
Effects of a 12-Week Recreational Skiing Program on Cardio-Pulmonary Fitness in the Elderly: Results from the Salzburg Skiing in the Elderly Study (SASES)

 , and
, and
Abstract
:1. Introduction
2. Methods
3. Results
4. Discussions
5. Conclusions
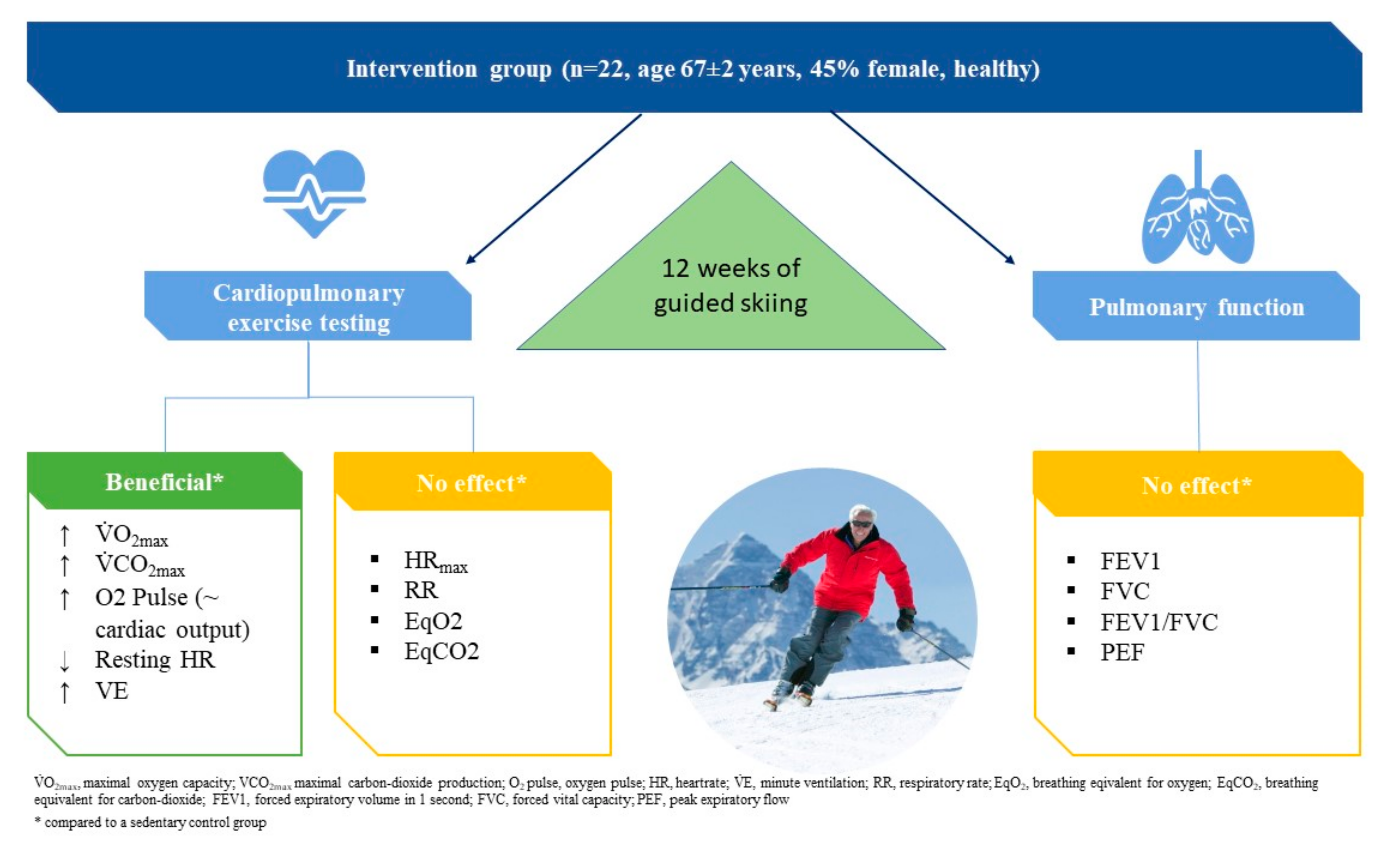
- In the elderly, regular recreational alpine skiing has similar effects on physical fitness as has been previously reported in moderate-to-high endurance training programs.
