
CD34 and CD105 Microvessels in Resected Bone Specimen May Implicate Wound Healing in MRONJ


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Inclusion Criteria
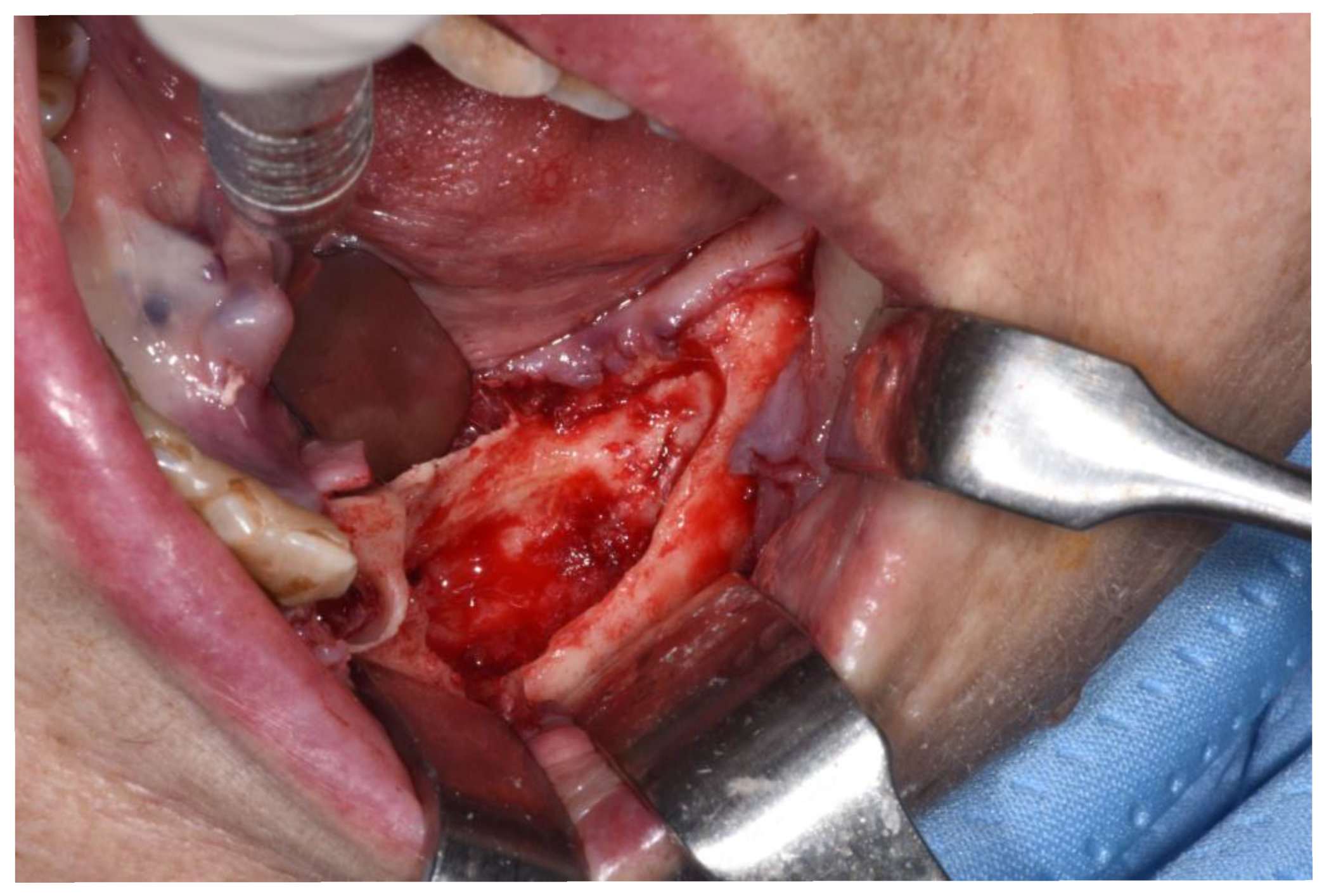
2.3. Surgery
2.4. Study Variables
2.5. Immunohistochemical Analysis
2.6. Statistical Analysis
3. Results
3.1. Conventional Risk Factors
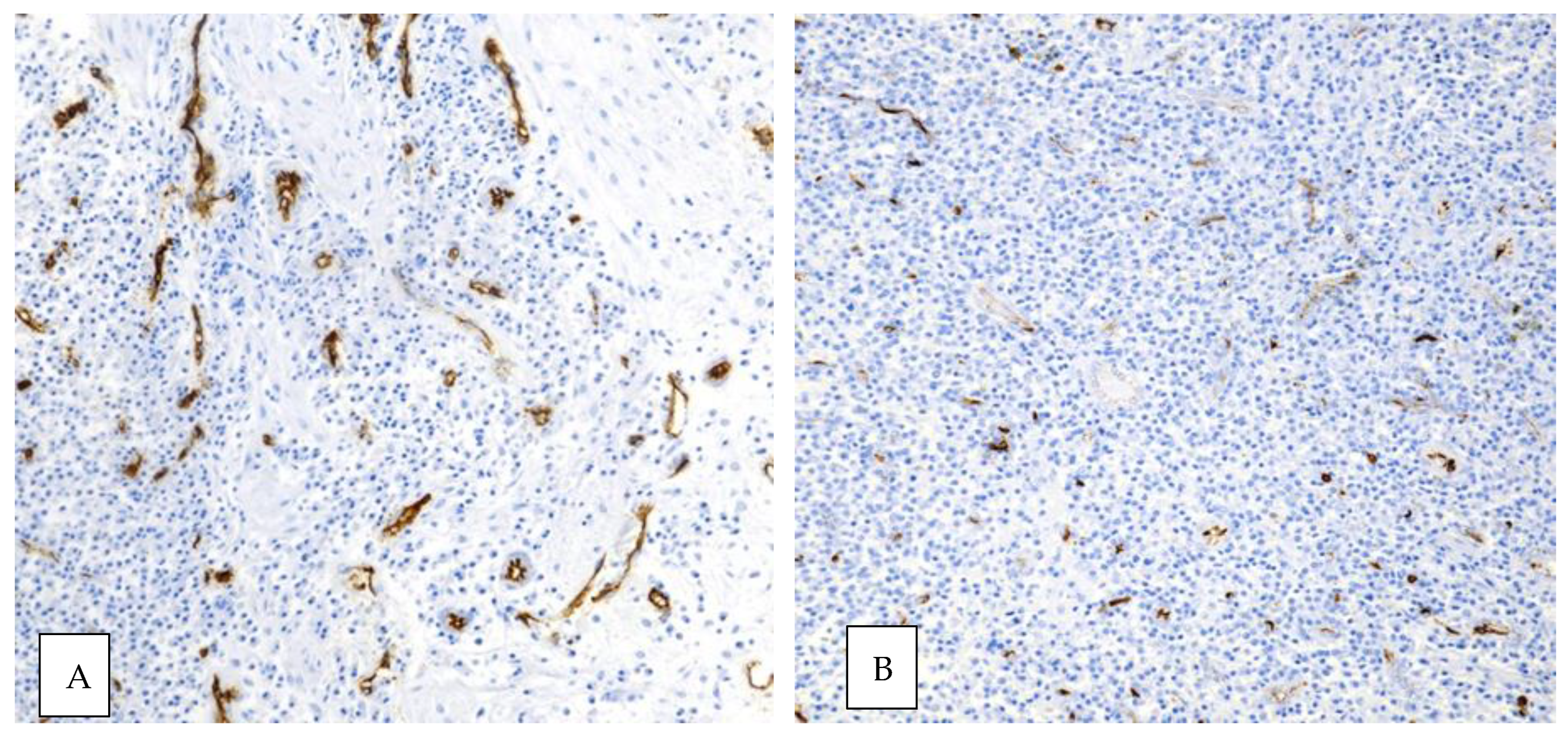
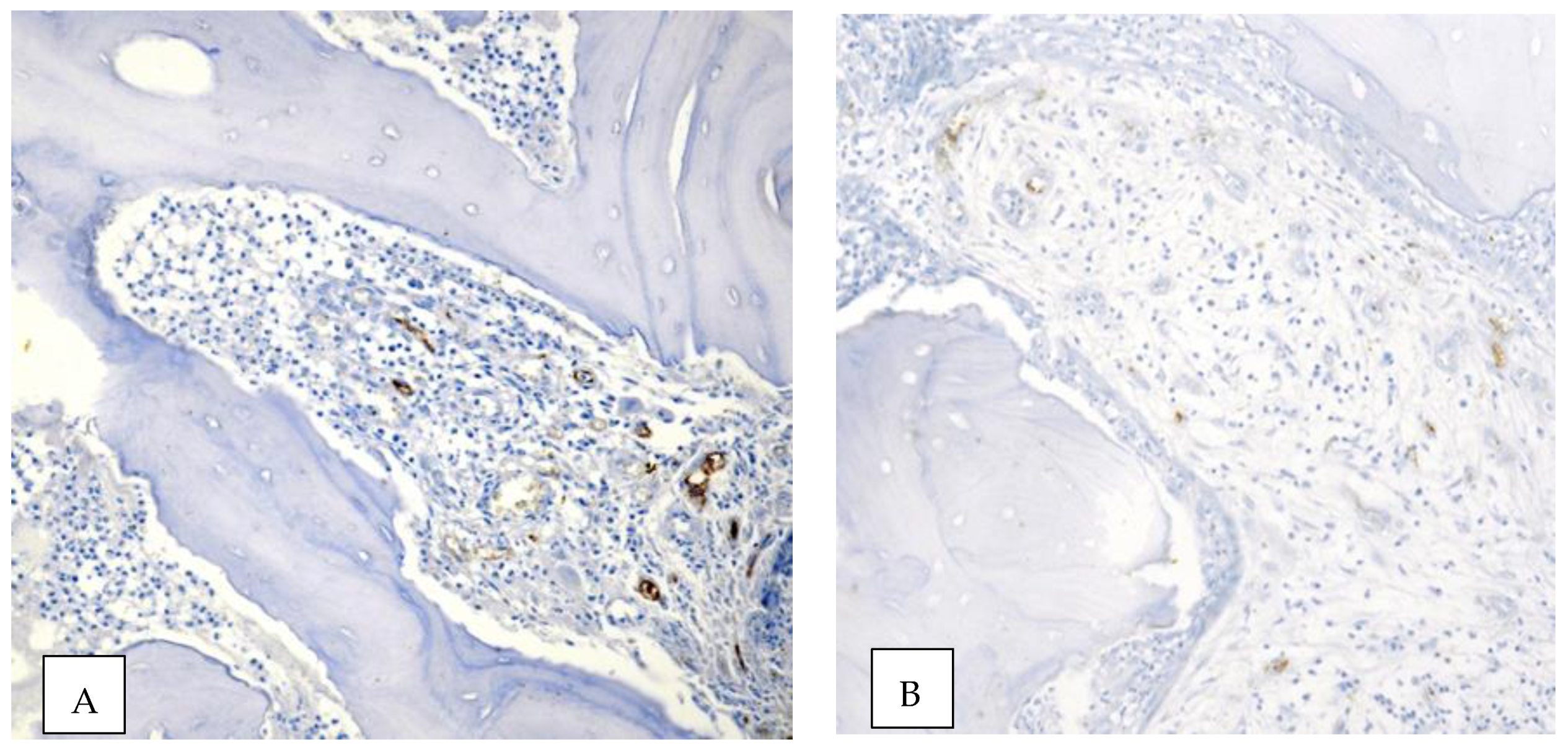
3.2. CD34 and CD105 Expression
3.3. Correlation between CD34 and CD105 Expression and Conventional Risk Factors
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ruggiero, S.L.; Dodson, T.B.; Fantasia, J.; Goodday, R.; Aghaloo, T.; Mehrotra, B.; O’Ryan, F. American Association of Oral and Maxillofacial Surgeons Position Paper on Medication-Related Osteonecrosis of the Jaw—2014 Update. J. Oral Maxillofac. Surg. 2014, 72, 1938–1956. [Google Scholar] [CrossRef]
- Oteri, G.; Trifirò, G.; Peditto, M.; Presti, L.L.; Marcianò, I.; Giorgianni, F.; Sultana, J.; Marcianó, A. Treatment of Medication-Related Osteonecrosis of the Jaw and its Impact on a Patient’s Quality of Life: A Single-Center, 10-Year Experience from Southern Italy. Drug Saf. 2017, 41, 111–123. [Google Scholar] [CrossRef]
- Oteri, G.; De Ponte, F.S.; Runci, M.; Peditto, M.; Marcianó, A.; Cicciù, M. Oral-Health-Related Quality of Life After Surgical Treatment of Osteonecrosis of the Jaws. J. Craniofacial Surg. 2018, 29, 403–408. [Google Scholar] [CrossRef] [PubMed]
- Graziani, F.; Vescovi, P.; Campisi, G.; Favia, G.; Gabriele, M.; Gaeta, G.M.; Gennai, S.; Goia, F.; Miccoli, M.; Peluso, F.; et al. Resective Surgical Approach Shows a High Performance in the Management of Advanced Cases of Bisphosphonate-Related Osteonecrosis of the Jaws: A Retrospective Survey of 347 Cases. J. Oral Maxillofac. Surg. 2012, 70, 2501–2507. [Google Scholar] [CrossRef]
- Bodem, J.P.; Schaal, C.; Kargus, S.; Saure, D.; Mertens, C.; Engel, M.; Hoffmann, J.; Freudlsperger, C. Surgical management of bisphosphonate-related osteonecrosis of the jaw stages II and III. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2016, 121, 367–372. [Google Scholar] [CrossRef] [PubMed]
- Voss, P.J.; Oshero, J.J.; Kovalova-Muller, A.; Merino, E.A.V.; Sauerbier, S.; Al-Jamali, J.; Lemound, J.; Metzger, M.C.; Schmelzeisen, R. Surgical treatment of bisphosphonate-associated osteonecrosis of the jaw: Technical report and follow up of 21 patients. J. Craniomaxillofac. Surg. 2012, 40, 719–725. [Google Scholar] [CrossRef]
