
Protocol for the Implementation and Evaluation of a Mindfulness-Based Intervention for Caregivers of Children with Mental Disorders in a Clinical Setting


Abstract
:1. Introduction
1.1. Parenting Children with Mental Health Disorders
1.2. Mindfulness as a Parenting Resource
1.3. The Mindfulness-Based Stress Reduction Program
1.4. Gaps in the Mindfulness-Based Stress Reduction Literature
1.5. Research Objectives
2. Materials and Methods
2.1. Study Design
2.2. Measures
2.2.1. Sociodemographic Profile Measures
2.2.2. Effectiveness Measures
2.2.3. Perceived Impact by the Participants and Implementation Analysis of the Program
2.2.4. Client Satisfaction
2.3. Study Setting
2.4. Participants
2.4.1. Characteristics
2.4.2. Recruitment, Inclusion, and Exclusion Criteria
2.5. Procedure
2.5.1. MBSR-P and Implementation
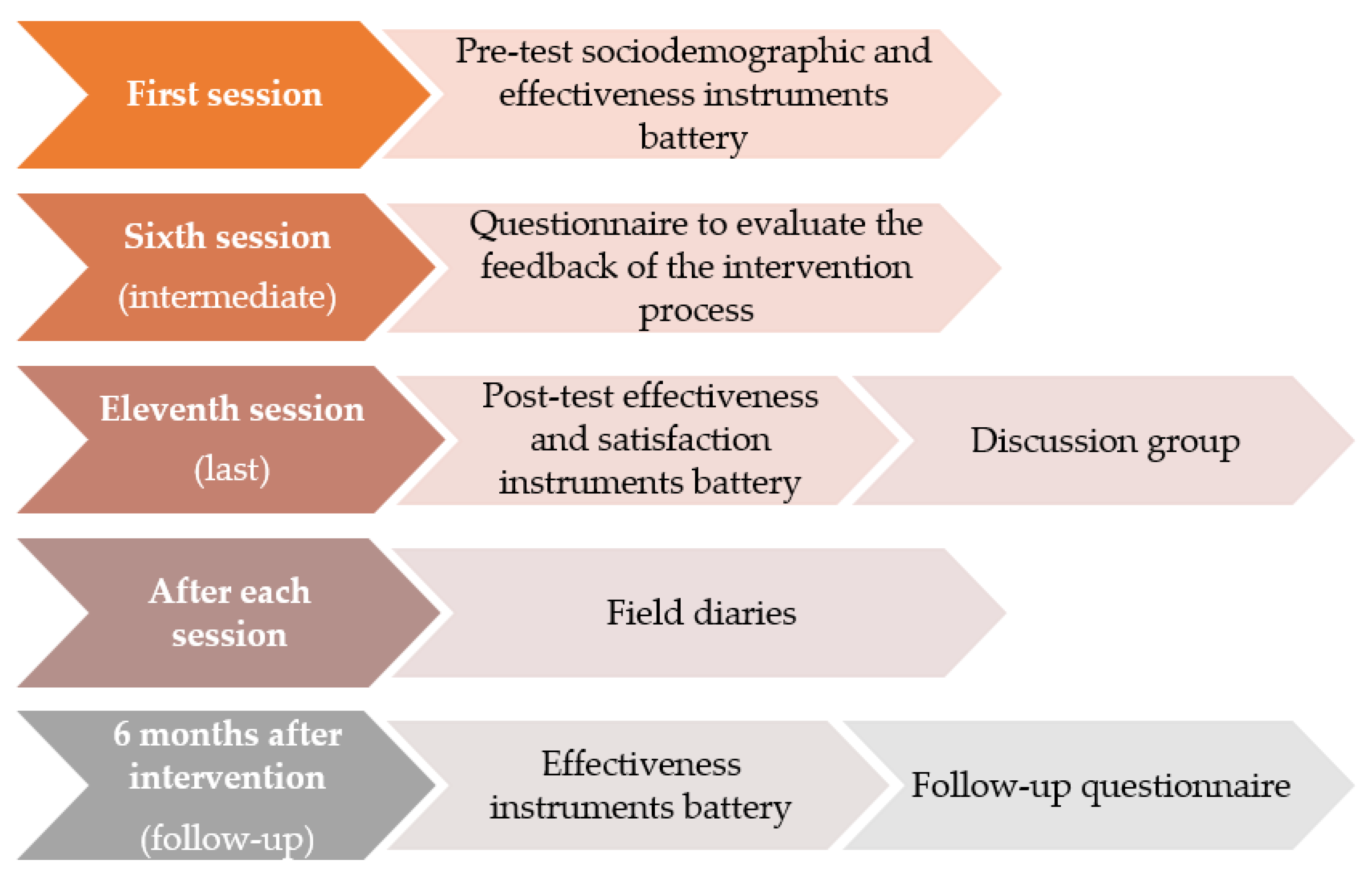
2.5.2. Process Evaluation
2.5.3. Sample Size
2.6. Data Analysis
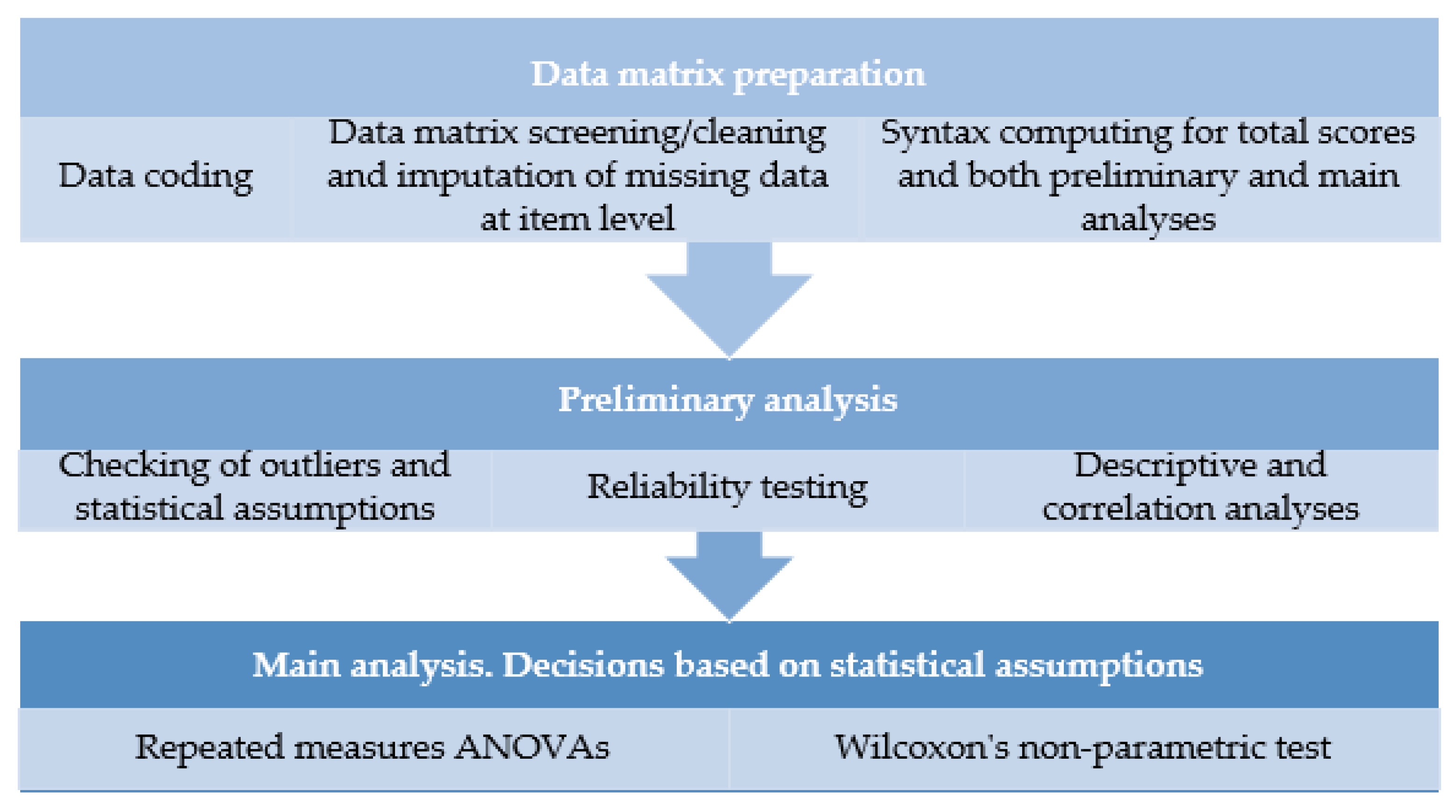
2.6.1. Quantitative Data
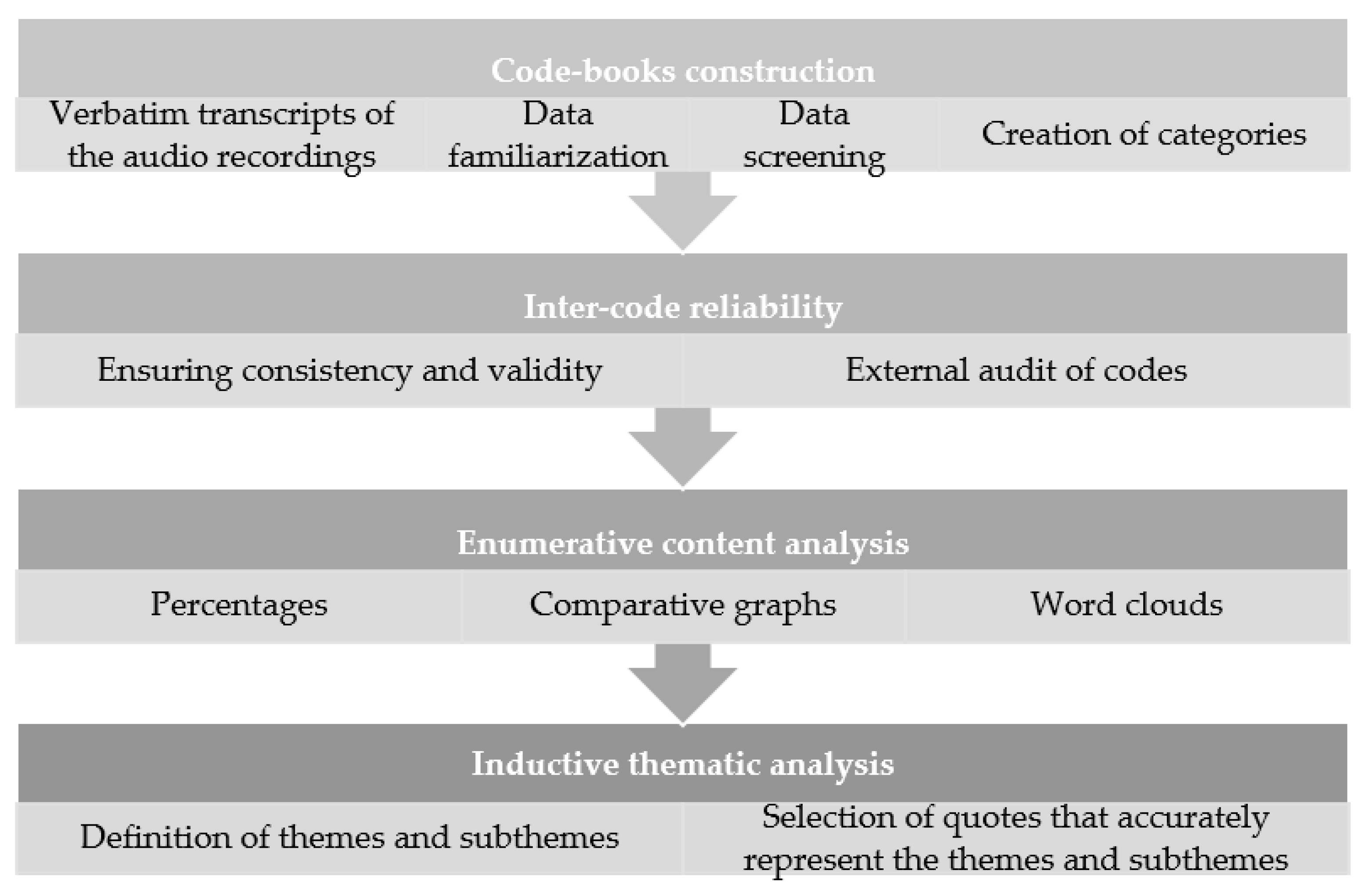
2.6.2. Qualitative Data
3. Discussion
3.1. Expected Results
3.2. Limitations
3.3. Practical Implications and Dissemination Plan
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
Appendix A.1. Sociodemographic Profile Questionnaire

{kind=link}
{kind=link}
{kind=link}
| A. THINK ABOUT YOURSELF | |
| 1. Age | |
| 2. Sex | 0. Man 1. Woman |
| 3. Educational level | 1. Without studies 2. Primary studies 3. Secondary studies 4. University studies |
| 4. Employment status | 1. Housewife or not looking for work 2. Unemployed but looking for work 3. Employed: (a) No qualification required (b) Requires medium qualification (c) Requires high qualification |
| 5. Job stability | 0. No 1. Yes |
| 6. Do you have previous experience with meditation or mindfulness? | 0. No 1. Yes. (a) Could you describe it? (b) How long? |
| 7. Do you do some kind of activity in your free time that you consider relaxing? (“stress reliever”, for example, sports, painting, cooking dances...) | 0. No 1. Yes (a) Which one? (b) How often? |
| B. THINK ABOUT YOUR FAMILY | |
| 1. Type of family | 1. Single parent 2. Bi-parental |
| 2. Number of people in the family | |
| 3. Number of children under 18 years old | |
| 4. Number of children under 14 years old | |
| 5. Family stability | 0. No 1. Yes |
| 6. Does the family own a car, van or truck? | 0. No 1. Yes, one 2. Yes, two or more |
| 7. Does each child have a room? | 0. No 1. Yes |
| 8. During the last 12 months, how many times have you traveled on family vacations (at least two nights away from home? | 0. None 1. Once 2. Twice 3. More than twice |
| 9. How many computers are there at home? (laptops and tablets are also considered computers) | 0. None 1. One 2. Two 3. More than two |
| C. THINK ABOUT YOUR CHILD | |
| 1. Age | |
| 2. Sex | 0. Boy 1. Girl |
| 3. Diagnostic category | 1. Externalizing disorders 2. Internalizing disorders 3. Others |
Appendix A.2. Feedback Questionnaire of the Intervention Process
| 1. What is your assessment of the training so far? |
| 2. Is the training meeting your expectations? |
| 3. Are you learning something useful? |
| 4. How are you feeling in the group? |
| 5. Do you think the level of explanations is appropriate for you? |
6. Do you notice changes in your body/mind as a result of these practices?
|
| 7. What are you doing to solve the difficulties you encounter? |
| 8. Honestly, do you think you spend enough time on home practices? |
| 9. To finish, I invite you to contribute with any suggestion or comment |
