
Shared Decision-Making Model for Adolescent Smoking Cessation: Pilot Cohort Study

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
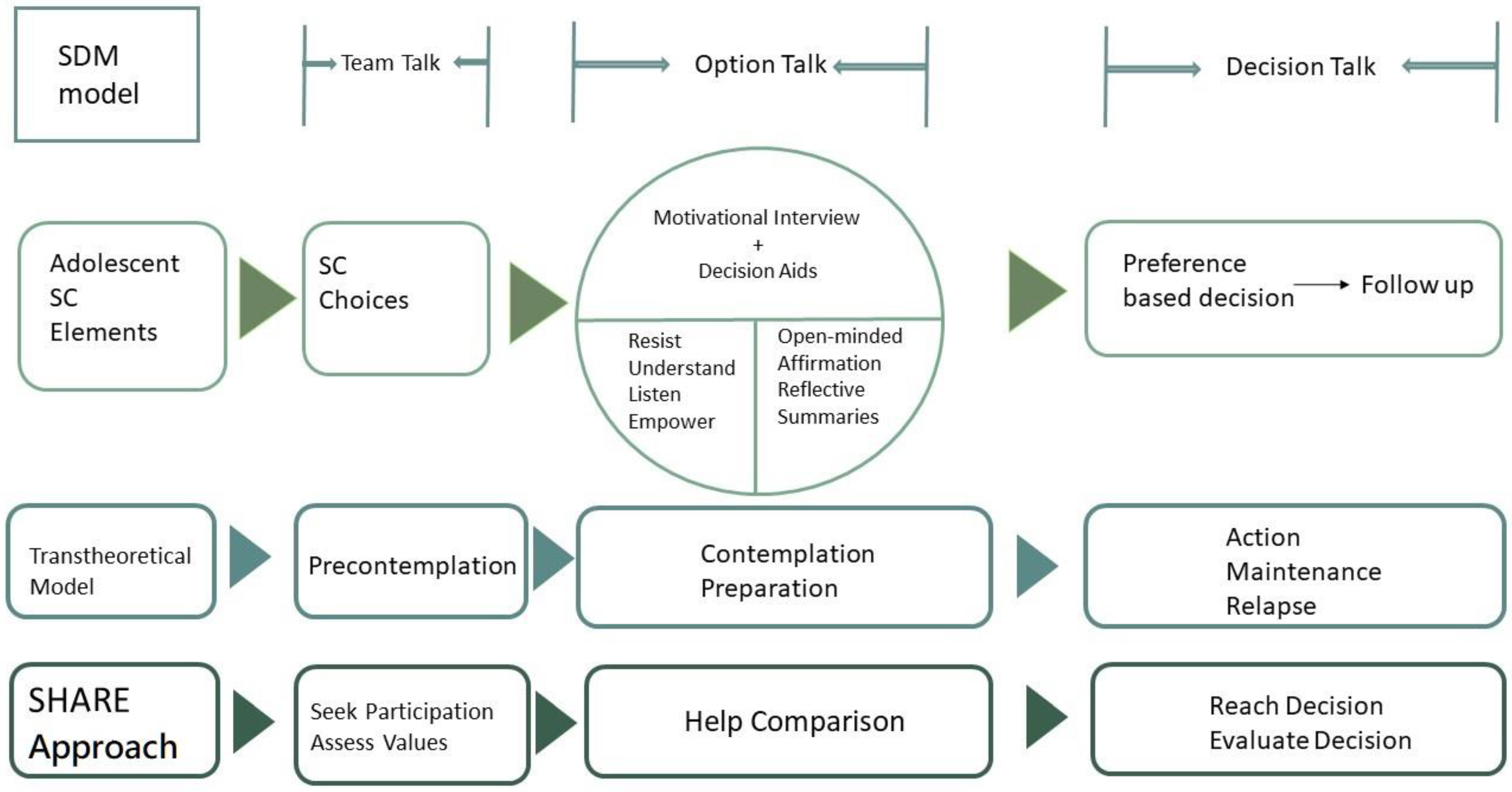
2.2. Framework of the SDM Model for Adolescent Smoking Cessation
2.3. Outcome Measurements and Analysis
3. Results
3.1. Participants
3.2. SDM Model Evaluation
3.2.1. Important Factors Related to Adolescent Smoking Cessation
3.2.2. Replies to Comprehension Test about Treatments
3.2.3. SURE Test