- Stockmann, P.; Burger, M.; von Wilmowsky, C.; Ebker, T.; Lutz, R.; Bauersachs, A.; Nkenke, E.; Neukam, F.W.; Wehrhan, F. The outcome after surgical therapy of bisphosphonate-associated osteonecrosis of the jaw- results of a clinical case series with an average follow-up of 20 months. Clin. Oral. Investig. 2014, 18, 1299–1304. [Google Scholar] [CrossRef]
- Stanton, D.C.; Balasanian, E. Outcome of Surgical Management of Bisphosphonate-Related Osteonecrosis of the Jaws: Review of 33 Surgical Cases. J. Oral Maxillofac. Surg. 2009, 67, 943–950. [Google Scholar] [CrossRef]
- Wilde, F.; Heufelder, M.; Winter, K.; Hendricks, J.; Frerich, B.; Schramm, A.; Hemprich, A. The role of surgical therapy in the management of intravenous bisphosphonates-related osteonecrosis of the jaw. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2011, 111, 153–163. [Google Scholar] [CrossRef]
- Carlson, E.R.; Basile, J.D. The role of surgical resection in the management of bisphosphonate-related osteonecrosis of the jaws. J. Oral Maxillofac. Surg. 2009, 67 (Suppl. 5), 85–95. [Google Scholar] [CrossRef]
- Kang, M.-H.; Lee, D.-K.; Kim, C.-W.; Song, I.-S.; Jun, S.-H. Clinical characteristics and recurrence-related factors of medication-related osteonecrosis of the jaw. J. Korean Assoc. Oral Maxillofac. Surg. 2018, 44, 225–231. [Google Scholar] [CrossRef] [Green Version]
- Mücke, T.; Koschinski, J.; Deppe, H.; Wagenpfeil, S.; Pautke, C.; Mitchell, D.A.; Wolff, K.D.; Hölzle, F. Outcome of treatment and parameters influencing recurrence in patients with bisphosphonate-related osteonecrosis of the jaws. J. Cancer Res. Clin. Oncol. 2011, 137, 907–913. [Google Scholar] [CrossRef] [PubMed]
- Klingelhöffer, C.; Zeman, F.; Meier, J.; Reichert, T.E.; Ettl, T. Evaluation of surgical outcome and influencing risk factors in patients with medication-related osteonecrosis of the jaws. J. Cranio-Maxillofac. Surg. 2016, 44, 1694–1699. [Google Scholar] [CrossRef]
- Holzinger, D.; Seemann, R.; Klug, C.; Ewers, R.; Millesi, G.; Baumann, A.; Wutzl, A. Long-term success of surgery in bisphosphonate-related osteonecrosis of the jaws (BRONJs). Oral Oncol. 2013, 49, 66–70. [Google Scholar] [CrossRef]
- Kim, H.Y.; Lee, S.-J.; Kim, S.M.; Myoung, H.; Hwang, S.J.; Choi, J.-Y.; Lee, J.-H.; Choung, P.-H.; Kim, M.J.; Seo, B.M. Extensive Surgical Procedures Result in Better Treatment Outcomes for Bisphosphonate-Related Osteonecrosis of the Jaw in Patients with Osteoporosis. J. Oral Maxillofac. Surg. 2017, 75, 1404–1413. [Google Scholar] [CrossRef] [Green Version]