Appendix A.3. Field Diary
| 1. Place where the session takes place | |
| 2. Professional in charge of the group | |
| 3. Which group is it? | |
| 4. Session number | |
| 5. Date | |
| 6. Approximate length of the session | |
| 7. Program activities developed during the session (indicate time) | |
| 8. How was the atmosphere during the development of the session? Indicate whether there has been harmony between the participants during the development of the activities | 1. Not adequate 2. Somehow adequate 3. Quite adequate 4. Very adequate |
| 9. What is your general assessment of the sessions? | 1-2-3-4-5-6-7-8-9-10 |
| 10. Any noticeable issues in the session? Strengths of the program, aspects of the program that have not worked well, or other observations about the course of the session, if there has been any modification in the planning… | |
| PARTICIPANTS (This information will be provided about every participant after each session) | |
| 1. Participant identifier |
2. Medium 3. High |
Appendix A.4. Follow-Up Questionnaire
| 1. What is your assessment of the training after 6 months? |
2. What changes/benefits have you noticed in your life?
|
| 3. What mindfulness practices have you incorporated in your daily life? |
| 4. Have you been doing the home practices continuously after the end of the program? 0. No 1. Yes, few times a month 2. Yes, often, weekly 3. Yes, daily |
| 5. What has helped you to incorporate the different practices in your daily life? |
| 6. What barriers have you encountered to incorporate the different practices in your daily life? |
| 7. To finish, I invite you to contribute with any suggestion or comment |
References
- Santamaría, M.; Cebolla-Martí, A.; Rodríguez, P.; Miró-Barrachina, M. La Práctica de La Meditación y La Atención Plena: Técnicas Milenarias Para Padres Del Siglo XXI. Rev. Psicoter. 2006, 17, 157–175. [Google Scholar] [CrossRef]
- Daly, M. Parenting in Contemporary Europe: A Positive Approach; Council of Europe Publishing: Strasbourg, France, 2007. [Google Scholar]
- Resch, J.; Mireles, G.; Benz, M.R.; Grenwelge, C.; Peterson, R.; Zhang, D. Giving Parents a Voice: A Qualitative Study of the Challenges Experienced by Parents of Children with Disabilities. Rehabil. Psychol. 2010, 55, 139–150. [Google Scholar] [CrossRef]
- Rodríguez-Meirinhos, A.; Antolín-Suárez, L.; Oliva, A. Support Needs of Families of Adolescents with Mental Illness: A Systematic Mixed Studies Review. Arch. Psychiatr. Nurs. 2018, 32, 152–163. [Google Scholar] [CrossRef]
- Meppelink, R.; de Bruin, E.I.; Wanders-Mulder, F.H.; Vennik, C.J.; Bögels, S.M. Mindful Parenting Training in Child Psychiatric Settings: Heightened Parental Mindfulness Reduces Parents’ and Children’s Psychopathology. Mindfulness 2016, 7, 680–689. [Google Scholar] [CrossRef] [Green Version]
- Bögels, S.; Lehtonen, A.; Restifo, K. Mindful Parenting in Mental Health Care. Mindfulness 2010, 1, 107–120. [Google Scholar] [CrossRef] [Green Version]
- Duncan, L.G.; Coatsworth, J.D.; Greenberg, M.T. A Model of Mindful Parenting: Implications for Parent-Child Relationships and Prevention Research. Clin. Child Fam. Psychol. Rev. 2009, 12, 255–270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abidin, R.R. The Determinants of Parenting Behavior. J. Clin. Child Psychol. 1992, 21, 407–412. [Google Scholar] [CrossRef]
- Moreira, H.; Gouveia, M.J.; Canavarro, M.C. Is Mindful Parenting Associated with Adolescents’ Well-Being in Early and Middle/Late Adolescence? The Mediating Role of Adolescents’ Attachment Representations, Self-Compassion and Mindfulness. J. Youth Adolesc. 2018, 47, 1771–1788. [Google Scholar] [CrossRef]