3.3. Satisfaction of the Cessation Model
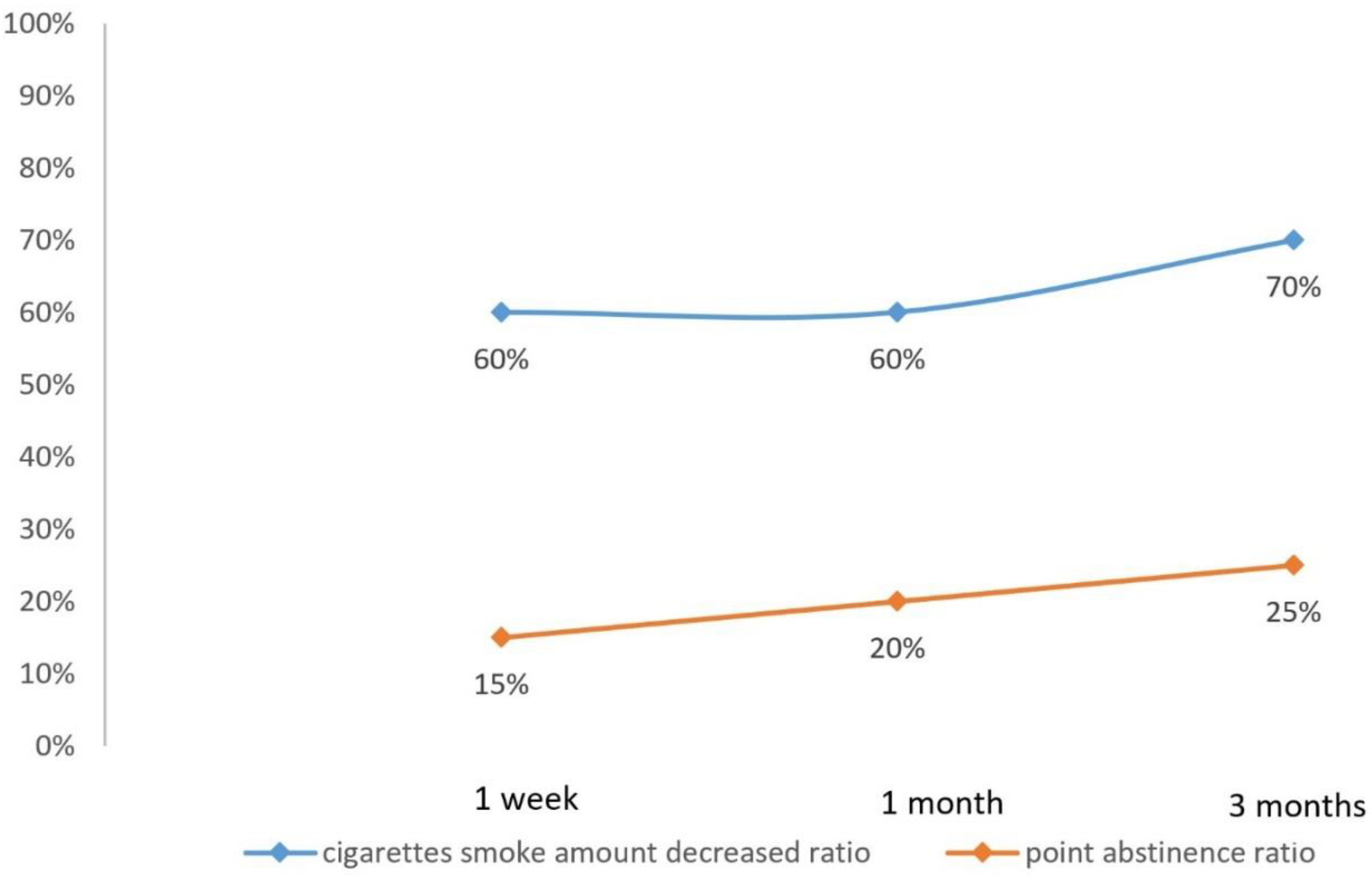
3.4. Decreased Cigarettes Smoked per Day Participants and Point Abstinence Ratio
4. Discussion
4.1. Participants Characteristics
4.2. SDM Model Evaluation
4.3. Effect on Smoking Cessation with SDM Integration
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Global Youth Tobacco Survey. GYTS. Available online: https://www.hpa.gov.tw/Pages/Detail.aspx?nodeid=1725&pid=9931 (accessed on 24 August 2021).