- Fortuna, G.; Ruoppo, E.; Pollio, A.; Aria, M.; Adamo, D.; Leuci, S.; Orabona, G.D.; Mignogna, M.D. Multiple myeloma vs. breast cancer patients with bisphosphonates-related osteonecrosis of the jaws: A comparative analysis of response to treatment and predictors of outcome. J. Oral Pathol. Med. 2011, 41, 222–228. [Google Scholar] [CrossRef]
- Lee, L.-W.; Hsiao, S.-H.; Chen, L.-K. Clinical treatment outcomes for 40 patients with bisphosphonates-related osteonecrosis of the jaws. J. Formos. Med. Assoc. 2014, 113, 166–172. [Google Scholar] [CrossRef] [Green Version]
- Bedogni, A.; Fedele, S.; Bedogni, G.; Scoletta, M.; Favia, G.; Colella, G.; Agrillo, A.; Bettini, G.; Di Fede, O.; Oteri, G.; et al. Staging of osteonecrosis of the jaw requires computed tomography for accurate definition of the extent of bony disease. Br. J. Oral Maxillofac. Surg. 2014, 52, 603–608. [Google Scholar] [CrossRef] [PubMed]
- Ristow, O.; Rückschloß, T.; Bodem, J.; Berger, M.; Bodem, E.; Kargus, S.; Engel, M.; Hoffmann, J.; Freudlsperger, C. Double-layer closure techniques after bone surgery of medication-related osteonecrosis of the jaw—A single center cohort study. J. Cranio-Maxillofac. Surg. 2018, 46, 815–824. [Google Scholar] [CrossRef]
- Stockmann, P.; Vairaktaris, E.; Wehrhan, F.; Seiss, M.; Schwarz, S.; Spriewald, B.; Neukam, F.-W.; Nkenke, E. Osteotomy and primary wound closure in bisphosphonate-associated osteonecrosis of the jaw: A prospective clinical study with 12 months follow-up. Support. Care Cancer 2009, 18, 449–460. [Google Scholar] [CrossRef] [PubMed]
- Aljohani, S.; Troeltzsch, M.; Hafner, S.; Kaeppler, G.; Mast, G.; Otto, S. Surgical treatment of medication-related osteonecrosis of the upper jaw: Case series. Oral Dis. 2019, 25, 497–507. [Google Scholar] [CrossRef]
- Park, J.-H.; Kim, J.-W.; Kim, S.-J. Does the Addition of Bone Morphogenetic Protein 2 to Platelet-Rich Fibrin Improve Healing After Treatment for Medication-Related Osteonecrosis of the Jaw? J. Oral Maxillofac. Surg. 2017, 75, 1176–1184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zirk, M.; Kreppel, M.; Buller, J.; Pristup, J.; Peters, F.; Dreiseidler, T.; Zinser, M.; Zöller, J.E. The impact of surgical intervention and antibiotics on MRONJ stage II and III—Retrospective study. J. Cranio-Maxillofac. Surg. 2017, 45, 1183–1189. [Google Scholar] [CrossRef]
- Hoefert, S.; Eufinger, H. Relevance of a Prolonged Preoperative Antibiotic Regime in the Treatment of Bisphosphonate-Related Osteonecrosis of the Jaw. J. Oral Maxillofac. Surg. 2011, 69, 362–380. [Google Scholar] [CrossRef]
- Marcianò, A.; Rubino, E.; Peditto, M.; Mauceri, R.; Oteri, G. Oral Surgical Management of Bone and Soft Tissues in MRONJ Treatment: A Decisional Tree. Life 2020, 10, 99. [Google Scholar] [CrossRef] [PubMed]