- Neece, C.L.; Chan, N.; Klein, K.; Roberts, L.; Fenning, R.M. Mindfulness-Based Stress Reduction for Parents of Children with Developmental Delays: Understanding the Experiences of Latino Families. Mindfulness 2018, 10, 1017–1030. [Google Scholar] [CrossRef]
- Conner, C.M.; White, S.W. Stress in Mothers of Children with Autism: Trait Mindfulness as a Protective Factor. Res. Autism Spectr. Disord. 2014, 8, 617–624. [Google Scholar] [CrossRef]
- Bazzano, A.; Wolfe, C.; Zylowska, L.; Wang, S.; Schuster, E.; Barrett, C.; Lehrer, D. Mindfulness Based Stress Reduction (MBSR) for Parents and Caregivers of Individuals with Developmental Disabilities: A Community-Based Approach. J. Child Fam. Stud. 2015, 24, 298–308. [Google Scholar] [CrossRef]
- Kabat-Zinn, J. Mindfulness-Based Interventions in Context: Past, Present, and Future. Clin. Psychol. Sci. Pract. 2003, 10, 144–156. [Google Scholar] [CrossRef]
- Bögels, S.; Hoogstad, B.; van Dun, L.; de Schutter, S.; Restifo, K. Mindfulness Training for Adolescents with Externalizing Disorders and Their Parents. Behav. Cogn. Psychother. 2008, 36, 193–209. [Google Scholar] [CrossRef] [Green Version]
- Dumas, J.E. Mindfulness-Based Parent Training: Strategies to Lessen the Grip of Automaticity in Families with Disruptive Children. J. Clin. Child Adolesc. Psychol. 2005, 34, 779–791. [Google Scholar] [CrossRef]
- Emerson, L.; Aktar, E.; de Bruin, E.; Potharst, E.; Bögels, S. Mindful Parenting in Secondary Child Mental Health: Key Parenting Predictors of Treatment Effects. Mindfulness 2019, 12, 532–542. [Google Scholar] [CrossRef]
- Bertolín, J. Eficacia-Efectividad Del Programa de Reducción Del Estrés Basado En La Conciencia Plena (MBSR): Actualización. Rev. Asoc. Española Neuropsiquiatr. 2015, 35, 289–307. [Google Scholar] [CrossRef] [Green Version]
- Kabat-Zinn, J. An Outpatient Program in Behavioral Medicine for Chronic Pain Patients Based on the Practice of Mindfulness Meditation: Theoretical Considerations and Preliminary Results. Gen. Hosp. Psychiatry 1982, 4, 33–47. [Google Scholar] [CrossRef]
- Grossman, P.; Niemann, L.; Schmidt, S.; Walach, H. Mindfulness-Based Stress Reduction and Health Benefits. J. Psychosom. Res. 2004, 57, 35–43. [Google Scholar] [CrossRef]
- Minor, H.; Carlson, L.; Mackenzie, M.; Zernicke, K.; Jones, L. Evaluation of a Mindfulness-Based Stress Reduction (MBSR). Program for Caregivers of Children with Chronic Conditions. Soc. Work Health Care 2006, 43, 91–109. [Google Scholar] [CrossRef] [PubMed]
- Rayan, A.; Ahmad, M. Effectiveness of Mindfulness-Based Intervention on Perceived Stress, Anxiety, and Depression Among Parents of Children with Autism Spectrum Disorder. Mindfulness 2017, 8, 677–690. [Google Scholar] [CrossRef]
- Leinonen, J.A.; Solantaus, T.S.; Punamäki, R.L. Parental Mental Health and Children’s Adjustment: The Quality of Marital Interaction and Parenting as Mediating Factors. J. Child Psychol. Psychiatry Allied Discip. 2003, 44, 227–241. [Google Scholar] [CrossRef]
- Brassell, A.A.; Rosenberg, E.; Parent, J.; Rough, J.N.; Fondacaro, K.; Seehuus, M. Parent’s Psychological Flexibility: Associations with Parenting and Child Psychosocial Well-Being. J. Contextual Behav. Sci. 2016, 5, 111–120. [Google Scholar] [CrossRef]
- Cejudo, J.; García-Castillo, F.; Luna, P.; Rodrigo-Ruiz, D.; Feltrero, R.; Moreno-Gómez, A. Using a Mindfulness-Based Intervention to Promote Subjective Well-Being, Trait Emotional Intelligence, Mental Health, and Resilience in Women with Fibromyalgia. Front. Psychol. 2019, 10, 1–11. [Google Scholar] [CrossRef] [Green Version]