- World Health Organization. WHO Global Report on Trends in Prevalence of Tobacco Smoking 2000–2025, 2nd ed.; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Barrington-Trimis, J.L.; Braymiller, J.L.; Unger, J.B.; McConnell, R.; Stokes, A.; Leventhal, A.M.; Sargent, J.D.; Samet, J.M.; Goodwin, R.D. Trends in the Age of Cigarette Smoking Initiation Among Young Adults in the US From 2002 to 2018. JAMA Netw. Open 2020, 3, e2019022. [Google Scholar] [CrossRef]
- Strong, C.; Juon, H.-S.; Ensminger, M.E. Effect of Adolescent Cigarette Smoking on Adulthood Substance Use and Abuse: The Mediating Role of Educational Attainment. Subst. Use Misuse 2016, 51, 141–154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thacher, J.D.; Schultz, E.S.; Hallberg, J.; Hellberg, U.; Kull, I.; Thunqvist, P.; Pershagen, G.; Gustafsson, P.M.; Melén, E.; Bergström, A. Tobacco smoke exposure in early life and adolescence in relation to lung function. Eur. Respir. J. 2018, 51, 1702111. [Google Scholar] [CrossRef]
- Tam, J.; Brouwer, A.F. Comparison of e-cigarette use prevalence and frequency by smoking status among youth in the United States, 2014–19. Addiction 2021, 116, 2486–2497. [Google Scholar] [CrossRef] [PubMed]
- Auf, R.; Trepka, M.J.; Selim, M.; Ben Taleb, Z.; De La Rosa, M.; Bastida, E.; Cano, M.Á. E-cigarette use is associated with other tobacco use among US adolescents. Int. J. Public Health 2019, 64, 125–134. [Google Scholar] [CrossRef] [PubMed]
- Leonardi-Bee, J.; Jere, M.L.; Britton, J. Exposure to parental and sibling smoking and the risk of smoking uptake in childhood and adolescence: A systematic review and meta-analysis. Thorax 2011, 66, 847–855. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leshargie, C.T.; Alebel, A.; Kibret, G.D.; Birhanu, M.Y.; Mulugeta, H.; Malloy, P.; Wagnew, F.; Ewunetie, A.A.; Ketema, D.B.; Aderaw, A.; et al. The impact of peer pressure on cigarette smoking among high school and university students in Ethiopia: A systemic review and meta-analysis. PLoS ONE 2019, 14, e0222572. [Google Scholar] [CrossRef]
- Lim, K.H.; Ghazali, S.M.; Lim, H.L.; Cheong, K.C.; Teh, C.H.; Lim, K.K.; Heng, P.P.; Cheah, Y.K.; Lim, J.H. Smoking susceptibility among non-smoking school-going adolescents in Malaysia: Findings from a national school-based survey. BMJ Open 2019, 9, e031164. [Google Scholar] [CrossRef]
- Pacek, L.R.; McClernon, F.J.; Bosworth, H.B. Adherence to Pharmacological Smoking Cessation Interventions: A Literature Review and Synthesis of Correlates and Barriers. Nicotine Tob. Res. 2018, 20, 1163–1172. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.; Kou, G.; Peng, Y.; Zhang, Y. Estimating priorities from relative deviations in pairwise comparison matrices. Inf. Sci. 2021, 552, 310–327. [Google Scholar] [CrossRef]