- Marcianó, A.; Peditto, M.; Cicciù, M.; Rubino, E.; Oteri, G. Role of Local Flaps to Achieve Primary Wound Closure in Medication-Related Osteonecrosis of the Jaws Osseous-Resective Surgery. J. Craniofacial. Surg. 2020, 31, e347–e352. [Google Scholar] [CrossRef] [PubMed]
- Kutzner, H. Expression of the human progenitor cell antigen CD34 (HPCA-1) distinguishes dermatofibrosarcoma protuberans from fibrous histiocytoma in formalin-fixed, paraffin-embedded tissue. J. Am. Acad. Dermatol. 1993, 28, 613–617. [Google Scholar] [CrossRef]
- Westra, W.H.; Gerald, W.L.; Rosai, J. Solitary Fibrous Tumor Consistent CD34 Immunoreactivity and Occurrence in the Orbit. Am. J. Surg. Pathol. 1994, 18, 992–998. [Google Scholar] [CrossRef]
- Favia, G.; Pilolli, G.; Maiorano, E. Histologic and histomorphometric features of bisphosphonate-related osteonecrosis of the jaws: An analysis of 31 cases with confocal laser scanning microscopy. Bone 2009, 45, 406–413. [Google Scholar] [CrossRef]
- Hansen, T.; Kunkel, M.; Weber, A.; Kirkpatrick, C.J. Osteonecrosis of the jaws in patients treated with bisphosphonates—Histomorphologic analysis in comparison with infected osteoradionecrosis. J. Oral Pathol. Med. 2006, 35, 155–160. [Google Scholar] [CrossRef]
- Wehrhan, F.; Stockmann, P.; Nkenke, E.; Schlegel, K.A.; Guentsch, A.; Wehrhan, T.; Neukam, F.W.; Amann, K. Differential impairment of vascularization and angiogenesis in bisphosphonate-associated osteonecrosis of the jaw-related mucoperiosteal tissue. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontology 2011, 112, 216–221. [Google Scholar] [CrossRef]
- Beth-Tasdogan, N.H.; Mayer, B.; Hussein, H.; Zolk, O. Interventions for managing medication-related osteonecrosis of the jaw. Cochrane Database Syst. Rev. 2017, 2017, CD012432. [Google Scholar] [CrossRef]
- Bedogni, A.; Fusco, V.; Agrillo, A.; Campisi, G. Learning from experience. Proposal of a refined definition and staging system for bisphosphonate-related osteonecrosis of the jaw (BRONJ). Oral Dis. 2012, 18, 621–623. [Google Scholar] [CrossRef] [Green Version]
- Watters, A.L.; Hansen, H.J.; Williams, T.; Chou, J.F.; Riedel, E.; Halpern, J.; Tunick, S.; Bohle, G.; Huryn, J.M.; Estilo, C.L. Intravenous bispho- sphonate-related osteonecrosis of the jaw: Long-term follow-up of 109 patients. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2013, 115, 192–200. [Google Scholar] [CrossRef] [PubMed]