- García, M. Inteligencia Emocional: Estudiando Otras Perspectivas. Rev. Educ. Cult. Soc. 2003, 3, 143–148. [Google Scholar]
- Jung, H.; Kaur, T. The Effect of Trait Emotional Intelligence on the Relationship between Dispositional Mindfulness and Self-Esteem. Mindfulness 2017, 8, 1206–1211. [Google Scholar] [CrossRef]
- Bao, X.; Xue, S.; Kong, F. Dispositional Mindfulness and Perceived Stress: The Role of Emotional Intelligence. Personal. Individ. Differ. 2015, 78, 48–52. [Google Scholar] [CrossRef]
- Nadler, R.; Carswell, J.; Minda, J. Online Mindfulness Training Increases Well-Being, Trait Emotional Intelligence, and Workplace Competency Ratings: A Randomized Waitlist-Controlled Trial. Front. Psychol. 2020, 11, 1–19. [Google Scholar] [CrossRef]
- Neece, C.L. Mindfulness-Based Stress Reduction for Parents of Young Children with Developmental Delays: Implications for Parental Mental Health and Child Behavior Problems. J. Appl. Res. Intellect. Disabil. 2014, 27, 174–186. [Google Scholar] [CrossRef] [PubMed]
- Astbury, B.; Leeuw, F.L. Unpacking Black Boxes: Mechanisms and Theory Building in Evaluation. Am. J. Eval. 2010, 31, 363–381. [Google Scholar] [CrossRef]
- Jiménez, L.; Hidalgo, M.V. La Promoción Del Desarrollo Infantil En El Ámbito de La Preservación Familiar. ¿Cómo Se Explica El Cambio En Las Familias Que Participan En Programas de Formación y Apoyo Familiar? Sist. Fam. 2012, 28, 7–24. [Google Scholar]
- Ozdemir, M. How Much Do We Know about the Long-Term Effectiveness of Parenting Programmes? Advances, Shortcomings, and Future Directions. J. Child. Serv. 2015, 10, 120–132. [Google Scholar] [CrossRef]
- Máiquez, M.L.; Rodrigo, M.J.; Capote, C.; Vermaes, I. Aprender En La Vida Cotidiana. Un Programa Experiencial Para Padres; Aprendizaje Visor: Madrid, Spain, 2000. [Google Scholar]
- Jiménez, L.; Astiz, D.; Hidalgo, V.; Contín, M. Ensuring respect for at-risk children’s rights. Lessons learned from home- and group-based family education programs. In Realising Children’s Rights through Supporting Parents; Moran, L., Canavan, J., Eds.; UNESCO Child and Family Research Centre: Galway, Ireland, 2019; pp. 46–60. [Google Scholar]
- Schwartz, D.L.; Goldstone, R. Learning as Coordination: Cognitive Psychology and Education. In Handbook of Educational Psychology; Crono, L., Anderman, E.M., Eds.; Routledge: New York, NY, USA, 2015; pp. 61–75. [Google Scholar]
- Chambers, J.; Chrisman, J.; Trotter-Mathison, M.; Schire, M.; Dahlen, P.; Christopher, S. Perceptions of the Long-Term Influence of Mindfulness Training on Counselors and Psychotherapists: A Qualitative Inquiry. J. Humanist. Psychol. 2010, 20, 1–32. [Google Scholar] [CrossRef] [Green Version]
- Asmussen, K. The Evidence-Based Parenting Practitioner’s Handbook; Routledge: London, UK, 2011. [Google Scholar]
- Rodrigo, M.J.; Máiquez, M.L.; Martín, J.C.; Rodríguez, B. La parentalidad positiva desde la prevención y la promoción. In Manual Práctico de Parentalidad Positiva; Síntesis: Madrid, Spain, 2015; pp. 25–43. [Google Scholar]
- Daly, M.; Bray, R.; Bruckauf, Z.; Byrne, J.; Margaria, A.; Pecnik, N.; Samms-Vaughan, M. Family and Parenting Support: Policy and Provision in a Global Context; Innocenti Insight, UNICEF Office of Research: Florence, Italy, 2015. [Google Scholar]
- Rodrigo, M.J.; Maíquez, M.L.; Martín, J.C.; Byrne, S. Preservación Familiar: Un Enfoque Positivo Para La Intervención Con Familias; Pirámide: Madrid, Spain, 2008. [Google Scholar]