- Elwyn, G.; Laitner, S.; Coulter, A.; Walker, E.; Watson, P.; Thomson, R. Implementing shared decision making in the NHS. BMJ 2010, 341, c5146. [Google Scholar] [CrossRef] [Green Version]
- McClure, J.B.; Hartzler, A.L.; Catz, S.L. Design Considerations for Smoking Cessation Apps: Feedback From Nicotine Dependence Treatment Providers and Smokers. JMIR Mhealth Uhealth 2016, 4, e17. [Google Scholar] [CrossRef] [PubMed]
- Willemsen, M.C.; Wiebing, M.; van Emst, A.; Zeeman, G. Helping smokers to decide on the use of efficacious smoking cessation methods: A randomized controlled trial of a decision aid. Addiction 2006, 101, 441–449. [Google Scholar] [CrossRef] [PubMed]
- Rios, L.E.; Herval, Á.M.; Ferreira, R.C.; Freire, M.d.C.M. Prevalences of Stages of Change for Smoking Cessation in Adolescents and Associated Factors: Systematic Review and Meta-Analysis. J. Adolesc. Health 2019, 64, 149–157. [Google Scholar] [CrossRef] [PubMed]
- Villanti, A.C.; West, J.C.; Klemperer, E.M.; Graham, A.L.; Mays, D.; Mermelstein, R.J.; Higgins, S.T. Smoking-Cessation Interventions for U.S. Young Adults: Updated Systematic Review. Am. J. Prev. Med. 2020, 59, 123–136. [Google Scholar] [CrossRef]
- Graham, A.L.; Amato, M.S.; Cha, S.; Jacobs, M.A.; Bottcher, M.M.; Papandonatos, G.D. Effectiveness of a Vaping Cessation Text Message Program Among Young Adult e-Cigarette Users. JAMA Intern. Med. 2021, 181, 923. [Google Scholar] [CrossRef] [PubMed]
- Chulasai, P.; Chinwong, D.; Chinwong, S.; Hall, J.J.; Vientong, P. Feasibility of a Smoking Cessation Smartphone App (Quit with US) for Young Adult Smokers: A Single Arm, Pre-Post Study. Int. J. Environ. Res. Public Health 2021, 18, 9376. [Google Scholar] [CrossRef]
- Elwyn, G.; Durand, M.A.; Song, J.; Aarts, J.; Barr, P.J.; Berger, Z.; Cochran, N.; Frosch, D.; Galasinski, D.; Gulbrandsen, P.; et al. A three-talk model for shared decision making: Multistage consultation process. BMJ 2017, 359, j4891. [Google Scholar] [CrossRef] [Green Version]
- Elwyn, G.; Frosch, D.; Thomson, R.; Joseph-Williams, N.; Lloyd, A.; Kinnersley, P.; Cording, E.; Tomson, D.; Dodd, C.; Rollnick, S.; et al. Shared decision making: A model for clinical practice. J. Gen. Intern Med. 2012, 27, 1361–1367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stiggelbout, A.M.; Pieterse, A.H.; De Haes, J.C. Shared decision making: Concepts, evidence, and practice. Patient Educ. Couns. 2015, 98, 1172–1179. [Google Scholar] [CrossRef] [PubMed]
- Rockville, M. The SHARE Approach. Available online: https://www.ahrq.gov/health-literacy/professional-training/shared-decision/index.html (accessed on 10 May 2021).