- McLeod, N.M.; Patel, V.; Kusanale, A.; Rogers, S.N.; Brennan, P.A. Bisphosphonate osteonecrosis of the jaw: A literature review of UK policies versus international policies on the management of bisphosphonate osteonecrosis of the jaw. Br. J. Oral Maxillofac. Surg. 2011, 49, 335–342. [Google Scholar] [CrossRef]
- Bedogni, A.; Saia, G.; Bettini, G.; Tronchet, A.; Totola, A.; Bedogni, G.; Ferronato, G.; Nocini, P.F.; Blandamura, S. Long-term outcomes of surgical resection of the jaws in cancer patients with bisphosphonate-related osteonecrosis. Oral Oncol. 2011, 47, 420–424. [Google Scholar] [CrossRef] [PubMed]
- Kather, J.N.; Marx, A.; Reyes-Aldasoro, C.C.; Schad, L.R.; Zöllner, F.G.; Weis, C.-A. Continuous representation of tumor microvessel density and detection of angiogenic hotspots in histological whole-slide images. Oncotarget 2015, 6, 19163–19176. [Google Scholar] [CrossRef] [Green Version]
- Landesberg, R.; Woo, V.; Cremers, S.; Cozin, M.; Marolt, D.; Vunjak-Novakovic, G.; Kousteni, S.; Raghavan, S. Potential pathophysiological mechanisms in osteonecrosis of the jaw. Ann. N. Y. Acad. Sci. 2011, 1218, 62–79. [Google Scholar] [CrossRef] [Green Version]
- Fantasia, J.E. The Role of Antiangiogenic Therapy in the Development of Osteonecrosis of the Jaw. Oral Maxillofac. Surg. Clin. N. Am. 2015, 27, 547–553. [Google Scholar] [CrossRef]
- Vincenzi, B.; Napolitano, A.; Zoccoli, A.; Iuliani, M.; Pantano, F.; Papapietro, N.; Denaro, V.; Santini, D.; Tonini, G. Serum VEGF levels as predictive marker of bisphosphonate-related osteonecrosis of the jaw. J. Hematol. Oncol. 2012, 5, 56. [Google Scholar] [CrossRef] [Green Version]
- Wood, J.; Bonjean, K.; Ruetz, S.; Bellahcène, A.; Devy, L.; Foidart, J.M.; Castronovo, V.; Green, J.R. Novel antiangiogenic effects of the bisphosphonate compound zoledronic acid. J. Pharmacol. Exp. Ther. 2002, 302, 1055–1061. [Google Scholar] [CrossRef]
- Allegra, A.; Oteri, G.; Nastro, E.; Alonci, A.; Bellomo, G.; Del Fabro, V.; Quartarone, E.; Alati, C.; De Ponte, F.; Cicciù, D.; et al. Patients with bisphosphonates-associated osteonecrosis of the jaw have reduced circulating endothelial cells. Hematol. Oncol. 2007, 25, 164–169. [Google Scholar] [CrossRef]
- Gao, S.-Y.; Lin, R.-B.; Huang, S.-H.; Liang, Y.-J.; Li, X.; Zhang, S.-E.; Ouyang, D.-Q.; Li, K.; Zheng, G.-S.; Liao, G.-Q. PDGF-BB exhibited therapeutic effects on rat model of bisphosphonate-related osteonecrosis of the jaw by enhancing angiogenesis and osteogenesis. Bone 2021, 144, 115117. [Google Scholar] [CrossRef]
- Allen, M.R.; Burr, D.B. The Pathogenesis of Bisphosphonate-Related Osteonecrosis of the Jaw: So Many Hypotheses, So Few Data. J. Oral Maxillofac. Surg. 2009, 67, 61–70. [Google Scholar] [CrossRef] [Green Version]