- While breathing economy, oxygen pulse, and oxygen consumption during exercise were significantly improved after alpine skiing, pulmonary function remained essentially unchanged.
- Downhill skiing is a potent and attractive exercise modality to improve cardio-pulmonary fitness in the elderly in alpine regions.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Beaver, W.L.; Wasserman, K.; Whipp, B.J. A new method for detecting anaerobic threshold by gas exchange. J. Appl. Physiol. 1986, 60, 2020–2027. [Google Scholar] [CrossRef]
- Wasserman, K.; Sietsema, K.E. Assessing Cardiac Function by Gas Exchange. Cardiology 1988, 75, 307–310. [Google Scholar] [CrossRef] [PubMed]
- Saltin, B.; Astrand, P.O. Maximal oxygen uptake in athletes. J. Appl. Physiol. 1967, 23, 353–358. [Google Scholar] [CrossRef]
- Makrides, L.; Heigenhauser, G.J.; Jones, N.L. High-intensity endurance training in 20- to 30- and 60- to 70-year-old healthy men. J. Appl. Physiol. 1990, 69, 1792–1798. [Google Scholar] [CrossRef]
- Niederseer, D.; Ledl-Kurkowski, E.; Kvita, K.; Patsch, W.; Dela, F.; Mueller, E.; Niebauer, J. Salzburg Skiing for the Elderly Study: Changes in cardiovascular risk factors through skiing in the elderly. Scand. J. Med. Sci. Sports 2011, 21, 47–55. [Google Scholar] [CrossRef]
- Badenhop, D.T.; Cleary, P.A.; Schaal, S.F.; Fox, E.L.; Bartels, R.L. Physiological adjustments to higher- or lower-intensity exercise in elders. Med. Sci. Sports Exerc. 1983, 15, 496–502. [Google Scholar] [CrossRef]
- Yerg, J.E., 2nd; Seals, D.R.; Hagberg, J.M.; Holloszy, J.O. Effect of endurance exercise training on ventilatory function in older individuals. J. Appl. Physiol. 1985, 58, 791–794. [Google Scholar] [CrossRef]
- Müller, E.; Gimpl, M.; Kirchner, S.; Kröll, J.; Jahnel, R.; Niebauer, J.; Niederseer, D.; Scheiber, P. Salzburg Skiing for the Elderly Study: Influence of alpine skiing on aerobic capacity, strength, power, and balance. Scand. J. Med. Sci. Sports 2011, 21, 9–22. [Google Scholar] [CrossRef]
- Scheiber, P.; Krautgasser, S.; von Duvillard, S.P.; Müller, E. Physiologic responses of older recreational alpine skiers to different skiing modes. Eur. J. Appl. Physiol. 2009, 105, 551. [Google Scholar] [CrossRef]
- HajGhanbari, B.; Yamabayashi, C.; Buna, T.R.; Coelho, J.D.; Freedman, K.D.; Morton, T.A.; Palmer, S.A.; Toy, M.A.; Walsh, C.; Sheel, A.W.; et al. Effects of respiratory muscle training on performance in athletes: A systematic review with meta-analyses. J. Strength Cond. Res. 2013, 27, 1643–1663. [Google Scholar] [CrossRef]
