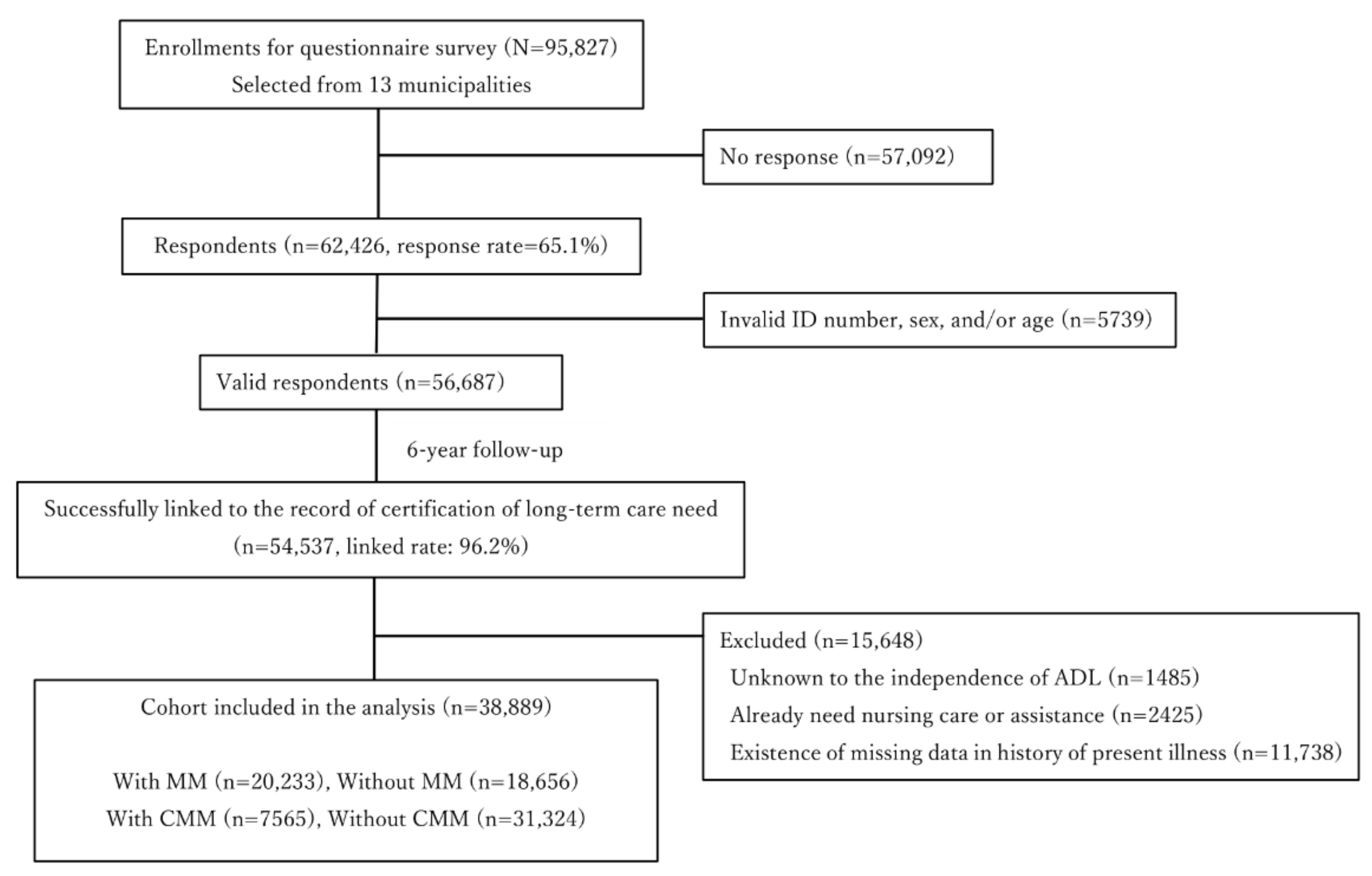
2.1. Study Cohort
2.2. Assessment of MM and CMM
2.3. Endpoint Assessment
2.4. Propensity Score Matching
2.5. Matching
2.6. Inverse Probability of Treatment Weighting (IPTW)
2.7. Statistical Analysis
2.8. Ethical Considerations
3. Results
3.1. Baseline Population Characteristics
3.2. MM Outcome
3.3. CMM Outcome
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Harris, J.R.; Wallace, R.B. The institute of medicine’s new report on living well with chronic illness. Prev. Chronic Dis. 2012, 9, E148. [Google Scholar] [CrossRef] [Green Version]
- Violan, C.; Foguet-Boreu, Q.; Flores-Mateo, G.; Salisbury, C.; Blom, J.; Freitag, M.; Glynn, L.; Muth, C.; Valderas, J.M. Prevalence, determinants and patterns of multimorbidity in primary care: A systematic review of observational studies. PLoS ONE 2014, 9, e102149. [Google Scholar] [CrossRef] [PubMed]
- Chudasama, Y.V.; Khunti, K.K.; Zaccardi, F.; Rowlands, A.V.; Yates, T.; Gillies, C.L.; Davies, M.J.; Dhalwani, N.N. Physical activity, multimorbidity, and life expectancy: A UK biobank longitudinal study. BMC Med. 2019, 17, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Willadsen, T.G.; Bebe, A.; Køster-Rasmussen, R.; Jarbøl, D.E.; Guassora, A.D.; Waldorff, F.B.; Reventlow, S.; Olivarius, N.d.F. The role of diseases, risk factors and symptoms in the definition of multimorbidity—A systematic review. Scand. J. Prim. Health Care 2016, 34, 112–121. [Google Scholar] [CrossRef]