- Maya, J.; Jiménez, L.; Hidalgo, V.; Lorence, B. Ten psychodramatic techniques for use in psychoeducational interventions. In Psychodrama. Advances in Psychotherapy and Psychoeducational Interventions; Maya, J., Maraver, J., Eds.; Nova Sciences: Hauppauge, NY, USA, 2021; pp. 45–76. [Google Scholar]
- Irving, J.A. Mindfulness-Based Medical Practice: A Mixed-Methods Investigation of an Adapted Mindfulness-Based Stress Reduction Program for Health Care Professionals; McGill University: Montreal, QC, Canada, 2011; ISBN 9780494786451. [Google Scholar]
- Perridge, D.; Hefferon, K.; Lomas, T.; Ivtzan, I. “I Feel I Can Live Every Minute If I Choose to”: Participants’ Experience of a Positive Mindfulness Programme. Qual. Res. Psychol. 2017, 14, 482–504. [Google Scholar] [CrossRef]
- Lieber, E.; Weisner, T.S. Handbook of mixed methods in the social and behavioral sciences. In Meeting the Practical Challenges of Mixed Methods Research; Tashakkori, A., Teddlie, C., Eds.; Sage Publications: Newbury Park, CA, USA, 2010; pp. 559–580. [Google Scholar]
- Flay, B.; Biglan, A.; Boruch, R.; Castro, F.; Gottfredson, D.; Kellam, S.; Mościcki, E.; Schinke, S.; Valentine, J.; Ji, P. Standards of Evidence: Criteria for Efficacy, Effectiveness and Dissemination. Prev. Sci. 2005, 6, 151–175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gottfredson, D.C.; Cook, T.D.; Gardner, F.E.; Gorman-Smith, D.; Howe, G.W.; Sandler, I.N.; Zafft, K.M. Standards of Evidence for Efficacy, Effectiveness, and Scale-up Research in Prevention Science: Next Generation. Prev. Sci. 2015, 16, 893–926. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boyce, W.; Torsheim, T.; Currie, C.; Zambon, A. The Family Affluence Scale as a Measure of National Wealth: Validation of an Adolescent Self-Report Measure. Soc. Indic. Res. 2006, 78, 473–487. [Google Scholar] [CrossRef]
- Currie, C.; Molcho, M.; Boyce, W.; Holstein, B.; Torsheim, T.; Richter, M. Researching Health Inequalities in Adolescents: The Development of the Health Behaviour in School-Aged Children (HBSC) Family Affluence Scale. Soc. Sci. Med. 2008, 66, 1429–1436. [Google Scholar] [CrossRef]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A Global Measure of Perceived Stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef] [PubMed]
- Remor, E. Psychometric Properties of a European Spanish Version of the Perceived Stress Scale (PSS). Span. J. Psychol. 2006, 9, 86–93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barajas, S.; Garra, L. Mindfulness and Psychopathology: Adaptation of the Mindful Attention Awareness Scale (MAAS) in a Spanish Sample. Clin. Salud 2014, 25, 19–37. [Google Scholar] [CrossRef] [Green Version]
- Brown, K.W.; Ryan, R.M. The Benefits of Being Present: Mindfulness and Its Role in Psychological Well-Being. J. Personal. Soc. Psychol. 2003, 84, 822–848. [Google Scholar] [CrossRef] [Green Version]
- Bar-On, R. The Bar-On Model of Emotional-Social Intelligence (ESI). Psicothema 2006, 18, 13–25. [Google Scholar]
- Bar-On, R. Emotional and social intelligence: Insights from the Emotional Quotient Inventory. In The Handbook of Emotional Intelligence; Bar-On, R., Parker, J.D.A., Eds.; Jossey-Bass: San Francisco, CA, USA, 2000; pp. 363–388. [Google Scholar]
- López-Zafra, E.; Martos, P.; Berrios, P. EQI-Versión Corta (EQI-C). Adaptación y Validación al Español Del EQ-i En Universitarios. Boletín Psicol. 2014, 110, 21–36. [Google Scholar]