- Roman, M.A.; Rossiter, H.B.; Casaburi, R. Exercise, ageing and the lung. Eur. Respir. J. 2016, 48, 1471–1486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kippelen, P.; Caillaud, C.; Robert, E.; Connes, P.; Godard, P.; Prefaut, C. Effect of endurance training on lung function: A one year study. Br. J. Sports Med. 2005, 39, 617–621. [Google Scholar] [CrossRef] [Green Version]
- Denguezli, M.; Ben Chiekh, I.; Ben Saad, H.; Zaouali-Ajina, M.; Tabka, Z.; Zbidi, A. One-year endurance training: Effects on lung function and airway inflammation. J. Sports Sci. 2008, 26, 1351–1359. [Google Scholar] [CrossRef]
- Müller, E.; Gimpl, M.; Poetzelsberger, B.; Finkenzeller, T.; Scheiber, P. Salzburg Skiing for the Elderly Study: Study design and intervention—Health benefit of alpine skiing for elderly. Scand. J. Med. Sci. Sports 2011, 21, 1–8. [Google Scholar] [CrossRef]
- Wanger, J.; Clausen, J.L.; Coates, A.; Pedersen, O.F.; Brusasco, V.; Burgos, F.; Casaburi, R.; Crapo, R.; Enright, P.; Van Der Grinten, C.P.M.; et al. Standardisation of the measurement of lung volumes. Eur. Respir. J. 2005, 26, 511–522. [Google Scholar] [CrossRef]
- Solberg, G.; Robstad, B.; Skjønsberg, O.H.; Borchsenius, F. Respiratory gas exchange indices for estimating the anaerobic threshold. J. Sports Sci. Med. 2005, 4, 29–36. [Google Scholar]
- Balady, G.J.; Arena, R.; Sietsema, K.; Myers, J.; Coke, L.; Fletcher, G.F.; Forman, D.; Franklin, B.; Guazzi, M.; Gulati, M.; et al. Clinician’s Guide to cardiopulmonary exercise testing in adults: A scientific statement from the American Heart Association. Circulation 2010, 122, 191–225. [Google Scholar] [CrossRef] [Green Version]
- Gitt, A.K.; Wasserman, K.; Kilkowski, C.; Kleemann, T.; Kilkowski, A.; Bangert, M.; Schneider, S.; Schwarz, A.; Senges, J. Exercise Anaerobic Threshold and Ventilatory Efficiency Identify Heart Failure Patients for High Risk of Early Death. Circulation 2002, 106, 3079–3084. [Google Scholar] [CrossRef] [Green Version]
- Hagberg, J.M. Effect of training on the decline of VO2max with aging. Fed. Proc. 1987, 46, 1830–1833. [Google Scholar]
- Seals, D.R.; Hagberg, J.M.; Hurley, B.F.; Ehsani, A.A.; Holloszy, J.O. Endurance training in older men and women. I. Cardiovascular responses to exercise. J. Appl. Physiol. 1984, 57, 1024–1029. [Google Scholar] [CrossRef]
- Hagberg, J.M.; Graves, J.E.; Limacher, M.; Woods, D.R.; Leggett, S.H.; Cononie, C.; Gruber, J.J.; Pollock, M.L. Cardiovascular responses of 70- to 79-year-old men and women to exercise training. J. Appl. Physiol. 1989, 66, 2589–2594. [Google Scholar] [CrossRef]