- Harrison, C.; Britt, H.; Miller, G.; Henderson, J. Examining different measures of multimorbidity, using a large prospective cross-sectional study in Australian general practice. BMJ Open 2014, 4, 4694. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harrison, C.; Henderson, J.; Miller, G.; Britt, H. The prevalence of complex multimorbidity in Australia. Aust. N. Z. J. Public Health 2016, 40, 239–244. [Google Scholar] [CrossRef] [Green Version]
- Lujic, S.; Simpson, J.M.; Zwar, N.; Hosseinzadeh, H.; Jorm, L. Multimorbidity in Australia: Comparing estimates derived using administrative data sources and survey data. PLoS ONE 2017, 12, e0183817. [Google Scholar] [CrossRef] [PubMed]
- Tsutsui, T.; Muramatsu, N. Care-needs certification in the long-term care insurance system of Japan. J. Am. Geriatr. Soc. 2005, 53, 522–527. [Google Scholar] [CrossRef]
- Ministry of Health. Summary of insured long-term care service report. 2020. Available online: https://www.mhlw.go.jp/topics/kaigo/osirase/jigyo/m20/dl/2001a.pdf (accessed on 20 April 2021).
- Ministry of Health. Summary of Comprehensive Survey of Living Conditions Report. 2016. Available online: https://www.mhlw.go.jp/toukei/saikin/hw/k-tyosa/k-tyosa16/ (accessed on 20 April 2021).