- Hellstein, J.W.; Marek, C.L. Bisphosphonate Osteochemonecrosis (Bis-Phossy Jaw): Is This Phossy Jaw of the 21st Century? J. Oral Maxillofac. Surg. 2005, 63, 682–689. [Google Scholar] [CrossRef]
- Martins, A.S.; Correia, J.A.; Salvado, F.; Caldas, C.; Santos, N.; Capelo, A.; Palmela, P. Relevant factors for treatment outcome and time to healing in medication-related osteonecrosis of the jaws—A retrospective cohort study. J. Cranio-Maxillofac. Surg. 2017, 45, 1736–1742. [Google Scholar] [CrossRef]
- Furtado, I.; Caldas, C.; Lança, F.; Salvado, F. Anatomic factors related to bisphosphonate osteonecrosis of the jaws: A Portuguese retrospective study. Acta Med. Port. 2012, 25, 106–110. [Google Scholar]
- Ruggiero, S.L.; Kohn, N. Disease Stage and Mode of Therapy Are Important Determinants of Treatment Outcomes for Medication-Related Osteonecrosis of the Jaw. J. Oral Maxillofac. Surg. 2015, 73, S94–S100. [Google Scholar] [CrossRef]
- Voss, P.J.; Soto, G.V.; Schmelzeisen, R.; Izumi, K.; Stricker, A.; Bittermann, G.; Poxleitner, P. Sinusitis and oroantral fistula in patients with bisphosphonate-associated necrosis of the maxilla. Head Face Med. 2016, 12, 3. [Google Scholar] [CrossRef] [Green Version]
- Zhou, Y.; Yu, Y.; Shi, Y.; Li, M.; Yang, C.; Wang, S. Combined Administration of Bisphosphonates, Chemotherapeutic Agents, and/or Targeted Drugs Increases the Risk for Stage 3 Medication-Related Osteonecrosis of the Jaw: A 4-Year Retrospective Study. BioMed. Res. Int. 2020, 2020, 5847429. [Google Scholar] [CrossRef]
- Khan, A.A.; Morrison, A.; Hanley, D.A.; Felsenberg, D.; McCauley, L.K.; O’Ryan, F.; Reid, I.R.; Ruggiero, S.L.; Taguchi, A.; Tetradis, S.; et al. Diagnosis and Management of Osteonecrosis of the Jaw: A Systematic Review and International Consensus. J. Bone Miner. Res. 2015, 30, 3–23. [Google Scholar] [CrossRef]
- Yoneda, T.; Japanese Allied Committee on Osteonecrosis of the Jaw; Hagino, H.; Sugimoto, T.; Ohta, H.; Takahashi, S.; Soen, S.; Taguchi, A.; Nagata, T.; Urade, M.; et al. Antiresorptive agent-related osteonecrosis of the jaw: Position Paper 2017 of the Japanese Allied Committee on Osteonecrosis of the Jaw. J. Bone Miner. Metab. 2016, 35, 6–19. [Google Scholar] [CrossRef]
- Owosho, A.A.; Liang, S.T.Y.; Sax, A.Z.; Wu, K.; Yom, S.; Huryn, J.; Estilo, C.L. Medication-related osteonecrosis of the jaw: An update on the memorial sloan kettering cancer center experience and the role of premedication dental evaluation in prevention. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2018, 125, 440–445. [Google Scholar] [CrossRef]