- Bhambhani, Y.; Norris, S.; Bell, G. Prediction of Stroke Volume from Oxygen Pulse Measurements in Untrained and Trained Men. Can. J. Appl. Physiol. 1994, 19, 49–59. [Google Scholar] [CrossRef]
- Myers, J.; Prakash, M.; Froelicher, V.; Do, D.; Partington, S.; Atwood, J.E. Exercise Capacity and Mortality among Men Referred for Exercise Testing. N. Engl. J. Med. 2002, 346, 793–801. [Google Scholar] [CrossRef] [PubMed]
- Flueck, M.; Eyeang-Békalé, N.; Heraud, A.; Girard, A.; Gimpl, M.; Seynnes, O.R.; Rittweger, J.; Niebauer, J.; Mueller, E.; Narici, M. Load-sensitive adhesion factor expression in the elderly with skiing: Relation to fiber type and muscle strength. Scand. J. Med. Sci. Sports 2011, 21, 29–38. [Google Scholar] [CrossRef] [Green Version]
- Van Ginkel, S.; Amami, M.; Dela, F.; Niederseer, D.; Narici, M.V.; Niebauer, J.; Scheiber, P.; Müller, E.; Flück, M. Adjustments of muscle capillarity but not mitochondrial protein with skiing in the elderly. Scand. J. Med. Sci. Sports 2014, 25, e360–e367. [Google Scholar] [CrossRef]
- Betros, C.L.; McKeever, K.H.; Kearns, C.F.; Malinowski, K. Effects of ageing and training on maximal heart rate and VO2max. Equine Vet. J. 2002, 34, 100–105. [Google Scholar] [CrossRef]
- Kiiski, R.; Takala, J.; Kari, A.; Milic-Emili, J. Effect of Tidal Volume on Gas Exchange and Oxygen Transport in the Adult Respiratory Distress Syndrome. Am. Rev. Respir. Dis. 1992, 146, 1131–1135. [Google Scholar] [CrossRef]
- Yao, Y.-X.; Sun, X.-G.; Zheng, Z.; Wang, G.-Z.; Hansen, J.E.; Stringer, W.W.; Wasserman, K.; Hu, S.-S. Better parameters of ventilation-CO?output relationship predict death in CHF patients. Zhongguo Ying Yong Sheng Li Xue Za Zhi 2015, 31, 508–516. [Google Scholar]
- Galloza, J.; Castillo, B.; Micheo, W. Benefits of Exercise in the Older Population. Phys. Med. Rehabil. Clin. N. Am. 2017, 28, 659–669. [Google Scholar] [CrossRef]
- Bianchi, S.; Maloberti, A.; Peretti, A.; Garatti, L.; Palazzini, M.; Occhi, L.; Bassi, I.; Sioli, S.; Biolcati, M.; Giani, V.; et al. Determinants of Functional Improvement After Cardiac Rehabilitation in Acute Coronary Syndrome. High Blood Press. Cardiovasc. Prev. 2021, 1–9. [Google Scholar] [CrossRef]
- Peretti, A.; Maloberti, A.; Garatti, L.; Palazzini, M.; Triglione, N.; Occhi, L.; Sioli, S.; Sun, J.W.; Moreo, A.; Beretta, G.; et al. Functional Improvement After Outpatient Cardiac Rehabilitation in Acute Coronary Syndrome Patients is Not Related to Improvement in Left Ventricular Ejection Fraction. High Blood Press. Cardiovasc. Prev. 2020, 27, 225–230. [Google Scholar] [CrossRef] [PubMed]