- Goldberg, D.; Hillier, V. A Scaled Version of the General Health Questionnaire. Psychol. Med. 1979, 9, 139–145. [Google Scholar] [CrossRef] [PubMed]
- Lobo, A.; Pérez-Echeverría, M.; Artal, J. Validity of the Scaled Version of the General Health Questionnaire (GHQ-28) in a Spanish Population. Psychol. Med. 1986, 16, 135–140. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, V.E.; Matthews, J.M.; Crawford, S.B. Development and Preliminary Validation of a Parenting Self-Regulation Scale: “Me as a Parent”. J. Child Fam. Stud. 2015, 24, 2853–2864. [Google Scholar] [CrossRef]
- Blacker, M.; Meleo, F.; Kabat-Zinn, J.; Santorelli, S. Reducción de Estrés Basado En Mindfulness. Mindfulness Based Stress Reduction (MBSR); Center for Mindfulness: Worcester, MA, USA, 2009. [Google Scholar]
- Larsen, D.L.; Attkisson, C.C.; Hargreaves, W.A.; Nguyen, T.D. Assessment of Client/Patient Satisfaction: Development of a General Scale. Eval. Program Plan. 1979, 2, 197–207. [Google Scholar] [CrossRef]
- Roberts, R.E.; Attkisson, C.C. Assessing Client Satisfaction among Hispanics. Eval. Program Plan. 1983, 6, 401–413. [Google Scholar] [CrossRef]
- Ley 2/1998, de 15 de Junio, de Salud de Andalucía. Boletín Oficial del Estado, 185, de 4 de Agosto de 1998, 1–28. Available online: https://www.boe.es/buscar/pdf/1998/BOE-A-1998-18720-consolidado.pdf (accessed on 10 April 2020).
- Junta de Andalucía. Conserjería de Salud. In III Plan Integral De Salud Mental De Andalucía 2016–2020; Consejería de Salud—Junta de Andalucía: Seville, Spain, 2016. [Google Scholar]
- Jiménez, P.; Baena, S.; López, E.; Martín, F.; Jiménez, L. Evaluación de Un Programa de Intervención Psicoeducativa Basado En MBSR. Una Experiencia Para La Promoción Del Bienestar y Humanización de La Sanidad a Través de La Atención Plena; University of Seville: Seville, Spain, 2017; unpublished work. [Google Scholar]
- The World Medical Association. Declaración de Helsinki de La AMM—Principios Éticos Para Las Investigaciones Médicas En Seres Humanos; World Medical Association: Ferney-Voltaire, France, 2013. [Google Scholar]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A. Statistical Power Analyses Using G*Power 3.1: Tests for Correlation and Regression Analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 1988. [Google Scholar]
- Cohen, J. Statistical Power Analysis. Curr. Dir. Psychol. Sci. 1992, 1, 98–101. [Google Scholar] [CrossRef]
- Tabachnick, B.G.; Fidell, L.S. Using Multivariate Statistics, 5th ed.; Pearson Education: New York, NY, USA, 2007. [Google Scholar]
- IBM Corp. SPSS for Windows, Version 25.0 [Computer Software]. 2017. Available online: https://www.ibm.com/es-es/analytics/spss-statistics-software (accessed on 10 July 2021).
- IBM SPSS. IBM SPSS Missing Data 25; IBM: Armonk, NY, USA, 2017. [Google Scholar]
- Moreno, E. SPSS User Manual, 1st ed.; UNED: Madrid, Spain, 2008. [Google Scholar]
- Hair, J.; Anderson, R.; Tatham, R.; Black, W. Multivariate Analysis; Pearson Prentice Hall: Hoboken, NJ, USA, 2008; ISBN 978-0138132637. [Google Scholar]
- Trigo, M.E. Diseños y Análisis Estadísticos Básicos En Psicología. Apuntes de Diseños y Análsis de Datos II; Iris Copy, S.L., Ed.; University of Seville: Seville, Spain, 2014; ISBN 978-84-941962-5-6. [Google Scholar]
- Field, A. Discovering Statistics Using SPSS, 3th ed.; SAGE Publications: London, UK, 2009. [Google Scholar]
- QSR International. NVivo Qualitative Data Analysis Software, Version 12.0 [Computer Software]. 2018. Available online: https://www.qsrinternational.com/nvivo-qualitative-data-analysis-software/home (accessed on 8 July 2021).