- Yarom, N.; Shapiro, C.L.; Peterson, D.E.; Van Poznak, C.H.; Bohlke, K.; Ruggiero, S.L.; Migliorati, C.A.; Khan, A.; Morrison, A.; Anderson, H.; et al. Medication-Related Osteonecrosis of the Jaw: MASCC/ISOO/ASCO Clinical Practice Guideline. J. Clin. Oncol. 2019, 37, 2270–2290. [Google Scholar] [CrossRef]
- Brott, D.; Gould, S.; Jones, H.; Schofield, J.; Prior, H.; Valentin, J.; Bjurstrom, S.; Kenne, K.; Schuppe-Koistinen, I.; Katein, A. Biomarkers of drug-induced vascular injury. Toxicol. Appl. Pharmacol. 2005, 207, 441–445. [Google Scholar] [CrossRef]
- Pusztaszeri, M.P.; Seelentag, W.; Bosman, F.T. Immunohistochemical Expression of Endothelial Markers CD31, CD34, von Willebrand Factor, and Fli-1 in Normal Human Tissues. J. Histochem. Cytochem. 2006, 54, 385–395. [Google Scholar] [CrossRef] [Green Version]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Healed (n° 9) | Not Healed (n° 6) | p-Value * | |
|---|---|---|---|
| Age years (average) | 68.22 ± 8.45 | 69.17 ± 6.05 | 0.8166 |
| Sex (%) | |||
| Female | 7 (77.8) | 1 (16.7) | 0.0406 |
| Male | 2 (22.2) | 5 (83.3) | |
| Primary disease (%) | |||
| Cancer | 6 (66.7) | 6 | 0.2286 |
| Osteoporotic | 3 (33.3) | / | |
| Antiresorptive medications (%) | |||
| Zoledronic acid | 3 | 5 (83.33) | 0.1189 |
| Denosumab | 3 | 1 | 0.6044 |
| Oral bisphosphonate | 3 | / | |
| Duration of antiresorptive therapy in months (SD) | |||
| Cancer patients | 35.33 ± 18.79 | 40.33 ± 20.71 | 0.6356 |
| Osteoporotic patients | 72.33 ± 51.73 | / | |
| MRONJ Location (%) | |||
| Lower jaw | 7 | 3 | 0.3287 |
| Upper jaw | 2 | 1 | 1.0000 |
| Both jaws | / | 2 | |
| MRONJ Stage (%) | |||
| I a | 1 | / | |
| I b | / | / | |
| II a | 4 (44.4) | 1 | 0.5804 |
| II b | 3 (33.3) | 2 | 1.0000 |
| III a | / | / | |
| III b | 1 | 3 | 0.2352 |
| Healed (n° 9) | Not Healed (n° 6) | t-Value | p-Value | |
|---|---|---|---|---|
| CD34 MVD (v/mm2)—median rate | 66.57 | 3.94 | −2.33203 | 0.015756 |
| CD105 MVD (v/mm2)—median rate | 19.33 | 0 | −3.59139 | 0.000973 |
| CD34 | p-Value * | CD105 | p-Value * | |||
|---|---|---|---|---|---|---|
| Present N = 11 | Absent N = 4 | Present N = 8 | Absent N = 7 | |||
| Sex (%) | ||||||
| Female | 8 | / | 0.0256 | 6 | 2 | 0.1319 |
| Male | 3 | 4 | 2 | 5 | ||
| Primary disease (%) | ||||||
| Cancer | 8 | 4 | 0.5165 | 6 | 6 | 1.0000 |
| Osteoporotic | 3 | / | 2 | 1 | ||
| Antiresorptive medications (%) | ||||||
| Zoledronic acid | 5 | 3 | 0.5692 | 3 | 5 | 0.3147 |