- Rossi, V.A.; Schmied, C.; Niebauer, J.; Niederseer, D. Cardiovascular effects and risks of recreational alpine skiing in the elderly. J. Sci. Med. Sport 2019, 22, S27–S33. [Google Scholar] [CrossRef]


{kind=link}
| Parameter | Unit | Intervention Group | Control Group | |||||||
| Age | years | 66.8 ± 2.0 | 67.8 ± 4.3 | |||||||
| Sex | n/% | m 12 (55%); f 10 (45%) | m 10 (59%); f 7 (41%) | |||||||
| BMI | kg/m3 | 27.0 ± 3.4 | 25.6 ± 2.0 | |||||||
| Current/former/never smokers | n/% | 2 (9%)/7 (32%)/13 (59%) | 0 (0%)/6 (35%)/11 (65%) | p-values | ||||||
| REST | AT | MAX | REST | AT | MAX | REST | AT | MAX | ||
| HR | bpm | 70 ± 12 | 118 ± 17 | 155 ± 13 | 77 ± 13 | 128 ± 17 | 168 ± 21 | 0.066 | 0.095 | 0.119 |
| VO2 | mL/min | 383 ± 144 | 1467 ± 495 | 2376 ± 854 | 400 ± 136 | 1392 ± 459 | 2174 ± 600 | 0.19 | 0.818 | 0.386 |
| VO2*kg−1 | mL/min/kg | 4.9 ± 1.7 | 18.8 ± 6.3 | 29.9 ± 8.6 | 5.4 ± 1.6 | 18.7 ± 3.7 | 29.5 ± 6.3 | 0.114 | 0.863 | 0.798 |
| VCO2 | mL/min | 330 ± 140 | 1470 ± 492 | 2524 ± 778 | 372 ± 165 | 1396 ± 456 | 2320 ± 579 | 0.302 | 0.794 | 0.291 |
| VCO2*kg−1 | mL/min/kg | 4.2 ± 1.6 | 18.9 ± 6.2 | 32.0 ± 8.6 | 5.2 ± 2.6 | 18.7 ± 3.7 | 31.6 ± 6.4 | 0.187 | 0.889 | 0.687 |
| O2-pulse | mL | 5.6 ± 1.9 | 12.5 ± 4.2 | 15.5 ± 5.9 | 5.4 ± 2.1 | 10.9 ± 3.6 | 13.0 ± 3.4 | 0.376 | 0.218 | 0.124 |
| MET | 3.5 mL/min/kg | 1.6 ± 0.9 | 5.4 ± 1.8 | 8.5 ± 2.5 | 1.5 ± 0.5 | 5.3 ± 1.1 | 8.4 ± 1.8 | 0.117 | 0.865 | 0.793 |
| RR | x/min | 20.4 ± 5.3 | 24.5 ± 6.0 | 43.6 ± 7.6 | 20.3 ± 5.5 | 21.5 ± 6.7 | 37.4 ± 5.2 | 0.572 | 0.419 | 0.008 * |
| VE | l/min | 14.1 ± 7.9 | 46.4 ± 16.8 | 88.0 ± 24.5 | 15.5 ± 10.7 | 43.1 ± 18.4 | 81.7 ± 22.7 | 0.463 | 0.845 | 0.42 |
| VT | l | 0.8 ± 0.5 | 1.9 ± 0.6 | 2.1 ± 0.6 | 0.8 ± 0.4 | 2.1 ± 0.6 | 2.2 ± 0.6 | 0.989 | 0.552 | 0.505 |
| EqO2 | l/l | 26.6 ± 5.8 | 29.8 ± 2.7 | 46.3 ± 5.2 | 23.8 ± 5.3 | 28.8 ± 3.2 | 45.5 ± 11.0 | 0.139 | 0.684 | 0.874 |
| EqCO2 | l/l | 32.7 ± 6.8 | 29.7 ± 2.7 | 39.7 ± 4.5 | 30.3 ± 6.8 | 28.7 ± 3.2 | 41.1 ± 10.4 | 0.402 | 0.748 | 0.383 |
| Parameter | Unit | Intervention Group (n = 22) | Control Group (n = 17) | IG vs. CG POST | |||||
|---|---|---|---|---|---|---|---|---|---|
| PRE | POST | p-Value | PRE | POST | p-Value | p-Value | Δ Mean | ||
| REST | |||||||||
| HR | bpm | 70 ± 12 | 67 ± 10 | 0.307 | 76 ± 12 | 73 ± 9 | 0.136 | 0.085 | −8% |
| VO2 | mL/min | 383 ± 144 | 449 ± 171 | 0.862 | 400 ± 135 | 450 ± 177 | 0.101 | 0.497 | −0.2% |
| VO2*kg−1 | mL/min/kg | 4.9 ± 1.7 | 5.8 ± 2.3 | 0.68 | 5.4 ± 1.6 | 6.3 ± 2.5 | 0.102 | 0.666 | −8% |
| VCO2 | mL/min | 330 ± 140 | 353 ± 128 | 0.877 | 371 ± 165 | 350 ± 140 | 0.12 | 0.484 | +0.6% |