- Beard, J.R.; Officer, A.; De Carvalho, I.A.; Sadana, R.; Pot, A.M.; Michel, J.P.; Lloyd-Sherlock, P.; Epping-Jordan, J.E.; Peeters, G.M.E.E.; Mahanani, W.R.; et al. The world report on ageing and health: A policy framework for healthy ageing. Lancet 2016, 387, 2145–2154. [Google Scholar] [CrossRef] [Green Version]
- Kondo, K. Progress in aging epidemiology in Japan: The JAGES project. J. Epidemiol. 2016, 26, 331–336. [Google Scholar] [CrossRef] [Green Version]
- Linn, B.S.; Linn, M.W.; Gurel, L. Cumulative illness rating scale—Anvita health wiki. J. Am. Geriatr. Soc. 1968, 16, 622–626. [Google Scholar] [CrossRef]
- Rosenbaum, P.R.; Rubin, D.B. The central role of the propensity score in observational studies for causal effects. Biometrika 1983, 70, 41–55. [Google Scholar] [CrossRef]
- Honaker, J.; King, G.; Blackwell, M. Amelia I,I. A program for missing data. J. Stat. Softw. 2011, 45, 1–47. [Google Scholar] [CrossRef]
- Graham, J.W.; Olchowski, A.E.; Gilreath, T.D. How many imputations are really needed? Some practical clarifications of multiple imputation theory. Prev. Sci. 2007, 8, 206–213. [Google Scholar] [CrossRef] [Green Version]
- Rubin, D.B. Multiple imputation after 18+ years. J. Am. Stat. Assoc. 1996, 91, 473–489. [Google Scholar] [CrossRef]
- Austin, P.C. The Use of propensity score methods with survival or time-to-event outcomes: Reporting measures of effect similar to those used in randomized experiments. Stat. Med. 2014, 33, 1242–1258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Austin, P.C. An introduction to propensity score methods for reducing the effects of confounding in observational studies. Multivar. Behav. Res. 2011, 46, 399–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Austin, P.C. The performance of different propensity score methods for estimating marginal hazard ratios. Stat. Med. 2013, 32, 2837–2849. [Google Scholar] [CrossRef] [Green Version]
- Xu, S.; Ross, C.; Raebel, M.A.; Shetterly, S.; Blanchette, C.; Smith, D. Use of Stabilized inverse propensity scores as weights to directly estimate relative risk and its confidence intervals. Value Health 2010, 13, 273–277. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Westreich, D.; Cole, S.R.; Funk, M.J.; Brookhart, M.A.; Stürmer, T. The role of the c-statistic in variable selection for propensity score models. Pharmacoepidemiol. Drug Saf. 2011, 20, 317–320. [Google Scholar] [CrossRef] [Green Version]
- Xie, J.; Liu, C. Adjusted Kaplan-Meier estimator and log-rank test with inverse probability of treatment weighting for survival data. Stat. Med. 2005, 24, 3089–3110. [Google Scholar] [CrossRef] [PubMed]
- Hirai, H.; Kondo, K.; Ojima, T.; Murata, C. Examination of risk factors for onset of certification of long-term care insurance in community-dwelling older people: AGES Project 3-Year follow-up study. Jpn. J. Public Health 2009, 56, 501–512. [Google Scholar] [CrossRef]
- Jindai, K.; Nielson, C.M.; Vorderstrasse, B.A.; Quiñones, A.R. Multimorbidity and functional limitations among adults 65 or older, NHANES 2005-2012. Prev. Chronic Dis. 2016, 13, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kato, D.; Kawachi, I.; Saito, J.; Kondo., N. Complex multimorbidity and mortality in Japan: A prospective propensity-matched cohort study. BMJ Open 2021, 11, e046749. [Google Scholar] [CrossRef]