- Joseph-Williams, N.; Newcombe, R.; Politi, M.; Durand, M.A.; Sivell, S.; Stacey, D.; O’Connor, A.; Volk, R.J.; Edwards, A.; Bennett, C.; et al. Toward Minimum Standards for Certifying Patient Decision Aids: A Modified Delphi Consensus Process. Med. Decis. Mak. 2014, 34, 699–710. [Google Scholar] [CrossRef] [PubMed]
- Lewis, K.B.; Wood, B.; Sepucha, K.R.; Thomson, R.G.; Stacey, D. Quality of reporting of patient decision aids in recent randomized controlled trials: A descriptive synthesis and comparative analysis. Patient Educ. Couns. 2017, 100, 1387–1393. [Google Scholar] [CrossRef] [PubMed]
- Miller, W.R.; Rose, G.S. Toward a theory of motivational interviewing. Am. Psychol. 2009, 64, 527–537. [Google Scholar] [CrossRef] [PubMed]
- Miller, W.R.; Rollnick, S. Ten things that motivational interviewing is not. Behav. Cogn. Psychother. 2009, 37, 129–140. [Google Scholar] [CrossRef] [PubMed]
- Legare, F.; Kearing, S.; Clay, K.; Gagnon, S.; D’Amours, D.; Rousseau, M.; O’Connor, A. Are you SURE?: Assessing patient decisional conflict with a 4-item screening test. Can. Fam. Physician 2010, 56, e308-14. [Google Scholar] [PubMed]
- Vallata, A.; O’Loughlin, J.; Cengelli, S.; Alla, F. Predictors of Cigarette Smoking Cessation in Adolescents: A Systematic Review. J. Adolesc. Health 2021, 68, 649–657. [Google Scholar] [CrossRef]
- Aveyard, P.; Massey, L.; Parsons, A.; Manaseki, S.; Griffin, C. The effect of Transtheoretical Model based interventions on smoking cessation. Soc. Sci. Med. 2009, 68, 397–403. [Google Scholar] [CrossRef]
- Sim, I.; Hwang, E.; Sin, B. A Self-Reflection Program for Smoking Cessation in Adolescents: A Phenomenological Study. Int. J. Environ. Res. Public Health 2020, 17, 1085. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Participants’ Characteristics | N (%) 1 |
|---|---|
| Gender | |
| Male | 19 (95) |
| Female | 1(5) |
| Age | |
| 16 | 3 (15) |
| 17 | 6 (30) |
| 18 | 6 (30) |
| 19 | 4 (20) |
| 21 | 1 (5) |
| Mean | 17.5 |
| Years smoked | |
| Less than one | 2 (10) |
| 1 | 4 (20) |
| 1.5 | 1 (5) |
| 2 | 5 (25) |
| 3 | 4 (20) |
| 5 | 2 (10) |
| 6 | 1 (5) |
| 8 | 1 (5) |
| Number of cigarettes per day | |
| 2 | 1 (5) |
| 4 | 2 (10) |
| 5 | 1 (5) |
| 7 | 1 (5) |
| 10 | 9 (45) |
| 20 | 5 (25) |
| 40 | 1 (5) |
| Pack–Year | |
| Less than one | 7 (35) |
| 1–2 | 7 (35) |
| 2–3 | 2 (10) |
| 3–4 | 1 (5) |
| 5–6 | 1 (5) |
| 6–7 | 1 (5) |
| 16–17 | 1 (5) |
| Betel nuts usage | |
| Yes | 0 (0) |
| No | 13 (65) |
| Ceased | 2 (10) |
| Missing | 5 (25) |
| E-cigarette or vape usage | |
| Yes | 9 (45) |
| No | 6 (30) |
| Missing | 5 (25) |
| Alcohol usage | |
| Yes | 5 (25) |
| No | 10 (50) |
| Missing | 5 (25) |
| Secondhand smoke exposure | |
| Yes | 12 (60) |
| No | 3 (15) |
| Missing | 5 (25) |
| Education | |
| High school | 20 (100) |
| FTND 2 | |
| 0 | 1 (5) |
| 1 | 3 (15) |
| 2 | 3 (15) |
| 3 | 3 (15) |
| 5 | 2 (10) |
| 6 | 2 (10) |
| 7 | 1 (5) |
| Unknown | 5 (25) |
| Important factors related to adolescent smoking cessation | ||||||
| Factor | Rating N (%) 1 | |||||
| 0 | 1 | 2 | 3 | 4 | 5 | |
| Nicotine addiction level | 2 (11) | 1 (5) | 2 (11) | 7 (37) | 3 (16) | 4 (21) |
| Cessation rate | 4 (21) | 1 (5) | 5 (26) | 5 (26) | 1 (5) | 3 (16) |
| Drug adverse effect | 5 (26) | 1 (5) | 3 (16) | 6 (32) | 0 (0) | 4 (21) |
| Treatment cost | 4 (21) | 2 (11) | 1 (5) | 3 (16) | 4 (21) | 5 (26) |