- Ngulube, P. Qualitative data analysis and interpretation: Systematic search for meaning. In Addressing Research Challenges: Making Headway for Developing Researchers; Mathipa, E., Gumbo, M., Eds.; Mosala-MASEDI Publishers & Booksellers CC: Midrand, Gauteng, South Africa, 2015; pp. 131–156. [Google Scholar]
- Braun, V.; Clarke, V. Using Thematic Analysis in Psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Campbell, J.L.; Quincy, C.; Osserman, J.; Pedersen, O.K. Coding In-Depth Semistructured Interviews: Problems of Unitization and Intercoder Reliability and Agreement. Sociol. Methods Res. 2013, 42, 294–320. [Google Scholar] [CrossRef]
- Hennink, M.M.; Kaiser, B.N.; Weber, M.B. What Influences Saturation? Estimating Sample Sizes in Focus Group Research. Qual. Health Res. 2019, 29, 1483–1496. [Google Scholar] [CrossRef] [PubMed]
- Kumpfer, K.L.; Magalhães, C.; Xie, J. Cultural Adaptations of Evidence-Based Family Interventions to Strengthen Families and Improve Children’s Developmental Outcomes. Eur. J. Dev. Psychol. 2012, 9, 104–116. [Google Scholar] [CrossRef]
- Hidalgo, M.V.; Jiménez, L.; López-Verdugo, I.; Lorence, B.; Sánchez, J. “Family Education and Support” Program for Families at Psychosocial Risk: The Role of Implementation Process. Psychosoc. Interv. 2016, 25, 79–85. [Google Scholar] [CrossRef] [Green Version]
- Lin, L.; He, G.; Yan, J.; Gu, C.; Xie, J. The Effects of a Modified Mindfulness-Based Stress Reduction Program for Nurses: A Randomized Controlled Trial. Workplace Health Saf. 2018, 67, 111–122. [Google Scholar] [CrossRef]
- Hou, R.J.; Wong, S.Y.; Yip, B.H.; Hung, A.T.; Lo, H.H.; Chan, P.H.; Lo, C.S.; Kwok, T.C.; Tang, W.K.; Mak, W.W.; et al. The Effects of Mindfulness-Based Stress Reduction Program on the Mental Health of Family Caregivers: A Randomized Controlled Trial. Psychother. Psychosom. 2014, 83, 45–53. [Google Scholar] [CrossRef] [Green Version]
- Keng, S.L.; Smoski, M.J.; Robins, C.J.; Ekblad, A.G.; Brantley, J.G. Mechanisms of Change in Mindfulness-Based Stress Reduction: Self-Compassion and Mindfulness as Mediators of Intervention Outcomes. J. Cogn. Psychother. 2012, 26, 270–280. [Google Scholar] [CrossRef]
- Alsubaie, M.; Abbott, R.; Dunn, B.; Dickens, C.; Keil, T.F.; Henley, W.; Kuyken, W. Mechanisms of Action in Mindfulness-Based Cognitive Therapy (MBCT) and Mindfulness-Based Stress Reduction (MBSR) in People with Physical and/or Psychological Conditions: A Systematic Review. Clin. Psychol. Rev. 2017, 55, 74–91. [Google Scholar] [CrossRef]
- Maddock, A.; Blair, C. How Do Mindfulness-Based Programmes Improve Anxiety, Depression and Psychological Distress? A Systematic Review. Curr. Psychol. 2021. [Google Scholar] [CrossRef]
- Parsons, C.E.; Crane, C.; Parsons, L.J.; Fjorback, L.O.; Kuyken, W. Home Practice in Mindfulness-Based Cognitive Therapy and Mindfulness-Based Stress Reduction: A Systematic Review and Meta-Analysis of Participants’ Mindfulness Practice and Its Association with Outcomes. Behav. Res. Ther. 2017, 95, 29–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yalom, I.D.; Leszcz, M. The Theory and Practice of Group Psychotherapy, 5th ed.; Basic Book: New York, NY, USA, 2005. [Google Scholar]
- Des Jarlais, D.C.; Lyles, C.; Crepaz, N.; Trend Group. Improving the Reporting Quality of Non-randomized Evaluations of Behavioral and Public Health Interventions: The TREND Statement. Am. J. Public Health 2004, 94, 361–366. [Google Scholar] [CrossRef] [PubMed]
- Dey, M.; Wang, J.; Jorm, A.F.; Mohler-Kuo, M. Children with Mental versus Physical Health Problems: Differences in Perceived Disease Severity, Health Care Service Utilization and Parental Health Literacy. Soc. Psychiatry Psychiatr. Epidemiol. 2015, 50, 407–418. [Google Scholar] [CrossRef] [Green Version]
- Alsem, M.W.; Siebes, R.C.; Gorter, J.W.; Jongmans, M.J.; Nijhuis, B.G.J.; Ketelaar, M. Assessment of Family Needs in Children with Physical Disabilities: Development of a Family Needs Inventory. Child Care Health Dev. 2014, 40, 498–506. [Google Scholar] [CrossRef]
- Kazdin, A.E. Evidence-Based Treatment Research: Advances, Limitations, and next Steps. Am. Psychol. 2011, 66, 685–698. [Google Scholar] [CrossRef] [Green Version]
- Council of Europe. Recommendation Rec (2006) 19 of the Committee of Ministers to Member States on Policies to Support the Positive Exercise of Parenting; Council of Europe: Strasbourg, France, 2006. [Google Scholar]
- Fixsen, D.; Naoom, S.; Blase, K.; Friedman, R.; Wallace, F. Implementation Research: A Synthesis of the Literature; University of South FL: Tampa, FL, USA, 2005. [Google Scholar]
- Small, S.A.; Cooney, S.M.; O’Connor, C. Evidence-Informed Program Improvement: Using Principles of Effectiveness to Enhance the Quality and Impact of Family-Based Prevention Programs. Fam. Relat. 2009, 58, 1–13. [Google Scholar] [CrossRef]
- Cartwright, N.; Hardie, J. Evidence-Based Policy. A Practical Guide to Doing It Better; Oxford University Press: Oxford, UK, 2012. [Google Scholar]
- Kilburn, M.R.; Mattox, T. Using Evidence to Strengthen Policies for Investing in Children; RAND Corporation: Santa Monica, CA, USA, 2016. [Google Scholar]



| Session | Contents |
|---|---|
| 1 | Informative session: Presentations, brief explanation of the program, guidelines to follow during the program, group norms, and recommendations to obtain the maximum benefit. Pre-test sociodemographic and effectiveness instruments battery; |
| 2 | Introduction to mindfulness: Theoretical and conceptual bases of the program, application of self-regulation skills, and introductory breathing practices. Theoretical explanation of the seven bases of mindfulness, such as nonjudgement, trusting, and beginner’s mind. Some of the practices will include the raising exercise to refine the senses and be aware of how one perceives one’s experiences through one’s senses. Home practices will be 10 min meditations focusing on breathing; |
| 3 | Finding your anchor: Meditation centered on breathing, and the foundation of the mindfulness triangle of thoughts, emotions, and sensations. Introduction of some inspirational readings, so as to be aware of the emotions, thoughts and sensations that emerge during those readings. Home practices will be 2 min breathing exercises and inspirational readings to observe the triangle previously described; |