| VCO2*kg−1 | mL/min/kg | 4.2 ± 1.6 | 4.6 ± 1.7 | 0.954 | 5.2 ± 2.6 | 4.9 ± 1.9 | 0.122 | 0.690 | −7% |
| O2 pulse | mL | 5.6 ± 1.9 | 6.9 ± 2.8 | 0.476 | 5.36 ± 2.07 | 6.3 ± 2.8 | 0.253 | 0.341 | +8% |
| MET | 3.5 mL/kg/min | 1.6 ± 0.9 | 1.6 ± 0.7 | 0.669 | 1.5 ± 0.5 | 1.8 ± 0.7 | 0.106 | 0.659 | −10% |
| RR | x/min | 20 ± 5 | 20 ± 5 | 0.147 | 20 ± 6 | 17 ± 3 | 0.683 | 0.648 | +15% |
| VE | l/min | 14 ± 8 | 13.1 ± 4.8 | 0.593 | 15.5 ± 10.7 | 12.7 ± 4.2 | 0.072 | 0.328 | +3% |
| VT | l | 0.8 ± 0.5 | 0.7 ± 0.3 | 0.788 | 0.8 ± 0.4 | 0.8 ± 0.2 | 0.449 | 0.67 | −10% |
| EqO2 | l/l | 26.6 ± 5.8 | 26.4 ± 6.6 | 0.747 | 23.8 ± 5.3 | 23.4 ± 3.9 | 0.247 | 0.053 | +11% |
| EqCO2 | l/l | 32.7 ± 6.8 | 33.3 ± 8.1 | 0.916 | 30.3 ± 6.8 | 29.8 ± 4.2 | 0.154 | 0.055 | +11% |
| AT | |||||||||
| HR | bpm | 118 ± 17 | 120 ± 16 | 0.408 | 128 ± 16 | 122 ± 16 | 0.03 * | 0.61 | −2% |
| Watt | W | 105 ± 31 | 112 ± 30 | 0.115 | 95 ± 40 | 94 ± 32 | 0.556 | 0.199 | +16% |
| VO2 | mL/min | 1467 ± 495 | 1655 ± 356 | 0.036 * | 1391 ± 459 | 1354 ± 353 | 0.909 | 0.116 | +18% |
| VO2*kg−1 | mL/kg | 18.8 ± 6.3 | 21.6 ± 3.8 | 0.011 * | 18.7 ± 3.7 | 18.6 ± 3.7 | 0.579 | 0.013 * | +14% |
| VCO2 | mL/min | 1469 ± 492 | 1667 ± 350 | 0.029 * | 1396 ± 455 | 1360 ± 353 | 0.832 | 0.105 | +18% |
| VCO2*kg−1 | mL/min/kg | 18.9 ± 6.2 | 21.6 ± 3.8 | 0.012 * | 18.7 ± 3.7 | 18.7 ± 3.7 | 0.496 | 0.01 * | +13% |
| O2 pulse | mL | 12.5 ± 4.2 | 13.9 ± 3.1 | 0.075 | 10.9 ± 3.6 | 11.1 ± 3 | 0.529 | 0.007 * | +20% |
| MET | 3.5 mL/kg/min | 5.4 ± 1.8 | 6.2 ± 1.1 | 0.011 * | 5.3 ± 1.1 | 5.3 ± 1.1 | 0.588 | 0.154 | +14% |
| RR | x/min | 24 ± 6 | 24 ± 6 | 0.911 | 22 ± 7 | 23 ± 7 | 0.157 | 0.945 | +5% |
| VE | l/min | 46.4 ± 16.8 | 52.4 ± 11.1 | 0.033 | 43.1 ± 18.4 | 42.7 ± 13.5 | 0.635 | 0.28 | +19% |
| VT | l | 1.9 ± 0.6 | 2.21 ± 0.48 | 0.068 | 2.1 ± 0.6 | 1.9 ± 0.4 | 0.068 | 0.05 * | +14% |
| EqO2 | l/l | 29.8 ± 2.7 | 30.6 ± 2.6 | 0.409 | 28.8 ± 3.2 | 29.4 ± 3.7 | 0.147 | 0.948 | +2.5% |
| EqCO2 | l/l | 29.7 ± 2.7 | 29.9 ± 2.6 | 0.241 | 28.7 ± 3.21 | 29.3 ± 3.19 | 0.241 | 0.973 | +2.2% |
| MAX | |||||||||
| HR | bpm | 154 ± 12 | 155 ± 14 | 0.921 | 168 ± 21 | 160 ± 13 | 0.092 | 0.643 | −4% |
| Watt | W | 173 ± 44 | 175 ± 47 | 0.724 | 152 ± 45 | 151 ± 45 | 0.367 | 0.114 | +14% |
| VO2 | mL/min | 2375 ± 854 | 2588 ± 651 | 0.09 | 2173 ± 599 | 2093 ± 585 | 0.242 | 0.021 * | +19% |
| VO2*kg−1 | mL/min/kg | 29.9 ± 8.6 | 34 ± 8 | 0.015 * | 29.5 ± 6.3 | 28.71 ± 5.9 | 0.441 | 0.03 * | +15% |
| VCO2 | mL/min | 2523 ± 777 | 2787 ± 645 | 0.033 | 2320 ± 578 | 2313 ± 608 | 0.644 | 0.023 * | +17% |