- Vinjerui, K.H.; Bjerkeset, O.; Bjorngaard, J.H.; Krokstad, S.; Douglas, K.A.; Sund, E.R.; Vinjerui, K.H.; Bjerkeset, O.; Bjerkeset, O.; Bjorngaard, J.H.; et al. Socioeconomic inequalities in the prevalence of complex multimorbidity in a Norwegian population: Findings from the cross-sectional HUNT Study. BMJ Open 2020, 10, e036851. [Google Scholar] [CrossRef] [PubMed]
- Jankovic, J.; Mirkovic, M.; Jovic-Vranes, A.; Santric-Milicevic, M.; Terzic-Supic, Z. Association between non-communicable disease multimorbidity and health care utilization in a middle-income country: Population-based study. Public Health 2018, 155, 35–42. [Google Scholar] [CrossRef]
- Catalá-López, F.; Alonso-Arroyo, A.; Page, M.J.; Hutton, B.; Tabarés-Seisdedos, R.; Aleixandre-Benavent, R. Mapping of global scientific research in comorbidity and multimorbidity: A cross-sectional analysis. PLoS ONE 2018, 13, 1–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cricelli, C.; Mazzaglia, G.; Samani, F.; Marchi, M.; Sabatini, A.; Nardi, R.; Ventriglia, G.; Caputi, A.P. Prevalence Estimates for chronic diseases in italy: Exploring the differences between self-report and primary care databases. J. Public Health Med. 2003, 25, 254–257. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Category | Disease |
|---|---|
| Circulation disorder | Heart disease (including arrhythmia) |
| Stroke | |
| High blood pressure | |
| Endocrine–metabolic disorder (General system) | Diabetes (including mild-type) |
| Obesity | |
| Dyslipidemia | |
| Eye disorder | Impaired vision |
| Gastrointestinal disorder | Gastrointestinal disease |
| Liver disease | |
| Hearing disorder | Impaired hearing |
| Mental and behavioral disorder | Mental disease |
| Sleep problem | |
| Musculoskeletal and connective disorder | Osteoporosis |
| Joint disease/Neuralgia | |
| Injury/Fracture | |
| Neoplasm | Cancer |
| Respiratory disorder | Respiratory disease |
| Characteristic | SMD b in Multiply Imputed Data | SMD in Matching Data |
|---|---|---|
| Age | 0.24 | 0.002 |
| Sex | 0.099 | 0.001 |
| Previous health check-up | 0.01 | 0.015 |
| The number of natural teeth | 0.11 | 0.019 |
| Consumption of meat and fish | 0.009 | 0.017 |
| Consumption of fruits and vegetables | 0.003 | 0.006 |
| Formal educational year | 0.093 | 0.045 |
| Marital status | 0.072 | 0.015 |
| Someone living with you | 0.06 | 0.033 |
| Residence type | 0.025 | 0.055 |
| Architectural type of home | 0.005 | 0.086 |
| Worries about unexpected expenses | 0.123 | 0.004 |
| Receiving pension | 0.023 | 0.022 |
| Current working status | 0.147 | 0.002 |
| Persons to have meal with | 0.089 | 0.02 |
| Alcohol | 0.107 | 0.015 |
| Smoking | 0.079 | 0.014 |
| Falling over | 0.223 | 0.004 |
| Worriees about falls | 0.266 | 0.001 |
| Going upstairs without support | 0.265 | 0.009 |
| Getting up out of chairs without support | 0.251 | 0.02 |
| Average time walking | 0.16 | <0.001 |
| Frequency of going out | 0.151 | 0.015 |
| Decrease in the frequency of going out | 0.243 | 0.001 |
| Engagement in leisure activities | 0.105 | 0.016 |
| Trust in neighbors | 0.079 | 0.027 |
| Support from neighbors | 0.074 | 0.015 |
| Attachment to residence | 0.053 | 0.036 |
| Contribution to residence | 0.095 | 0.009 |
| Uneasiness about safety in residence | 0.073 | 0.011 |
| Participation in local events | 0.085 | 0.009 |
| Interactions with neighborhood | 0.02 | 0.031 |
| Near to residence | ||
| Locations with graffiti or garbage | 0.009 | 0.02 |
| Parks or foot paths | 0.059 | 0.045 |
| Locations difficult for walking | 0.076 | 0.012 |
| Risky roads or crossroads for traffic accidents | 0.044 | 0.005 |
| Fascinating views or buildings | 0.04 | <0.001 |