| Course completion difficulty | 5 (26) | 2 (11) | 2 (11) | 4 (21) | 2 (11) | 4 (21) |
| Time needed to complete course | 5 (26) | 1 (5) | 2 (11) | 4 (21) | 3 (16) | 4 (21) |
| Effect on health brought about by cessation | 4 (21) | 1 (5) | 2 (11) | 6 (32) | 2 (11) | 4 (21) |
| Replies to comprehension test about treatments | ||||||
| Question | Replies; N (%) | |||||
| True | False | Not sure | ||||
| 1. The more times of counseling, the easier to achieve cessation. | 9 (47) | 3 (16) | 7 (37) | |||
| 2. All pharmacotherapy have adverse effects, better not use them. | 8 (42) | 2 (11) | 9 (47) | |||
| 3. Emotional pressure burden is better handled with professional psychological counseling. | 13 (68) | 1 (5) | 5 (26) | |||
| 4. Smoking cessation is a matter of will, counseling won’t help much. | 6 (32) | 8 (42) | 5 (26) | |||
| SURE test | ||||||
| Factor | Participants’ replies; N (%) | |||||
| Yes | No | |||||
| 1. Are you certain about your optimal choice? | 19 (100) | 0 (0) | ||||
| 2. Are you clear about the risk and benefits of each choice? | 19 (100) | 0 (0) | ||||
| 3. Are you certain about what risk and benefit has the most importance to you? | 19 (100) | 0 (0) | ||||
| 4. Did you get enough help, opinions, and support to make decisions? | 19 (100) | 0 (0) | ||||
| Factors | Rating 1 | N (%) |
|---|---|---|
| 1. Do you consider the health educational decision aids provided by the cessation team sufficient? | 5 | 7 (50) |
| 4 | 4 (29) | |
| 3 | 3 (21) | |
| 2 | 0 (0) | |
| 1 | 0 (0) | |
| 2. Were decision aids provided by the cessation team helpful in increasing the confidence of successful cessation? | 5 | 6 (43) |
| 4 | 5 (36) | |
| 3 | 3 (21) | |
| 2 | 0 (0) | |
| 1 | 0 (0) | |
| 3. Are you satisfied with the content of the cessation model? | 5 | 8 (57) |
| 4 | 3 (21) | |
| 3 | 3 (21) | |
| 2 | 0 (0) | |
| 1 | 0 (0) | |
| 4. Are you satisfied with the location of implementing the cessation model? | 5 | 8 (57) |
| 4 | 3 (21) | |
| 3 | 3 (21) | |
| 2 | 0 (0) | |
| 1 | 0 (0) | |
| 5. Are you satisfied with the overall cessation model? | 5 | 6 (43) |
| 4 | 5 (36) | |
| 3 | 3 (21) | |
| 2 | 0 (0) | |
| 1 | 0 (0) |
| 1 Week | 1 Month | 3 Months | |
|---|---|---|---|
| Decreased cigarettes smoked per day participants; N (%) | 12 (60) | 12 (60) | 14 (70) |
| Point abstinence participants ratio; N (%) | 3 (15) | 4 (20) | 5 (25) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, K.-L.; Hsu, Y.-C.; Li, Y.-H.; Guo, F.-R.; Tsai, J.-S.; Cheng, S.-Y.; Huang, H.-L. Shared Decision-Making Model for Adolescent Smoking Cessation: Pilot Cohort Study. Int. J. Environ. Res. Public Health 2021, 18, 10970. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182010970
Chen K-L, Hsu Y-C, Li Y-H, Guo F-R, Tsai J-S, Cheng S-Y, Huang H-L. Shared Decision-Making Model for Adolescent Smoking Cessation: Pilot Cohort Study. International Journal of Environmental Research and Public Health. 2021; 18(20):10970. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182010970
Chicago/Turabian StyleChen, Kuan-Lun, Yun-Chen Hsu, Yi-Hsuan Li, Fei-Ran Guo, Jaw-Shiun Tsai, Shao-Yi Cheng, and Hsien-Liang Huang. 2021. "Shared Decision-Making Model for Adolescent Smoking Cessation: Pilot Cohort Study" International Journal of Environmental Research and Public Health 18, no. 20: 10970. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182010970