| VCO2*kg−1 | mL/min/kg | 32.0 ± 8.6 | 36 ± 8 | 0.012 * | 31.6 ± 6.4 | 31.8 ± 6.5 | 0.387 | 0.051 | +12% |
| O2 pulse | mL | 15.5 ± 5.9 | 17 ± 4 | 0.152 | 13 ± 3.4 | 13.2 ± 4 | 0.632 | 0.01 * | +22% |
| MET | 3.5 mL/kg/min | 8.5 ± 2.5 | 10 ± 2 | 0.015 * | 8.4 ± 1.8 | 8.2 ± 1.7 | 0.417 | 0.029 * | +15% |
| RR | x/min | 43 ± 7 | 43 ± 7 | 0.805 | 37 ± 5 | 38 ± 8 | 0.494 | 0.037 * | +11% |
| VE | l/min | 88.0 ± 24.5 | 97 ± 18 | 0.017 * | 81.7 ± 22.7 | 81.3 ± 21.9 | 0.833 | 0.025 * | +16% |
| VT | l | 2.1 ± 0.6 | 2 ± 1 | 0.032 * | 2.2 ± 0.6 | 2.2 ± 0.6 | 0.738 | 0.441 | +6% |
| EqO2 | l/l | 46.3 ± 5.2 | 47 ± 6 | 0.406 | 45.5 ± 11 | 50.0 ± 6.2 | 0.390 | 0.49 | −7% |
| EqCO2 | l/l | 39.7 ± 4.5 | 42 ± 7 | 0.616 | 41.1 ± 10.3 | 42.5 ± 8 | 0.866 | 0.527 | −2% |
| Parameter | Unit | Intervention Group | Control Group | IG vs. CG POST | ||||
|---|---|---|---|---|---|---|---|---|
| PRE | POST | p-Value | PRE | POST | p-Value | p-Value | ||
| FEV1 | l | 2.91 ± 0.63 | 2.91 ± 0.53 | 0.996 | 2.74 ± 0.63 | 2.62 ± 0.57 | 0.039 | 0.107 |
| FVC | l | 3.95 ± 0.85 | 3.77 ± 0.79 | 0.010 * | 3.62 ± 0.77 | 3.52 ± 0.76 | 0.037 * | 0.318 |
| FEV1/FVC | l/l | 74.0 ± 5.5 | 77.7 ± 3.7 | <0.001 * | 75.5 ± 5.6 | 74.7 ± 5.6 | 0.683 | 0.061 |
| PEF | l/s | 6.77 ± 1.76 | 6.83 ± 1.82 | 0.803 | 6.04 ± 1.53 | 6.26 ± 2.16 | 0.507 | 0.363 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Niederseer, D.; Walser, R.; Schmied, C.; Dela, F.; Gräni, C.; Bohm, P.; Müller, E.; Niebauer, J. Effects of a 12-Week Recreational Skiing Program on Cardio-Pulmonary Fitness in the Elderly: Results from the Salzburg Skiing in the Elderly Study (SASES). Int. J. Environ. Res. Public Health 2021, 18, 11378. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182111378
Niederseer D, Walser R, Schmied C, Dela F, Gräni C, Bohm P, Müller E, Niebauer J. Effects of a 12-Week Recreational Skiing Program on Cardio-Pulmonary Fitness in the Elderly: Results from the Salzburg Skiing in the Elderly Study (SASES). International Journal of Environmental Research and Public Health. 2021; 18(21):11378. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182111378
Chicago/Turabian StyleNiederseer, David, Roman Walser, Christian Schmied, Flemming Dela, Christoph Gräni, Philipp Bohm, Erich Müller, and Josef Niebauer. 2021. "Effects of a 12-Week Recreational Skiing Program on Cardio-Pulmonary Fitness in the Elderly: Results from the Salzburg Skiing in the Elderly Study (SASES)" International Journal of Environmental Research and Public Health 18, no. 21: 11378. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182111378