| Shops selling fresh fruits and vegetables | 0.074 | 0.023 |
| Dangerous places walking alone at night | 0.013 | 0.019 |
| Comfortable houses or facilities | 0.066 | 0.024 |
| Someone listening to your concerns | 0.019 | 0.01 |
| Someone looking after you in the case of illness | 0.049 | 0.023 |
| Attendance | ||
| Sports group or club | 0.063 | 0.008 |
| Leisure activity group | 0.06 | 0.006 |
| Characteristic | SMD b in Multiply Imputed Data | SMD in Matching Data |
|---|---|---|
| Age | 0.327 | 0.025 |
| Sex | 0.139 | 0.004 |
| Previous health check-up | 0.02 | 0.005 |
| The number of natural teeth | 0.16 | 0.005 |
| Consumption of meat and fish | 0.017 | 0.016 |
| Consumption of fruits and vegetables | 0.035 | 0.012 |
| Formal educational year | 0.151 | 0.004 |
| Marital status | 0.118 | 0.002 |
| Someone living with you | 0.1 | 0.011 |
| Residence type | 0.058 | 0.008 |
| Architectural type of home | 0.02 | 0.006 |
| Worries about unexpected expenses | 0.21 | 0.012 |
| Receiving pension | 0.022 | 0.006 |
| Current working status | 0.225 | 0.004 |
| Persons to have meal with | 0.17 | 0.014 |
| Alcohol | 0.145 | 0.013 |
| Smoking | 0.098 | 0.016 |
| Falling over | 0.307 | 0.013 |
| Worries about falls | 0.396 | 0.005 |
| Going upstairs without support | 0.348 | 0.005 |
| Getting up out of chairs without support | 0.343 | 0.01 |
| Average time walking | 0.203 | 0.001 |
| Frequency of going out | 0.207 | 0.003 |
| Decrease in the frequency of going out | 0.352 | 0.006 |
| Engagement in leisure activities | 0.145 | 0.008 |
| Trust in neighbors | 0.135 | 0.009 |
| Support from neighbors | 0.109 | 0.002 |
| Attachment to residence | 0.086 | 0.002 |
| Contribution to residence | 0.129 | 0.007 |
| Uneasiness about safety in residence | 0.105 | 0.01 |
| Participation in local events | 0.114 | 0.008 |
| Interactions with neighborhood | 0.049 | 0.007 |
| Near to residence | ||
| Locations with graffiti or garbage | 0.019 | 0.014 |
| Parks or foot paths | 0.097 | <0.001 |
| Locations difficult for walking | 0.132 | 0.007 |
| Risky roads or crossroads for traffic accidents | 0.061 | 0.002 |
| Fascinating views or buildings | 0.074 | 0.004 |
| Shops selling fresh fruits and vegetables | 0.091 | 0.001 |
| Dangerous places walking alone at night | 0.016 | <0.001 |
| Comfortable houses or facilities | 0.107 | 0.011 |
| Someone listening to your concerns | 0.075 | 0.007 |
| Someone looking after you in the case of illness | 0.094 | 0.026 |
| Attendance | ||
| Sports group or club | 0.117 | 0.031 |
| Leisure activity group | 0.088 | 0.007 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kato, D.; Kawachi, I.; Saito, J.; Kondo, N. Complex Multimorbidity and Incidence of Long-Term Care Needs in Japan: A Prospective Cohort Study. Int. J. Environ. Res. Public Health 2021, 18, 10523. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph181910523
Kato D, Kawachi I, Saito J, Kondo N. Complex Multimorbidity and Incidence of Long-Term Care Needs in Japan: A Prospective Cohort Study. International Journal of Environmental Research and Public Health. 2021; 18(19):10523. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph181910523
Chicago/Turabian StyleKato, Daisuke, Ichiro Kawachi, Junko Saito, and Naoki Kondo. 2021. "Complex Multimorbidity and Incidence of Long-Term Care Needs in Japan: A Prospective Cohort Study" International Journal of Environmental Research and Public Health 18, no. 19: 10523. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph181910523