| Denosumab | 3 | 1 | 1.0000 | 3 | 1 | 0.5692 |
| Oral bisphosphonate | 3 | / | 2 | 1 | 1.0000 | |
| Duration of antiresorptive therapy in months | ||||||
| ≤24 months | 5 | 1 | 0.6044 | 4 | 2 | 0.6084 |
| >24 months | 6 | 3 | 4 | 5 | ||
| MRONJ Location (%) | ||||||
| Lower jaw | 2 | 1 | 1.0000 | 1 | 2 | 0.5692 |
| Upper jaw | 9 | 1 | 0.0769 | 7 | 3 | 0.1189 |
| Both jaws | / | 2 | / | 2 | ||
| MRONJ Stage (%) | ||||||
| I a | 1 | / | 1 | / | ||
| I b | / | / | / | / | ||
| II a | 5 | / | 3 | 2 | 1.0000 | |
| II b | 3 | 2 | 0.5604 | 3 | 2 | 1.0000 |
| III a | / | / | / | / | ||
| III b | 2 | 2 | 0.5165 | 1 | 3 | 0.2821 |
| Patient Number | Age/Gender | Site of Carcinoma | Cancer Medications |
|---|---|---|---|
| 1 | 70/male | Prostate | Degarelix |
| 2 | 68/male | Myeloma | Bortezomib + Melphalan; Daratumumab; Lenalidomide + Dexamethasone |
| 3 | 79/male | Prostate | Enantone + 22RaCl |
| 4 | 72/male | Myeloma | Lenalidomide |
| 5 | 63/female | Breast | Fulvestrant Palbociclib Letrozolo |
| 6 | 63/male | Renal cell | Sunitinib; Everolimus; Sorafenib |
| 7 | 60/male | Prostate | Bicalutamide; Abiraterone acetate |
| 8 | 59/female | Breast | Tamoxifen, Letrozole, Lapatinib, Fulvestrant, Exemestane, Docetaxel, Capecitabine, Vinorelbine, Cyclophosphamide, Methotrexate, Eribulin, Doxorubicin, Palbociclib + Fulvestrant, Fluorouracil (5-FU) |
| 9 | 67/female | Breast | Everolimus; Paclitaxel; Exemestane; Doxorubicin; Anastrozole; Eribulin |
| 10 | 72/male | Breast | Cyclophosphamide + Methotrexate |
| 11 | 80/female | Breast | Everolimus + Exemestane |
| 12 | 79/female | Myeloma | Lenalidomide + Dexamethasone; Bortezomib + Melphalan + Prednisolone |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marcianò, A.; Ieni, A.; Mauceri, R.; Oteri, G. CD34 and CD105 Microvessels in Resected Bone Specimen May Implicate Wound Healing in MRONJ. Int. J. Environ. Res. Public Health 2021, 18, 11362. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182111362
Marcianò A, Ieni A, Mauceri R, Oteri G. CD34 and CD105 Microvessels in Resected Bone Specimen May Implicate Wound Healing in MRONJ. International Journal of Environmental Research and Public Health. 2021; 18(21):11362. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182111362
Chicago/Turabian StyleMarcianò, Antonia, Antonio Ieni, Rodolfo Mauceri, and Giacomo Oteri. 2021. "CD34 and CD105 Microvessels in Resected Bone Specimen May Implicate Wound Healing in MRONJ" International Journal of Environmental Research and Public Health 18, no. 21: 11362. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182111362