| 4 | Corporal scanning: Conscious stretching exercises. Body scan, guiding practice so as to be able to become aware of the sensations that are emerging through attention to breathing. Sequenced aware movements will also be introduced. Home practices will be 10 min meditations and a calendar of positive events, where participants will write down certain positive events that have happened throughout the week in a systematic way, following certain directions; |
| 5 | Connecting with stress: Reflection on stressful experiences, how they are coped with, and how they interfere with daily life (being aware of their emotional reactivity and behavioral patterns). Identification and naming of the stressors in their parenting role. Distinction between reacting and responding to stress, being aware of their reactivity in those stressful situations and learning to put a stop to it; One-to-one communication dynamic to help the participants to be aware of their own active hearing and their communication patterns, and how a lot of their parenting stressors are related to communication problems. Group sharing of the calendar of positive events and their parenting experience, also connecting their own parenting experiences and the pain and difficulties they have faced with their physical experience. Home practices will be 24 min meditations and a calendar of negative events; |
| 6 | Open meditation: Meditation with the five elements: breathing, body, sounds, thoughts as conscious events (differentiating the event from the content), and open presence (receive what there is in the present moment). Group sharing of the calendar of negative events. Incorporation of more silent spaces in the guided meditations. Second communicative dynamic, with a focus on coping strategies focused on the problem and the emotion. The session will finish with an inspirational reading. Home practices will be 24 min meditations, and applying the reactivity versus responding in those situations that are stressors for them. Conscious movements and watching of audiovisual material with a focus on parenting (being aware that parenting involves letting go and giving life for them to be autonomous). Questionnaire to evaluate the feedback of the intervention process; |
| 7 | Relating to new experiences: Group dynamic that makes the participants change their sitting place and change their routine, reflecting on how that change influences their thoughts, emotions, and bodily experiences. Transformational coping strategies, attitudes, and behaviors that improve psychological characteristics such as strength in the face of stress or resilience. Group dynamic on relational styles (role-playing with the different relational styles and after group discussion). Emphasis on the internal resources and being able to identify them. Communication dynamic to identify different communication patterns, with participants identifying their own communication styles. Learning of other anchors besides breathing. Questionnaire to evaluate the feedback of the intervention process. Home practices will be 24 min meditations; |
| 8 | Strengthening learning (intensive day): Day of silence, application of MBSR-based skills in different life situations. Emphasis on the awareness of the present moment and silent sharing with other parents. Importance of walking meditation. Emphasis on the fact that this day does not necessarily involve a nice experience, and acceptance of this uncomfortable experience; |
| 9 | Listen to yourself: Meditation practices in silence without guidance. Discovering inner voices through guided meditations and encouraging personal reflection. Reflection on what the participants want to remember, what they have learned about themselves, and things that they have been emotional about. Writing of a letter with three short-term challenges and long-term challenges, and the possible barriers. Introduction of the positive parenting sessions; |
| 10 | Specific positive parenting session: Emphasis on the complexity of the parenting role and reflection on how each person’s own history shapes how they are as parents, working on the awareness of their established patterns as a parent. Attachment and communication along with the promotion of autonomy in their children. Communication dynamics based on listening with full attention, non-judgmental acceptance, and compassion. Additionally, assertive communication strategies, with an emphasis on being aware of the child’s thoughts and feelings and not judging them while talking to them; |
| 11 | Specific positive parenting session: Parenting practices related to establishing limits without being authoritarian, adapting those practices to the developmental period of their children and the importance of negotiation, particularly during adolescence. Focus on self-regulation and expectations as key elements to avoid the escalation of possible conflictive situations. Role-playing of emerging situations related to their parenting roles. For example, a common emergent situation would be a child arriving home after curfew. Parents represent those situations and work on how to avoid reacting rather than responding, how to handle their emotions, and how to be aware of their own and their child’s responses. Post-test effectiveness and satisfaction instruments battery and discussion group. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pizarro-Carmona, A.; Baena, S.; Jiménez, P.; Jiménez, L. Protocol for the Implementation and Evaluation of a Mindfulness-Based Intervention for Caregivers of Children with Mental Disorders in a Clinical Setting. Int. J. Environ. Res. Public Health 2021, 18, 10777. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182010777
Pizarro-Carmona A, Baena S, Jiménez P, Jiménez L. Protocol for the Implementation and Evaluation of a Mindfulness-Based Intervention for Caregivers of Children with Mental Disorders in a Clinical Setting. International Journal of Environmental Research and Public Health. 2021; 18(20):10777. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182010777
Chicago/Turabian StylePizarro-Carmona, Ana, Sofía Baena, Patricia Jiménez, and Lucía Jiménez. 2021. "Protocol for the Implementation and Evaluation of a Mindfulness-Based Intervention for Caregivers of Children with Mental Disorders in a Clinical Setting" International Journal of Environmental Research and Public Health 18, no. 20: 10777. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182010777